Maini A. Short-term cosmetic orthodontics for general dental practitioners. Br Dent J. 2013; 214:83-84
Luqmani S. The limitations of short-term orthodontics and why we still need specialists – a review of the current literature. Dent Update. 2017; 44:64-69
Pabari S, Moles DR, Cunningham SJ. Assessment of motivation and psychological characteristics of adult orthodontic patients. Am J Orthod Dentofacial Orthop. 2011; 140:E263-E272
Bradnock G, White DA, Nuttall NM, Morris AJ, Treasure ET, Pine CM. Dental attitudes and behaviours in 1998 and implications for the future. Br Dent J. 2001; 190:228-232
Al-Kharboush GH, Asimakopoulou K, Aljabaa AH, Newton JT. The role of social comparison in social judgments of dental appearance: an experimental study. J Dent. 2017; 61:33-38
de Souza RA, de Oliveira AF, Pinheiro SM, Cardoso JP, Magnani MB. Expectations of orthodontic treatment in adults: the conduct in orthodontist/patient relationship. Dental Press J Orthod. 2013; 18:88-94
Josefsson E, Lindsten R, Hallberg LRM. A qualitative study of the influence of poor dental aesthetics on the lives of young adults. Acta Odontol Scand. 2010; 68:19-26
Eli L, Bar-Tal Y, Kostovetzki I. At first glance social meanings of dental appearance. J Public Health Dent. 2001; 61:150-154
Kerusuou H, Hausen H, Laine T, Shaw WC. The influence of incisal malocclusion on the social attractiveness of young adults in Finland. Eur J Orthod. 1995; 17:505-512
Mihalik CA, Proffit WR, Phillips C. Long-term follow-up of Class II adults treated with orthodontic camouflage: a comparison with orthognathic surgery outcomes. Am J Orthod Dentofacial Orthop. 2003; 123:266-278
Kershaw S, Newton JT, Williams DM. The influence of tooth colour on the perceptions of personal characteristics among female dental patients: comparisons of unmodified, decayed and ‘whitened’ teeth. Br Dent J. 2008; 204
Newton JT, Prabhu N, Robinson PG. The impact of dental appearance on the appraisal of personal characteristics. Int J Prosthodont. 2003; 16:429-434
Klages U, Bruckner A, Zentner A. Dental aesthetics, self-awareness, and oral health-related quality of life in young adults. Eur J Orthod. 2004; 26:507-514
Johal A, Alyaqoobi I, Patel R, Cox S. The impact of orthodontic treatment on quality of life and self-esteem in adult patients. Eur J Orthod. 2015; 37:233-237
Cochrane SM, Cunningham SJ, Hunt NP. A comparison of the perception of facial profile by the general public and 3 groups of clinicians. Int J Adult Orthodon Orthognath Surg. 1999; 14:291-295
Chate RAC. Truth or consequences: the potential implications for short-term cosmetic orthodontics for general dental practitioners. Br Dent J. 2013; 215:551-553
Mitchell L. Adult orthodontics. In: Littlewood SJ, Nelson-Moon ZL, Dyer F (eds). England: Oxford University Press; 2013
Little RM. Stability and relapse of dental arch alignment. Br J Orthod. 1990; 17:235-241
