Whaites E., 3rd edn. London: Elsevier (Churchill Livingstone);
Grossmann SM, Machado VC, Xavier GM, Moura MD, Gomez RS, Aguiar MCF Demographic profile of odontogenic and selected nonodontogenic cysts in a Brazilian population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 104:e35-41
Daley TD, Wysocki GP, Pringle GA. Relative incidence of odontogenic tumors and oral and jaw cysts in a Canadian population. Oral Surg Oral Med Oral Pathol. 1994; 77:276-280
Elliott KA, Franzese CB, Pitman KT. Diagnosis and surgical management of nasopalatine duct cysts. The Laryngoscope. 2004; 114:1336-1340
Swanson KS, Kaugars GE, Gunsolley JC. Nasopalatine duct cyst: an analysis of 334 cases. J Oral Maxillofac Surg. 1991; 49:268-271
Allard RHB, Van Der Kwast WAM, Van der Waal I. Nasopalatine duct cyst: review of the literature and report of 22 cases. Int J Oral Surg. 1981; 10:447-461
Bodin I, Isacsson G, Julin P. Cysts of the nasopalatine duct. Int J Oral Maxillofac Surg. 1986; 15:696-706
Escoda Francolí J, Almendros Marqués N, Berini Aytés L, Gay Escoda C. Nasopalatine duct cyst: report of 22 cases and review of the literature. Med Oral Patol Oral Cirugia Bucal. 2008; 13:E438-443
Dachi SF, Haley JV, Sanders JE. Standardization of a test for dental sensitivity to cold. Oral Surg Oral Med Oral Pathol. 1967; 24:687-692
Fulling HJ, Andreasen JO. Influence of maturation status and tooth type of permanent teeth upon electrometric and thermal pulp testing. Scand J Dent Res. 1976; 84:286-290
Mainkar A, Kim SG. Diagnostic accuracy of 5 dental pulp tests: a systematic review and meta-analysis. J Endod. 2018; 44:694-702
Fuss Z, Trowbridge H, Bender IB, Rickoff B, Sorin S. Assessment of reliability of electrical and thermal pulp testing agents. J Endodont. 1986; 12:301-305
Carrotte P. Endodontics: Part 2: Diagnosis and treatment planning. Br Dent J. 2004; 197:231-238
Estrela C, Bueno MR, Leles CR, Azevedo B, Azevedo JR. Accuracy of Cone Beam Computed Tomography and panoramic and periapical radiography for detection of apical periodontitis. J Endod. 2008; 34:273-279
Pauwels R, Beinsberger J, Collaert B, Theodorakou C, Rogers J, Walker A Effective dose range for dental cone beam computed tomography scanners. Eur J Radiol. 2012; 81:267-271
Hilfer PB, Bergeron BE, Ozgul ES, Wong DK. Misdiagnosis of a nasopalatine duct cyst: a case report. J Endod. 2013; 39:1185-1188
Wray D, Stenhouse D, Lee D, Clark AJE.London: Elsevier (Churchill Livingstone); 2003
Nasopalatine Cyst or Apical Pathology? A Diagnostic Dilemma and How to Manage It Marialena Cresta Robert Philpott Eleni Besi Dental Update 2024 47:2, 707-709.
Nasopalatine cysts (NPCs) present as maxillary midline radiolucencies and are the most common radiolucency of non-odontogenic origin. The proximity of these radiolucencies to the apical region of the maxillary anterior teeth may complicate diagnosis. We are presenting two cases of maxillary midline radiolucencies with a similar presentation but different diagnoses. Reaching a definitive diagnosis may be complicated, even when a detailed clinical examination has been carried out. The use of CBCT has been a valuable addition to the diagnostic armamentarium which can help clinicians reach more accurate diagnoses in such cases. A definitive diagnosis may be established following histopathological analysis, which is indicated in symptomatic cases.
CPD/Clinical Relevance: This article highlights the importance of careful assessment of apical radiolucencies associated with the maxillary midline, leading to the correct diagnoses and appropriate treatment planning.
Article
Marialena Cresta
Nasopalatine cysts (NPCs) arise from the epithelial remnants of Jacobson’s organ along the nasopalatine duct.1 NPCs are located in the midline of the anterior maxilla and may also be referred to as nasopalatine, incisive canal, median palatine, palatine papilla or median alveolar cysts. NPCs are the most common non-odontogenic cyst, found in 1−4% of the total population and present more commonly in males in the 4th decade.2,3,4
The cause of the epithelial remnant proliferation and cyst formation is not fully understood. It has been suggested that NPCs arise from the entrapment of epithelium during fusion of the embryological process. More recently, the theory most accepted is that NPCs originate from the presence of oronasal ducts in the incisive canal.5 The development of NPCs is stimulated by trauma, bacterial infections and mucous retention.2
NPCs present most frequently in the maxillary midline and have a round shape which, due to the superimposition of the nasal septum, may appear heart-shaped.
