Accidental Administration of Auto-Injectable Adrenaline into a Digit Christine Wanis Huda Jawad Richard J Moore Julie Burke Dental Update 2024 47:1, 707-709.
Authors
ChristineWanis
MFDS RCS(Ed), BDS Hons(Lond), PGCertDentEd
StR in Oral Surgery, Yorkshire and the Humber Deanery
General Dental Practitioners (GDPs) and Dental Care Professionals (DCPs) have a duty of care to ensure that patient safety is at the forefront of their clinical practice. Medical emergencies, although rare, can occur in the dental setting, and early, effective management of these emergencies can, not only save lives, but also improve long-term outcomes. A case is reported which highlights a safety incident involving accidental self-administration of an adrenaline auto-injector (AAI) into a digit during a medical emergencies training session. Consequently, the aim is to raise awareness of these unexpected safety incidences and propose a protocol for the treatment of such injuries.
CPD/Clinical Relevance: This paper highlights the importance of vigilance when undertaking a medical emergency training course, and the introduction of a new protocol to be used in cases of accidental AAI injury.
Article
Christine Wanis Huda Jawad
Medical emergency training in dentistry is an essential part of both undergraduate teaching, and a recommended postgraduate core subject in continued professional development (CPD) outlined by the General Dental Council (GDC).1 Anaphylactic reactions to drugs used in dentistry, or substances found in dental settings, are well reported.2 The most commonly described anaphylaxis in the dental setting is to antibiotics,3 however, chlorhexidine allergies, although rare, are on the rise,4 although the incidence is unknown.5 Its extensive use to reduce infection has potentially sensitized a small portion of patients, leading to life-threatening anaphylaxis on exposure.6 Owing to the possibility of anaphylaxis in the dental setting, it is imperative that dental care providers should have up-to-date training and should feel confident in the use of AAIs, when needed.
Adrenaline is the gold standard for the management of anaphylaxis7 and the prescription of adrenaline auto-injectors (AAIs) is commonplace across the world. The European Academy of Allergy and Clinical Immunology released guidelines in 2014 for prescribing AAI.8 Although clinicians are advised to deliver an intramuscular dose of 0.5 mg of 1:1000 for adults, the EpiPen® delivers a lower single dose of 0.3 mg of 1:1000. The doses differ with age for those under 16 years of age. This allows patients to manage their reactions immediately and then summon medical assistance. It also allows healthcare professionals in remote locations, or those in non-acute medical environments, to have pre-loaded syringes to manage medical emergencies appropriately. Drawing up adrenaline in a medical emergency situation in the correct dose using a hypodermic needle and syringe is thought to be more difficult than using an auto-injector, potentially risking spillage of the drug, incorrect dose administration, self-injury due to breaking vials,9 and therefore potential contamination of the drug. This is thought to be even more likely for DPs and DCPs, who are unlikely to be drawing up medications from glass vials on a regular basis unless treating patients under intravenous sedation.
The use of pre-filled syringes and AAIs is encouraged for use by dental practices, as advised by the GDC and Resuscitation Council, UK.10 However, a recent reminder (9 October 2018) to healthcare professionals from the Chief Dental Officer, England, states that, due to shortage of AAIs and the need to keep them within the community setting, DCPs are asked to replace AAIs with ampoules when renewing adrenaline in their medical emergency kits.11
GDPs and DCPs are required to undergo training in the use of AAI pens, but should also be competent to draw up and administer 0.5 mL of 1:1000 adrenaline from ampoules with a normal syringe and needle for intra-muscular administration. The British National Formularly12 advises that half doses of adrenaline may be safer for patients who are taking amitriptyline, imipramine and beta-blockers.
Owing to the fact that anaphylaxis is rare in the dental setting, GDPs may become de-skilled in the use and administration of AAIs. The Department of Health notes that ‘wrongly prepared high risk injectables’ is a ‘Never Event’.13 Consequently, it is essential during medical emergency training that dental teams are not only taught on the correct preparation of intra-muscular adrenaline, but also in the correct use of pre-prepared adrenaline, such as the EpiPen®.
A case of inadvertent self-administration of AAI into the thumb, whilst on a postgraduate medical emergencies training course, is reported. This was considered a ‘Serious Incident’ (SI), and consequently the trainers and educators should be mindful that such SIs may occur during training sessions, and therefore should be trained in managing them. At present, there are no guidelines regarding this, and it is suggested that this should be taken into consideration when developing medical emergency training courses.
