Eversole R, Su L, ElMofty S. Benign fibro-osseous lesions of the craniofacial complex. A review. Head Neck Pathol. 2008; 2:177-202
Oluwaseun AA, Salcedo SE, Borad V, Richard SS, Workman AD, Ray AO. Fibrous dysplasia: an overview of disease process, indications for surgical management, and a case report. Eplasty. 2015; 15
Alawi F. Benign fibro-osseous diseases of the maxillofacial bones. A review and differential diagnosis. Am J Clin Pathol. 2002; 118:50-70
Amit M, Fliss DM, Gil Z. Fibrous dysplasia of the sphenoid and skull base. Otolaryngol Clin North Am. 2011; 44:891-902
Penn LD, Tartarini RJ, Glass CH, Girolami UD, Zamani AA, Dunn IF. Natural history of cranial fibrous dysplasia revealed during long-term follow-up: case report and literature review. Surg Neurol Int. 2017; 8
Lane MJ, Khan SN, OConnor WJ Bisphosphonate therapy in fibrous dysplasia. Clin Orthop Relat Res. 2001; 382:6-12
Stanton RP, Ippolito E, Springfield D, Lindaman L, Wientroub S, Leet A. The surgical management of fibrous dysplasia of bone. Orphanet J Rare Dis. 2012; 7:1172-1177
Kaira S, Jain V. Dental complications and management of patients on bisphosphonate therapy: a review article. J Oral Biol Craniofac Res. 2013; 3:25-30
Kontio R. Update on mandibular reconstruction: computer-aided design, imaging, stem cells and future applications. Curr Opin Otolaryngol Head Neck Surg. 2014; 22:307-315
Fibrous dysplasia is a bone disorder whereby normal medullary bone is replaced by fibrous tissue. Many sites may be affected, including the craniofacial skeleton. A 33-year-old female presented at the Bristol Dental Hospital in 2007 complaining of a prominent and expanding lower jaw as well as poor aesthetics. She was diagnosed with craniofacial polyostotic fibrous dysplasia. In order to manage her concerns and the ongoing growth of the polyostotic lesions, a combined maxillofacial and restorative approach was utilized. After ten years of ongoing management and care, including surgery and dental rehabilitation, her primary concerns have been addressed.
CPD/Clinical Relevance: The clinician should be able to understand the clinical and radiographic appearance of craniofacial fibrous dysplasia, how the condition can impact a patient and the complex management that may be involved.
Article
There have been many classifications of bone-related conditions and fibro-osseous lesions. The most recent classification includes the one by Eversole et al,1 which is as follows:
Bony dysplasias;
Cemento-osseous dysplasias;
Inflammatory/reactive lesions;
Metabolic diseases, eg hyperparathyroidism;
Neoplastic lesions.
Fibrous dysplasia (FD) is a rare congenital sporadic disease of bone, which can affect the jaws, as well as other bones in the skeleton. First reported by Von Recklinghausen in 1891,2 it is known to develop in childhood, manifesting before the age of 10. Histologically, it is characterized by the resorption of normal bone, and subsequent replacement by a benign connective tissue matrix, haphazardly arranged, and poorly calcified woven bone. These lesions may become more radio-opaque with age due to the increase in bone density associated with bone expansion.1
Classification
There are two subtypes of fibrous dysplasia in the literature:
Monostotic fibrous dysplasia – a lesion which affects a single bone, common in the posterior maxilla;
Polyostotic fibrous dysplasia – multiple bones are affected, which can be subdivided into:
Jaffe type – with endocrine association;
McCune-Albright syndrome – associated with endocrine disturbances and skin lesions.
