Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations. Int J Oral Maxillofac Implants. 2004; 19:43-61
Dawson A, Chen S, Buser D, Cordaro L, Martin W, Belser U. The SAC Classification in Implant Dentistry.: Quintessence Publishing Co Ltd; 2009
Pjetursson BE, Brägger U, Lang NP. Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clin Oral Implants Res. 2007; 18:97-113
Buser D, von Arx T, ten Bruggenkate CM, Weingart D. Basic surgical principles with ITI implants. Clin Oral Implants Res. 2000; 11:59-68
Morton D, Chen ST, Martin WC. Consensus statements and recommended clinical procedures regarding optimizing esthetic outcomes in implant dentistry. Int J Oral Maxillofac Implants. 2014; 29:216-220
Chen S, Buser D. Implants in post-extraction sites: a literature update. In: Buser D, Belser U, Wismeijer D (eds). Berlin: Quintessence; 2008
Schropp L, Isidor F. Timing of implant placement relative to tooth extraction. J Oral Rehabil. 2008; 35:33-43
Chen ST, Buser D. Clinical and esthetic outcomes of implants placed in post-extraction sites. Int J Oral Maxillofac Implants. 2009; 24:186-217
Araujo MG, Sukekava F, Wennstrom JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. J Clin Periodontol. 2005; 32:645-652
Chen ST, Buser D. Clinical and esthetic outcomes of implants placed in post-extraction sites. Int J Oral Maxillofac Implants. 2009; 24:186-217
Chen ST, Beagle J, Jensen SS, Chiapasco M, Darby I. Consensus statements and recommended clinical procedures regarding surgical techniques. Int J Oral Maxillofac Implants. 2009; 24:272-278
Chen ST, Wilson TG, Hämmerle CH. Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes. Int J Oral Maxillofac Implants. 2004; 19:12-25
Hämmerle CH, Chen ST, Wilson TG Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int J Oral Maxillofac Implants. 2004; 19:26-28
Glossary of Oral and Maxillofacial Implants. In: Laney WR (ed). Berlin: Quintessence; 2007
Buser D, Chappuis V, Bornstein MM, Wittneben JG, Frei M, Belser UC. Long-term stability of contour augmentation with early implant placement following single tooth extraction in the esthetic zone: a prospective, cross-sectional study in 41 patients with a 5–to 9–year follow-up. J Periodontol. 2013; 84:1517-1527
Chiapasco M, Casentini P, Zaniboni M. Bone augmentation procedures in implant dentistry. Int J Oral Maxillofac Implants. 2009; 24:237-259
Jensen SS, Terheyden H. Bone augmentation procedures in localized defects in the alveolar ridge: clinical results with different bone grafts and bone-substitute materials. Int J Oral Maxillofac Implants. 2009; 24:218-236
Sailer I, Mühlemann S, Zwahlen M. Cemented and screw-retained implant reconstructions: a systematic review of the survival and complication rates. Clin Oral Implants Res. 2012; 23:163-201
Wismeijer D, Brägger U, Evans C, Kapos T, Kelly JR, Millen C Consensus statements and recommended clinical procedures regarding restorative materials and techniques for implant dentistry. Int J Oral Maxillofac Implants. 2014; 29:137-140
Weber HP, Kim DM, Ng MW. Peri-implant soft-tissue health surrounding cement- and screw-retained implant restorations: a multi-center, 3-year prospective study. Clin Oral Implants Res. 2006; 17:375-379
Wilson TG. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 2009; 80:1388-1392
Chee WW, Duncan J, Afshar M, Moshaverinia A. Evaluation of the amount of excess cement around the margins of cement-retained dental implant restorations: the effect of the cement application method. J Prosthet Dent. 2013; 109:216-221
Weber HP, Sukotjo C. Does the type of implant prosthesis affect outcomes in the partially edentulous patient?. Int J Oral Maxillofac Implants. 2007; 22:140-172
Keenan AV, Levenson D. Are ceramic and metal implant abutments performance similar?. Evid Based Dent. 2010; 11:68-69
Sailer I, Philipp A, Zembic A, Pjetursson BE, Hämmerle CH, Zwahlen M. A systematic review of the performance of ceramic and metal implant abutments supporting fixed implant reconstructions. Clin Oral Implants Res. 2009; 20:4-31
Zembic A, Bösch A, Jung RE, Hämmerle CH, Sailer I. Five-year results of a randomized controlled clinical trial comparing zirconia and titanium abutments supporting single-implant crowns in canine and posterior regions. Clin Oral Implants Res. 2013; 24:384-390
van Brakel R, Meijer GJ, Verhoeven JW, Jansen J, de Putter C, Cune MS. Soft tissue response to zirconia and titanium implant abutments: an in vivo within-subject comparison. J Clin Periodontol. 2012; 39:995-1001
