Petrikowski CG, Peters E. Longitudinal radiographic assessment of dense bone islands of the jaws. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997; 83:627-634
McDonnell D. Dense bone island: a review of 107 patients. Oral Surg Oral Med Oral Pathol. 1993; 76:124-128
Eversole LR, Stone CE, Strub D. Focal sclerosing osteomyelitis/focal periapical osteopetrosis: radiographic patterns. Oral Surg Oral Med Oral Pathol. 1984; 58:456-460
White SC, Pharoah MJ. Oral Radiology: Principles and Interpretation.Oxford: Elsevier Health Sciences; 2014
Ternent CA, Thorson AG. BMJ Best Practice Familial Adenomatous Polyposis Syndromes. BMJ. 2016;
Is stroke care improving? The second SSNAP Annual Report.London: HQIP; 2015
Wyman RA, Fraizer MC, Keevil JG, Busse KL, Aeschlimann SE, Korcarz CE Ultrasound-detected carotid plaque as a screening tool for advanced subclinical atherosclerosis. Am Heart J. 2005; 150:1081-1085
Friedlander AH, Lande A. Panoramic radiographic identification of carotid arterial plaques. Oral Surg Oral Med Oral Pathol. 1981; 52:102-104
Friedlander AH, Baker JD. Panoramic radiography: an aid in detecting patients at risk of cerebrovascular accident. J Am Dent Assoc. 1994; 125:1598-1603
Carter LC, Haller AD, Nadarajah V, Calamel AD, Aguirre A. Use of panoramic radiography among an ambulatory dental population to detect patients at risk of stroke. J Am Dent Assoc. 1997; 128:977-984
Cohen SN, Friedlander AH, Jolly DA, Date L. Carotid calcification on panoramic radiographs: an important marker for vascular risk. Oral Surg Oral Med Oral Pathol Oral Radiol Endodont. 2002; 94:510-514
Doris I, Dobranowski J, Franchetto AA, Jaeschke R. The relevance of detecting carotid artery calcification on plain radiograph. Stroke. 1993; 24:1330-1334
Friedlander AH, Manesh F, Wasterlain CG. Prevalence of detectable carotid artery calcifications on panoramic radiographs of recent stroke victims. Oral Surg Oral Med Oral Pathol. 1994; 77:669-673
Khosropanah SH, Shahidi SH, Bronoosh P, Rasekhi A. Evaluation of carotid calcification detected using panoramic radiography and carotid Doppler sonography in patients with and without coronary artery disease. Br Dent J. 2009; 207
Horner K, Eaton K. Selection Criteria for Dental Radiography, 3rd edn. : FGDP; 2013
Sakhaee K, Chan Jr AVC. BMJ Best Practice Osteoporosis.: BMJ; 2016
Jonasson G, Alstad T, Vahedi F, Bosaeus I, Lissner L, Hakeberg M. Trabecular pattern in the mandible as bone fracture predictor. Oral Surg Oral Med Oral Pathol Oral Radiol Endodont. 2009; 108:e42-51
Horner K, Devlin H, Harvey L. Detecting patients with low skeletal bone mass. J Dent. 2002; 30:171-175
Lee K, Taguchi A, Ishii K, Suei Y, Fujita M, Nakamoto T Visual assessment of the mandibular cortex on panoramic radiographs to identify postmenopausal women with low bone mineral densities. Oral Surg Oral Med Oral Pathol Oral Radiol Endodont. 2005; 100:226-231
Damilakis J, Vlasiadis K. Have panoramic indices the power to identify women with low BMD at the axial skeleton?. Phys Medica. 2011; 27:39-43
Taguchi A, Tsuda M, Ohtsuka M, Kodama I, Sanada M, Nakamoto T Use of dental panoramic radiographs in identifying younger postmenopausal women with osteoporosis. Osteoporos Int. 2006; 17:387-394
Devlin H. Identification of the risk for osteoporosis in dental patients. Dent Clin North Am. 2012; 56:847-861
Arifin AZ, Asano A, Taguchi A, Nakamoto T, Ohtsuka M, Tsuda M Computer-aided system for measuring the mandibular cortical width on dental panoramic radiographs in identifying postmenopausal women with low bone mineral density. Osteoporos Int. 2006; 17:753-759
Muramatsu C, Matsumoto T, Hayashi T, Hara T, Katsumata A, Zhou X Automated measurement of mandibular cortical width on dental panoramic radiographs. Int J Comput Assist Radiol Surg. 2013; 8:877-885