Case report
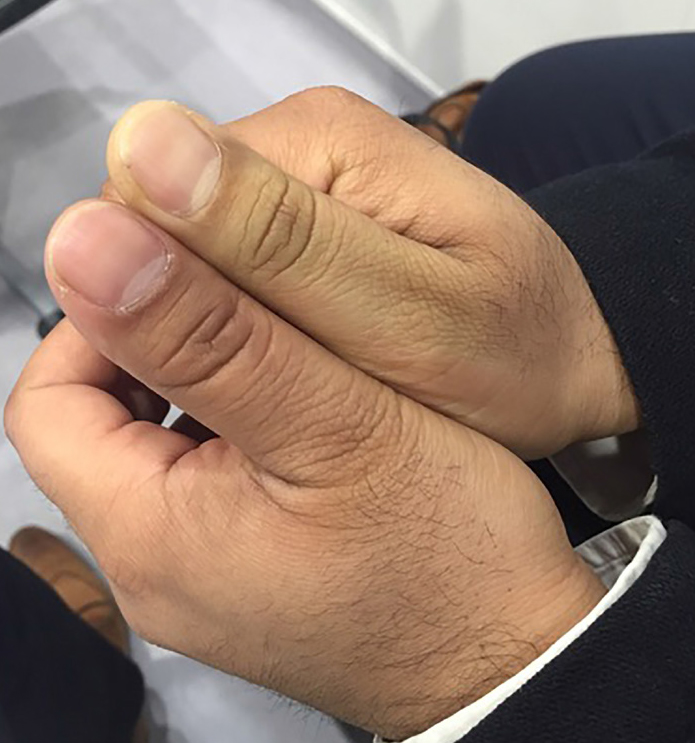
A 36-year-old male, who was otherwise fit and well, managed to discharge the EpiPen® into his right thumb whilst undergoing training in anaphylaxis. He immediately informed the trainer of the incident. Figure 1 shows the right thumb was pale compared to the left non-injured thumb. Initial examination revealed no evidence of capillary refill, the digit was insensate. He was advised to seek urgent care at the nearest Emergency Department (ED). He was seen and, after some deliberation and searching of the internet by ED staff, phentolamine, a reversible alpha-adrenergic antagonist which reverses the effects of adrenaline, was administered into the digit, which proved effective.
Figure 1. Delegate's right thumb minutes after inadvertently administering AAI into it.
Within a few hours the main symptoms resolved but, for a few days afterwards, he had altered sensation in the thumb, causing some discomfort. The symptoms after three months have completely resolved and there appears to be no long-lasting or permanent effects.
Discussion
The first reported cases of injection of adrenaline into a digit was by Jordan in 1969,14 where a dental assistant deliberately injected adrenaline into her finger to stop bleeding from a laceration. She developed blanched cold digit. Two hours afterwards, she immersed it in warm water, but this had no effect. Amyl-nitrite inhalations were attempted but to no avail but, when 5 ml of phentolamine was injected circumferentially around the finger, there was instant return of spurting arterial blood from the original injury.
Anecdotally, Denkler reported a case of digital necrosis after adrenaline-containing local anaesthetics, although most of these relate to times when the concentration of adrenaline was unpredictable.15 It is still taught that adrenaline is not safe to be used with local anaesthetics in peripheries such as digits, nose and ears due to the vasoconstrictive effect of the adrenaline and the risk of vascular insufficiency or, at worst, necrosis of the structure. However, there are reports showing that its use in surgery of the digits is safe and effective.16
There have been reports of a variety of treatment options which include administration of nitroglycerine (a potent vasodilator), topically and systemically, infiltration of phentolamine locally and regionally, proximal intra-arterial injection, digital sympathectomy via a digital block, and systemic or topical calcium channel blockers.17 Phentolamine administered topically in a rat tail arterial model has resulted in complete relief of adrenaline-induced vasospasm.18 It is a short-acting reversible competitive inhibitor of α1 and α2 adrenergic receptors. The side-effects of systemic administration of phentolamine include hypotension, reflex tachycardia, arrhythmias and cardiac ischaemia.19 Delivery of the drug through local or regional infiltration at low doses reduces the risk of these potentially significant side-effects. Phentolamine appears to be the most common treatment of choice for the accidental injection of adrenaline. It is recommended, although not licensed, to infiltrate locally 2–2.5 mg phentolamine mesylate at the puncture site as soon as possible. Small volumes should be used, for example 1–2 mLs, however, due to its short half-life, the treatment may need to be repeated. Resolution of the signs and symptoms usually occurs within 60 minutes.
