Head and neck cancer part 3: dental management Stephanie Hackett Oliver Jones Despoina Chatzistavrianou David Newsum Dental Update 2024 46:11, 707-709.
Specialist in Prosthodontics, Specialty Registrar in Restorative Dentistry, Birmingham Dental Hospital and University of Birmingham School of Dentistry, Birmingham Community Healthcare NHS Trust, Birmingham, UK
Consultant in Restorative Dentistry, BDS, MFD RCS, MSc, MRCPS, MRD RCSEd, FDS(Rest Dent) RCSEd, Birmingham Dental Hospital and School of Dentistry, Birmingham Community Healthcare NHS Foundation Trust, Birmingham, UK
This is the third and final paper in the series. Oral and dental complications of head and neck cancers, and the associated treatments, can be devastating to patients. General dental practitioners are likely to encounter affected patients at various points along their treatment journey, which may involve the management of treatment side-effects or facilitating the post-treatment rehabilitation. This paper will discuss accepted preventive regimens for patients, management of treatment side-effects and specific cases of restorative rehabilitation post-treatment, highlighting the levels of treatment that can usually be provided in primary and secondary care settings.
CPD/Clinical Relevance: This paper aims to provide the reader with knowledge and confidence to manage the dental needs of head and neck cancer patients and post-treatment side-effects.
Article
Stephanie Hackett
Management of treatment side-effects
Head and neck cancer can result in significant short- and long-term complications which can affect function, aesthetics and social wellbeing. As discussed in the previous paper in this series, there are short- and long-term side-effects associated with surgery, radiotherapy and chemotherapy. Table 1 provides an overview of common side-effects and management techniques. Clinicians can utilize this advice to help relieve patients of oral mucositis, infections, trismus, xerostomia and caries.
Oral Mucositis
Local measures:
Adjust sharp teeth/restorations
Ensure dentures are kept clean and well adapted to tissues. Instruct patients not to wear them at night and during radiotherapy treatment
If brushing becomes very painful a very soft brush (eg TePe Special Care Toothbrush™ can be substituted. Normal brushing should resume at the earliest opportunity1
Ice can be used to relieve the pain of mucositis
Medication:
Benzydamine mouthwash has been recommended for those patients receiving moderate radiation without concomitant chemotherapy2
Fungal Infections
Topical agents:
Nystatin sugar-free oral suspension 100,000 units per ml four times daily for at least 7 days and 48 hours after resolution
Note: Compliance may be poor due to unpleasant taste
Miconazole oral gel 24 mg/ml 10 ml applied four times daily continued for 48 hours after resolution is an alternative
Chlorhexidine gluconate has antifungal and antibacterial properties in addition to antiplaque effects3,4
Note: its value is still unconfirmed2
Systemic agents:Systemic agents have more consistent efficacy
Fluconazole is recommended for moderate to severe oropharyngeal candidiasis or unresponsive infection – 50 mg capsules/suspension daily 7–14 days5
General Dental Practitioners (GDPs) should be aware of the importance of effective preventive regimens for head and neck cancer patients in order to assist in the holistic management alongside secondary care teams. The side-effects of treatment can place patients at lifelong high risk of dental disease and they should be managed accordingly, with full guidance taken from Delivering Better Oral Health.7 An individualized preventive regimen should also be implemented with advice taken from the lead Restorative Dentist in the multidisciplinary team (MDT). Recall intervals should be reduced to 3–4 monthly in line with NICE recall guidance.10
Restorative management in primary care
Following completion of treatment and rehabilitation for head and neck cancer, patient's care may be transferred to the GDP for long-term maintenance and review. Others may be placed under shared care between the GDP and Restorative specialist team during their rehabilitative treatment. GDPs are responsible for the management of primary disease within their scope of clinical competence and should monitor for recurrence of disease.6 Head and neck cancer patients should be treated carefully after treatment with respect to their general dental management and it is essential for dentists to recognize which dental treatments can be provided effectively and safely in primary care. In the authors' experience, restorative, oral surgery and maxillofacial colleagues will readily provide advice to GDPs when required. Individualized treatment plans will be provided to GDPs for prevention and routine care, such as fillings and extractions, from the MDT pre-treatment dental assessment clinic. Teeth of poor prognosis which are located in the radiotherapy field are often extracted in the local oral surgery department to ensure timely, atraumatic treatment. Post-treatment extractions in the radiotherapy field generally require referral to the local oral and maxillofacial surgery unit. However, extractions of teeth that are not in the radiotherapy field may be more suitably provided in primary care and this is often at the request of the assessing Restorative Dentist. Clarification of the radiotherapy fields should be sought from the Head and Neck service beforehand.