Little RM, Riedel RA, Artun J. An evaluation of changes in mandibular anterior alignment from 10 to 20 years postretention. Am J Orthod Dentofacial Orthop. 1988; 93:423-428
Atack N, Harradine N, Sandy JR, Ireland AJ. Which way forward? Fixed or removable lower retainers. Angle Orthod. 2007; 77:954-959
Feldmann I. Satisfaction with orthodontic treatment outcome. Angle Orthod. 2014; 84:581-587
Kacer K, Valiathan M, Narendran S Retainer wear and compliance in the first 2 years after active orthodontic treatment. Am J Orthod Dentofacial Orthop. 2010; 138:592-598
Schneider E, Ruf S. Upper bonded retainers. Angle Orthod. 2011; 81:1050-1056
Kotecha S, Gale S, Khamashta-Ledezma L A multicentre audit of GDP's knowledge of orthodontic retention. Br Dent J. 2015; 218:649-653
Powell S. Short-term orthodontics: History puts it straight. Br Dent J. 2014; 217
Huntley P. Orthodontics: fast and furious. Br Dent J. 2015; 218:2-3
Chate RAC. Short-Term Orthodontics Debate. Br Dent J. 2014; 216:388-389
Storey M, Forde K, Littlewood SJ, Scott P, Luther F, Kang J. Bonded versus vacuum-formed retainers: a randomized controlled trial. Part 2: periodontal health outcomes after 12 months. Eur J Orthod. 2018; 40:399-408
Boyd RL, Leggott PJ, Quinn RS, Eakle WS, Chambers D. Periodontal implications of orthodontic treatment in adults with reduced or normal periodontal tissues versus those of adolescents. Am J Orthod Dentofacial Orthop. 1989; 96:191-198
Mitchell L. Adult orthodontics. In: Littlewood SJ, Nelson-Moon ZL, Dyer F (eds). England: Oxford University Press; 2013
Gill DS, Barker CS. The multidisciplinary management of hypodontia: a team approach. Br Dent J. 2015; 218:143-149
Noar JH, Sharma S, Roberts-Harry D, Qureshi T. A discerning approach to simply aesthetic orthodontics. Br Dent J. 2015; 218:157-166
Short-term orthodontics (STO) is a concept that is being utilized principally on adult patients to correct minor dental irregularities. It is a cosmetically motivated treatment that is being increasingly sought as an alternative to conventional orthodontic treatment (COT). Although general dental practitioners (GDPs) who have completed further training can provide STO, for quality care delivery it is important to know the limitations of the scope of practice. This article aims to discuss the reasons for adults seeking STO, the societal pressures responsible for desiring it, precautions required by GDPs during patient selection and its associated risks.
CPD/Clinical Relevance: Most importantly, GDPs should have a good understanding of societal pressures that induce patients' desires to seek STO. Therefore, the dental practitioner can manage patient expectations appropriately. This highlights the challenge that not every patient's desires can be delivered with STO. Furthermore, the article explains the limits and risks of STO which should be thoroughly explained to patients in the process of obtaining valid consent.
Article
