Wassell R, Naru A, Steele J, Nohl F. Applied Occlusion, 2nd edn. London: Quintessence; 2015
McCullock AJ. Making occlusion work: 1. Terminology, occlusal assessment and recording. Dent Update. 2003; 30:150-157
Davies S, Gray R. A Clinical Guide to Occlusion.London: British Dental Association; 2002
Posselt U. Studies in the Mobility of the Human Mandible.Copenhagen: Acta Odontologica Scandinavica; 1952
Steele J, Nohl F, Wassell R. Crowns and other extra-coronal restorations: occlusal considerations and articulator selection. Br Dent J. 2002; 192:377-387
Wilson P, Banerjee A. Recording the retruded contact position: a review of clinical techniques. Br Dent J. 2004; 196:395-402
Ferrario V, Sforza C, Serrao G, Schmitz J. Three-dimensional assessment of the reliability of a postural face-bow transfer. J Prosthet Dent. 2002; 87:210-215
Wise MD, Laurie A. Failure in the Restored Dentition: Management and Treatment.London: Quintessence; 1996
Nohl F, Steele J, Wassell R. Crowns and other extra-coronal restorations: aesthetic control. Br Dent J. 2002; 192:443-450
Tiu J, Al-Amleh B, Waddell J, Duncan W. Reporting numeric values of complete crowns. Part 2: Retention and resistance theories. J Prosthet Dent. 2015; 114:75-80
Dahl BL. Dentine/pulp reactions to full crown preparation procedures. J Oral Rehabil. 1977; 4:247-254
Blair F, Wassell R, Steele J. Crowns and other extra-coronal restorations: preparations for full veneer crowns. Br Dent J. 2002; 192:561-571
Poyser N, Porter R, Briggs P, Chana H, Kelleher M. The Dahl Concept: past, present and future. Br Dent J. 2005; 198:669-676
Occlusally challenging scenarios can arise during the restoration of teeth involved in the patient's Retruded Contact Position (RCP). During preparation of a tooth that provides the RCP, practitioners may encounter problems whereby they lose occlusal clearance to place an occlusal coverage restoration over the tooth in question. This may come as a shock to the practitioner, often resulting in further excessive and unplanned tooth preparation, or reduction of the opposing tooth to create occlusal clearance. This paper aims to provide a guide on how to recognize and avoid the potential pitfalls of restoring retruded contact position, through the use of proper planning and by employing appropriate management techniques.
CPD/Clinical Relevance: Understanding of the relevant occlusal considerations will allow the practitioner to restore teeth involved with RCP predictably and conservatively.
Article
Many practitioners will be able to relate to the clinical situation where a posterior tooth, often the last standing tooth, is treatment planned and prepared for a full or partial coverage restoration. During occlusal preparation, adhering to the depth requirements of the intended restoration, an assessment of occlusal space for the restoration is made and it is surprising to see that the preparation is still in contact with its antagonist. The first question asked is how this has arisen, and then how, clinically, the situation can be overcome. This paper aims to give a guide to dentists on how to avoid this situation and how, through careful planning and execution, it can be managed.1 A number of descriptive occlusion terms will be employed, which are commonly interchangeable with other referenced nomenclature. These terms are outlined in Table 1.2, 3
Term
Alternative Names
Definition
Inter-Cuspal Position (ICP)
Maximum Inter-Cuspation (MI[P]), Centric Occlusion (CO)
Mandibulo-maxillary relationship at the point of maximum tooth inter-cuspation
Retruded Contact Position (RCP)
Centric Relation Contact Position (CRCP)
Initial point of tooth contact during mandibular closure with the condyles in centric relation and the mandible in the retruded arc of closure
Centric Relation (CR)
Retruded Axis Position (RAP), Terminal Hinge Axis (THA), Retruded Axis (RA)
A condylar position where the condyles are situated in the most antero-superior position within the glenoid fossa. It is a clinically reproducible position
Retruded Arc of Closure (RAC)
The range of movement of the mandible, whereby the condyles rotate about the Terminal Hinge Axis. The condyles are in centric relation
Background
The mechanism behind the situation of the last tooth in the arch syndrome is that the tooth being prepared had previously acted as a posterior fulcrum when the patient occluded, initiating a slide to ICP. This tooth, or more accurately the area of contact on the tooth itself, is known as the Retruded Contact Position (RCP).1, 2 The phenomenon explored in this article is therefore not strictly limited to only the last tooth in the arch; this is merely a classical example that can give rise to the situation. However, other teeth may provide RCP, and similar consequences may arise.1
Inter-cuspal position (ICP) is a ‘memory state’ controlled by neuromuscular feedback to higher neural centres, alongside the temporo-mandibular joint and the dentition – the so-called posterior and anterior determinants of occlusion.1, 3 In a fully or partially dentate arch, a patient may close straight into ICP as a result of learned, habitual neuromuscular control and therefore occlusal clearance may not be lost following tooth preparation at RCP. If this is the situation, then we may introduce a new deflective interfering dental contact following the fit of the new restoration.