The use of remineralizing toothpastes, such as GC Tooth Mousse®, have been shown to have added benefit in prevention of root caries in patients who have received head and neck radiotherapy, by providing surplus calcium and phosphate ions to the tooth surface, which are often dimished in patients with reduced saliva flow.8
Fluoride prescriptions and saliva substitutes should be prescribed on a long-term basis to dentate patients as indicated in Table 1. Fluoride trays (Figure 1) may be of benefit to provide long-duration application of high dose fluoride to compromised teeth.
Figure 1. Fluoride trays to aid in the prevention of post-radiotherapy dental caries.
Consideration of the patient's physical restrictions is paramount when providing care in primary and secondary settings. Patients may have remarkable trismus or altered anatomy which may make providing routine treatment more difficult. Dentists are to be reassured that the indications and techniques required for providing the following routine care remain largely the same as for a healthy patient:
Scale and polish;
Root surface debridement (seek advice from Oral and Maxillofacial Surgery/Restorative Consultant);
Impressions for fluoride trays, mouthguards and simple removable/fixed prostheses;
Direct restorations;
Simple single unit indirect restorations (not implant-supported);
Dentures (if not already provided by the Restorative Team in secondary care);
Endodontic treatment;
Extractions outside the primary beam of radiotherapy and within scope of practice.
