Philipsen H. Adenomatoid odontogenic tumour: facts and figures. Oral Oncol. 1999; 35:125-131
Handschel J, Depprich R, Zimmermann A, Braunstein S, Kübler N. Adenomatoid odontogenic tumor of the mandible: review of the literature and report of a rare case. Head Face Med. 2005; 1
Toida M, Hyodo I, Okuda T, Tatematsu N. Adenomatoid odontogenic tumor: report of two cases and survey of 126 cases in Japan. J Oral Maxillofac Surg. 1990; 48:404-408
WHO Classification of Head and Neck Tumours, 4th edn. In: El-Naggar A, Chan J, Grandis J, Takata T, Slootweg P (eds). : International Agency for Research on Cancer; 2017
Philipsen H, Samman N, Ormiston I, Wu P, Reichart P. Variants of the adenomatoid odontogenic tumor with a note on tumor origin. J Oral Pathol Med. 1992; 21:348-352
Mutalik V, Shreshtha A, Mutalik S, Radhakrishnan R. Adenomatoid odontogenic tumor: a unique report with histological diversity. J Oral Maxillofac Pathol. 2012; 16:118-121
Philipsen H, Reichart P, Nikai H. The Adenomatoid Odontogenic Tumour(AOT): an update. Oral Med Pathol. 1997; 2:55-60
Assael LA. Surgical management of odontogenic cysts and tumors. In: Peterson LJ, Indresano TA, Marciani RD, Roser SM (eds). Philadelphia: JB Lippincott; 1992
Garg D, Palaskar S, Shetty V, Bhushan A. Adenomatoid odontogenic tumor – hamartoma or true neoplasm: a case report. J Oral Sci. 2009; 51:155-159
More C, Das S, Gupta S, Bhavsar K. Mandibular adenomatoid odontogenic tumor: radiographic and pathologic correlation. J Nat Sci Biol Med. 2013; 4:457-462
The 2007 Recommendations of the International Commission on Radiological Protection.Elsevier: Annals of the ICRP 37;
1990 Recommendations of the International Commission on Radiological Protection. Sage Journals: Annals of the ICRP 21.
Motamedi M, Shafeie H, Azizi T. Salvage of an impacted canine associated with an adenomatoid odontogenic tumour: a case report. Br Dent J. 2005; 199:89-90
Unusual presentation of a tooth associated with an adenomatoid odontogenic tumour Nimit J Patel Simon Toms Fraser McDonald Joanna Johnson Louis McArdle Dental Update 2024 46:6, 707-709.
Authors
Nimit JPatel
BDS (Hons), MFDS, RCPS(Glas), PGCert(DentEd)
Paediatric Dentistry, Guy's and St Thomas' NHS Foundation Trust
Unilocular radiolucent lesions of the dental hard tissues can present regularly, however they are impossible to diagnose definitively without appropriate imaging and histopathology. A case is reported that involves a 14-year-old that presented with a history of an unerupted maxillary first premolar. An initial Dental Panoramic Tomograph (DPT) did not identify any localized opacities and was diagnosed as a dentigerous cyst. A Cone Bean Computed Tomogram (CBCT) identified calcified opacities resulting in a re-evaluated radiological interpretation. With the help of a multidisciplinary approach, the removal of the benign lesion allowed orthodontic traction to extrude the tooth and for it to be brought into alignment.
CPD/Clinical Relevance: This report highlights the importance of three-dimensional imaging as an adjunct to aid diagnosis and highlights the importance of multidisciplinary teams in the management of clinical challenges.