Fibrous dysplasia can present in any bone in the body; the most common sites include the ribs, femur and craniofacial skeleton. A higher prevalence is noted in the maxilla, rather than the mandible, with maxillary lesions extending to include the maxillary sinus, zygoma, sphenoid bone and floor of the orbit.3 Fibrous dysplasia can cause bony pain, dental anomalies, pathological fractures, as well as facial deformities, and therefore management can be challenging.4
Diagnosis
Fibrous dysplasia can vary in its appearance radiographically, but usually presents as a zone of radiolucency initially. Gradually, these lesions become radio-opaque, which may be described as ground glass, fingerprint, or an orange peel appearance. There is usually loss of the lamina dura of affected teeth, and there also may be enlargement of the bone. Teeth affected are rarely resorbed but may be displaced. In the maxilla, if present, it may cause obliteration of associated structures, such as the maxillary antrum and the base of the skull. Diagnosis is based upon patient history, clinical and radiographic examination1
Prevalence
Fibrous dysplasia affects males and females equally and the condition is usually diagnosed earlier in young children. The exact incidence and prevalence of the disorder is unknown. Due to lack of symptom presentation, mild cases can go undiagnosed, making it difficult to determine the true prevalence of fibrous dysplasia. Monostotic FD is more common than polyostotic FD and, according to some reports, by a ratio of 4:1.4 The craniofacial presentation is known to be more common than the polyostotic variant. Interestingly, the monostatic variant may arrest at puberty, whereas conversely the polyostotic variants have been known to progress until adulthood.5
Aetiology
The underlying aetiology of FD is not completely understood. Research indicates that the condition is characterized by a postzygotic mutation in the gene GNAS1, which may ultimately lead to proliferation of undifferentiated mesenchymal cells. This gene mutation is somatic. It therefore occurs after fertilization of the embryo, the presence of these mutated cells causing an abnormal bone matrix and growth. FD is thus not inherited, and so affected individuals do not pass the mutation on to their children and can present at any age.6 Malignancy has been shown in less than 1% of cases.
Management
Fibro-osseous lesions such as fibrous dysplasia may cause significant cosmetic and functional disturbances and should be managed according to their clinical presentation. For monostatic FD, surgical management should be delayed until skeletal growth has completed, as it tends to stabilize at this time. However, for symptomatic fibrous dysplasia, bisphosphonate therapy is utilized. It is important that the clinician differentiates between fibrous dysplasia and other radiographically and histologically similar lesions, such as ossifying fibroma. Management is usually as part of a multidisciplinary team, depending on the type of FD, and the location.
Case report
A 33-year-old female attended an oral maxillofacial surgery clinic at Bristol Dental Hospital regarding her mandibular overgrowth. Her main complaint was primarily of poor aesthetics as she was unhappy with the prominent appearance of her lower jaw. She reported that her jaws had appeared to grow in size since the age of 15 and her mother, who had a similar appearance of her jaws, was diagnosed with fibrous dysplasia in China. There was no history of dental pain but she did note that her teeth did not meet well when biting. Medically she was fit and healthy.
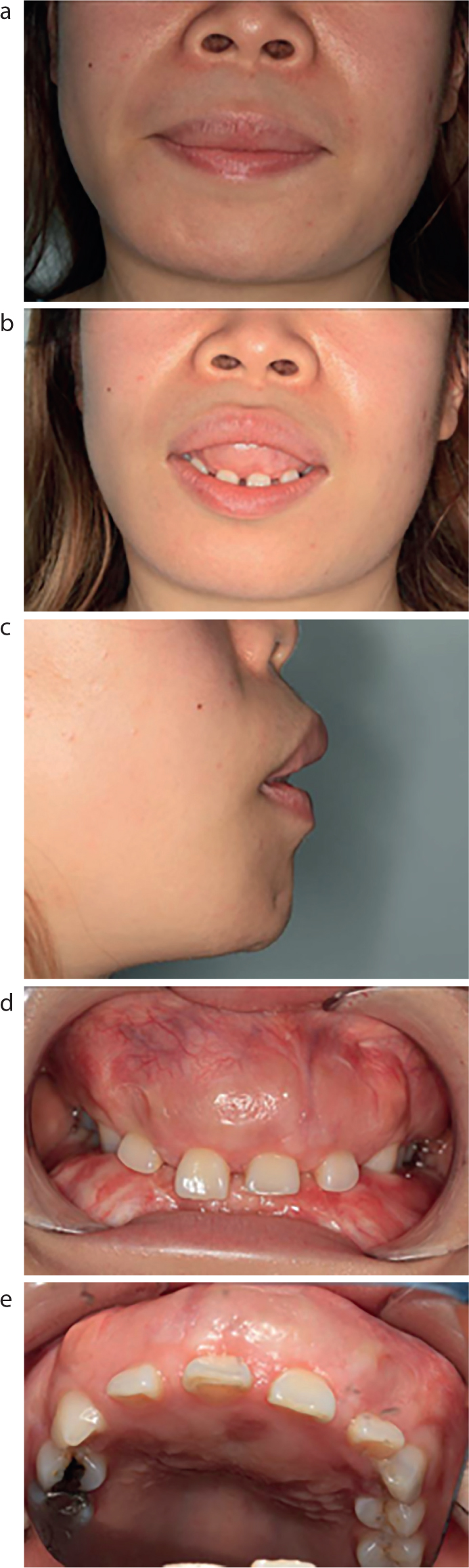
On extra oral examination
There was protrusion of the upper lip and lower lip and lip incompetence at rest (Figure 1). Intra-orally, the maxilla and mandible had bony enlargement. The bone was hard on palpation and the overlying mucosa of the lesion was intact.