Zembic A, Kim S, Zwahlen M, Kelly JR. Systematic review of the survival rate and incidence of biologic, technical, and esthetic complications of single implant abutments supporting fixed prostheses. Int J Oral Maxillofac Implants. 2014; 29:99-116
Larsson C, Wennerberg A. The clinical success of zirconia-based crowns: a systematic review. Int J Prosthodont. 2014; 27:33-43
Slot W, Raghoebar GM, Vissink A, Huddleston Slater JJ, Meijer HJ. A systematic review of implant-supported maxillary overdentures after a mean observation period of at least 1 year. J Clin Periodontol. 2010; 37:98-110
Raghoebar GM, Meijer HJ, Slot W, Slater JJ, Vissink A. A systematic review of implant-supported overdentures in the edentulous maxilla, compared to the mandible: how many implants?. Eur J Oral Implantol. 2014; 7:191-201
Feine JS, Carlsson GE, Awad MA, Chehade A, Duncan WJ, Gizani S, Head T, Heydecke G, Lund JP, MacEntee M, Mericske-Stern R, Mojon P, Morais JA, Naert I, Payne AG, Penrod J, Stoker GT, Tawse-Smith A, Taylor TD, Thomason JM, Thomson WM, Wismeijer D. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Gerodontology. 2002; 19:3-4
Thomason JM, Feine J, Exley C, Moynihan P, Müller F, Naert I, Ellis JS, Barclay C, Butterworth C, Scott B, Lynch C, Stewardson D, Smith P, Welfare R, Hyde P, McAndrew R, Fenlon M, Barclay S, Barker D. Mandibular two implant-supported overdentures as the first choice standard of care for edentulous patients--the York Consensus Statement. Br Dent J. 2009; 207:185-186
Rentsch-Kollar A, Huber S, Mericske-Stern R. Mandibular implant overdentures followed for over 10 years: patient compliance and prosthetic maintenance. Int J Prosthodont. 2010; 23:91-98
Cehreli MC, Karasoy D, Kokat AM, Akca K, Eckert SE. Systematic review of prosthetic maintenance requirements for implant-supported overdentures. Int J Oral Maxillofac Implants. 2010; 25:163-180
Martin W, Lewis E, Nicol A. Local risk factors for implant therapy. Int J Oral Maxillofac Implants. 2009; 24:28-38
Salvi GE, Brägger U. Mechanical and technical risks in implant therapy. Int J Oral Maxillofac Implants. 2009; 24:69-85
Cochran DL, Schou S, Heitz-Mayfield LJ, Bornstein MM, Salvi GE, Martin WC. Consensus statements and recommended clinical procedures regarding risk factors in implant therapy. Int J Oral Maxillofac Implants. 2009; 24:86-89
Krennmair G, Krainhöfner M, Piehslinger E. The influence of bar design (round versus milled bar) on prosthodontic maintenance of mandibular overdentures supported by 4 implants: a 5-year prospective study. Int J Prosthodont. 2008; 21:514-520
Pjetursson BE, Asgeirsson AG, Zwahlen M, Sailer I. Improvements in implant dentistry over the last decade: comparison of survival and complication rates in older and newer publications. Int J Oral Maxillofac Implants. 2014; 29:308-324
Pjetursson BE, Lang NP. Prosthetic treatment planning on the basis of scientific evidence. J Oral Rehabil. 2008; 35:72-79
A guide to implant dentistry part 2: surgical and prosthodontic considerations Despoina Chatzistavrianou Paul HR Wilson Philip Taylor Dental Update 2024 46:6, 707-709.
Authors
DespoinaChatzistavrianou
DDS MFDS RCSEd, MClinDent Pro, MPros RCSEd
Specialist in Prosthodontics, Specialty Registrar in Restorative Dentistry, Birmingham Dental Hospital and University of Birmingham School of Dentistry, Birmingham Community Healthcare NHS Trust, Birmingham, UK
Senior Lecturer and Honorary Consultant in Restorative Dentistry, The Royal London Dental Hospital and Queen Mary University of London, Barts and the London School of Medicine and Dentistry, London, UK
Implant rehabilitation is a successful treatment modality for the replacement of missing teeth, but careful treatment planning, restoratively-driven implant placement and individualized maintenance are prerequisites for success in order to control and minimize technical and biologic complications. The first part of the series focused on new patient assessment and pre-operative planning. The second part of the series will discuss the surgical and prosthodontic considerations and maintenance of implant-supported restorations.
CPD/Clinical Relevance: To provide the dental practitioner with an evidence-based overview regarding treatment planning, surgical and prosthodontic considerations and maintenance of implant-supported restorations.