Attempts should be made to retain teeth which have previously been in the primary beam of radiotherapy rather than performing extractions, to reduce the risk of developing osteoradionecrosis of the jaws.
Patients requiring the following procedures should be referred to and managed by the local secondary care Restorative or Oral Surgery Department:
Minor oral surgical procedures;
Surgical periodontal procedures;
Implants;
Extraction of teeth in the radiotherapy field;
Complex multiple-unit indirect restorations;
Removable prostheses with obturator components or to restore large hard and soft tissue defects.
Restorative rehabilitation in secondary care
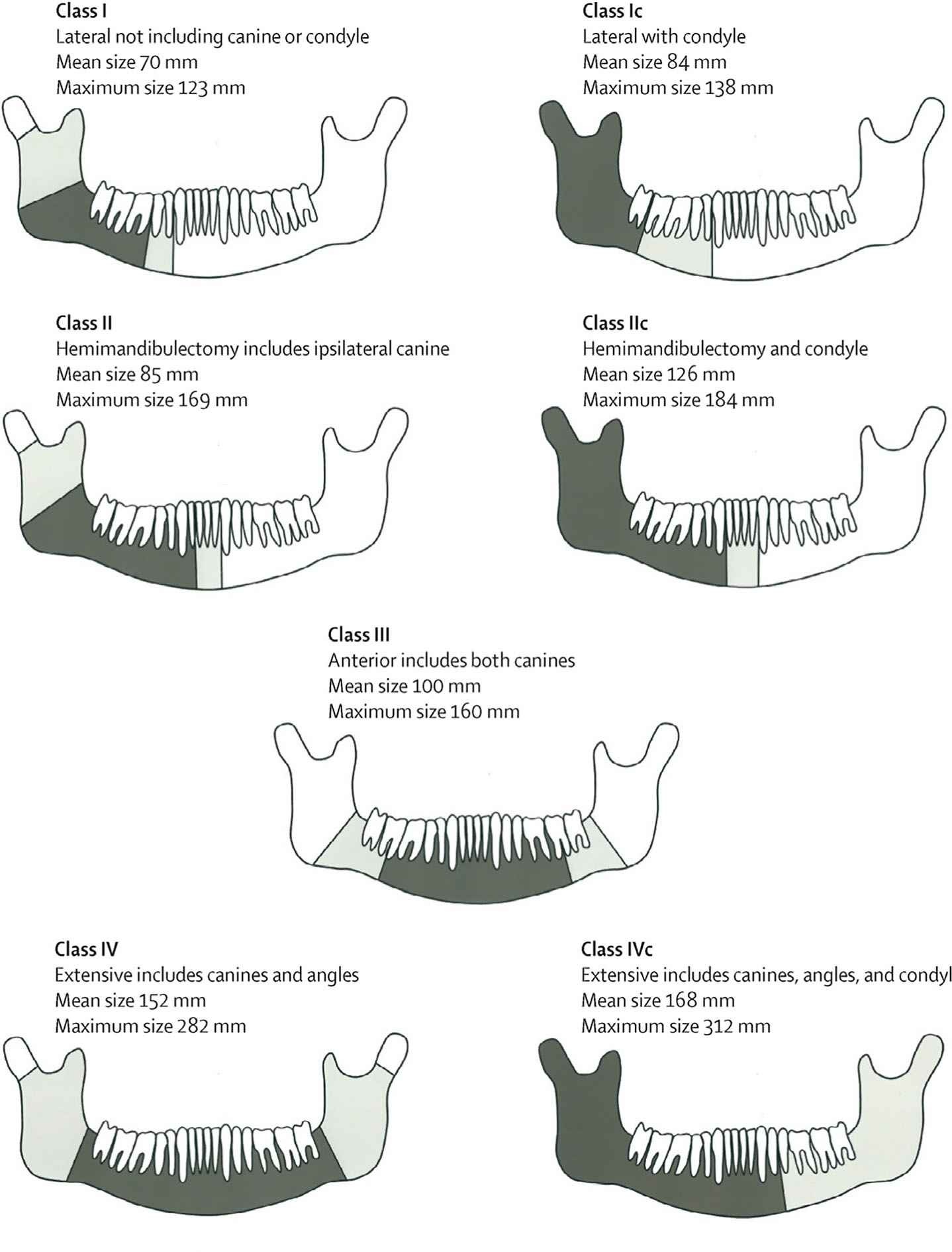
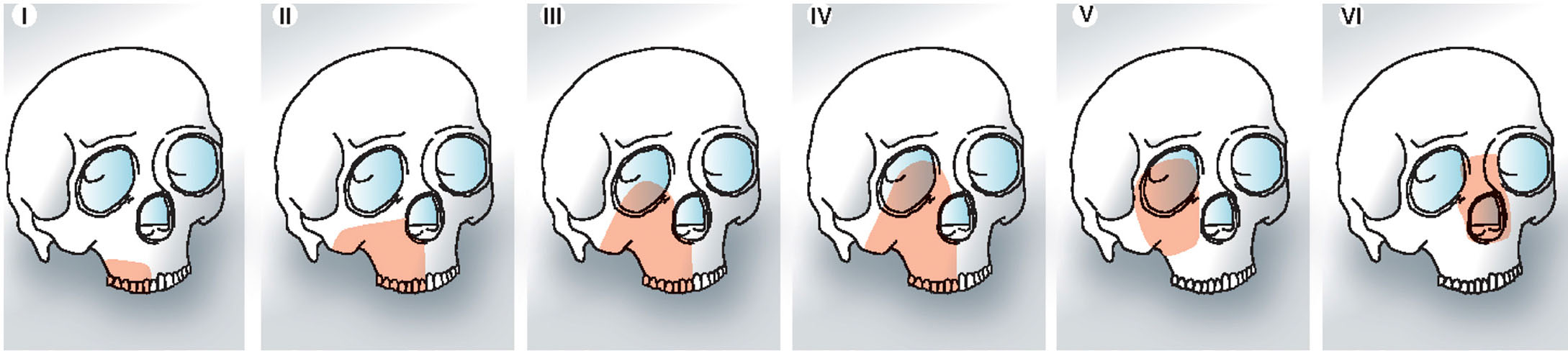
After completion of treatment for head and neck cancer, the Restorative Dentist will assess the patient for functional and aesthetic limitations and plan the rehabilitative phase of treatment. Due to pre-treatment extractions, patients may often have difficulty when they resume normal function after treatment. In cases of maxillary or mandibular resection, the reconstruction is unique and requires attention to form and function. Figures 211 and 312 outline classifications of maxillary and mandibular defects following resective surgery.
Figure 2. Mandibular defects following resective surgery.11 Permission to use figure has been granted by Mr James Brown.Figure 3. Brown et al's classification of maxillary defects following resective surgery.12 Permission to use figure has been granted by Mr James Brown.