Devlin H, Allen PD, Graham J, Jacobs R, Karayianni K, Lindh C Automated osteoporosis risk assessment by dentists: a new pathway to diagnosis. Bone. 2007; 40:835-842
Kavitha MS, An SY, An CH, Huh KH, Yi WJ, Heo MS Texture analysis of mandibular cortical bone on digital dental panoramic radiographs for the diagnosis of osteoporosis in Korean women. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015; 119:346-356
Horner K, Allen P, Graham J, Jacobs R, Boonen S, Pavitt S The relationship between the OSTEODENT index and hip fracture risk assessment using FRAX. Oral Surg Oral Med Oral Pathol Oral Radiol Endodont. 2010; 110:243-249
All relevant ‘dental’ radiographic anomalies require a report, be they related to the teeth, mandible, maxillary sinuses, temporomandibular joints or soft tissues. However, non-dental incidental findings are often present on dental radiographs, some of which may be due to systemic disease: these should also be assessed. We compare the confidence at diagnosing, and subsequent management of, three such incidental findings between specialist dental and maxillofacial radiologists and recently qualified dentists. The imaging features and clinical implications of dense bone islands, carotid artery calcification and osteoporosis are described.
CPD/Clinical Relevance: Dental panoramic radiographs cover structures not confined to the tooth-bearing areas and incidental findings in these regions should be recognized and appropriately reported, in line with IR(ME)R legislation.
Article
Dental panoramic tomograms (DPTs) are widely used to support dental treatment. The DPT image is not confined to the tooth-bearing area and includes the surrounding anatomical structures, including the mandibular and maxillary bone and the soft tissue structures of the neck. Incidental findings not related to the ‘dentition’ may be detected and, under IR(ME)R legislation, should be recorded in the radiographic report. In the last few years, it has been suggested that three such incidental findings may have implications in systemic disease, such as dense bone islands (DBI), carotid artery calcification (CAC) and osteoporosis, could be picked up by the dentist from DPTs taken for other reasons. Dense bone islands have been implicated in Gardner's syndrome (multiple osteomas and polyposis coli), carotid artery calcification in increased risk of stroke, and osteoporosis in increased risk of fractures. The authors are aware that clinicians can struggle to identify findings not related to the dentition reliably, and that most of the publications have been in specialist dentomaxillofacial journals. They therefore wanted to compare the confidence of diagnosis of such lesions between specialist dental radiologists and newly qualified dentists and to see whether there were differences in their subsequent recommendation of management of the patient so that areas where specific training needs were required could be identified.
Procedure
A written survey was sent to all qualified dental and maxillofacial radiologists working in dental hospitals in the UK. They were asked to grade how confident they were in diagnosing dense bone islands, carotid artery calcification and osteoporosis from DPTs on a scale of very confident, quite confident or not confident. For each of these conditions, participants were also asked whether they would inform the referring clinician of the incidental finding in a comments box.
A similar questionnaire was given in person to a group of newly qualified dentists (up to 3 years post qualification) attending a regional DCT study day. They were asked to grade their confidence in identifying the three incidental findings, using the same scale, and to state whether they would inform the patient after reporting the radiograph.
All the results were reviewed by the authors who combined the results and took into consideration the comments given by some respondents.