Article
Replacement of missing teeth with implant-supported prostheses is a challenging process and each case presents different degrees of complexity and surgical, restorative and aesthetic risk factors.1, 2 Although implant reconstructions offer high survival rates, their complication rate and level of maintenance are high as well.3 The first part of the series focused on new patient assessment regarding general and local factors that affect the case complexity and pre-operative planning. The second part of the series will discuss the surgical and prosthodontic considerations and maintenance of implant-supported restorations, equally important factors to their long-term success.
Surgical considerations
Successful implant rehabilitation requires careful surgical manipulation which will take into consideration anatomic structures and will follow a strict surgical protocol regarding drill sequence and an aseptic technique.4 Each case will have a different degree of surgical complexity depending on the site (aesthetic versus non-aesthetic), the number of missing teeth and the soft and hard tissue deficiencies (Table 1).2
Simple
Advanced
Complex
Sites without bone defects
Edentulous mandible with 2 implants for a removable denture (ball attachment or bar)
Distal-extension situation maxilla/mandible
Extended edentulous gap in posterior maxilla/mandible
Extended edentulous gap in anterior mandible
Single-tooth gap in posterior area
Single-tooth gap in anterior mandible
Edentulous mandible with 4 to 6 implants for a bar-supported prothesis or full-arch prosthesis
Edentulous maxilla for removable denture
Single-tooth gap in anterior maxilla
Extended edentulous gap in anterior maxilla
Edentulous maxilla for a fixed full-arch prosthesis
Sites with bone defects
None
Implants with simultaneous membrane application
Implants placed with osteotome technique
Implants combined with ‘bone splitting’ of the alveolar crest
All 2-stage bone augmentation procedures
Sinus floor elevation with the window technique