Low level maxillary defects levels I and II involve communication with the antrum and oral cavity, lending to sensitivity, speech defects and difficulty swallowing. For this reason, these defects are often more complex to rehabilitate than higher level defects that involve orbital structures (levels III, IV, V and VI).
Restorative treatment options that can be employed to rehabilitate patients after undergoing treatment for head and neck cancer are broadly categorized as follows:
No treatment;
Rehabilitation with fixed prostheses; and
Rehabilitation with removable prostheses.
No treatment
Although patients will often present with missing teeth, they may opt for nonrestorative treatment. Careful restorative planning prior to head and neck cancer treatment can sometimes leave patients with functioning shortened dental arches and no communication between oral and midface spaces. In these cases, maintenance of the dentition and a strict preventive regimen as described previously is advised.
Fixed prostheses
Conventional or adhesive prostheses can be used to replace single or small spans of missing teeth provided that the status of the remaining teeth is satisfactory. Adhesive bridges should be preferred to conventional since they are non-invasive and carry minimal risks to the abutment teeth whilst providing satisfactory survival rates if designed correctly.13 Fixed prostheses can be tooth-borne or implant-supported.
Removable prostheses
Conventional or implant-supported removable prostheses are able to replace both hard and soft tissues. Patients may encounter difficulties whilst trying to adapt psychologically and socially if they have no previous denture-wearing experience.
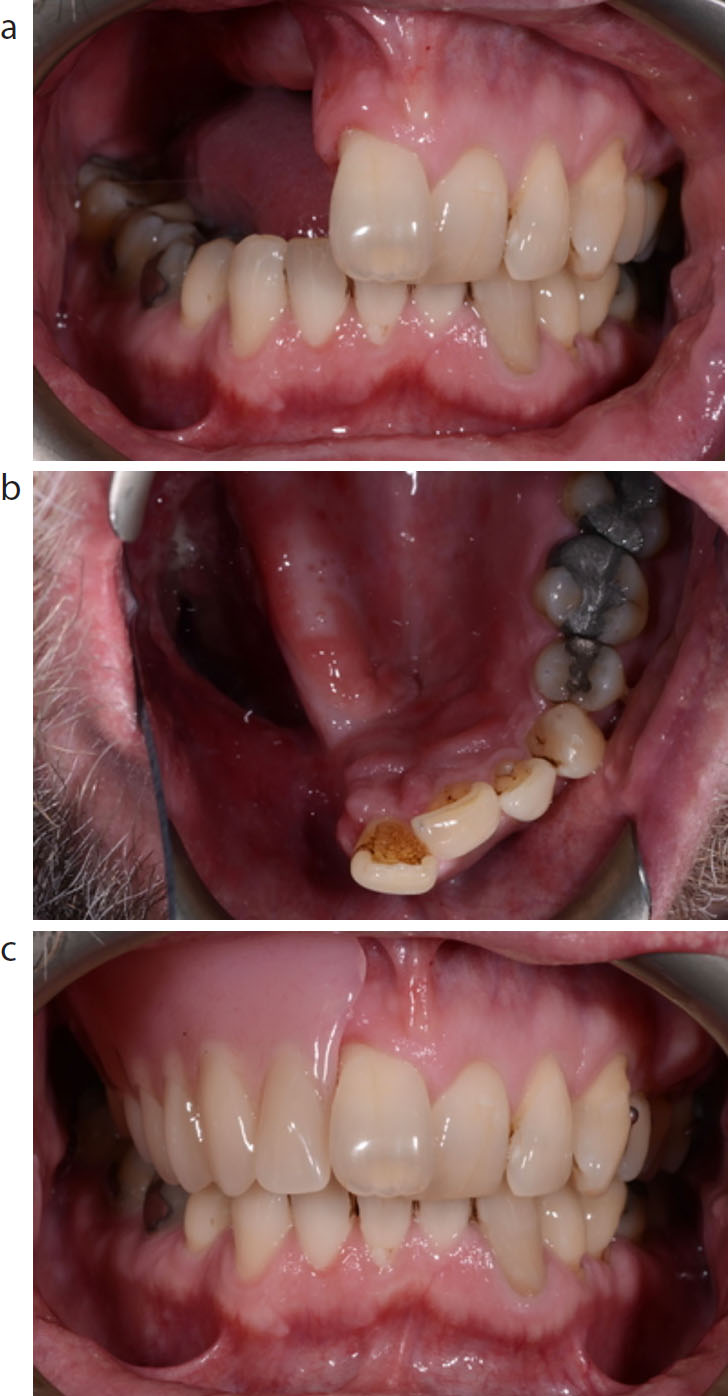
Partial dentures may also be appropriate treatment options for those who have multiple edentulous spans that require restoration. Figure 4 shows a patient who has had a partial glossectomy and floor of mouth resection, partial mandibular rim resection, bilateral neck dissections and reconstruction with a radial free forearm flap. This patient was rehabilitated simply with a lower partial denture to replace teeth, hard and soft tissue defects.