Orthodontic treatment under the National Health Service is free for children under 18 years and, in some cases, adults with severe malocclusions.1 For adults with a persisting malocclusion or aesthetic concern, treatment may be sought at an older age. Reasons for seeking adult orthodontic treatment include:
Lack of awareness to seek orthodontic treatment during adolescence;
Lack of compliance with orthodontic treatment during adolescence;
Previously failed orthodontic treatment attempts; and
Relapse presenting after active orthodontic treatment.
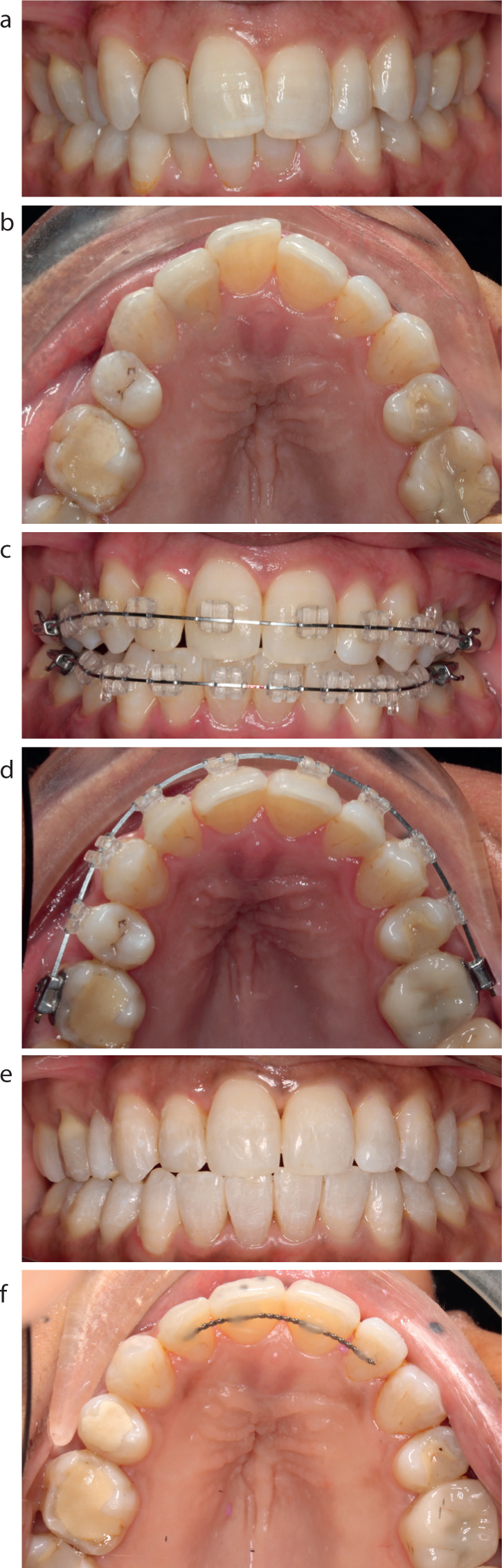
Often there is an autosuggestion that many adults do not want to wear conventional orthodontic appliances for several years; advanced restorative treatment modalities are seen as an alternative often to achieve quick results (Figure 1).
Figure 1.
(a, b) UR2 has been restored with a composite veneer to camouflage its misalignment within the maxillary arch. This restorative intervention was an unsatisfactory outcome for the patient. (c, d) A course of conventional orthodontic treatment using a fixed appliance commenced following removal of the veneer. (e, f) Post-orthodontic treatment outcome with higher patient satisfaction.
With the advent of short-term orthodontics (STO), no longer do adults have to wear fixed appliances for several years; STO can allegedly be completed in as little as 6 months.2
Therefore, this article will focus on:
Motivational factors for adult patients seeking orthodontic treatment;
Societal pressures compelling patients to seek orthodontic treatment;
Risks associated with STO; and
The precautions required in patient selection for STO.
What is short-term orthodontics?
Short-term orthodontics is a cosmetically motivated treatment, aiming to correct minor dental aesthetic anomalies, using controlled orthodontic forces over a relatively short period of time.3 STO appliances can be broadly categorized as fixed or removable (Table 1). As only certain features of an occlusion are corrected, STO is used to deliver what is referred to as Limited Treatment Orthodontics (LTO).4 These treatments appeal to adults as they tend to correct the rotations on anterior teeth alone, which are adult patients' main focus.
Fixed
Removable
Six Month Smiles®
Fastbraces®
QuickStraightTeethTM
Sectional lingual braces, eg IncognitoTM, STb Social 6TM
Inman Aligner®
Clear aligners, eg Invisalign®, ClearCorrectTM
Claims for STO
The following claims have been found whilst searching for STO benefits on the internet:5,7,8
STO is minimally invasive and can be relatively affordable;
STO is designed to minimize effects on a person's lifestyle;
Fast results are delivered as per patient expectations;
Appliances aim to be occult when eating, laughing and during social interaction; and
Comparisons have been drawn between STO versus conventional fixed orthodontic appliances; convoluting facts that STO is a conservative treatment modality when compared to conventional orthodontics.