Combined bone and soft tissue augmentation procedures
(Classification of the Swiss Society of Oral Implantology, 1999)
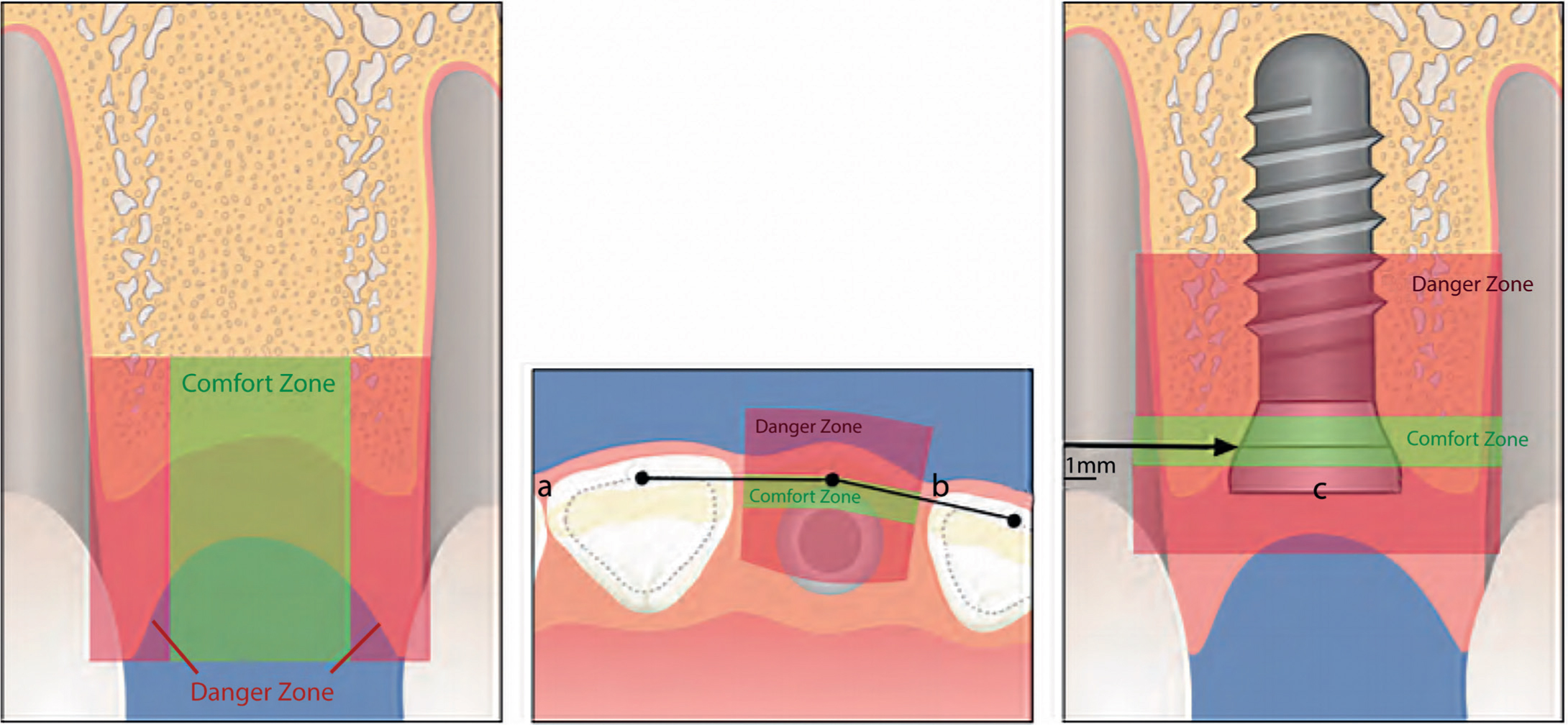
A surgical guide is advisable to facilitate a restoratively-driven implant placement; fixtures should be positioned in the correct three-dimensional position to achieve an optimum emergence profile (Figure 1).4 The correct type of implant should also be selected for a favourable emergence profile; narrow neck implants are used for maxillary lateral incisors and mandibular incisors, standard-neck implants are used for maxillary central incisors, canines and premolar teeth and wide-neck configuration for replacement of molar teeth.1, 5
Figure 1. The correct three-dimensional implant position (a) mesio-distal, (b) oro-facial, (c) apico-coronal.4
The timing of implant placement following tooth extraction has been investigated in various studies in the literature (Table 2).6, 7, 8 Similar survival rates have been reported for all types of implant placement but outcomes might be adversely affected by timing of implant placement.6, 7, 8
Classification
Descriptive terminology
Desired clinical outcome
Type 1
Immediate placement
An extraction socket with no healing of bone or soft tissues
Type 2
Early placement with soft tissue healing (typically 4 to 8 weeks of healing)
A postextraction site with healed soft tissues but without significant bone healing
Type 3
Early placement with partial bone healing (typically 12 to 16 weeks of healing)
A postextraction site with healed soft tissues and with significant bone healing
Type 4
Late placement (more than 6 months of healing)
A fully healed socket
Type 1 implant placement
This allows the extraction and implant placement to take place in the same surgical procedure, thereby reducing the treatment time. Immediate implant placement shows similar survival rates as delayed implant placement, but cannot prevent bone remodelling after tooth loss.9, 10 An immediate implant placement requires primary implant stability and a restoratively-driven implant placement. It can be related to increased risk of gingival recession. For this latter reason, immediate placement can be considered in cases of minimal aesthetic risk, such as replacement of mandibular incisors or premolar teeth.11, 12