Figure 4. (a–c) Post-treatment images of partial glossectomy and floor of mouth resection, partial mandibular rim resection, bilateral neck dissections and reconstruction with a radial free forearm flap. This partial denture replaces missing teeth, hard and soft tissue defects.
Obturators
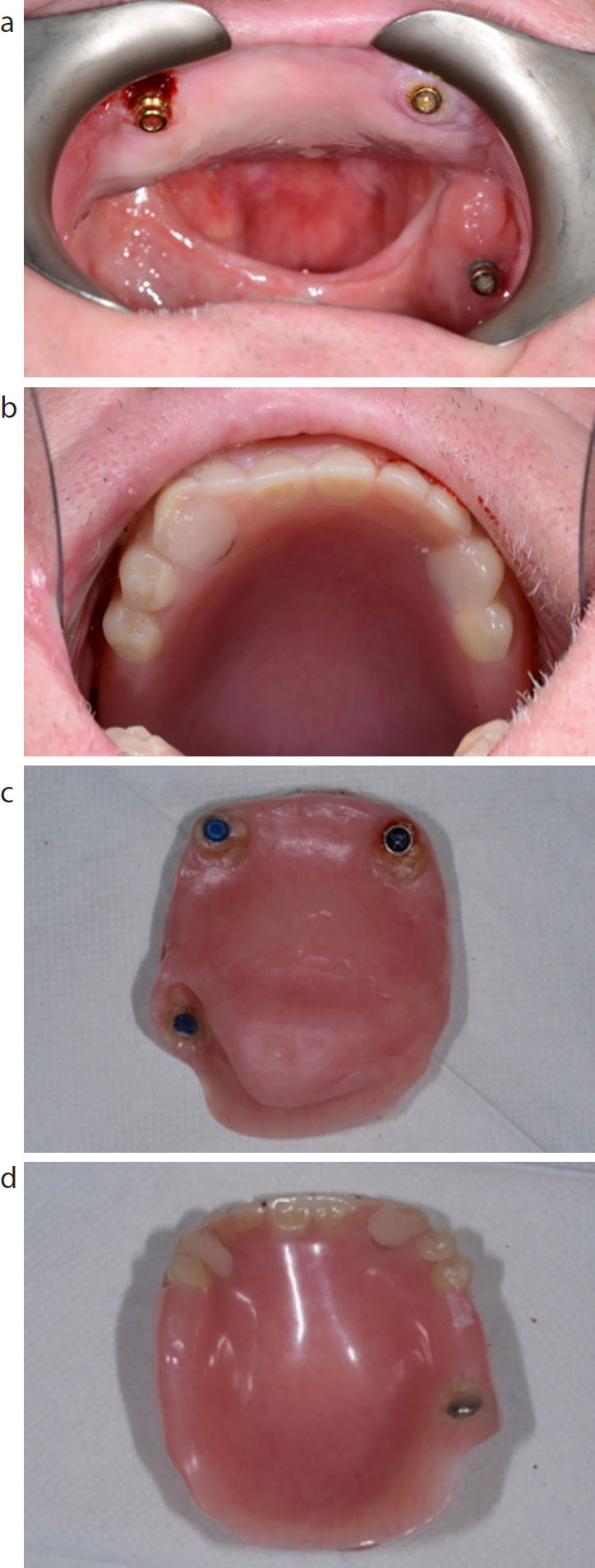
These are removable prostheses that occlude a maxillary defect. They can be implant-retained (Figure 5), supported entirely by mucosa (Figures 6 and 7) or tooth-supported. Obturators are provided by the secondary care restorative team but general dental practitioners may still be asked to maintain the remaining dentition.