Figure 1.
(a–e) Pre-operative views of the patient on presentation in 2016.
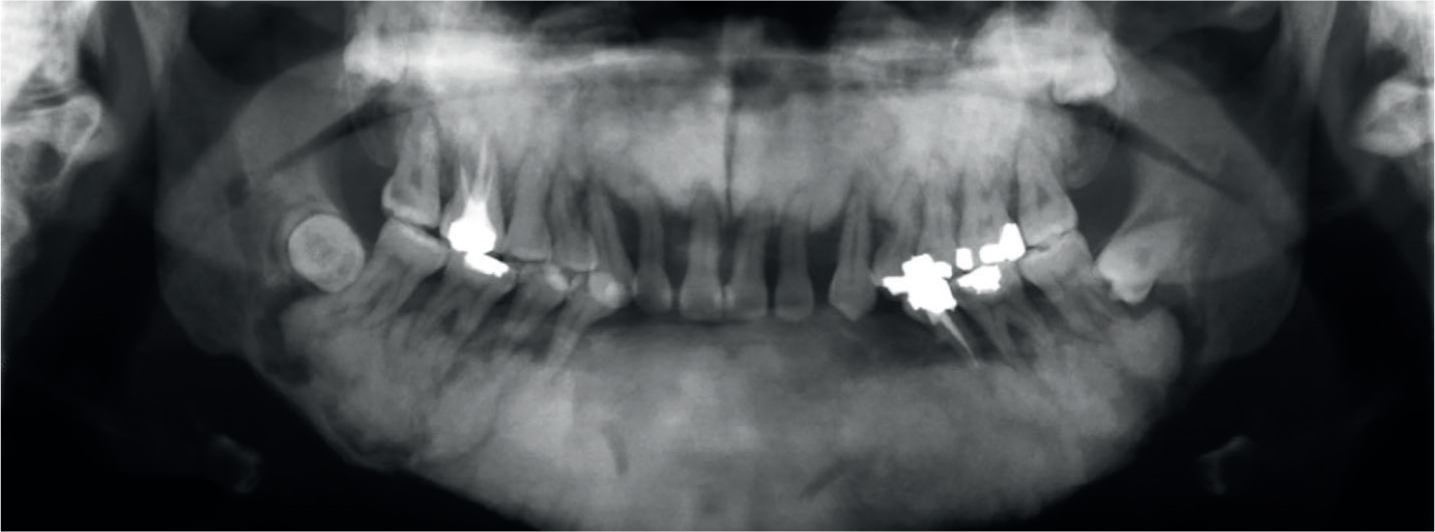
Radiographic investigation
An initial orthopantogram (OPG) radiograph (Figure 2) revealed generalized severe periodontal bone loss, and multiple mixed patchy radiolucencies, with areas of opacification, especially seen in the lower posterior quadrants. LL4 to LR3 were missing and had been extracted as part of the treatment provided (see later). There is evident loss of lamina dura on the remaining teeth, and the patient had a heavily restored dentition.
Figure 2. OPG radiograph from 2012, prior to restorative rehabilitation.