A retrospective cohort study that reviewed 334 NPC cases found that the mean radiographic diameter was 17.1 mm. The study concluded that there was no correlation between the radiographic size, patient age, presenting symptoms or type of epithelium. NPCs are often asymptomatic unless they become infected. In those cases, the clinical presentation may involve a painful swelling, more frequently palatally located, along with a salty discharge.1,6
The decision to treat NPCs surgically is based on the presence of clinical symptoms.7 The proximity of the lesion to the local neural anatomy, and the likelihood of the post-operative complications arising out of this, may also influence the decision-making. When a surgical procedure is considered along with the usual risks associated with all minor oral surgical procedures, the patient should be informed of a higher risk of temporary or permanent paraesthesia and neuropathic pain.8 Following surgical removal, recurrence is unlikely, however, there have been reported low recurrences of 2% over various time periods, ranging from 3 months to 6 years.6 Follow-up of those cases is therefore recommended.9
Case 1
A 53-year-old male, with a non-contributory medical history, was referred to the oral surgery department with a suspected cyst associated with the UL1. The symptoms began while the patient was on holiday with throbbing pain from the UL1, which resolved spontaneously. Root canal treatment of the UL1 was completed by the patient’s referring dentist and the patient was subsequently referred to the Oral Surgery Department at the Edinburgh Dental Institute.
Clinical and radiographic examination were carried out. As the patient was asymptomatic, a review was arranged 6 months following the completion of endodontic treatment (Figure 1). At the review appointment, the patient reported intermittent symptoms. Further radiograph examination revealed no changes in the size of the apical radiolucency (Figure 2).
Figure 1. Case 1: Radiograph taken on the initial consultation.Figure 2. Case 1: Radiograph taken at 6-month review appointment.
A CBCT was then requested in order to aid diagnosis and treatment planning. The scan showed an 8 mm diameter radiolucency located at the palatal region of UL1, UL2 roots, which was distinct from the apex of the UL1 (Figure 3). This additional information confirmed a nasopalatine cyst as being the most likely diagnosis. A surgical approach was adopted to enucleate the lesion and histopathological analysis confirmed the diagnosis of a NPC.
Figure 3. Case 1: Sagittal section of pre-operative CBCT scan.
Case 2
A 74-year-old male was referred to the Oral Surgery Department of Edinburgh Dental Institute due to the presence of a large radiolucency associated with the upper anterior region. The patient at that time was receiving treatment for prostate cancer. He presented with tenderness and swelling of the tissues associated with tooth UR1. Clinical examination revealed slight tenderness on palpation of the soft tissues apical to the UR1. The tooth was heavily restored and gave negative responses to pulp sensibility testing.
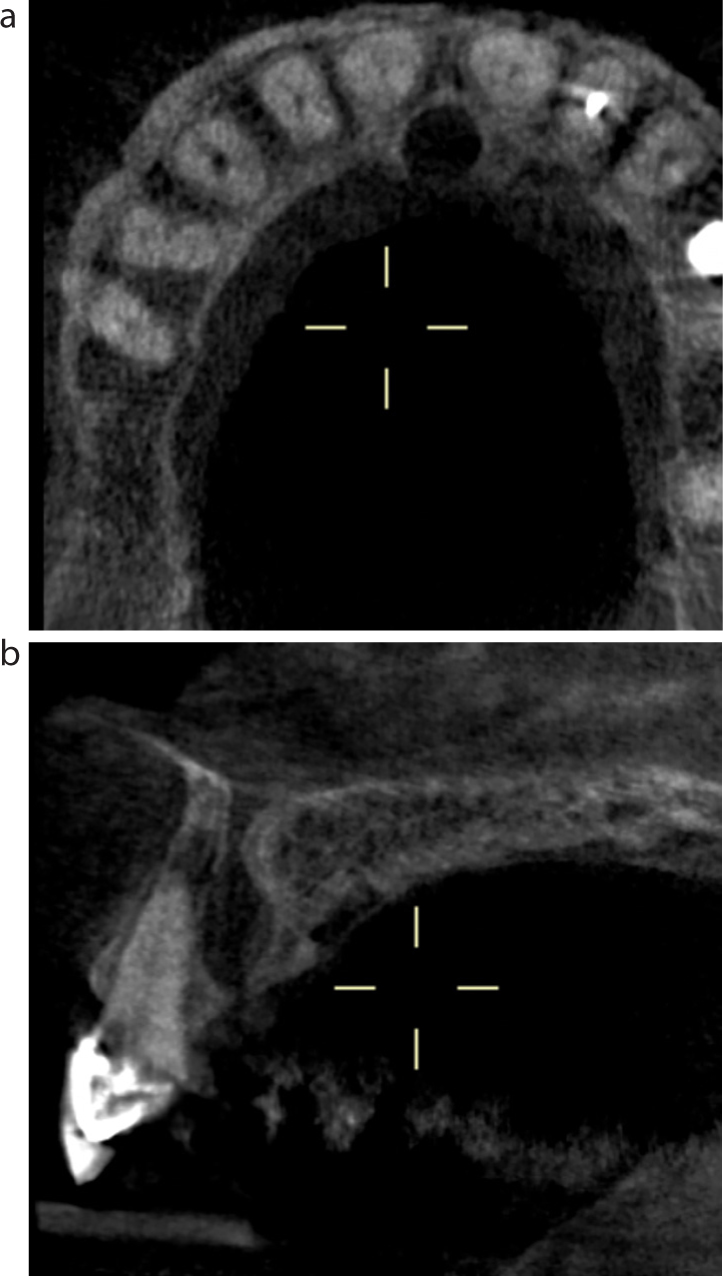
