The role of antimicrobials in management of periodontal diseases Bilawal Aziz Firdaus Praveen Sharma Michael Milward Dental Update 2024 46:10, 707-709.
Authors
Bilawal AzizFirdaus
Final Year Dental Undergraduate Student, University of Birmingham School of Dentistry, Birmingham, B5 7EG UK
With the looming threat posed by antimicrobial resistance, appropriate prescribing of antimicrobials, including antibiotics, is increasingly relevant. In this article, the reasons why antimicrobial therapy is not the mainstay of treatment for most patients with periodontitis will be explored. Some specific exceptions to this rule will also be investigated, including why such exceptions exist. In addition, the protocols for periodontal and antimicrobial therapy to maximize the treatment response when adjuvant antimicrobials are used will be presented.
CPD/Clinical Relevance: This article highlights the need for appropriate prescribing within dentistry as a whole and specifically when it comes to the management of periodontal diseases, where antimicrobials do not form the mainstay of treatment, with some exceptions.
Article
Bilawal Aziz Firdaus
Given that periodontitis, on a basic level, is an imbalance between the microbial load and the host-response to that microbial load, at first glance it may appear that antimicrobials, specifically antibiotics, should be the mainstay of treating periodontitis. However, this is not the case. Before we discuss this further, it is useful to clarify some terminology. An antimicrobial is a substance capable of killing or inhibiting the growth of any micro-organism, whereas an antibiotic is a substance capable of killing or inhibiting the growth of bacteria specifically. The mainstay of managing periodontitis is not via the use of antibiotics. It is rather via the lowering of the bacterial load, as discussed in other papers in this issue, by mechanical removal (brushing and interdental cleaning). This can be aided by the removal of plaque retentive factors (PRFs) by a dental care provider, along with bearing the periodontium in mind when dentally rehabilitating the patient by providing restorations that are designed to minimize plaque retention and are cleansable by the patient. In this paper, the following will be discussed:
Reasons why antibiotics are not routinely indicated in the treatment of periodontitis;
Reasons for using antibiotics sparingly;
Exceptional circumstances in which antibiotics may be indicated in the management of periodontitis;
Types of antibiotics (local/systemic).
Reasons why antibiotics are not routinely indicated in the treatment of periodontitis
Site of periodontitis
In periodontitis, the bacteria are mainly contained in the biofilm present on the tooth/root surface. This site is effectively external to the body and the defence mechanisms therein. The challenge of this external infection is compounded by the fact that the bacteria are present in a biofilm, as opposed to floating around planktonically. Figure 1 shows a probe inserted into a mesio-buccal pocket with suppuration evident. Consider the environment that the probe is in. Is it ‘inside’ or ‘internal’ to the body? Or can it be thought of as being on the ‘surface’ of the body? Bacteria that exist in this environment exist in a biofilm on the surface of the tooth and planktonically in the exudate from the pocket.
Figure 1. Probe placed in mesio-buccal pocket of lower left canine tooth.
Treating this suppuration with antibiotics alone would be challenging as biofilms are notoriously resistant to penetration by antibiotics.1 Therefore, disrupting this biofilm, by mechanical instrumentation, would greatly increase the efficacy of any antibiotic used as an adjunct in the management of periodontitis (Figure 2). All systemic medications need to be initially absorbed by the gastro-intestinal tract and then pass through the liver, before being available in the bloodstream. This can limit the systemic concentration. In addition, for an antibiotic to reach the gingival crevicular environment, it needs to be able to pass through the gingival tissues and be present in the gingival crevicular fluid (GCF) before it can act in the periodontal pocket. This limits the effective dose reaching the gingival crevicular environment, as well as the time that the antibiotic remains in this environment, both of which further limit the effectiveness of antibiotics in these sites.
Figure 2. Diagram to represent (a) the biofilm present on the root surface and (b) how instrumentation disrupts the biofilm to produce a single cell planktonic bacterial suspension. The bacteria are represented by blue cocci and red bacilli, and antibiotics by yellow arrows. It can be seen in (a) that the antibiotic struggles to penetrate the biofilm and has the ability to act on a small surface area of the bacterial surface, whereas when the biofilm is disrupted by instrumentation the antibiotic can easily access the bacterial cell surface, resulting in enhanced efficacy.