Interpretation
Sixteen dental and maxillofacial radiologists and 39 newly qualified dentists responded to the questionnaire, encompassing nearly all the radiologists and a proportion of regional newly qualified dentists. All specialists were confident in diagnosing dense bone islands and would record the incidental finding in their report. The majority would only consider Gardner's syndrome in the presence of more than five lesions. There was divided opinion on informing the referring clinician, with half of the specialists responding that they would raise the possibility of Gardner's syndrome, when five or more lesions are present. Over half (55%) of the newly qualified dentists were confident in diagnosing DBI. The majority (77%) would consider Gardner's syndrome and subsequently inform the patient.
Almost all (15 of 16) of the specialists were very or somewhat confident in diagnosing CAC on a DPT. Opinion was mixed as to whether or not the referring clinician ought to be informed, with 5 of the 16 saying that they would not alert the clinician. Most (92%) of newly qualified dentists were not confident in diagnosing CAC, but three-quarters would inform the patient if they did recognize the incidental finding.
Similar to CAC, almost all (15 of 16) of the specialists were at least somewhat confident at diagnosing osteoporosis, and half would alert the referring clinician. In contrast, no recently qualified dentists were very confident, and only 23% were somewhat confident at identifying signs of osteoporosis on a DPT. Three-quarters, however, would make the patient aware of the diagnosis.
Discussion
Dense bone islands
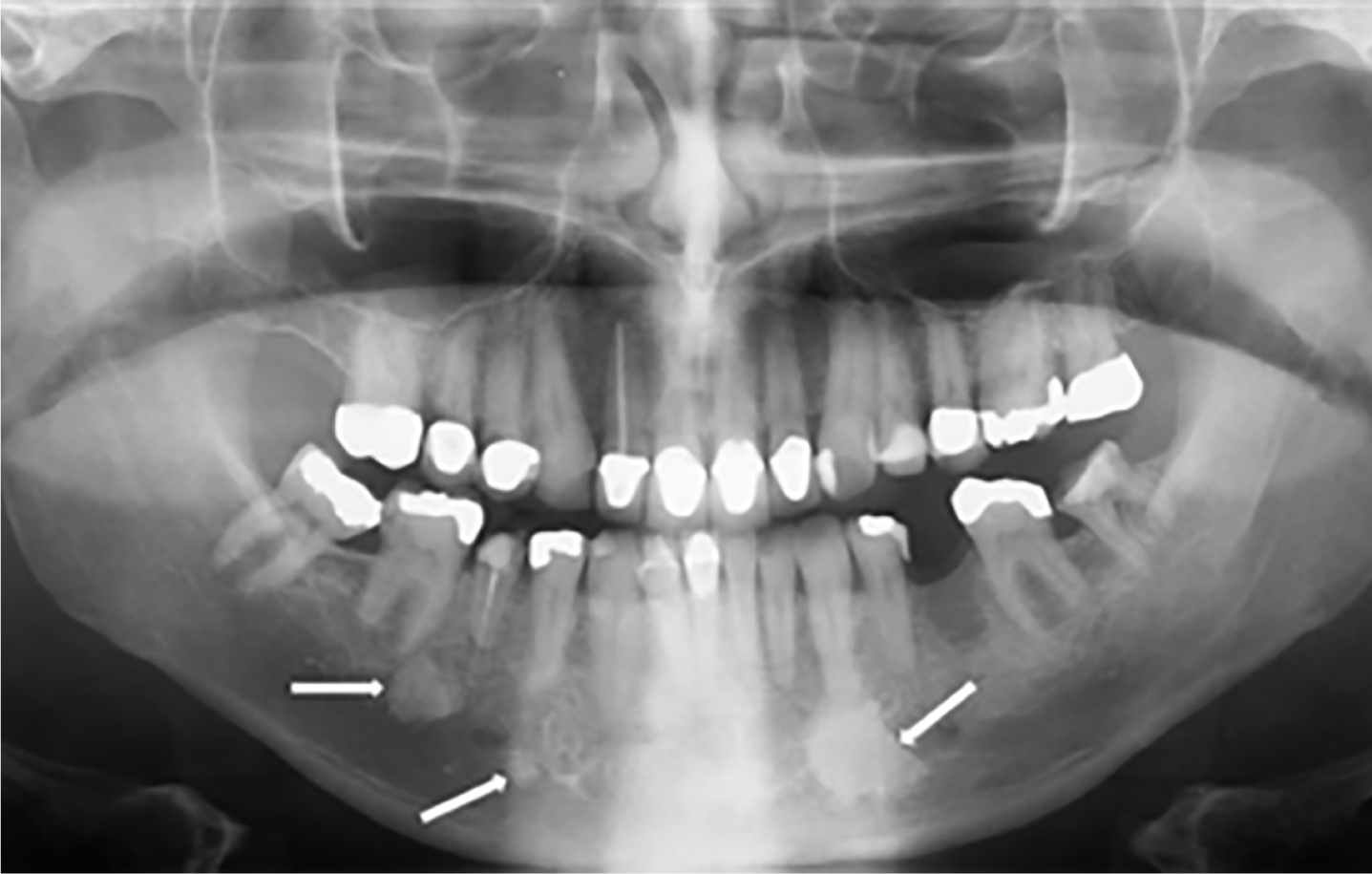
Dense bone islands are localized growths of compact cortical bone that develop within cancellous bone, and are of unknown aetiology. DBIs are often noted as incidental findings due to their asymptomatic nature. They are more common in the mandible, particularly in the premolar or molar region, with an incidence of 2.3–9.7%.1, 2 Radiographically, these appear as well-defined, homogeneous radio-opacities within normal bone. An example of dense bone islands on a DPT is seen in Figure 1. Root resorption associated with dense bone islands located periapical to teeth has been reported, however, it is usually self-limiting and the teeth remain vital.3, 4 Dense bone islands do not normally require treatment or intervention.
