Diagnosis and management of chronic osteomyelitis and cemento-osseous dysplasia of the mandible Arifa Akram Tajinder Lidhar Katy Marie Valentine Roger Webb Dental Update 2024 46:11, 707-709.
Chronic osteomyelitis is a severe and persistent infection of the bone including the bone marrow. Cemento-osseous dysplasias are a group of conditions arising from the periodontal ligament tissue and are categorized into peri-apical, focal and florid. A case of a patient with buccal and submandibular swelling associated with a discharging sinus between LR45 was presented. History, examination and investigations confirmed a diagnosis of chronic osteomyelitis and an incidental finding of florid cemento-osseous dysplasia of the mandible. The patient's treatment is discussed within the context of important clinical considerations required in managing these patients.
CPD/Clinical Relevance: It is pertinent for a general practitioner to be aware of signs and symptoms associated with chronic osteomyelitis and understand the management options.
Article
Arifa Akram
Case report
A 67-year-old fit and well female of Nigerian origin was referred to the Accident and Emergency department by her general dental practitioner (GDP) with a one-week history of right-sided buccal and submandibular swelling. The patient complained of right-sided jaw pain, had mild trismus and an intra-oral discharging sinus in the buccal alveolus between the LR45. Furthermore, her dental history revealed that she had two dental extractions carried out in this sextant within the last year. An orthopantomogram (OPG) (Figure 1) and CT scan (Figure 2) demonstrated