Non-specific bacteria involved in periodontitis
Unlike some diseases, periodontitis does not have one causal organism implicated in its pathogenesis. Not only this, there are many types of bacteria implicated in the pathogenesis of periodontitis. These are predominately anaerobic, ie bacteria that have a preference of an oxygen depleted environment which is found in the periodontal pocket. Bacteria are also classified on the basis of Gram staining which is where certain bacteria, with a cell wall with a thick peptidoglycan layer, stain up blue in the presence of a dye. These are termed Gram positive bacteria. Other bacteria, whose cell wall does not have a thick peptidoglycan layer, do not get stained blue and are termed Gram negative. Periodontitis is most commonly associated with Gram negative bacterial types. It would be ideal to have an antibiotic that just specifically targets these periodontal pathogens but such an antibiotic is not available and the antibiotics we do use will have a wider systemic effect, eg impact on the gastro-intestinal tract flora. One of the potential serious consequences is overgrowth of the bacterium Clostridium difficile, leading to diarrhoea. Another issue with the use of non-specific or broad-spectrum antibiotics is the potential emergence of resistance, which will be discussed later in this article.
Patient compliance
The predominant method of reducing bacterial plaque levels is by instigating patient-based, tailored oral hygiene methods. Dental care professionals can aid this by the removal of PRFs, including calculus and overhanging restoration/s, as well as always designing restorations or removable partial dentures that minimize plaque retention. One of the key reasons for the ineffectiveness of general systemic antibiotic use is patient compliance in regard to frequency of use and taking a full course of antibiotics as prescribed. Deviation from the prescribed course of antibiotics will lead to a reduction in their effectiveness.
In summary, the site of the infection in periodontitis being on the ‘surface’ of the body, the bacteria being in a biofilm, the sheer variety of bacteria involved with periodontitis, doubts about patient compliance and that non-surgical periodontal treatment in most cases produces good outcomes, all conspire against the use of antibiotics in most cases of periodontitis.
Reasons for using antibiotics sparingly
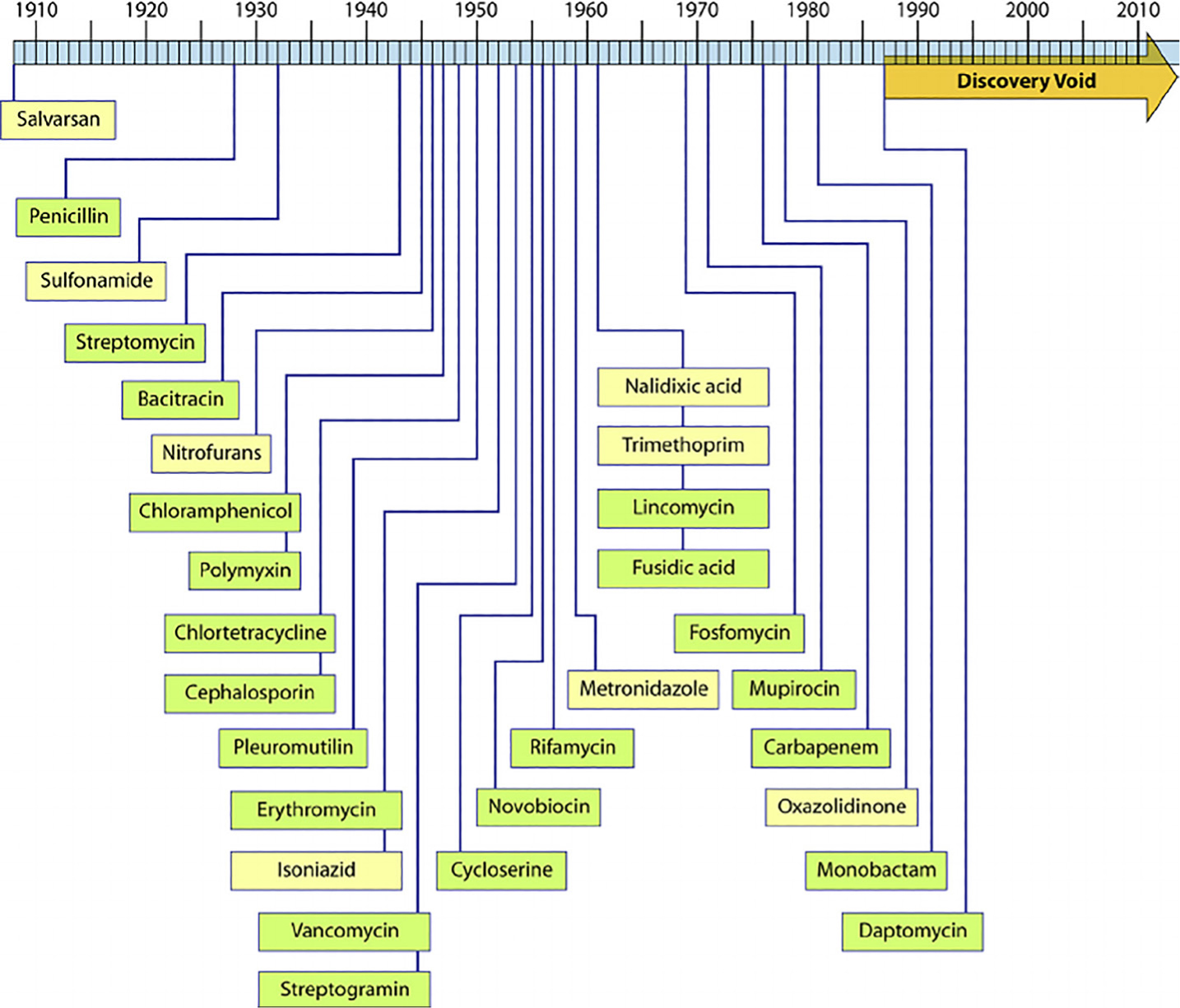