Motivational factors for adult patients seeking orthodontic treatment
A questionnaire-based survey highlighted the popularity of private orthodontic treatments amongst adult patients.9 It revealed that, annually, approximately 28 private adult orthodontic cases were treated by a specialist orthodontist in primary care for every 21 NHS adult orthodontic cases within secondary care.9 An elevated social acceptance of orthodontic appliances, their improved appearance, and abundant appliance choices, are some of the reasons why more adults are undergoing treatment.10 A survey in 2009 found that the principal reasons for adults seeking orthodontic treatment were purely appearance-related such as: discoloured teeth; ‘crookedness’ of teeth; dental protrusion; tooth irregularity; and spaced arches.11 Often, patients relate the physical beauty to optimistic disposition in life.12 Treatment is more sought after by women, with the expectation that correcting dental irregularities will improve their facial appearance and quality of life.12,13
Societal pressures compelling patients to seek orthodontic treatment
Social stereotyping may be a key factor in determining why adults are concerned by minor dental irregularities.12,14 On some level, people are a product of their own environment. What we see in films, television, magazines, the internet, billboard advertising, etc can influence how we think and the choices we make.14 People are seeking perfection defined by the media, which unrealistically portrays celebrities as beautiful, wealthy, intelligent and socially adept. This can make people want to change themselves, including their physical appearance.12 Public and self-perception, that is, how others perceive us and how we perceive ourselves are greatly influenced by what society deems acceptable. Physical attractiveness, for example, is stereotyped by the clothes people wear, their hairstyles and dento-facial appearance.
Positive cultural association of ‘dental attractiveness’
The attractiveness theory suggests that a favourable personality is assigned to people who are perceived to be attractive.12 Research suggests physical appearance influences one's social actions and attitudes, and attractive people are preferred as potential friends.15 The attractiveness theory can be applied to dental aesthetics, where facial attractiveness has been associated with straight teeth.15 Some adults believe that dental aesthetic enhancement will positively influence social interaction and contribute to their general well-being.16 Interestingly, Mihalik et al found, in their study, that a sample of women with a mild Class II skeletal pattern, who received orthodontic camouflage treatment versus orthognathic surgery, both appeared to be satisfied with their treatment. Both groups rated aspects of their facial appearance positively.17 This suggests that even a mild skeletal II pattern is perceived to be attractive in women.
Negative cultural association of ‘dental weariness’
Several studies have shown that the presence of decay, the colour of teeth and a crowded arch can induce social judgements that can play a pronounced role in various social encounters.12,18,19 These include first impressions, employability, the ability to find a partner and interpersonal relationships.12,16 Research investigating the importance of dento-facial appearance on perceived social attractiveness found that young adult patients were seen as having lower intelligence and being less socially successful.16 Dental appearance can affect a person's facial body image perception which, in turn, reduces self-confidence, self-esteem and oral health-related quality of life (OHQoL).20 However, the severity of malalignment does not correlate with the psychosocial impact which it has on an individual.21 Someone with a severe malocclusion might not be concerned by it, thus having minimal effects on their OHQoL, whereas others with a minor irregularity may have a negative perception of their dental appearance, significantly affecting their psychosocial construct.20 Furthermore, clinicians judge a skeletal II profile more critically as compared to lay people, such as patients.22 Therefore, the motives behind adults seeking orthodontic treatment may be more complex than we believe.
Risks associated with STO
Root resorption
STO primarily involves orthodontic movements which are intrinsically unstable: incisor proclination, inter-canine width expansion or space closure by tipping movement alone.23 These unstable movements can result in increased stresses and strains in the periodontal ligament surrounding a tooth, which can ultimately lead to ligament death and root resorption.23 The risk of external resorption is higher if the orthodontic force applied is excessive.23
Relapse
With all types of orthodontic treatment, there is an element of risk of relapse attached; patients are advised to wear retainers to avoid this.2 In STO, however, the risk of relapse is thought to be much higher, due to the unstable tipping orthodontic tooth movements. Bodily movements and root torquing are considered to be more stable when compared to tipping movement. However, bodily tooth movements increase the duration of active orthodontic treatment considerably when compared to orthodontic tipping.24 Conversely, orthodontic tipping can be facilitated within months, thus reducing the overall treatment time.