Type 2 implant placement
This is the most commonly employed technique in the aesthetic zone. It offers additional soft tissue volume, which facilitates the surgical manipulation and enhances soft tissue aesthetics. This approach also allows resolution of local pathology through bone remodelling.12, 13
Type 3 implant placement
This facilitates additional soft tissue volume for flap closure and partial bone healing for primary stability but varying amounts of resorption might compromise bone availability.11, 13 Type 3 implant placement is indicated for the replacement of multi-rooted teeth.
Type 4 implant placement
This shows additional soft tissue volume and bone healing but greatest chance of increased bone resorption, thereby limiting the volume of bone for implant placement.11, 13 Type 4 implant placement should be considered in cases of excessive local pathology.11, 13
Peri-implant defects with gaps of less than 2 mm following type 1 and type 2 implant placement may heal spontaneously.11 However, peri-implant defects of 2 mm or more in the oro-facial dimension show reduced predictability for spontaneous bone regeneration.11 Guided Bone Regeneration (GBR) is a bone augmentation technique in localized alveolar ridge defects using semi-permeable membranes with different particulate bone filler materials.14
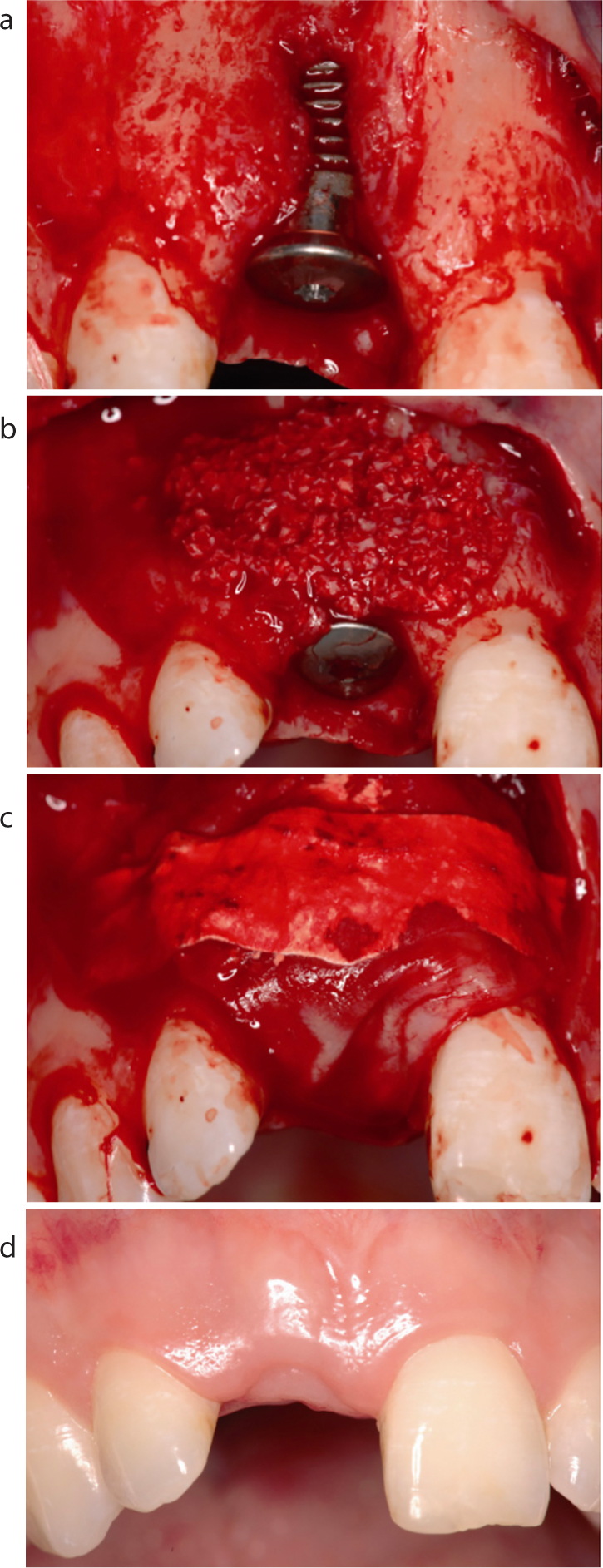
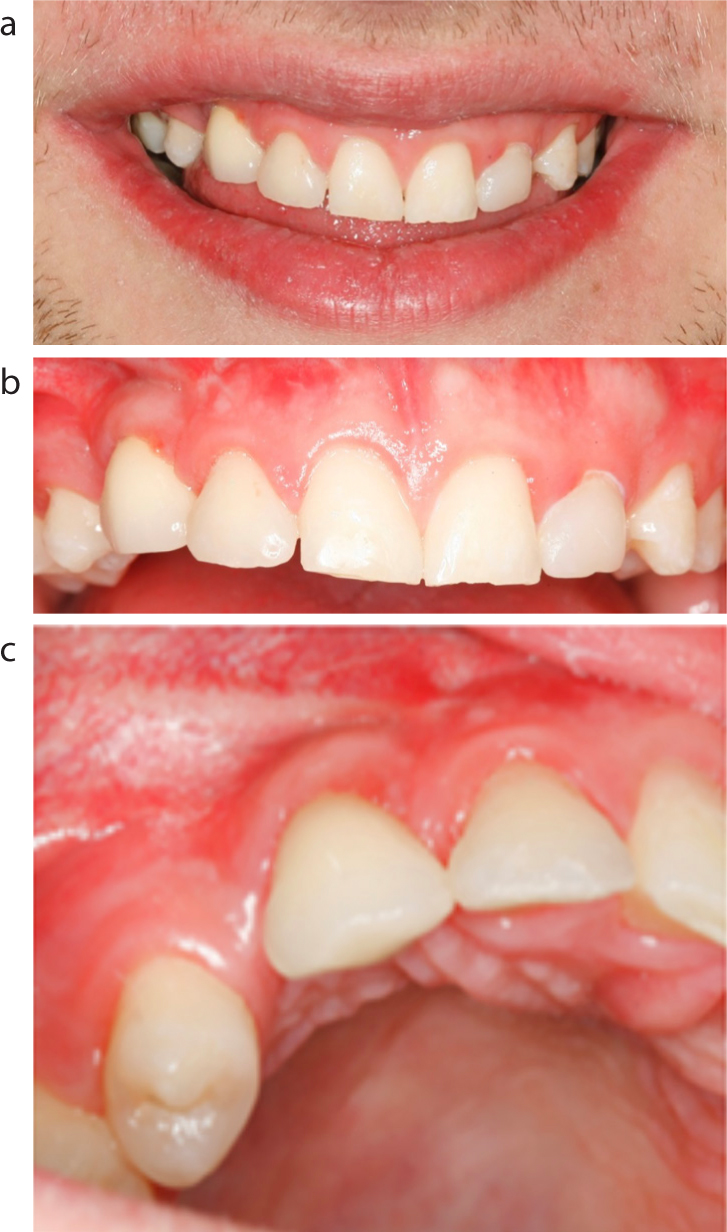
Bone augmentation procedures show high survival rates of 95.7%, and dehiscence and fenestration resolution of 54% and 97%, respectively. GBR is more effective with type 1 and 2 implant placement (Figure 2).12 The technique offers bone fill and defect resolution in peri-implant defects, improved soft tissue contour and hence aesthetics, and minimizes the risk of gingival recession (Figure 3).15, 16
Figure 2.