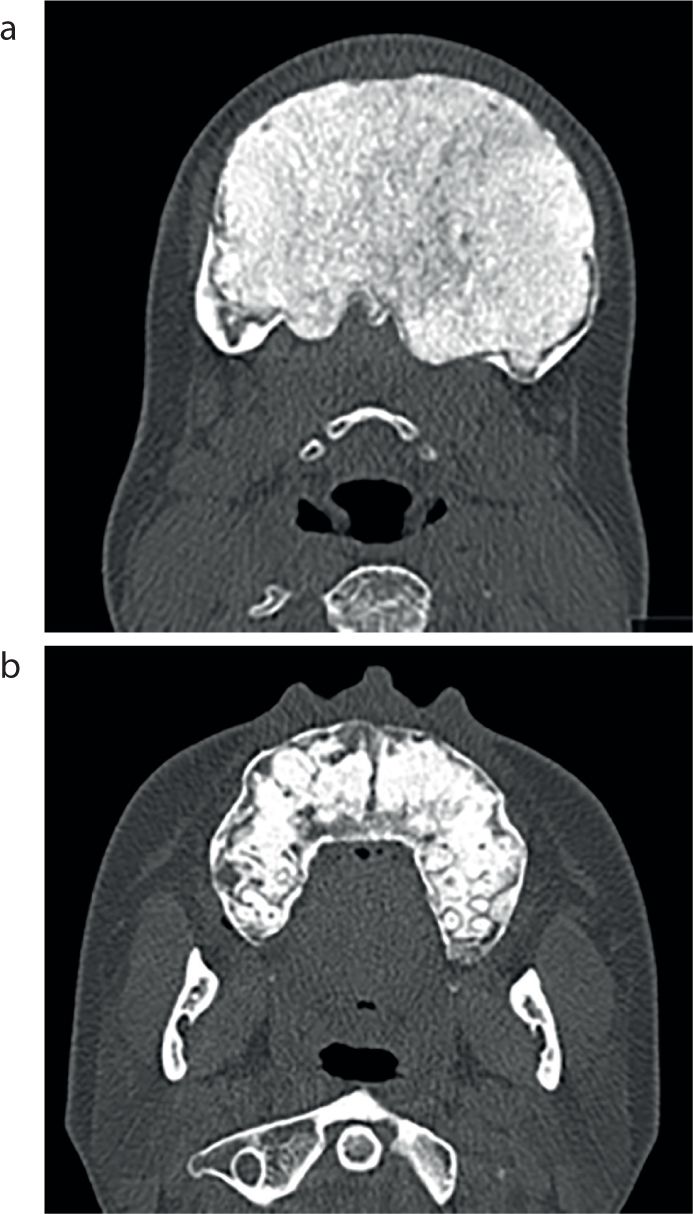
A CT scan of the facial bones showed gross expansion of the entire body of mandible and alveolar process of the maxilla, which extended into the floor of the maxillary antrum and posteriorly into the hard palate (Figure 3). The cortex was intact but the bone internally showed an amorphous calcific appearance, which was characteristic of established fibrous dysplasia.
Diagnosis was achieved on clinical and radiographic examination, which was craniofacial polyostotic fibrous dysplasia.