Long-term retention is paramount to a successful treatment outcome. Several studies indicate that, without some form of retention, teeth will relapse; for patients wearing retainers for 1−2 years, 70% of them required retreatment 10 years later.25,26 Long-term retention can be achieved using removable vacuum-formed retainers (VFR) or bonded retainers. Research shows that both types of retainer are similar in the amount of relapse seen.27 Although it is presumed that all patients have the potential to relapse, patient compliance with long-term retainer use has been shown sometimes to be more demanding than treatment itself.28 Kacer et al found that patient compliance rate with removable retainers declined to 45% at the end of 2 years following orthodontic treatment.29 Within the first year of retention, some 27% (maxillary) and 22% (mandibular) of the VFR were lost and up to 31% (maxillary) and 49% (mandibular) were broken.23 Regarding bonded retainers, research has indicated that 58% of palatal bonded retainers fail between 8 and 42 months, with operator inexperience correlating with higher failure rates.6,30 GDPs involved in the prescription, placement and review of retainers should have further training so that patients are managed appropriately. A questionnaire-based audit found that GDPs are reluctant to prescribe, fit or review bonded retainers, with more than 72% wanting further training on the subject of retention.31 This illustrates the need for education on retention at both an undergraduate and postgraduate level.
Medico-legal issues
A poor final outcome can result in patients seeking re-treatment and settling for a compromised outcome. If this occurs, there are several issues to consider:23,32,33
A repeat course of orthodontic treatment might be offered;
During repeated orthodontic treatments the risk of root resorption is increased, where teeth are cyclically exposed to inflammation caused by orthodontic tooth movement;
Advanced restorative interventions to camouflage the relapsed misalignments might be proposed as a choice of treatment;
Ultimately, considerable amount of financial and treatment time reinvestment might be expected from a patient and these would inevitably deflate any patient's morale.
However, some patients may consider entering a re-treatment phase out of desperation. Logic suggests that not all these cases are referred to hospital service units and often enter the re-treatment phase privately.
Patient vulnerability
GDPs do not require any postgraduate qualifications to prescribe STO; they can simply attend a two-day short course provided by different commercial companies.3 This can result in gaps in the quality of a practitioner's knowledge and a false sense of reassurance that one is competent enough to deliver orthodontic treatment with STO for various cases.3 This may lead to poor quality delivery of care and potential harm towards patients. Primary care-givers should not enlist vulnerable patients into unnecessary treatment for financial gain. Marketing propaganda for different STO modalities lend themselves to patients by offering enhancement of the ‘social six’, the upper and lower anterior teeth, without correcting any posterior malocclusions.3 STO is advertised on many primary care practice websites across the UK, many of which do not outline the risks of STO.34 Furthermore, there are now services available offering orthodontic treatment without visiting a dentist. Patients can use a home impression-taking kit and take photos of their teeth which they send to a company. The company will fabricate aligners and send them to the ‘customer’ for immediate use.34 These ‘treatments’ are unsupervised and progress is not monitored.34 To determine whether someone is suitable for orthodontic treatment, seeing a qualified clinician for a detailed clinical examination is essential.34,35 Without this, patients who opt for ‘Do-it-yourself’ braces are at risk of causing permanent damage to their oral health, which may require further treatment as a consequence. The British Orthodontic Society strongly advises against such treatments.34
The precautions required in patient selection for STO: point-by-point
1. Consent
Before the commencement of any treatment, valid consent must be obtained. For consent to be valid, the following must be discussed with all patients before commencing STO: the type of treatment proposed, its intended short-, medium- and long-term benefits and potential risks/complications, other treatment options, potential costs of all treatment options and the consequences of not doing anything.36 Remember that STO is still orthodontic treatment and, as such, all the risks must be explained clearly in a way that patients can understand. Treatment risks include: pain/discomfort, demineralization, periodontal attachment loss, root resorption, loss of vitality, stained teeth and relapse.36,37,38 In addition, for the inherently unstable orthodontic alignments that short-term or limited objective orthodontic treatments produce, it is also strongly recommended that, as part of a patient's pre-treatment consent, he/she should be apprised of the long-term failure rates associated with fixed and removable retainers and therefore be advised of the potential for rapid relapse in such circumstances and, as such, come to appreciate the urgency of a retainer's repair or replacement, should the need arise.39
Patient expectations
Be wary of patients with unrealistic expectations. These may include an unreasonable timeframe for treatment completion and experiencing no pain or discomfort during treatment. One study involving adult patients undergoing orthodontic treatment found that pain was the main complaint during treatment, followed by treatment length.13 Other unachievable outcomes are the expectation of improvement in their skeletal pattern with mere orthodontic alignment, and guaranteeing success for life. If patient expectations cannot be managed, then they may be unsuitable for STO. Approximating treatment length will assist in treatment planning and the consent process, which in turn can allow patient expectations to be managed.4 Furthermore, another unknown contributor could be changing deadline for treatment completion with altered personal circumstances such as relocation of his/her work or family.