(a–d) Type 2 implant placement with GBR technique (double layer technique).Figure 3.
(a–c) Improved soft tissue contour and aesthetics with type 2 implant placement of UR3 with the use of simultaneous GBR technique.
Survival rates of implants placed in guided tissue regenerated bone after treatment of localized defects in an alveolar ridge are comparable to survival rates of implants placed in native bone.17 Furthermore, the superiority of one augmentation technique over another, based on implant survival rates, was not demonstrated.17
Prosthodontic considerations
Fixed or removable implant-supported prostheses can be used to replace missing teeth as part of implant rehabilitation. Fixed implant-supported prostheses can be classified based on the number of teeth they are replacing: single crowns, short span, long span or full arch bridges, or classified based on the type of retention: screw- or cement-retained.
The choice between screw- and cement-retained, implant-supported prostheses remains controversial in the literature.18, 19 Screw-retained prostheses show more technical problems, such as screw loosening or ceramic fracture compared to cemented-retained restorations that can present with greater biological complications, such as peri-implant bone loss associated with marginal cement extrusion.20, 21, 22, 23 Ideally, screw-retained prostheses may be more desirable since they offer restoration retrievability, which facilitates long-term maintenance provision.24 The provision of a screw-retained prosthesis requires accurate restoratively-driven implant placement, so that the implants are parallel and the screw emergence is not visible. It can be technique-sensitive, as optimal implant position and passive fit of the prosthesis are a pre-requisite to avoid problems.1
The choice of material for the abutment of the definitive implant-supported reconstruction is generally between zirconium and titanium. Which material is more appropriate remains highly debatable in the available literature.24, 25, 26 The 5-year survival rate, technical and biological complications are similar for zirconium and titanium abutments supporting implant restorations.25, 26 Moreover, no differences have been found in soft tissue response in the peri-implant area between zirconium and titanium surfaces.27 For prostheses in the aesthetic zone, zirconia abutments may be indicated to enhance the aesthetic outcome, but the clinical use of ceramic abutments in posterior sites or bridges should be used with caution (Figures 4–6).25, 28 Although zirconium and titanium abutments show similar survival rates, zirconium abutments require careful manipulation since adjustment of zirconium can adversely affect its mechanical properties.29 Careful polishing is recommended after adjusting the abutments to keep surface roughness and phase transformation (commonly referred to as ‘ageing’) low.29
Figure 4. All-ceramic crown supported by zirconium abutment at UL3 site.Figure 5.
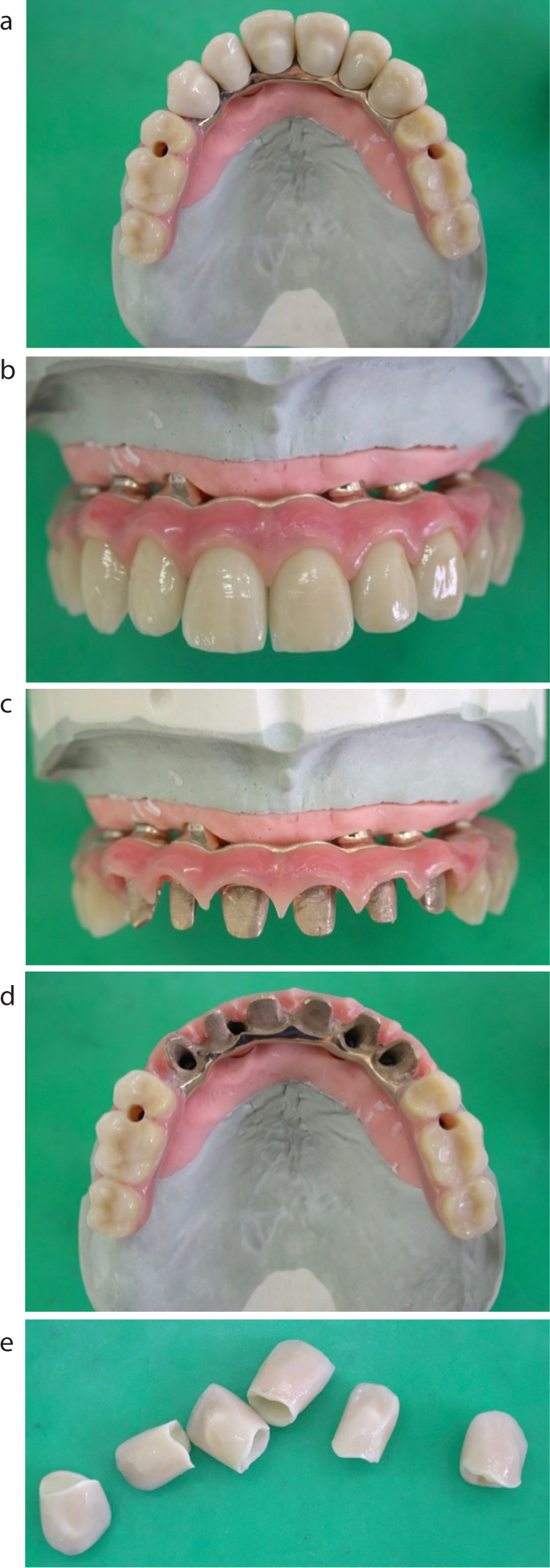
(a–d) Metal-ceramic bridges supported by milled titanium framework.Figure 6.