Figure 5. (a–d) Implant-retained obturator for occlusion of maxillary defect and restoration of missing teeth.Figure 6. (a–c) Mucosa-borne obturator to restore maxillary defect following hemimaxillectomy surgery.Figure 7. (a–d) Partial maxillectomy restored with a removable obturator.
Obturators can be designed either as single or multiple part prostheses. They can be hollow, which allows them to be up to 50% lighter, and be lined with supported or unsupported silicone, which engages undercuts. As with all prostheses, support and retention can be gained from teeth, mucosa and/or implants.14 Problems encountered by patients who wear obturators may include speech difficulties, masticatory difficulties and leakage into oral or nasal cavities.15 There is also a maintenance burden on dental professionals to ensure prostheses continue to function throughout the patient's life.
Dental implants
Osseointegrated dental and zygomatic implants can be used to facilitate rehabilitation by providing additional retention, stability and support for prostheses. They can either be placed at the time of surgery (primary) or at a later date (secondary). Delayed implant placement allows for more time to plan the case prosthodontically and for a detailed assessment of an individual's prognosis and risk factors. However, primary implant placement facilitates more timely rehabilitation in selected cases.
In cases of segmental resection and reconstruction of the mandible, implant survival and usefulness is improved by delayed placement after suitable prosthodontic planning.16 If implants are to be placed in irradiated bone, careful planning is required, as failure rates are higher and there is a risk of osteoradionecrosis.17 Implants can also be placed into vascularized bone flaps at primary or secondary stage to facilitate prosthodontic rehabilitation.18 As well as conventional dental implants, zygomatic implants can be used to help retain prostheses by providing remote anchorage in larger defect cases. However, their placement requires additional skill expertise and has associated risks.19
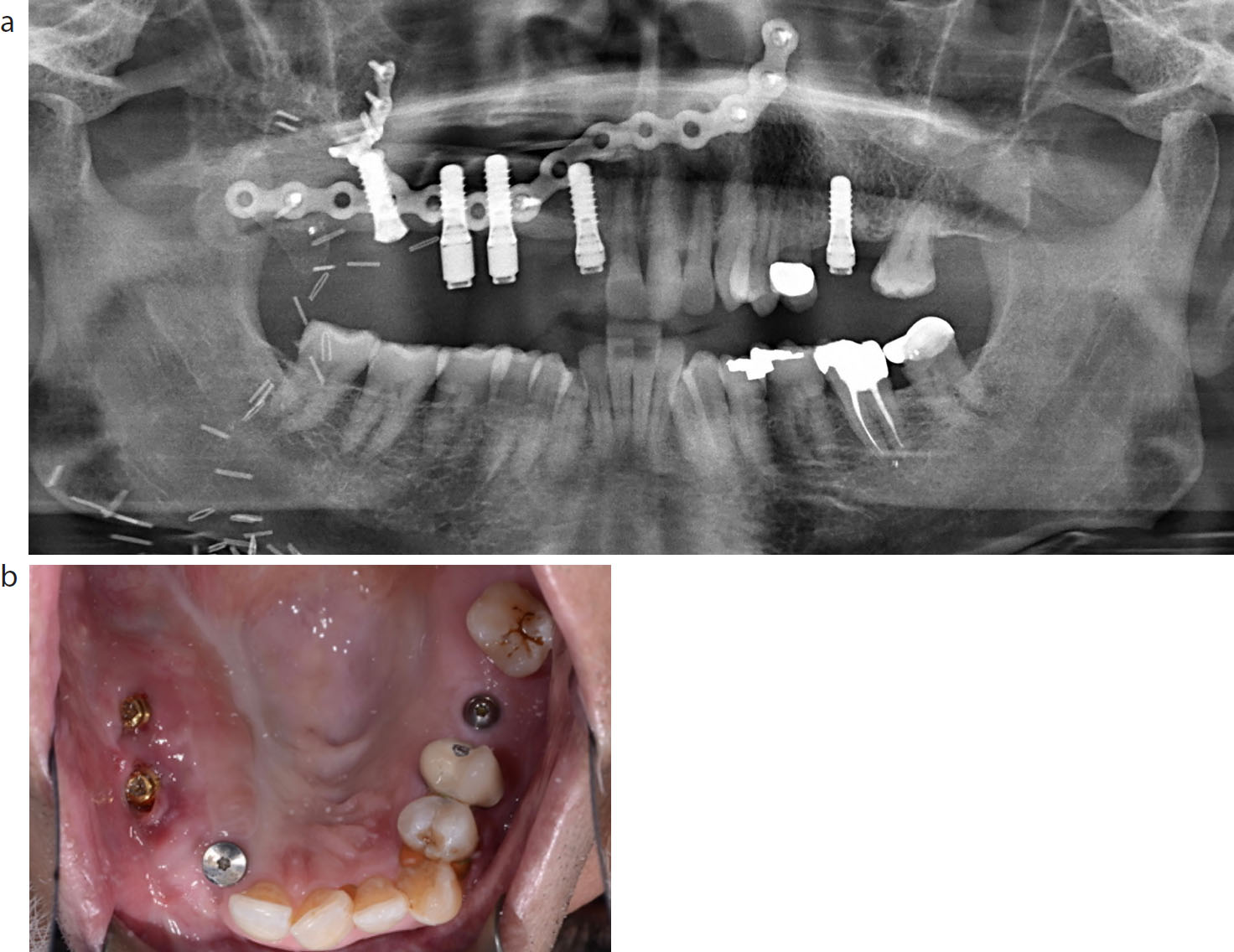
The DPT in Figure 8a illustrates implants and reconstruction plate used in the maxilla. Surgical clips can sometimes be seen as artefacts on intra-oral radiographs. Figure 8b shows an intra-oral view of implants placed in a bone flap in the upper right quadrant after a partial maxillectomy. Primary closure has been achieved by using the soft tissue from the buccal mucosa.
Figure 8.
(a) DPT shows maxillary reconstruction plate, implants and surgical clips. (b) Implant placement in the maxillary ridge and free flap reconstruction of the same patient.