The profession of this patient may have swayed the attending emergency doctor actively to treat him, rather than manage this conservatively, as the low risk of digit necrosis could impact significantly on the patient's profession. On reviewing the literature, there appear to be no case reports of confirmed digit necrosis, irrespective of active or conservative management.
Summary
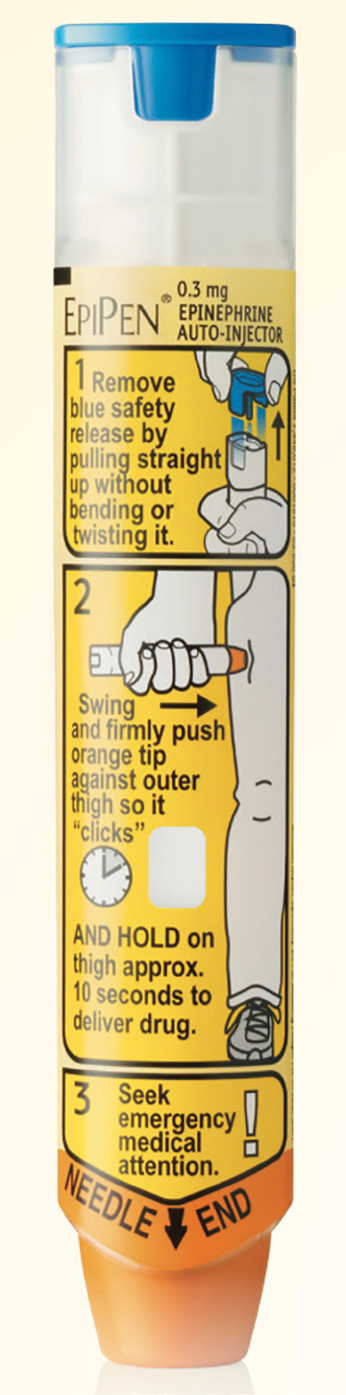
It has become evident from the literature,20 and is also highlighted in this case, that the cause of potential accidental self-injection is in the incorrect holding of the auto-injector pens. They should be held with a fist grip, as in Figure 2, so that, when removing the end, one's thumb is away from the dispensing end, and hence the discharging of the needle is into the patient, and not into the clinician's thumb pad.