(a–e) Full arch, metal-ceramic bridge supported by milled framework with individual crowns at the maxillary anterior teeth to correct angulation discrepancies.
Apart from the abutment material, the design of the prosthetic superstructure is of paramount importance. Designs should be smooth and convex to allow oral hygiene access and hence minimize biological complications.19, 28 Although CAD/CAM fabricated prostheses demonstrate similar survival rates to conventionally fabricated prostheses, reproducibility, passive fit and reduced stress at the implant-fixture interface can be more easily achieved with digital technology.19
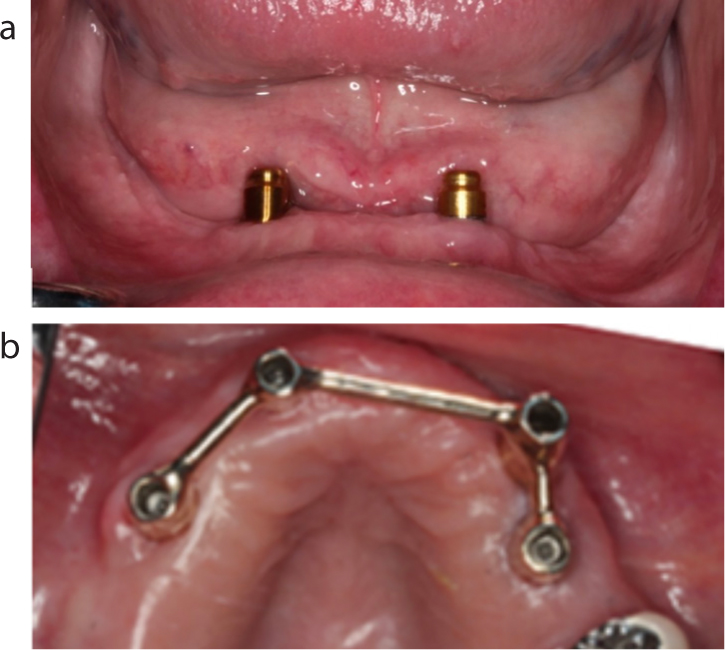
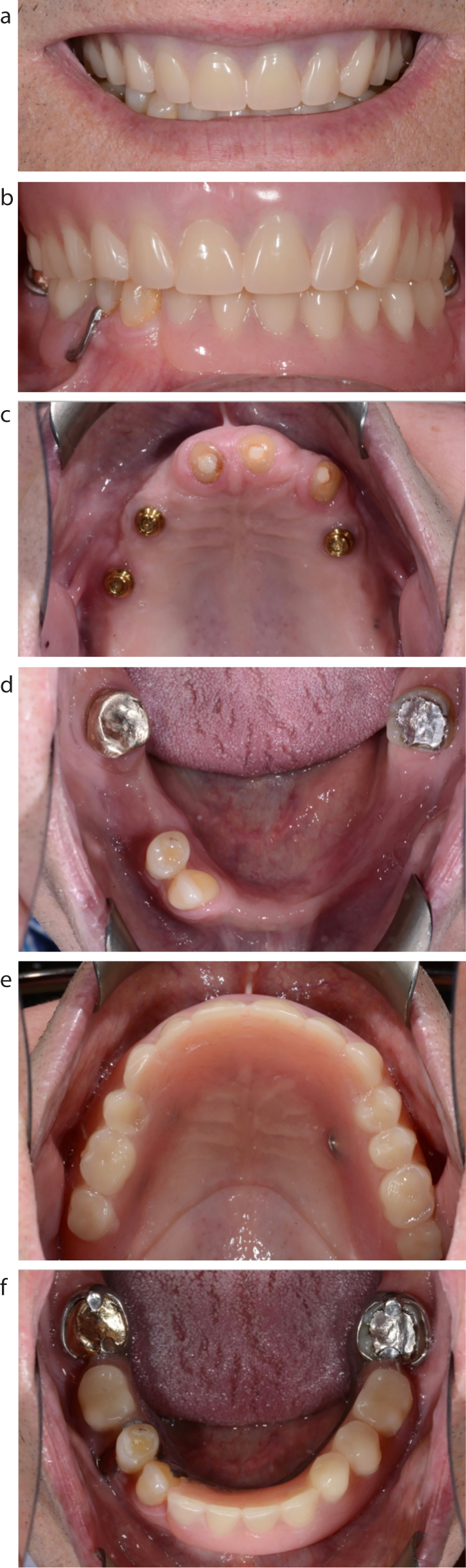
Removable implant-supported prostheses can be classified as bar-retained or retained on individual attachments (balls, studs or magnets) (Figures 7, 8). For mandibular overdentures, two individual attachments are preferable to bars since they offer adequate retention and stability, similar patient satisfaction, easier fabrication, maintenance and are cost-effective.30 For maxillary overdentures, bars supported by four or more implants show better outcomes regarding survival of both the implants and the prosthesis compared to four or less implants and individual attachments.31, 32 Implant-supported prostheses offer improved outcomes compared to conventional dentures and some clinicians suggest that two-implant supported mandibular overdentures should be the minimum offered to edentulous patients as a first choice of treatment.33, 34
Figure 7. Implant reconstruction for overdentures: (a) individual attachments; (b) cast bar.Figure 8.
(a–f) Oral rehabilitation of a case with an edentulous maxilla and partially dentate mandible with an implant-supported overdenture on individual attachments and a conventional removable prosthesis.
Maintenance
Although clinical and technological advances have led to an evolution in implant therapy, technical and biological complications are commonly encountered both in fixed and removable prostheses.3, 35, 36 Systemic conditions and treatments that might affect healing or susceptibility to disease, history of treated periodontitis and smoking are related to increased incidences of biological complications. Mechanical factors such as excessive cantilever extension, the vertical height of the superstructure, parafunctional activity or a patient with a history of previous complications, may increase the incidence of technical complications.37, 38, 39