Figure 9 demonstrates the rehabilitation of a patient who underwent right maxillary resection following a diagnosis of verrucous hyperplasia, and was rehabilitated with an implant-retained partial denture.
Figure 9. (a–d) Implant-retained maxillary prosthesis following surgical removal of verrucous hyperplasia and reconstruction.
The role of the maxillofacial technicians in the functional and social rehabilitation of patients should also be highlighted. They have an important role in planning and creating intra- and extra-oral prostheses, including prosthetic eyes, ears and noses that may have been removed in higher level maxillary defects (Brown et al's classification V and VI).12
Conclusions
The effects of treatment for head and neck cancer, both physically and psychologically, can be life-changing and debilitating for patients. General dental practitioners should recognize their importance in the wider head and neck MDT and should work in collaboration with secondary care services to ensure prevention of disease, limitation of side-effects and rehabilitation. Table 2 summarizes the role of primary and secondary care dental services in the head and neck cancer pathway.
Phase
Stage
Provider
Pre-treatment
Dental assessment
Secondary care
Pre-treatment extractions (if required)
Secondary care (to speed up treatment process)Can also be requested to Primary care
Periodontal and pre-treatment restorations
Primary care
Prevention
Primary and Secondary care
Peri-treatment
Emergency dental work
Secondary care
Prevention
Primary and Secondary care
Post-treatment
Post-treatment dental assessment
Secondary care
Rehabilitation
Secondary care
Extractions/Minor oral surgery
If in radiotherapy field – Secondary careIf not in radiotherapy field – Primary careLiaise with Secondary care if unsure
Prevention
Primary care
Routine restorative treatment
Primary care
Rehabilitation services provided in secondary care include reconstruction and advanced prosthodontics. This does not only help to restore patients functionally and aesthetically, but can also go a long way in ensuring social and psychological rehabilitation to improve a patient's overall quality of life following this disease.
In this three-part series, readers have been provided with an overview of risk factors, diagnosis and classification of head and neck cancers, as well as the pathway for treatment and rehabilitation. A good knowledge of these different aspects should improve confidence in engaging in the care pathway of affected patients and allow for continued support throughout their journey.