Figure 1. Dental panoramic demonstrating bone islands in the mandible (arrows). If more than five dense bone islands are seen, Gardner's syndrome should be considered.
If more than five dense bone islands are identified, it is important to consider Gardner's syndrome: a clinical variant of familial adenomatous polyposis (FAP).2 FAP is an autosomal dominant condition with an incidence at birth of 1 in 10,000 and is characterized by the development of multiple colorectal adenomas.5 Affected individuals are at almost 100% risk of colorectal cancer by the age of 40, if colectomy is not performed prophylactically. Gardner's syndrome is a rare variant of FAP which, in addition to colorectal adenomas, has extra-intestinal features, including dense bone islands, osteomas, supernumerary teeth and epidermoid cysts.
Our survey revealed that all of the specialists were confident at diagnosing dense bone islands. In line with the few recommendations that exist in the literature, the majority only considered Gardner's syndrome in cases of five or more DBIs. There is disparity amongst the newly qualified dentists where just over half were confident in diagnosis but more than half would have considered Gardner's and informed the patient. What is a little concerning is that nearly half were not confident in diagnosing DBIs, which are a relatively common incidental finding.
In summary, dense bone islands are largely asymptomatic incidental findings rarely necessitating intervention. If multiple islands are noted, patients' family history should be reviewed and consideration of referral to their GP. There would appear to be further training required in their identification.
Carotid artery calcification
Carotid artery calcification (CAC) may be related to significant stenosis of the arterial lumen, which has been shown to be a positive predictor for ischaemic events, including stroke. The incidence of stroke is estimated to be approximately 100,000 per year.6 Stroke is the fourth leading cause of death within the UK. Clinical factors contribute to the risk of stroke and these are outlined in Table 1.