Implant-supported overdentures are a favourable solution for edentulous patients with 80% survival rate over 10 years.35 Overdentures require regular maintenance, such as replacement of worn or deformed female retainers, repair of fractured bars, fractured acrylic or replacement of worn abutments. These maintenance episodes are reported to be approximately 85% for such prostheses.35 Other common complications are repeated adjustment, loose abutments or attachments, denture fracture, denture reline, soft tissue hypertrophy around bars, peri-implant bone loss and implant failure.36 Bar-retained overdentures require less maintenance compared to those dentures retained on individual attachments, but the former complications are usually more complex and financially costly.37 Bar design and configuration may influence prosthetic maintenance. For example, round cross-sectional bars require more maintenance (1.2% complications per year) compared to milled bars (0.3% complications per year) due to reduced movement and rotation of the prosthesis.40 Also, the presence of cantilever extension(s) over 15 mm are related to increased incidence of technical complications.38, 39
Implant rehabilitation with fixed implant-supported prostheses demonstrate high survival rates; the 10-year survival rate of implant-supported crowns and implant-supported bridges are 89.4% and 86.7%, respectively.3, 41 Although survival rates are high, the complication rate is also high; 38.7% over a 5-year period, with implant-supported bridges showing higher incidences of technical complications compared to implant-supported crowns (Table 3).3, 42 The most frequent technical complications were fractures of the veneer material (ceramic fractures or chipping), abutment or screw loosening and loss of retention.3 Biological complications were encountered with similar incidences between the two treatment modalities.3, 42
SC
FDP
Implant fracture
0.14%
0.5%
Screw abutment loosening
5.6%
5.6%
Screw abutment fracture
0.35%
1.5%
Ceramic/veneer fracture
3.5%
8.6%
Loss of retention
5.5%
5.7%
Soft tissue complication
7.1%
8.5%
Summary
Implant rehabilitation is considered a predictable treatment modality to replace single and multiple missing units with high survival rates. Technical and biological complications are commonly encountered and careful treatment planning, restorative-driven implant placement and long-term maintenance are prerequisites of a successful implant rehabilitation minimizing these complications. The buccal bone thickness and interproximal bone levels for soft tissue stability, the correct implant dimensions for a favourable emergence profile, careful surgical technique, pink and white aesthetic harmony, design of the prosthesis to permit adequate oral hygiene, and planning for long-term maintenance care are the most important elements of treatment planning for implant-supported reconstructions. Attention paid to these factors will result in successful reconstructions with high patient satisfaction levels.