Article
Adenomatoid odontogenic tumours are benign, slow growing lesions and are more often found in the maxilla than the mandible in a ratio of 2.1:1.1, 2 The ratio of occurrence in males and females is skewed 1:1.9, however, certain Asian populations demonstrate the ratio as being 1:3.2.3 They often present in the second decade of life and, according to the WHO classification of odontogenic tumours, are primarily composed of odontogenic epithelium with ductal type structures.4 The lesion can present as three different variants (follicular, extrafollicular and peripheral) and radiographically are unilocular; with two-thirds of cases presenting with radio-opaque foci.5 Areas of the tumour can also appear cystic.6 Treatment for this type of tumour is enucleation or curettage: recurrence is reported to be rare, with only three cases highlighting reappearance.7 Dentigerous cysts present often as unilocular radiolucent lesions surrounding an unerupted tooth which starts at the cemento-enamel junction.8, 9
Case report
A 15-year-old African-Caribbean male patient presented, having been referred by his orthodontist regarding an unerupted upper left first premolar (UL4) to a joint orthodontic/oral surgery clinic. The orthodontist provided an initial DPT showing all adult teeth present (taken in 2013), a retained upper left first deciduous molar (ULD) and an unerupted UL4. The UL4 was associated with an enlarged follicle (approximately 4 mm between follicle and tooth, radiolucent and well-defined area). It spanned from the mesial of the UL5, to the mesial of the UL3. The lesion was unilocular and was around the cemento-enamel junction (CEJ) of the unerupted tooth. The orthodontist referred the patient back to the General Dental Practitioner (GDP) to remove the ULD under local anaesthetic. The UL4 went under review and had not erupted after reviewing after a 2-year period.
On examination, the patient presented with no abnormalities extra-orally or intra-orally, but the UL4 was palpable buccally. He was medically fit and well with no known drug allergies.
Special investigations included a new DPT (taken in 2015) (Figure 1) which showed the lesion surrounding the UL4 to be around the root of the tooth, as well as it being much larger. There was no root resorption associated with the adjacent teeth. A radiological report was sought and it was believed to be a dentigerous cyst.
Figure 1. DPT showing a large unilocular lesion associated with the UL4. It is well-defined, corticated and envelops the crown of the tooth.
Based on these findings, a CBCT of the left maxilla was carried out to determine the size and exact location of the lesion. The report confirmed a well-defined radiolucency enveloping the crown and extending up the mesial and palatal root surfaces. Within the radiolucency, numerous small focal radio-opacities were located. There was expansion and thinning of buccal and palatal plates, with no other pathology associated with the other teeth or sinus. A differential diagnosis was provided:
Adenomatoid odontogenic tumour;
Calcifying epithelial odontogenic cyst.
The patient and parents gave consent for a general anaesthetic to enucleate and curette the possible tumour and expose and bond the tooth to bring it into alignment.
A three-sided, full thickness, mucoperiosteal flap was raised buccally and palatally. The possible tumour was exposed revealing a mobile UL4 with a rosehead. The lesion was curetted and irrigated with saline. A gold chain and orthodontic bracket were bonded to the occlusal surface of the UL4 with composite, with the mucosal flaps being closed with resorbable sutures. The remnant chain was sutured to the mucosa with black silk.