extensive erosion of the body of the mandible from the LR4 to LR6 region, which was predominantly lytic; reactive sclerosis of the adjacent bone and dense irregular bone fragments within the lytic areas, resembling sequestrum, was also noted. An incidental finding of dense sclerotic regions associated with the roots of these teeth, particularly localized to the lower left mandible and maxilla, was noted, showing features consistent with florid cemento-osseous dysplasia (FCOD). After discussion with the patient, surgical debridement and sequestrectomy of the right hemi-mandible were performed and specimens collected were sent for histological/microbiology examination.
Figure 1. OPG showing radiolucent areas and radio-opaque involucrum of the lower right body of the mandible. Note the dense sclerotic regions associated with the roots of the teeth on the lower left mandible.Figure 2. CT mandible showing extensive lytic areas extending from LR4 to LR6. Sequestra-dense bone within these lytic regions was also noted.
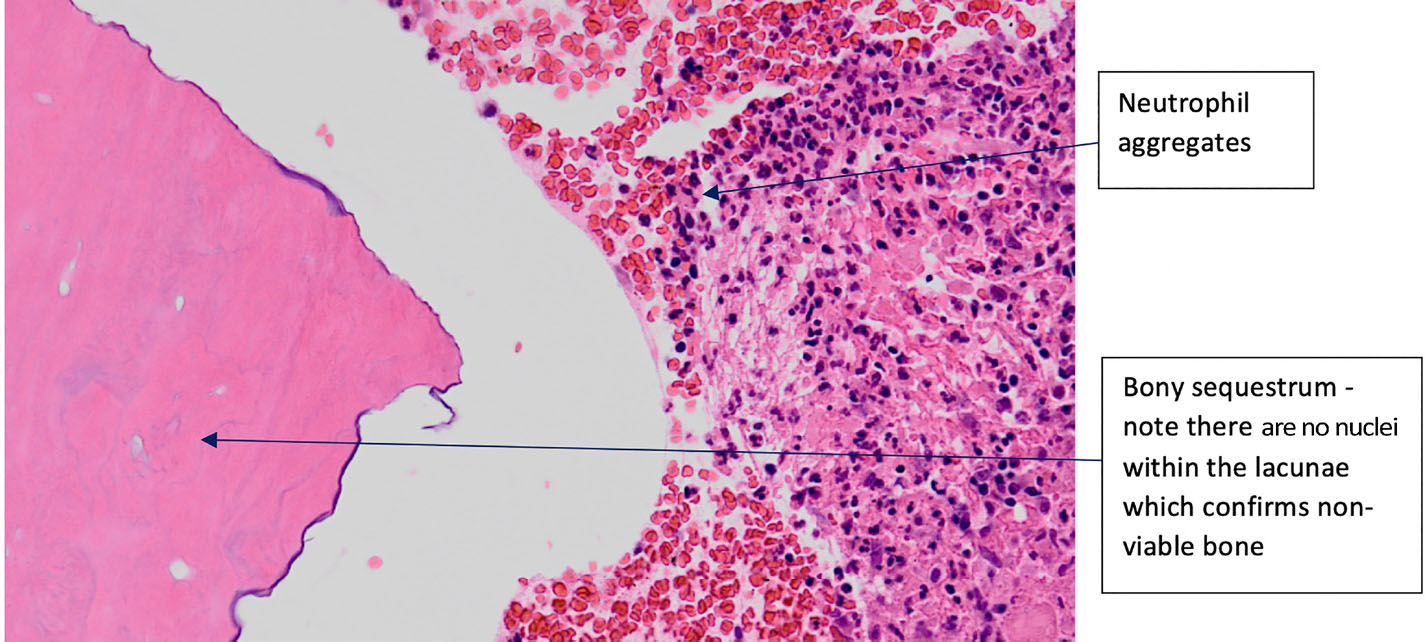
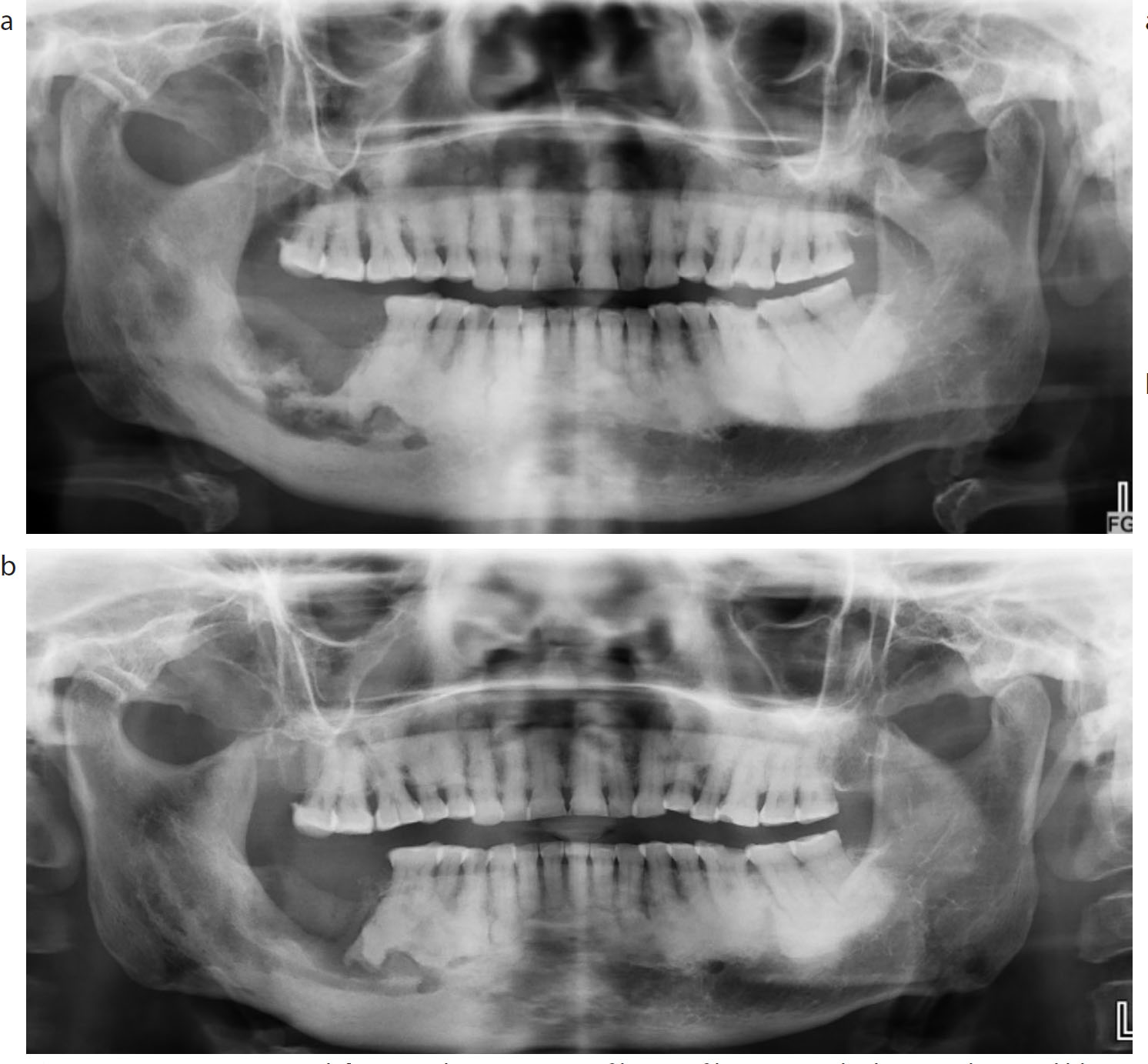
Hard and soft tissue histological findings confirmed inflamed granulation tissue of the right mandible and the presence of dead lamellar bone with a moth-eaten appearance (Figure 3). Microbiology results showed growth of coliforms and the patient was started on a 6-week course of Co-trimoxazole. Regular outpatient consultations showed an uncomplicated recovery with a healed sinus and no symptoms. Sequential orthopantomograms confirmed signs of bony infiltration when compared to previous radiographs (Figure 4).