3. Compliance
Irregular attendees are not deemed suitable for STO, as treatment requires patients to attend numerous appointments over the course of several weeks-months. Not only can failure to attend affect treatment progress, but also a lack of compliance with the chosen treatment modality. For instance, removable retainers not being worn as advised. A detailed assessment of patient motivation and his/her social history should be carried out prior to beginning treatment. In addition to assessing treatment compliance, clinicians should explain to patients the importance of adhering to the post-treatment regimen to prevent relapse. One study has shown that, in comparison to vacuum-formed retainers, a bonded retainer is associated with more gingival inflammation.40 The same study suggested that wearing a bonded retainer does not adversely affect periodontal health.40 However, patients must be clearly informed that a bonded retainer is a plaque retentive factor and requires interdental cleaning aids regularly. Therefore, poor compliance to use of interdental cleaning aids can increase the risk of developing periodontal disease and caries.40
4. Active disease
STO is contra-indicated in patients with poor oral hygiene or active caries/periodontal disease. Suboptimal oral health in conjunction with the provision of STO can worsen one's oral health. STO should only be considered once disease has been stabilized. Whilst a reduced but healthy periodontal support is not a contra-indication to orthodontic treatment,41 active periodontal disease must be stabilized prior to commencing orthodontic treatment.42
5. Treatment complexity
Short-term orthodontics are primarily suitable to align teeth mildly out of position. STO cannot be used for correcting complex problems such as: management of impacted teeth, hypodontia, midline discrepancies, open bites, crossbites, Class II/III malocclusions or closing spacing greater than 2 mm. Often, such cases require multidisciplinary input from different specialties, such as orthodontics, restorative dentistry and oral surgery.43 However, while STO cannot be used successfully to correct the more complex malocclusions, increasingly, Invisalign® is being developed to tackle these types of irregularities, especially in the hands of qualified orthodontic specialists, albeit at levels of outcome that have yet to be validated, in comparison to those that can be achieved with full fixed appliances.44
Paediatric and adolescent patients
There is a danger that clinicians with limited training may lack the experience or clinical expertise to manage these patients appropriately. Referrals should be made by GDPs to their local orthodontist for an assessment, even when they are in doubt of the patient's suitability for orthodontic treatment based on the IOTN (Index of Orthodontic Treatment Need).45
Conclusion
The primary reason for adults seeking short-term orthodontic treatment is to improve their physical appearance. STO is a suitable option for correcting minimally malaligned teeth. However, an emphasis on lifelong retention is paramount to positive long-term outcomes.44 Furthermore, precautions must be taken when selecting patients for treatment. GDPs must recognize which patients are either not suitable for treatment or require assessment by a specialist orthodontist. Although orthodontics can improve oral health-related quality of life in adults, there are currently no published guidance documents on case selection for STO. In addition, GDPs attempting STO on cases outside the scope of their practice are increasing the potential risk of harm to both groups; the patients from ill-treatment and themselves through higher likelihood of litigation. Orthodontics is a dental specialty that requires further accredited postgraduate training. GDPs performing STO should receive more support from local orthodontists to ensure that treatment is carried out safely. Evidence-based guidelines provided by orthodontic professional bodies would be useful for GDPs who prescribe the majority of STO in the UK, to aid in recognizing which cases are within the scope of their practice.