This relates to periodontal disease management as well as inappropriate use of antibiotics in dentistry as a whole. The use of antibiotics leads to the development of resistant strains of bacteria. These strains are often termed ‘super-bugs’ in the media. There is an evolutionary pressure for bacteria to resist the antibiotics designed to kill them or inhibit their growth. This can be illustrated via a sobering video by Harvard Medical School (https://www.youtube.com/watch?v=plVk4NVIUh8). This video highlights the natural evolution of bacterial resistance and the fact that this is accelerated by the evolutionary pressure exerted by the use of antibiotics. Added to this is the lack of development in the field of antibiotics, with the last new class of antibiotics developed in the mid-1980s, leading to a ‘discovery void’ since then (Figure 3).2
Figure 3. Timeline of antibiotic discovery/patent showing the lack of development of new antibiotics.2
The growing antibiotic resistance, coupled with a lack of development of new antibiotics, means that, in the future, infections that are commonly treated with antibiotics will become harder and harder to treat. The responsibility for the appropriate prescription of antibiotics lies with the prescriber but the greater threat of antibiotic resistance needs tackling on a few fronts, including the misuse of antibiotics in farming and agriculture.3
Types of antibiotics
Antibiotics have two modes of action, they can either be bactericidal, in which case they kill or lyse bacteria, or they can be bacteriostatic, in which case they prevent bacterial multiplication, thereby allowing the host's inflammatory response to remove bacteria. The bacteriostatic or bactericidal actions may be achieved in a wide variety of ways. These include inhibiting the bacterial cell from synthesizing essential components such as cell walls or proteins or nucleic acids.
In addition, antibiotics can be classified as systemic or local delivery, with the former affecting the whole body, as well as the site of need and the latter having a limited effect on the rest of the body, apart from the site of need/delivery. The advantages and disadvantages of local delivery systems, compared to systemic antibiotics, are summarized in Table 1.
Advantages
Disadvantages
Reduced systemic dose
Expensive
High local concentration
Still require RSD or biofilm disruption
Superinfections, such as with Clostridium difficile, unlikely
Limited indications
Drug interactions unlikely
Site specific
Patient compliance not an issue as applied by heathcare provider
Can utilize agents which can't be utilized systemically, eg chlorexidine
In the next section, systemic and local delivery of antimicrobials shall be discussed, in the management of periodontitis.
Indications for the use of systemic antibiotics in periodontitis
There are a few exceptions to the general rule of not prescribing antibiotics in the management of periodontitis.4 These include:
The disease formally known as ‘Aggressive periodontitis’;
Necrotizing Periodontal Diseases (NPDs).