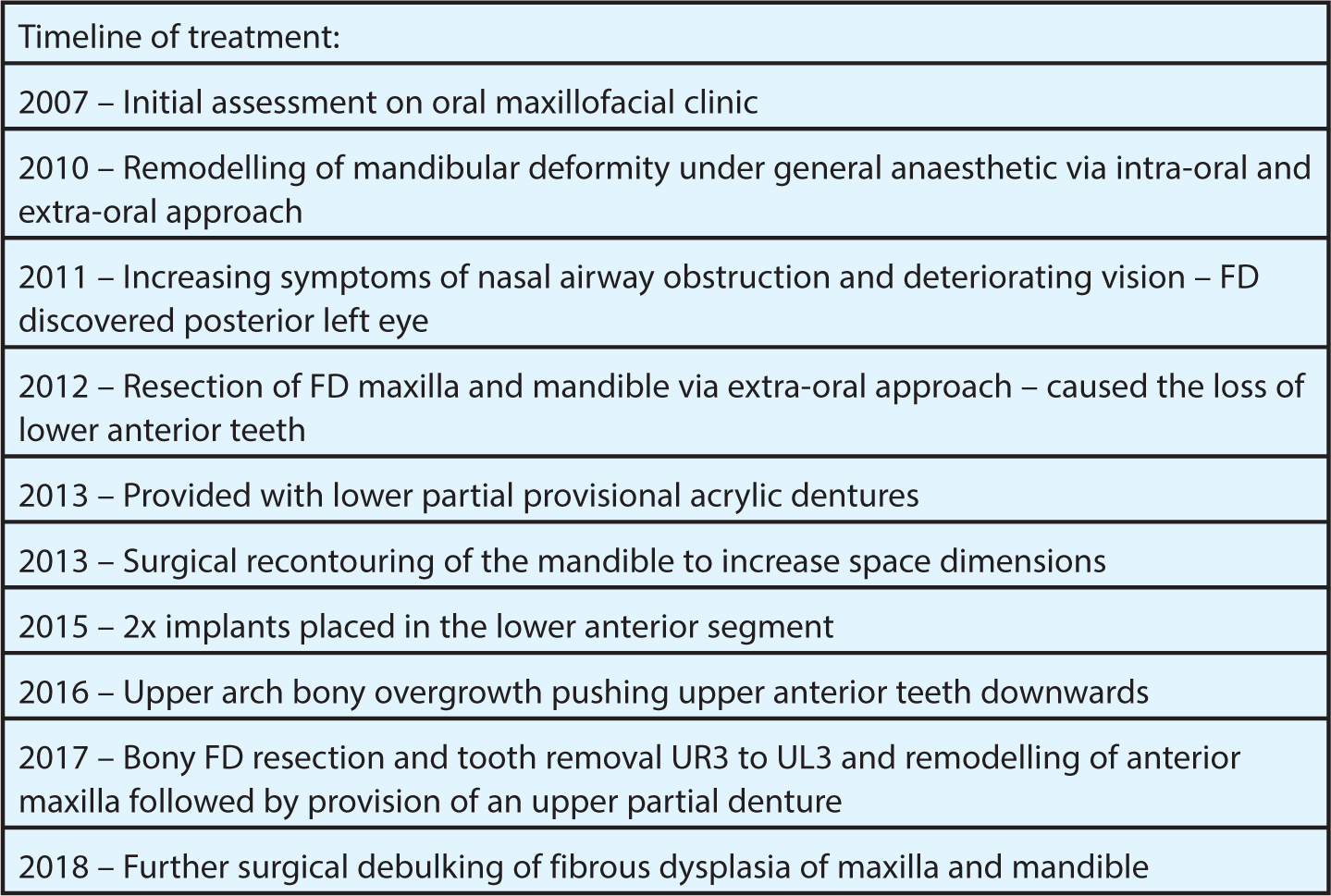
The patient was originally seen in 2007, at the oral surgery and maxillofacial department at Bristol Dental hospital. From 2007–2017, the patient underwent multiple courses of surgical and restorative treatment, using a multidisciplinary approach (see Figure 4 for timeline of treatment: Figures 5–8). It was noted, after initial bony augmentation, the fibrous dysplasia was seen to increase to the posterior aspect of the left orbit, which was noted due to nasal airway disturbances reported by the patient.