Radiographic examination revealed a well-defined radiolucency in the maxillary midline (Figure 4). Further imaging, in the form of Cone-Beam Computerized Tomography (CBCT), was carried out that revealed widening of the periodontal ligament of UR1, confirming that this tooth was the most likely source of the patient’s symptoms (Figure 5). The report added that the incisive canal appeared enlarged, measuring 8 mm medio-laterally, which may be suggestive of a nasopalatine duct cyst development.
Figure 4. Case 2: Radiograph taken at initial consultation.Figure 5. Case 2: (a, b) Axial and sagittal view of the CBCT scan.
A diagnosis of chronic apical periodontitis with a necrotic tooth UR1 was made. The patient was referred back to the care of the general dental practitioner for endodontic treatment of tooth UR1. Due to the absence of signs and symptoms suggestive of infection associated with the NPC, surgical intervention was not warranted. Further follow-up was arranged.
Discussion
Misdiagnosis of NPCs is possible owing to the anatomical appearance and superimposition of structures in the maxillary anterior region on periapical radiographs. The differential diagnoses most commonly considered are an enlarged nasopalatine duct and apical pathology associated with upper cental incisors. However, central giant cell granuloma and other maxillary cysts have also been recommended.9Table 1 describes the most common features of these lesions.
Differential Diagnosis of Midline Lesion
Key Frequent Features
Nasopalatine cyst
Palatine swelling with salty discharge
Positive sensibility testing
Midline well defined radiolucency
Heart-shaped
Enlarged nasopalatine foramen
No symptoms
Oval radiolucency
Well defined laterally
Less than 6 mm diameter
Apical periodontitis
Pain history
History relating to loss of vitality
Buccal swelling
Negative sensibility testing
Radiolucency continous with apices
Often, this can be incorrectly diagnosed as a periapical lesion associated with the upper central incisors and confusion can be created when the nasopalatine foramen is large.2 The normal appearance of the nasopalatine foramen is an oval radiolucency with well-defined borders laterally but not circumferentially. The features differentiating the lesion from the nasopalatine foramen would be the size, being larger than 6 mm, and the inverted teardrop shape which appears relatively more radiolucent.2
A thorough clinical examination to assess the presence of signs of infection or inflammation should be carried out. This should be supplemented with appropriate sensibility testing of the teeth in the region.
The major limitation of the sensibility testing is that information is provided regarding the neural response of the pulp and not the vascular supply. The responses are dichotomous, without giving information about the range of state of the pulp (normal, reversible pulpitis, irreversible pulpitis, partially necrotic pulp, necrotic pulp). Furthermore, these investigations are technique sensitive and this should be taken into account when interpreting the results. By assessing a tooth that the clinician expects to provide a normal response first, the range of responses for the patient can be appreciated. When using a cold test, a response within 5 seconds should be expected.