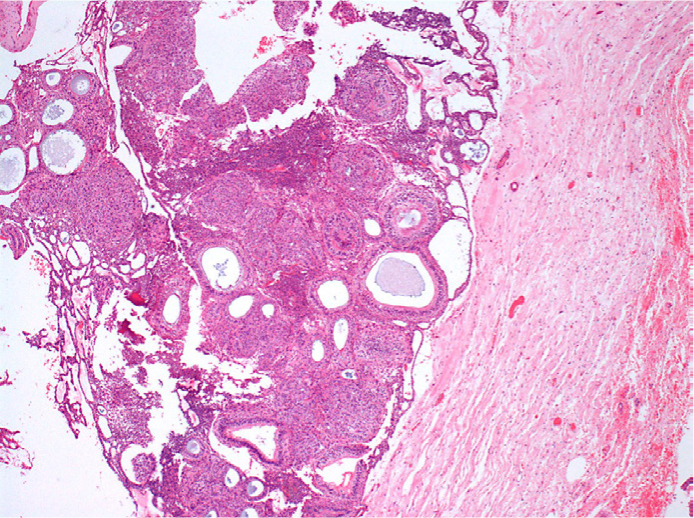
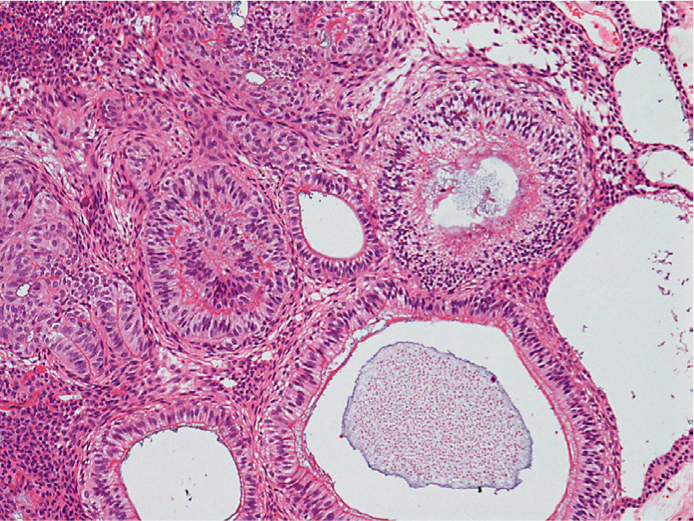
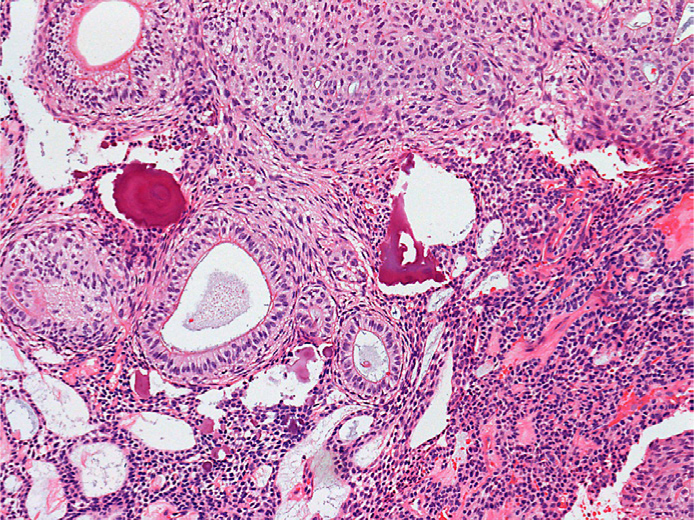
The specimen was reviewed histologically, revealing that, within the main cyst wall, there were clusters of islands of odontogenic epithelium some of which showed mineralization. The lesion itself presented with part solid and part cystic areas (Figure 2). Parts showed ductal structures with loosely cohesive epithelial cells (Figure 3) and areas of calcification, as well as epithelial cells in a whorl-like arrangement (Figure 4).
Figure 2. Part solid and part cystic areas are evident in this slice.Figure 3. Ductal structures are visible and there is also the presence of epithelial cells.Figure 4. Note the whorl-like arrangement associated with this lesion and areas of calcification.