Older age
Male sex
African-American or Hispanic ancestry
Family history of stroke
History of ischaemic stroke
HTN
Smoking
Diabetes mellitus
Atrial fibrillation
Co-morbid cardiac conditions
Carotid artery stenosis
Sickle cell disease
Atherosclerotic plaque formation is a process where fatty deposits, cholesterol, calcium and platelets are deposited within the arterial lumen lining. Over time, these plaques may calcify, leading to obstruction of the luminal wall which subsequently can lead to compromised blood flow. Early detection and preventive measures, such as reduction of risk factors with lifestyle changes and pharmacological therapy, is critical in order to reduce the likelihood of vascular events. Duplex ultrasound sonography is the most commonly used non-invasive gold standard for identification of the presence of atherosclerotic plaques.7 In this technique, using soundwaves, a greyscale image demonstrates anatomy, whilst flow within vessels is displayed in colour. It is generally only used in the UK if there have been relevant signs and symptoms.
Carotid artery calcifications can appear as heterogeneous radio-opaque masses which may look linear and are commonly situated inferior to the mandibular angle and adjacent to the third and fourth cervical vertebrae, near the hyoid bone (Figure 2). Calcification in the carotid arteries has been seen in up to 4% of neurologically asymptomatic patients over 55 years of age.8, 9, 10 Cohen et al conducted a retrospective review to determine whether CAC can predict increased risk of future ischaemic events, such as myocardial infarction, angina, stroke or transient ischaemic attack.11 During the follow-up period (mean 3.6 years), 41% of patients with carotid artery calcification proceeded to have at least one ischaemic event, with 15% mortality rate. Doris et al demonstrated fair correlation between CAC on a plain radiograph of the neck and clinically significant carotid artery stenosis was assessed by intravenous angiography.12 As a result of this, and similar evidence, some authors have advised managing CAC findings with prompt referral to relevant medical teams for vascular assessment and treatment.8, 13
Figure 2. Cropped panoramic showing carotid artery calcification as radio-opacities in the right neck (arrow) at the level of C4.
Conversely, Khosropanah et al demonstrated relatively low sensitivity rates (50%) in identification of carotid artery calcifications on panoramic radiographs in patients with normal duplex ultrasound.14 As the correlation between these two imaging methods is relatively weak, the authors concluded that DPTs are not an accurate diagnostic measure and should not be used as an independent screening tool. Consistent with this recommendation, the FGDP Selection Criteria guidelines for prescription of panoramic radiographs do not recommend their use as a screening tool, including for CAC.15 The Royal College of Radiologists do not recommend any imaging for routine screening of asymptomatic patients for assessment of cardiovascular risk.16
Whilst the majority of specialists were somewhat confident in identification of CAC on DPTs, the majority of newly qualified dentists were not. If some specialists find it difficult to diagnose CAC, then it cannot be expected that general dental practitioners will be confident in the diagnosis of this incidental finding. On balance, with the difficulty of diagnosis and poor sensitivity rates, it is not practical to investigate all patients with carotid artery calcification on DPTs.
Osteoporosis
Osteoporosis is a metabolic disorder in which bone mineral density (BMD) decreases below a defined normal limit. Primary osteoporosis, where no identifiable cause is demonstrated, is generally seen in postmenopausal women and the elderly. Secondary osteoporosis can be related to a range of causes, such as nutritional deficiencies, inactivity or corticosteroid use. Strong clinical risk factors for osteoporosis are detailed in Table 2.