Figure 3. Histology slide of bone and soft tissue right mandible. Hard tissue sections show dead lamellar bone with a moth-eaten appearance, together with neutrophilic aggregates and bacteria present at the surface. The features seen are of bony sequestrum.Figure 4. OPGs (a) 2016 and (b) 2017 showing signs of bony infiltration on the lower right mandible.
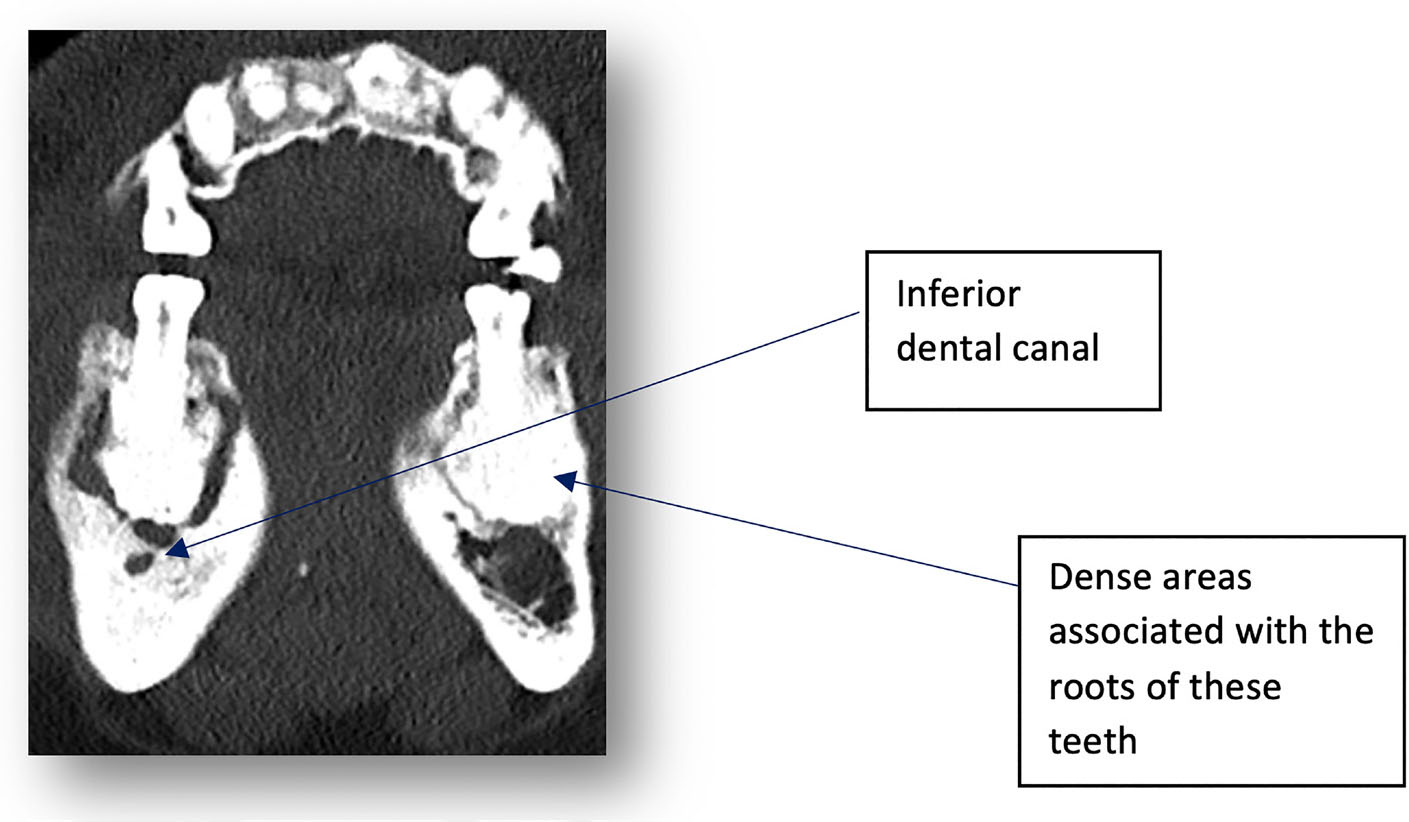
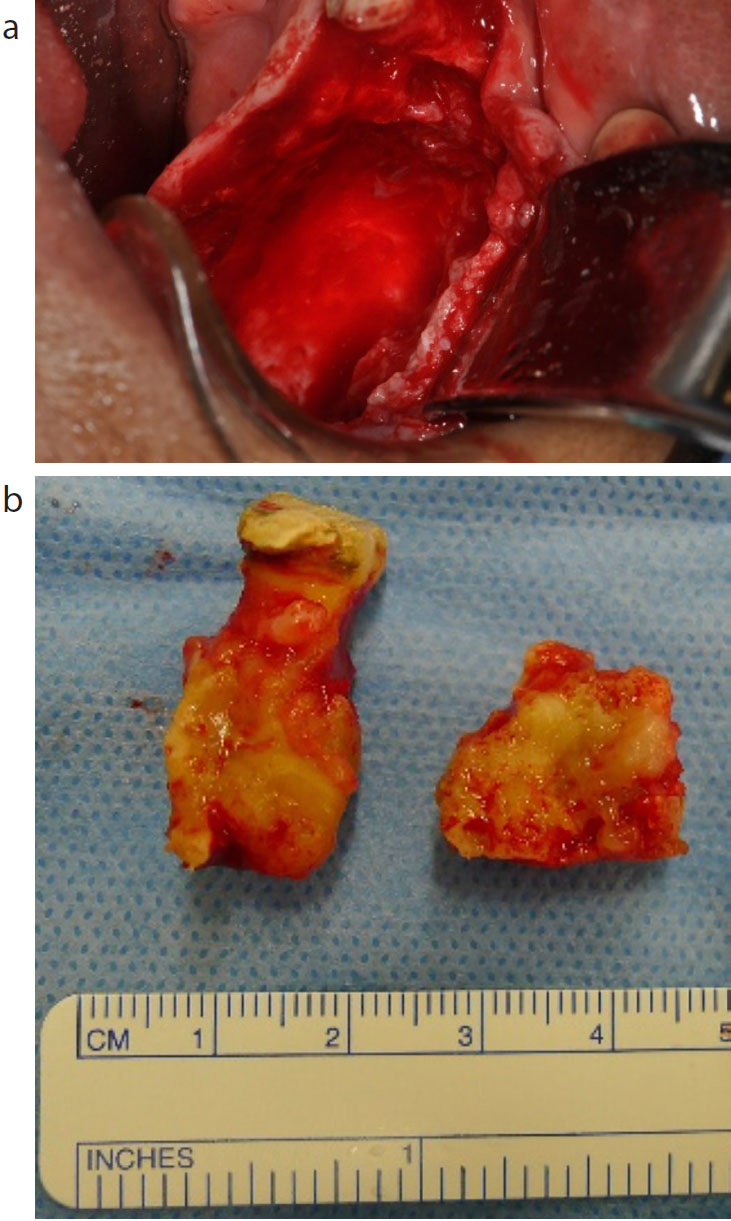
Over the course of the following year, the patient presented with similar symptoms and another sinus was found adjacent to the LR3. A CT scan of the mandible revealed ongoing infection. An interesting finding was the close approximation of the lytic regions in relation to the inferior dental canal (Figure 5); the patient's inferior dental nerve function remained intact throughout all presentations. A diagnosis of ongoing chronic osteomyelitis was confirmed, and the patient was taken to theatre for further debridement plus dental extractions of LR3456 (Figure 6), followed by an extended course of oral antibiotics. Outpatient consultations to date have demonstrated uncomplicated resolution with no return of signs or symptoms.
Figure 5. CT mandible clearly outlining the close approximation of the inferior dental canal to the lytic areas. Also note the dense regions associated with the roots on the lower left.Figure 6. (a, b) Intra-operative views: (a) showing extensive debridement and removal of sequestra of right body of mandible; (b) showing a sample of removed teeth plus sequestrum. Note the cemento-osseous sequestrum is walled-off by inflammatory soft tissue which, when curetted, leaves a smooth bony cavity.