The disease formally known as ‘Aggressive periodontitis’
The new classification of periodontitis, discussed in this issue, has removed the term ‘Aggressive periodontitis’. This is because it is now thought to be a variant of periodontitis, as opposed to a unique identity in itself. The cases which would have been captured as ‘Aggressive periodontitis’ are now captured either as periodontitis with a molar-incisor pattern or periodontitis of grade C or even grade B. However, these categories also capture cases of periodontal disease which would not traditionally have been classified as ‘Aggressive periodontitis’. For example, a 70-year-old patient with >70% bone loss in the worst site would be grade C but would not previously have been thought of as ‘Aggressive periodontitis’. Similarly, a 35-year-old with a third bone loss at the worst site would currently be grade B, but previously may have been considered a case of ‘Aggressive periodontitis’. The distinguishing feature would still be bone loss not in keeping with the patient's level of oral care and/or absence of other risk factors and the rapidly progressive nature of disease. In this respect, there is clarification needed between the old and new classification, which is particularly relevant in cases previously thought of as aggressive, because these had a specific management protocol which included the use of systemic antibiotics and currently this has not been fully elucidated in the new classification. This was because it was believed that, in aggressive disease, in addition to being present in a biofilm on the tooth surface, bacteria were also able to invade the local soft tissue and act as a reservoir there. Hence, biofilm disruption by means of root surface debridement (RSD) alone would be ineffective in removing this reservoir. For this reason, antibiotics are recommended in such cases with the following protocol:
Instigate oral hygiene measures, complete RSD of all sites indicated by Detailed Pocket Chart (DPC) in as short a time as possible, ideally, within one week. Immediately following the completion of the last visit of RSD, and the ensuing disruption of biofilm, the patient is to start amoxicillin 500 mg and metronidazole 400 mg TDS for 7 days. Patients need to be cautioned regarding alcohol intake while taking metronidazole and should abstain from alcohol for a couple of days following the end of metronidazole use. Similarly, care must be taken with the patient's existing medication when prescribing antibiotics, for example patients on warfarin may find their INR raised as there is an increased anti-coagulant effect of warfarin. Metronidazole is best avoided in such patients but, if it is used, liaison with the anticoagulant clinic with close INR monitoring will be required. Cases of amoxicillin interacting with warfarin are rare. In cases where the amoxicillin and metronidazole regimen cannot be prescribed, such as in patients allergic to penicillin or patients on warfarin, the antibiotic of choice is doxycycline, which is prescribed as a 21-day course of 100 mg, once a day with a ‘loading dose’ of 200 mg on the first day. Like all tetracyclines, the use of doxycycline should be avoided in patients who are pregnant or breastfeeding due to the risk of deposition of the drug in developing bones and teeth leading to discoloration (tetracycline staining). As with all antibiotics, it is important to stress that patients take these as prescribed and finish the course of antibiotics. An alternative regimen to doxycycline, without the shortcomings of loss of compliance with a 21-day course of antibiotics as well as contra-indications in pregnant/breastfeeding patients, is azithromycin prescribed 500 mg doses once a day for three days. Patients may comply better with this short course antibiotic and the drug is thought to be retained in the tissues for a period of time such that a missed dose may be compensated for by continuing the drug on the following day. Azithromycin has been shown to be beneficial, especially in deeper sites of more rapidly progressing (grade C) periodontitis.5,6,7
Necrotizing Periodontal Diseases (NPDs)
The new classification of periodontitis categorizes necrotizing periodontitis and necrotizing gingivitis together as NPDs. NPD usually presents in young adults, smokers, patients with poor oral hygiene and diet and those under increased stress. Patients with NPDs typically have pain associated with the condition, which is unlike most cases of periodontal disease, and typically present with sloughing of the interdental papillae and characteristic halitosis. In such cases, antimicrobials are also indicated due to the relatively narrow range of bacteria involved in these disease processes (anaerobic spirochetes and fusiform bacteria). For this particular form of periodontal disease, metronidazole is the drug of choice as it is particularly effective against anaerobic bacteria. Patients should receive a course of 400 mg of metronidazole, TDS for 3 days with a review at this point. The cautions regarding the use of metronidazole in the previous section also apply here. In the management of NPDs, risk factors such as smoking and stress should be managed and antibiotics may need to be prescribed prior to non-surgical debridement as the gingivae may be too painful to debride. It goes without saying that the hesitance in prescribing antibiotics should be balanced with the immediate medical needs of the patient. As such, signs of spreading infections, such as lymphadenopathy, swellings which may compromise the airway or approaching the infra-orbital areas or pyrexia, may still warrant the use of systemic antibiotics, even if such infections are periodontal in origin. In severe cases, such as when the infection is threatening the airway, patients should be urgently referred for inpatient management.