Female gender
Maternal history of fragility fracture/osteoporosis
Older age
Post-menopause or secondary amenorrhea
Low body mass index or body weight
Corticosteroid use
Smoking
Excessive alcohol use
Prolonged immobilization
Low calcium intake
Vitamin D deficiency
Dual energy X-ray absorptiometry (DXA) is considered the standard measurement of BMD.17 By using two x-ray beams with different energies, absorption by the soft tissues can be subtracted and the bone density determined. Decreasing bone density is commonly asymptomatic, but affected bones become increasingly fragile and prone to fracture. The increased risk of hip fracture in osteoporotic individuals is of particular consideration, with its 20% risk of mortality within a year.18 First-line management of osteoporosis is with bisphosphonates, particularly in post-menopausal women. Bisphosphonates have been shown to reduce the risk of further fracture in individuals with a history of fragility fracture, ie fractures which have occurred as a result of low-level trauma, such as a fall from standing height.19
Plain radiographic appearances are those of decreased bone density, seen as a reduction in bone opacity (Figure 3). The teeth are unaffected by osteoporosis, so within the jaws they can be used as a reference for comparison of bone density.4 Sparse cancellous bone pattern in the mandibular premolar region has been shown to be associated with an increased number of self-reported fragility fractures.20
Figure 3. Cropped panoramic showing decreased bone density in osteoporosis. Note thinning of the inferior cortex of the mandible (arrow) compared with a normal cortex seen in Figure 1. Note the irregularity of the cortex with an increase in Haversian canals.
Reduced width of the inferior cortex of the mandible in at risk patients can assist identification of affected individuals.21, 22, 23, 24 The measurement is taken below the mental foramen. Horner et al reported using a threshold of 3 mm for the mandibular cortical width (MCW), which gave a low sensitivity but high specificity (8% and 98.7%, respectively) with low BMD, determined by DXA of the femur or spine.21 Using a higher threshold enables greater detection of cases of asymptomatic osteoporosis, however, this increases the risk of over-investigation of unaffected individuals.25
A subjective index of erosion of the mandibular cortex, termed the mandibular cortical index (MCI), makes use of the increase of Haversian canals in the mandibular cortex in osteoporosis. Haversian canals are seen as black lines within the cortex, parallel to the inferior border of the mandible.17 The MCI assesses the integrity of the inferior cortex between the mental foramen and the antegonial region. The cortex is graded as normal, mild to moderately eroded, or severely eroded (when the cortex is clearly porous). Evidence is mixed as to the usefulness of MCI in the assessment of osteoporosis risk and it has been noted that intra- and inter-observer agreement may not be sufficient in the absence of specialist radiology training.
The increased use of digital radiography in dentistry has aided the development of computer-aided diagnosis (CAD) tools in the assessment of osteoporosis on DPT. CAD systems can automatically measure the MCW, and analyse the texture of the inferior cortex of the mandible.26, 27, 28, 29 By combining these tools, CAD has the potential to increase ease and reliability of assessment of osteoporosis risk in general dental practice.
Dental panoramics can be used to identify individuals at increased risk of osteoporosis and, as a result, may improve the prevention of hip fractures, with their associated morbidity.30 As their accuracy is not 100%, it is not recommended that they are taken with the sole purpose of osteoporosis diagnosis. However, identification of the imaging features of high risk individuals on dental imaging taken for other purposes is important.25 If imaging features are suggestive of osteoporosis, with clinical risk factors identified in the medical and social history, referral to the general medical practitioner for assessment may be appropriate.
Only half of the specialists were somewhat confident in the diagnosis of osteoporosis and the majority of newly qualified dentists were not confident. The future adoption of CAD technologies may address this lack of confidence.
Conclusion
The three incidental findings considered in this study have different implications for ongoing management. In the case of dense bone islands, which are a common finding, no further management is indicated unless there are five or more, in which case Gardner's syndrome should be considered. Carotid artery calcifications visible on DPTs are uncommon. There is no convincing evidence to support further investigations in the absence of ischaemic symptoms. DPTs can be used to identify patients at risk of osteoporosis and in the presence of other risk factors referral to the GMP may be appropriate.
Dense bone islands, in particular, are a common incidental finding and the lack of confidence in their diagnosis by newly qualified dentists indicates a training need. Lack of agreement in specialist opinion suggests, however, that diagnosis of CAC and osteoporosis on DPTs is difficult and may be beyond the scope of a general dental practitioner.
In conclusion, the clinician should be able to identify, report on and be aware of the clinical implications of radiographic findings. When in doubt, it is important to refer to a specialist.