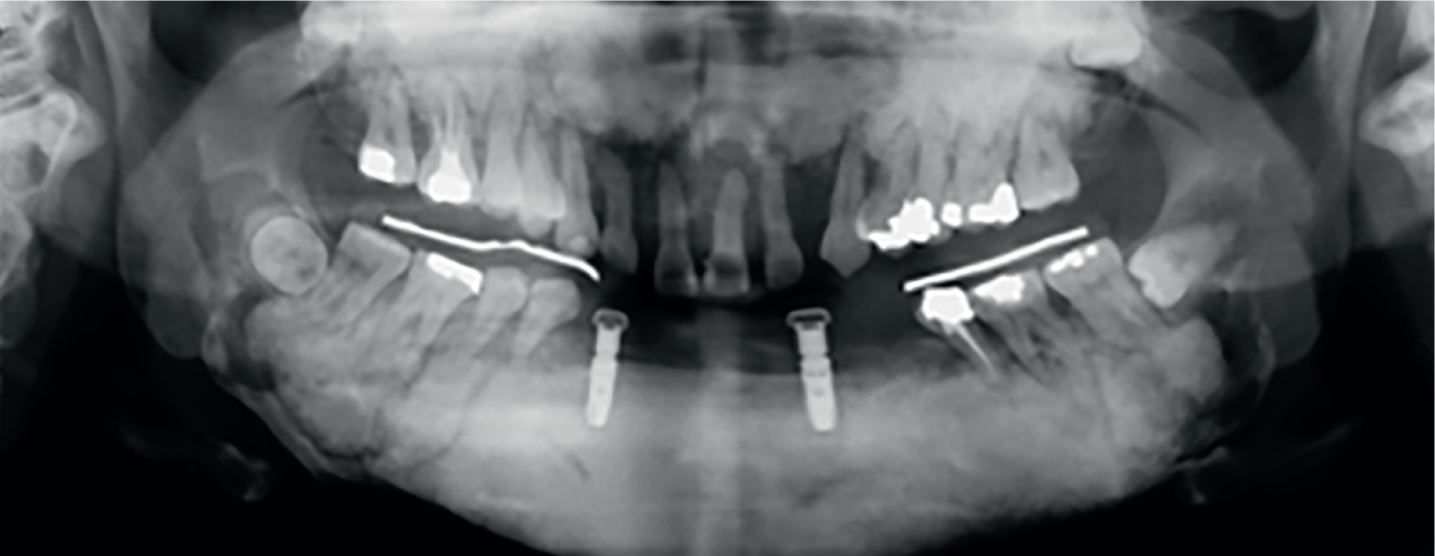
Figure 4. Timeline of the patient's restorative and surgical journey.Figure 5. OPG taken after placement of implants LR3, LL3 regions in 2015. Note the extensive bony destruction which had begun in UR321, UL123.Figure 6.
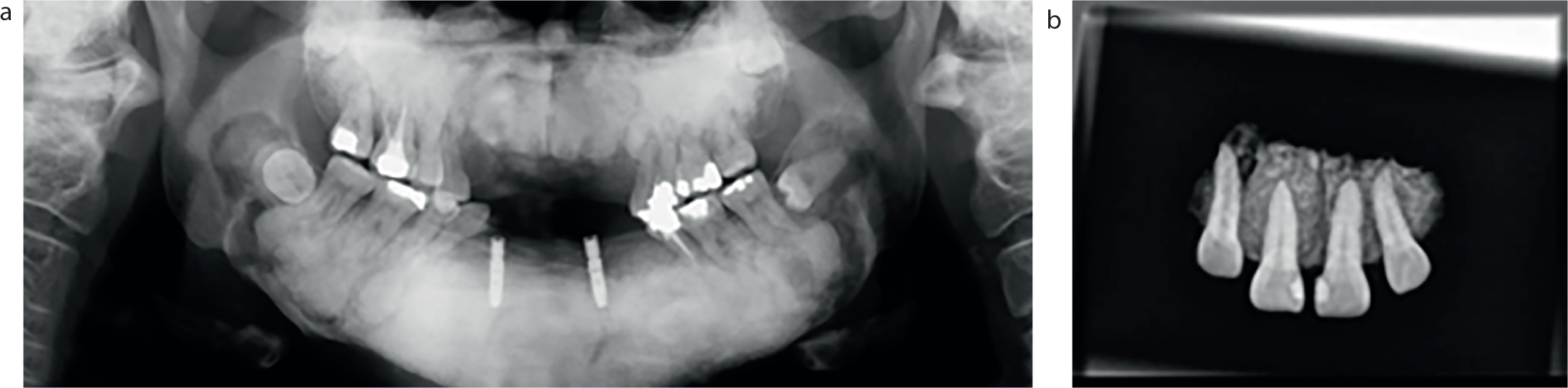
(a) Post-operative OPG after removal of upper anterior dysplastic segment in 2017. (b) Plain radiograph of dysplastic segment shown.Figure 7.