Clinicians should consider exploring two independent signs or symptoms, prior to reaching a diagnosis.10,11 A recent systematic review showed that the electric pulp test had high accuracy in testing vital teeth. Cold tests showed significantly higher sensitivity and the ability to detect the presence of disease, compared to electric pulp tests (EPTs).12 When available, the use of different investigations to assess the tooth’s neural response should be used in an attempt to gather as much diagnostic information as possible, prior to reaching a definitive diagnosis. However, in practice, cold testing is far more commonly used. Amongst the cold testing agents, the use of refrigerant agents (eg Dichlorodifluoromethane spray) was found most reliable compared to ethyl chloride owing to the greater temperature decrease (-20 to -50).13
Table 2 shows a comparison of the diagnostic accuracy of various pulp tests. Sensibility testing can be challenging when teeth are restored with either large direct or indirect restorations. An in vitro study showed greater temperature change with the application of CO2 snow when applied on porcelain fused to metal and all-ceramic crowns. An alternative technique would be to use the electric pulp tester on a probe that is placed beyond the crown margin so that it is in contact with the tooth, or the use of a special tip placed between the crown and the gingivae.14 Careful application of the tip should be carried out to avoid touching the gingival margin, which might result in false positive results.
Sensitivity
Specificity
Adjusted accuracy
Adjusted positive predictive value
Adjusted negative predictive value
Cold tests
0.87
0.84
0.84
0.81
0.87
EPT
0.72
0.93
0.82
0.89
0.80
Heat pulp testing
0.78
0.67
0.72
0.62
0.79
Laser Doppler flowmetry
0.98
0.95
0.97
0.94
1.00
Pulse oximetry
0.97
0.95
0.97
0.94
0.99
It has been suggested that the radiographic size of the lesion might be used as a guide for the differential diagnosis. The average diameter of the incisive foramen is approximately 3 mm and it has been recommended that lesions less than 6 mm should be regarded as normal anatomy.6 The limitations of radiography in the diagnosis of different types of apical pathosis is well documented.15 The angulation of the radiographic beam might distort the image and the lesion might have a decisive size. When using panoramic radiographs, magnification of the lesions should be taken into account.6
The relatively recent introduction of CBCT in the diagnostic armamentarium has assisted clinicians in reaching an accurate diagnosis. The primary advantage of this is related to the 3-dimensional nature of the imaging modality. However, the increase in effective dose to the patient must also be considered. There is a variety of field of view (FOV) CBCT machines available and the effective radiation dose may vary at a 20-fold range.16 Small FOV CBCT, less than 5 x 5 cm, result in a significantly reduced effective dose. However, clinicians should always justify the imaging chosen and select the view that reduces the radiation dose to ‘as low as reasonably practicable’ (ALARP). Table 3 shows a comparison of the effective radiation dose for different small volume CBCT in relation to panoramic radiographs and daily background radiation.
CBCT Unit
Technique
Effective Dose (μSv)
Panoramic Equivalent
No of Days of Annual per capita Background
Kodak 9000 3D
Anterior maxilla
5.3
0.4
0.6
3D Accuitomo
Anterior 4 x 4 cm
20
1.4
2.5
3D Accuitomo
Anterior 6 x 6 cm
43
3.1
5.2
Veraview
Anterior 4 x 4 cm
31
2.2
3.8
When the treatment of choice is a surgical approach, NPC should be enucleated. By removing the lesion without rupture of the cystic lining, the complete excision will more confidently be confirmed, although this may prove to be technically difficult. The surgical approach involves the elevation of a palatal full thickness flap, the extent of which depends on the size of the lesion. Following enucleation, it has been suggested to use a bone graft on the defect site, with a view to preserving the horizontal ridge.17 In cases of large lesions, a palatal plate can help prevent the development of a haematoma.18
Once the lesion is sent for histopathological analysis it is expected to confirm the presence of stratified squamous epithelium and ciliated columnar epithelium. Occasionally, mucous glands and neurovascular bundles may be present in the wall of the specimen.1
It is not recommended to marsupialize NPCs, as it will not allow complete bony infill.18 However, there have been a few recent case reports that have treated large NPCs with an endoscopic endonasal marsupialization. This approach offers the advantage of being less invasive compared to enucleation and the reports suggested satisfactory healing.19,20,21
Conclusion
These are two cases of the same pathology presenting differently clinically. The first resulted in the removal of the cyst and potentially unnecessary root canal treatment. In the second case, root canal treatment was delayed due to the concurrent presence of the cyst. It is very important for clinicians to understand fully the differential diagnosis and appreciate the limitations of the assessment tools used. NPCs can have a variety of presentations, both clinically and radiographically, and it is the correlation of all the findings that leads to an accurate diagnosis. When suspecting such lesions, referral to a specialist/tertiary setting is recommended.