Discussion
Osteomyelitis is inflammation of the bone which initiates in the medullary cavity and extends to the periosteum; it can present as localized jaw pain, swelling, purulent discharge, unhealed soft tissue in the oral cavity, paraesthesia of the affected side and pathological fractures.1
Acute osteomyelitis occurs up to one month after the onset of symptoms, whereas chronic osteomyelitis is present for a minimum of one month.2 Primary chronic osteomyelitis (PCO), termed Garre's osteomyelitis, is defined as non-suppurative osteomyelitis and usually arises in children and adolescents. Secondary chronic osteomyelitis (SCO) has an infectious aetiology and is associated with fistula, abscess and sequestra formation.2
Chronic osteomyelitis primarily has a microbiological cause which can be in the form of trauma, long-standing dental infection and post-extraction complications.1 The aetiology in our case is likely to be a consequence following dental extractions. Chronic osteomyelitis is also commonly found in individuals from developing countries due to an increased prevalence in conditions which increase the risk of infection and adversely inhibit/alter the healing process. These include malnutrition, anaemia and malaria.3 It is rare to find this condition in developed countries, particularly in a healthy individual. However, individuals on bisphosphonates and those who are immunocompromised are more susceptible to these pathologies.
Radiologically, osteomyelitis will show regions of bone destruction and sequestrum formation. The presence of sequestra and laminations of periosteal new bone are key radiological features of osteomyelitis; however, positive radiographic findings are often absent in an acute setting.1 A diagnosis is achieved by combining clinical, radiological, histological and microbiological findings. Histopathology usually demonstrates chronic inflammatory cells, increased osteoblasts, thickened bony trabecula and fibrous marrow replacement.1 In this patient, hard and soft tissue findings confirmed bony sequestra and granulation tissue with no evidence of dysplasia or malignancy.
The treatment of choice for chronic osteomyelitis of the mandible involves surgical debridement of non-vital bone/necrotic tissue followed by prolonged antimicrobial therapy based on microbiology sensitivity results. Radical surgery is key in the success of treatment as the retention of devitalized teeth can be a cause of ongoing signs/symptoms.4
Florid cemento-osseous dysplasia (FCOD) is a rare benign condition affecting two or more quadrants of the maxilla/mandible and is often bilateral. It is characterized by replacement of normal trabecular bone with osseous tissue and dense acellular cementum and arises from a spectrum of non-neoplastic fibro-osseous lesions of the jaws known an cementoosseous dysplasias (CODs).5 These areas are usually asymptomatic in the absence of infection and present as non-expansile masses that surround the root apices of vital teeth, as well as edentulous regions of the jaw.5 GDPs should ensure that they are familiar with this entity to prevent misdiagnosis and inappropriate intervention.
Florid cemento-osseous dysplasia and chronic osteomyelitis are two independent conditions. However, studies6,7 have shown that individuals with FCOD are at increased risk of chronic osteomyelitis. A study looked at individuals with FCOD who developed chronic osteomyelitis after surgery. Of individuals with FCOD who required dental extraction, 28% went on to develop chronic osteomyelitis.7 This is probably reflective of reduced local blood supply to the jaw bones, subsequently decreasing the bone's ability to counter infection. This emphasizes the need for prevention amongst GDPs, particularly in individuals with FCOD to reduce the need for dental extractions.
Conclusion
This case highlights the signs/symptoms, diagnosis and subsequent management of patients presenting with chronic osteomyelitis alongside co-existing cemento-osseous dysplasia. Before dental extractions, GDPs should risk assess patients based on their age, gender, ethnicity and medical history to ascertain the likelihood of post-extraction osteomyelitis, as well as other complications. High risk cases should be reviewed both clinically and radiologically after dental extractions to identify signs of acute/chronic osteomyelitis.
Signs of osteomyelitis warrants a referral to hospital/specialist for further management. The case highlights the pertinence of a multidisciplinary team to manage these cases successfully; microbiologists, histopathologists and radiologists are crucial to aid in the diagnosis of the condition, whilst the surgical team plays a key role in the surgical debridement of the necrotic bone. The input of each team assists in successfully managing a condition which can present a challenge to treat at times and warrants surgical debridement and extended courses of long-term antibiotics guided by a microbiologist.
Lastly, this case reinforces the importance of GDPs to have an understanding of benign fibro-osseous lesions such as cemento-osseous dysplasia. Asymptomatic cemento-osseous dysplasia lesions are routinely found during radiological examinations. However, these lesions present as radiolucent areas during early stages and progressively become radio-opaque due to the increase in mineral content. Depending on the stage of these lesions, the list of differential diagnoses can be extensive. Therefore, GDPs should consider the patient's age, gender, ethnicity, presenting complaint, clinical and radiological features very carefully before arriving at a definitive diagnosis, as a misdiagnosis can result in endodontic treatment, apicectomy and even exodontia, whereas asymptomatic cemento-osseous dysplasia does not require surgical intervention and requires long-term radiological follow-up.