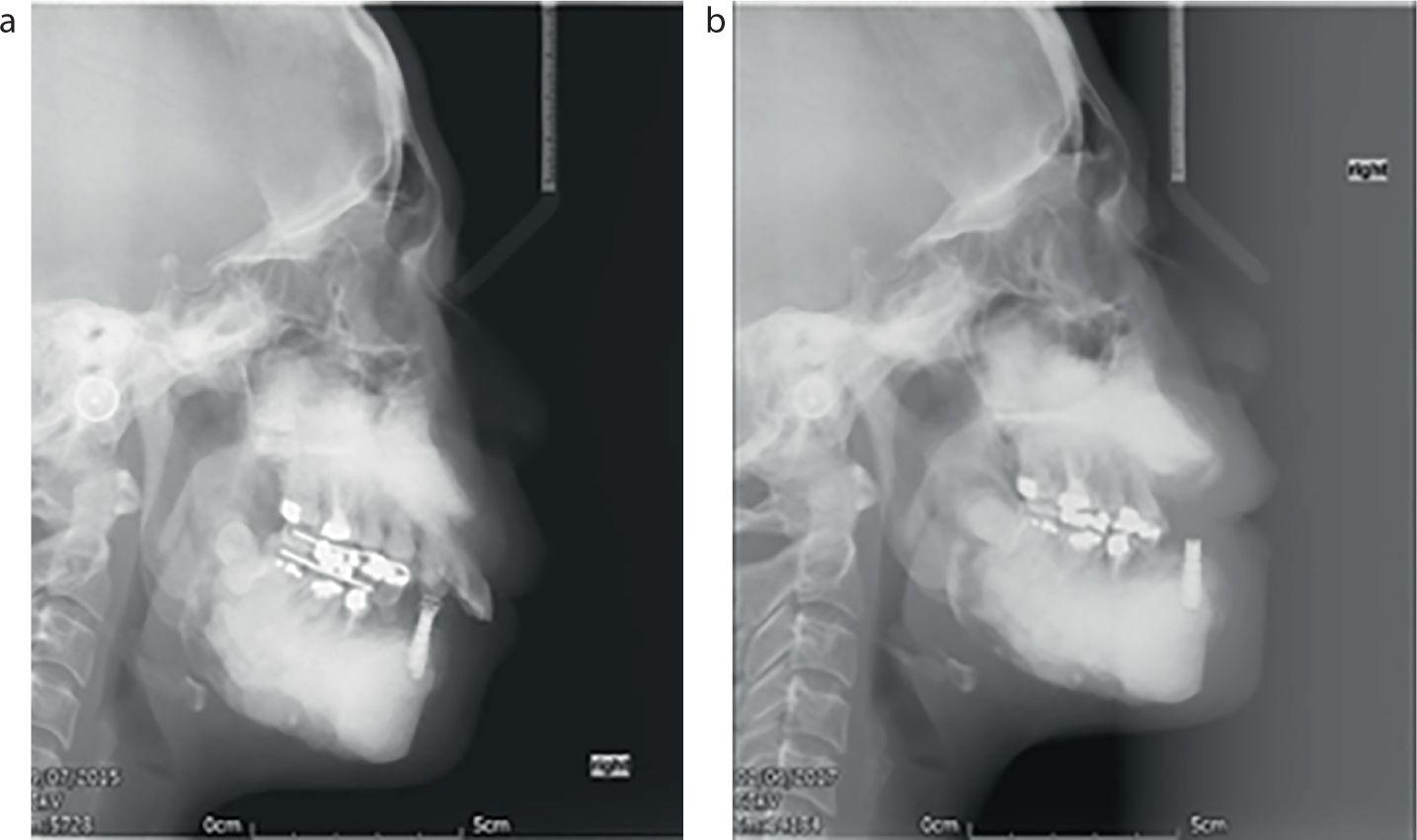
(a, b) Post-operative lateral cephalograms after implant placement: 2015 vs 2017.Figure 8.
(a-e) Pre- and post-operative images of patient after maxillary surgery and restorative rehabilitation in 2017.
As the dysplasia was seen to increase, and was most severe in the anterior segment, in 2012 the patient underwent resection of the dysplastic tissue in the anterior segments of the mandible. This led to the loss of her lower anterior teeth, shown in the patient's OPG from 2012 (Figure 2). After this, a provisional lower removable prosthesis was constructed, conforming to the occlusion. The patient struggled to wear this denture, even after multiple remakes.
In 2013, the bony overgrowth in the anterior mandible was propping the mouth open, causing trauma to the palate and bilateral open bites. The posterior mandibular teeth were becoming more lingually inclined. The patient could no longer wear her lower partial denture. The decision was made to undergo surgical recontouring of the edentulous anterior mandible. Post resection surgery, the restorative plan was construction of an onlay denture with consideration of anterior dental implants with locator attachments.