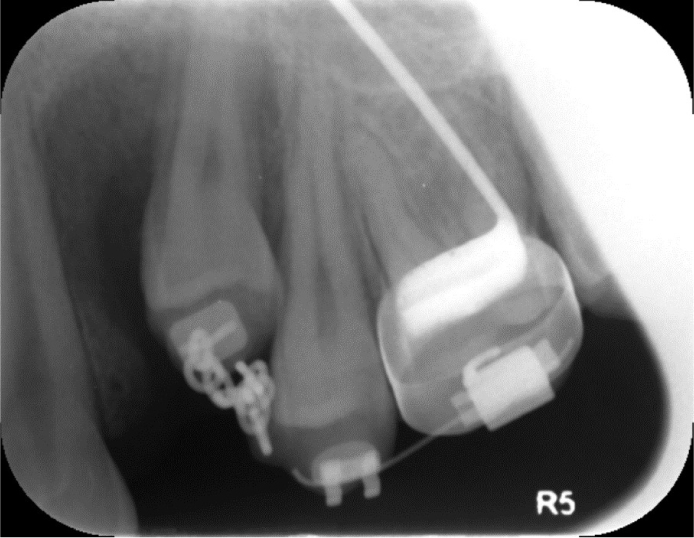
Following successful surgery, the patient was reviewed in the orthodontic department. A transpalatal arch with attachment for sectional fixed appliance for traction of UL4 was subsequently provided. He did not wish for alignment or adjustment of other teeth. The patient was reviewed regularly for periapical radiographs, as the tooth erupted buccally, and to assess for bony healing (Figure 5). The final occlusion consisted of Class I molars and canines, with some residual spacing. The patient was happy with the appearance and debond was arranged with an upper Essix retainer fitted on the same day.
Figure 5. Peri-apical radiograph (PA) showing movement of UL4 in relation to previous radiographs.
Discussion
This case demonstrates how important diagnosis (with the aid of appropriate special investigations) is to treatment planning. The initial DPT suggested that the most likely diagnosis was an enlarged follicle. An intra-oral radiograph may have revealed details such as internal calcifications. Use of CBCT scans are becoming more frequent in a multitude of scenarios, ranging from the association of wisdom teeth with the inferior dental nerve, to assessing and planning of implant restorations or, as in this case, the location and exact site of the UL4 and associated radiolucent lesion. Incidentally, finding the radio-opaque foci allowed the likely diagnosis to change from a dentigerous cyst to an adenomatoid odontogenic tumour or calcifying epithelial odontogenic cyst.
Adenomatoid odontogenic tumours can often be confused with dentigerous cysts, with two-thirds of cases being associated with an unerupted tooth.10, 11
Use of CBCT has its associated risks, with an increased radiation dose to patients. This can increase the chance of negative stochastic effects from occurring. With the use of SEDENTEXCT guidance, the risk coefficient in accordance with age for this patient is 11.4.12, 13 This coefficient takes into account the patient's age and is applied to the relative cancer and hereditable risk for stochastic effects in the population. This figure attempts to describe and estimate cancer incidence weighted for lethality and life impairment. However, the diagnostic yield is high and, for this patient, the calculated radiation dose is 40 μSv. This was on the basis of a 5 cm x 8 cm volume size, 90 kV, 3.0 mA and voxel size of 0.125 mm. Dose reduction measures were not undertaken. This equates to 5.4 days of background radiation in the UK.
The literature shows a low recurrence rate of the tumour, therefore we can be confident that curettage of the lesion and its removal is definitive. Salvaging an unerupted tooth such as this with orthodontic movement has been demonstrated previously.14 As a result, treatment planning, which included exposing and bonding the unerupted and mobile premolar, was well thought out and allowed the tooth to be saved.
The care for this patient included members from all aspects of the dental profession. A GDP, specialist and consultant orthodontists, a consultant oral surgeon, a consultant head and neck pathologist and consultant in dental and maxillofacial radiology. This demonstrates how a multidisciplinary approach to patient care can yield outstanding results.
One of the most interesting factors of this case is that the tooth was initially found to be mobile and, as a result, created some cause for concern. However, with successful bonding, the tooth successfully moved into the line of the arch. Radiographs taken demonstrated how good bony healing was achieved.
Conclusion
With the advent of three-dimensional imaging becoming readily available, when used appropriately and in accordance to guidance, it is now possible to have a better understanding of lesions of the dental hard tissues. In this case, the ability of clinicians demonstrated how a tooth with questionable prognosis could be saved and provide a pleasing and aesthetic end result for the patient.