Figure 2. Correct handling of AAI device.
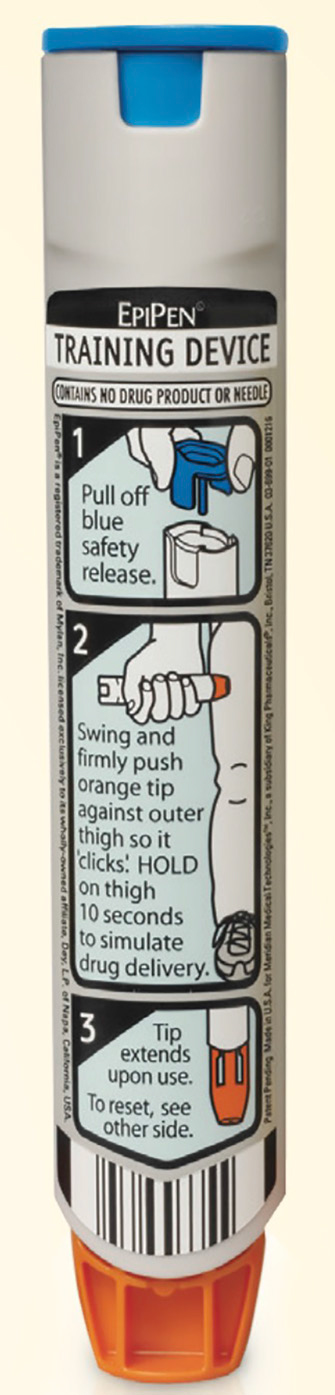
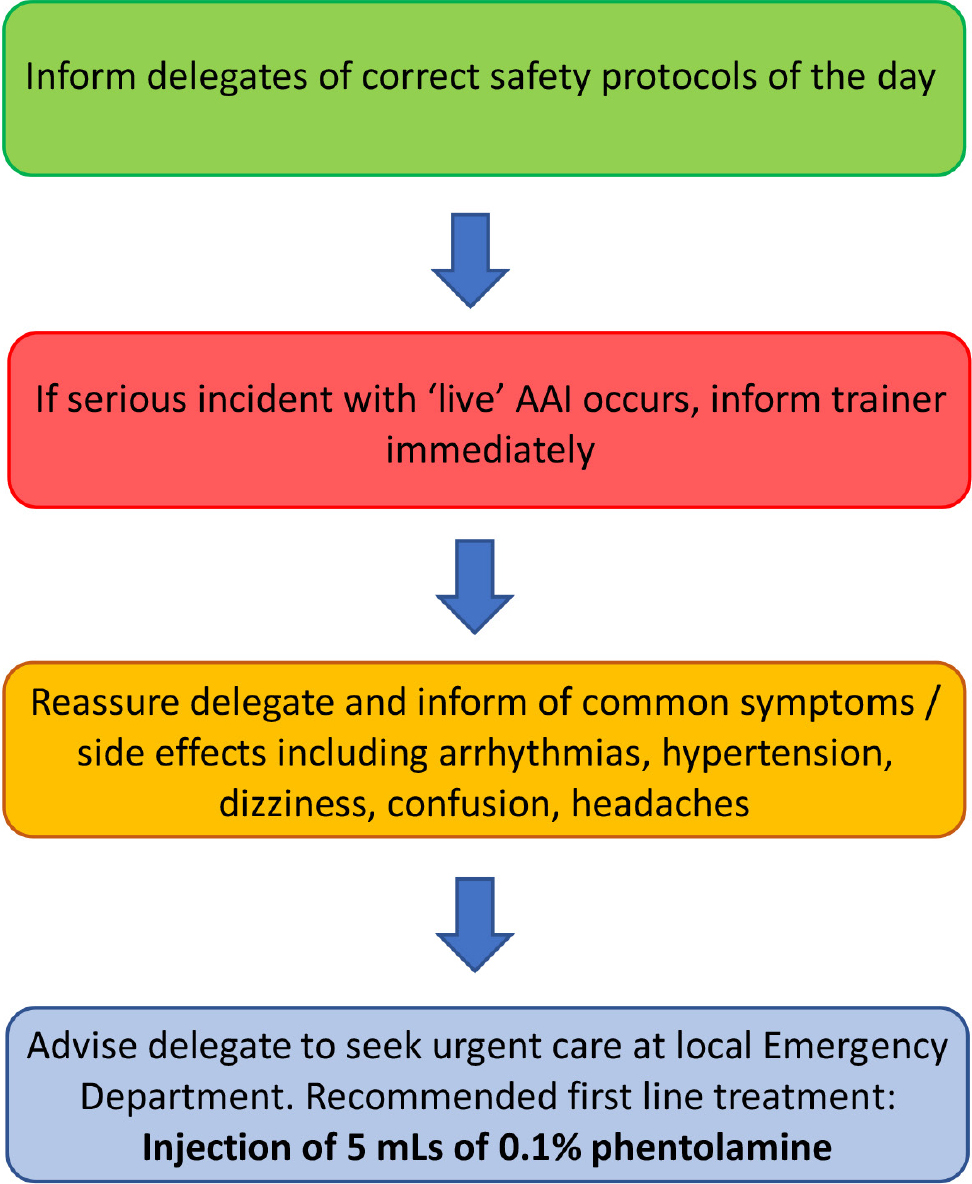
This case reinforces the need for careful instruction when teaching with ‘live’ equipment, and the need for an awareness of the risks associated with such training, highlighting the need for protocols for treatment. Furthermore, one should consider the use of an AAI training device (Figure 3), which contains no medicine, and no needle, when training for medical emergencies. We propose a simple-to-follow safety protocol flowchart to be used for any accidental AAI injury in medical education training (Figure 4).
Figure 3. Example of a training AAI device.Figure 4. Safety protocol flowchart for accidental AAI injury in medical emergency training.