The onlay denture was planned to correct the angulation and increase the height of the posterior teeth. These posterior onlay components were planned to regain posterior contacts (close the remaining posterior open bites after surgery) and establish a more average overbite anteriorly. Due to the patient's anxiety about surgery and risks of treatment, she wanted to wait until she felt it totally necessary to undergo any surgery.
After the resection in 2013, a standard lower partial denture was constructed with posterior overlay to increase posterior contacts. Eighteen months later the patient was struggling with the retention and decided that she was ready to go forward with dental implant placement in the mandible. In 2015, two implants were placed in the lower canine regions to improve retention and stability of the removable onlay prosthesis. The implants placed in the mandible are still utilized today, with an onlay denture, but they appear to have a fibrous union in the bone which results in some movement. This is believed to be a result of the healing with fibrous bone, as can be seen in fibrous dysplasia.2 There is no soft tissue breakdown around the implants and they remain asymptomatic.
However, after review in 2016, the patient had noticed that the upper anterior teeth were starting to be pushed towards the lower teeth. This additional downward and outward growth had resulted in lip incompetence, making function very challenging. Clinical examination revealed further bony growth of the upper anterior arch. The UR123 and UL123 had also become periodontally compromised and were mobile. The patient underwent a bony resection of the dysplastic tissue UR3, UL3, including the incisors and canines. An upper immediate denture was provided and then a new partial denture was constructed after 3 weeks of healing. The patient was pleased with the aesthetic result and improved lip competence.
Following review in 2018, clinical and radiographic investigation had revealed further bony growth encroaching on the floor of the mouth, subjecting the patient to an increased airway risk. In May 2018, the patient had further surgery to debulk the fibrous lesions in her maxilla and mandible. Further investigation is planned due to extension of the lesion towards her optic nerve.
Discussion
Craniofacial involvement of fibrous dysplasia is reported in up to 50% of polyostotic cases. Symptoms can be minimal and patients commonly present with a cosmetic complaint. Presenting features of craniofacial fibrous dysplasia may include cranial asymmetry, facial deformity, nasal blockage, proptosis and visual impairment.
Treatment is indicated for those with impaired function or those who wish to improve aesthetics. There has been much debate over the ideal timing and extent of treatment, ie early vs late intervention and minimal vs radical resection.
General management for FD includes preventive orthopaedic procedures, such as curettage, internal fixation, and bone grafting. The main aim of these procedures is to manage the extent of the lesion and to treat any subsequent pathologic fractures in the affected areas.7 Complete resection of the affected bone is not usually achievable as lesions are commonly large and extensive, involving complex facial anatomy. In this case in particular, full resection was not possible due to the extension of the lesions into the condyles.
As fibrous dysplasia is associated with excess of osteoclastic activity with increased bone resorption, bisphosphonate therapy has been a logical treatment in some cases of FD affecting the femur and ribs.7 This has yielded positive results, indicating diminished pain, reduced fracture rate and bone pain, alongside radiographic resolution of fibrous dysplasia lesions.8 However, this management may not be possible for patients who have craniofacial fibrous dysplasia and require repeated surgery to resect growing lesions, as bisphosphonate therapy increases the risk of developing osteonecrosis of the jaw.9
Following resective surgery of the fibrous lesion, computer-aided design and computer-aided manufacturing (CAD/CAM) may become a viable method to regenerate jaw bone. Bone tissue regeneration is reliant on factors such as biocompatible patient-specific scaffolds and matrices, osteogenic cells and osteo-inductive and angio-inductive growth factors. CAD/CAM enables patient-specific scaffold and matrix manufacturing, which could replace the missing part of the jaw and allows osteogenic cells to generate bone accordingly. With further research and human studies, this may be a viable treatment option in future to replace fibrous tissue and regenerate bone in the craniofacial skeleton.10
Conclusion
Fibrous dysplasia can be a chronically debilitating condition, which requires extensive surgical and restorative rehabilitation. This case has demonstrated that, despite our best efforts, in extreme circumstances, conservative management may not be appropriate. This is a rare and severe case of fibrous dysplasia, which will require long-term maintenance and review. It is important that clinicians are aware of the clinical and radiographic appearance of FD, as well as the urgency for referral if appropriate, and to organize long-term follow-up for this cohort of patients. This patient was delighted with the aesthetic results of her treatment and, although a long road to recovery is ahead, all her original aesthetic and occlusal concerns had been addressed.