Indications for the use of local antimicrobials in periodontitis
The use of local antimicrobials allows for the targeted deposition of a higher dose of antimicrobials, in a sustained fashion, at the site of the disease to the gingival crevice, thereby limiting the systemic dose of the antimicrobial agent. This also limits potential side-effects and drug interactions.
Local antimicrobials are only indicated for the odd site that does not respond to conventional, non-surgical RSD in a patient with well-controlled risk factors, including good oral hygiene and no detectable subgingival calculus deposits. They should not be used as the first line of therapy, in the absence of non-surgical therapy, in patients with poor oral hygiene, on multiple sites, or to treat endo-perio lesions. Prior to prescribing local antimicrobials, the reasons for failure of conventional RSD to resolve pocketing should be investigated. These are mentioned in more detail in the paper on ‘The Role of Maintenance in Periodontal Disease’ in this issue. Common reasons for a non-response to initial periodontal therapy include incomplete removal of subgingival deposits, poor oral hygiene on the part of the patient, lack of addressing of risk factors such as smoking cession, and endo-perio lesions, which will not respond to periodontal therapy alone. If a patient does not have these reasons for non-responsiveness, other strategies, such as periodontal surgery or use of local/systemic antimicrobials may be considered.
Whilst surgical treatment is an option, local delivery systems may be a suitable first option as it is less invasive in nature and doesn't require the specialist skills needed for surgical management. A systematic review on the effects of local antimicrobials8 as adjuncts to subgingival debridement in treating chronic periodontitis looked at 56 papers and came to the conclusion that the use of local antimicrobials is worthwhile in deep or recurrent sites and that those with sustained release properties (that have a mechanism to ensure the antimicrobial agent is retained in the pocket for longer) produce better results.
Commonly used local delivery systems for the management of periodontitis include PerioChip® and Chlo-site® which contain the antimicrobial agent chlorhexidine, Dentomycin and Atridox® which contain the antibiotic tetracycline, and Elyzol® which contains the antibiotic metronidazole. It is beyond the scope of this paper to discuss these in detail and practitioners are recommended to ensure adequate training before utilizing these systems. A comprehensive review by Jepsen and Jepsen offers a useful insight into their use.9
Alternative therapies
There are two further therapy modalities used in the management of periodontitis which will be considered in this article:
Periostat®; and
PerioWave™.
Periostat®
This consists of 20 mg of doxycycline, given twice a day for 3 months, systemically, as an adjunct to supra-/sub-gingival instrumentation. This low dose of doxycycline is considered to be sub-antimicrobial, meaning that the dose is insufficient to inhibit the growth of bacteria, rather it is prescribed for its role as a collagenase inhibitor. Collagenase, an enzyme produced by both bacterial and human cells, is responsible for the breakdown of collagen and is implicated in periodontal breakdown; therefore blocking this enzyme may have efficacy in the management of periodontitis.
A review by Preshaw et al highlighted that Periostat®, when used as an adjunct to periodontal therapy (Scaling and Root Planing (SRP)) yielded clinically and statistically significant reductions in probing depths and gains in clinical attachment levels compared with those seen with SRP alone.10 The authors also concluded that using a sub-antimicrobial dose of doxycycline was unlikely to exert a significant evolutionary pressure and therefore less likely to accelerate the development of drug-resistant bacteria.
PerioWave™
This is an example of an antimicrobial photodynamic therapy (aPDT) which utilizes a photoactivatable agent that absorbs light of a specific wavelength and is able to be taken up preferentially by bacteria. When the agent is exposed to this specific wavelength of light, in the presence of oxygen, free radicals are produced that are cytotoxic to micro-organisms and their products.11
Systematic review and meta-analysis of aPDT shows limited data but the data available show a mean pocket depth improvement of 0.19 mm and mean clinical attachment gain of 0.37 mm. This review/analysis came to the conclusion that aPDT produces short-term benefits over conventional therapy and the evidence for medium/long-term benefits is insufficient and further studies are required.11
Conclusion
This paper aimed to give an overview of the use of antibiotics in managing periodontal disease, but also how their abuse in the wider community has led to problems in terms of resistance. It is well recognized that the overuse of antibiotics has led to the development of resistant bacteria which have resulted in significant problems in the control of infectious diseases. It is of the utmost importance that all healthcare professionals recognize the value of antibiotics and ensure that they are only used in appropriate situations; this equally applies to management of periodontitis – there are limited situations where their use can be justified.