When most people occlude (around 90% of the population), their RCP is different from their ICP.1, 4 Due to the effect of neuromuscular control, this learned ‘memory’ can be lost within minutes if patients aren't allowed to occlude, thus proprioceptive feedback from the periodontal ligaments is abolished. Patients' jaw musculature will then relax and their condyles will reposition within to the glenoid fossa.1, 2 Therefore, in the absence of this neuromuscular memory, their RCP acts as both a pivot and slide to guide patients subconsciously into their ICP. This deflective movement can be considered as a 3-dimensional combination of vertical and horizontal components. However, when the RCP is removed, either due to wear of tooth or restoration, extraction, fracture (possibly by parafunction) or critically by tooth preparation, the mandible loses its deflective contact into ICP. This may have a series of implications:
When closing, the condylar heads are no longer ‘guided’ by the previous RCP into their ‘usual’ position in ICP;
The condyles of the mandible therefore remain in their superior position within the glenoid fossa;
The lower jaw is now able to rotate further along the retruded arc of closure (RAC), as it has not been deflected out of centric relation by the original RCP (Figure 1);
The deflective contact will often have moved to another location, importantly, at a reduced occlusal vertical dimension relative to the previous RCP. Either:
RCP moves to a different pair of teeth; or
RCP remains on the same tooth but more cervically positioned than the previous RCP. This still allows the prepared tooth to remain in occlusion, despite reducing the occlusal height of the tooth.
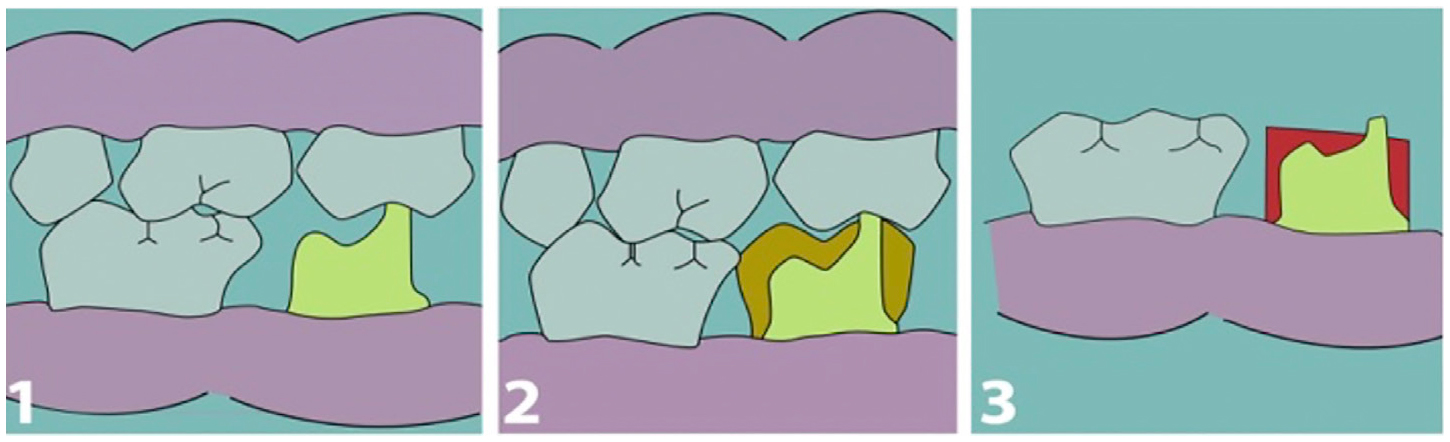
Figure 1.
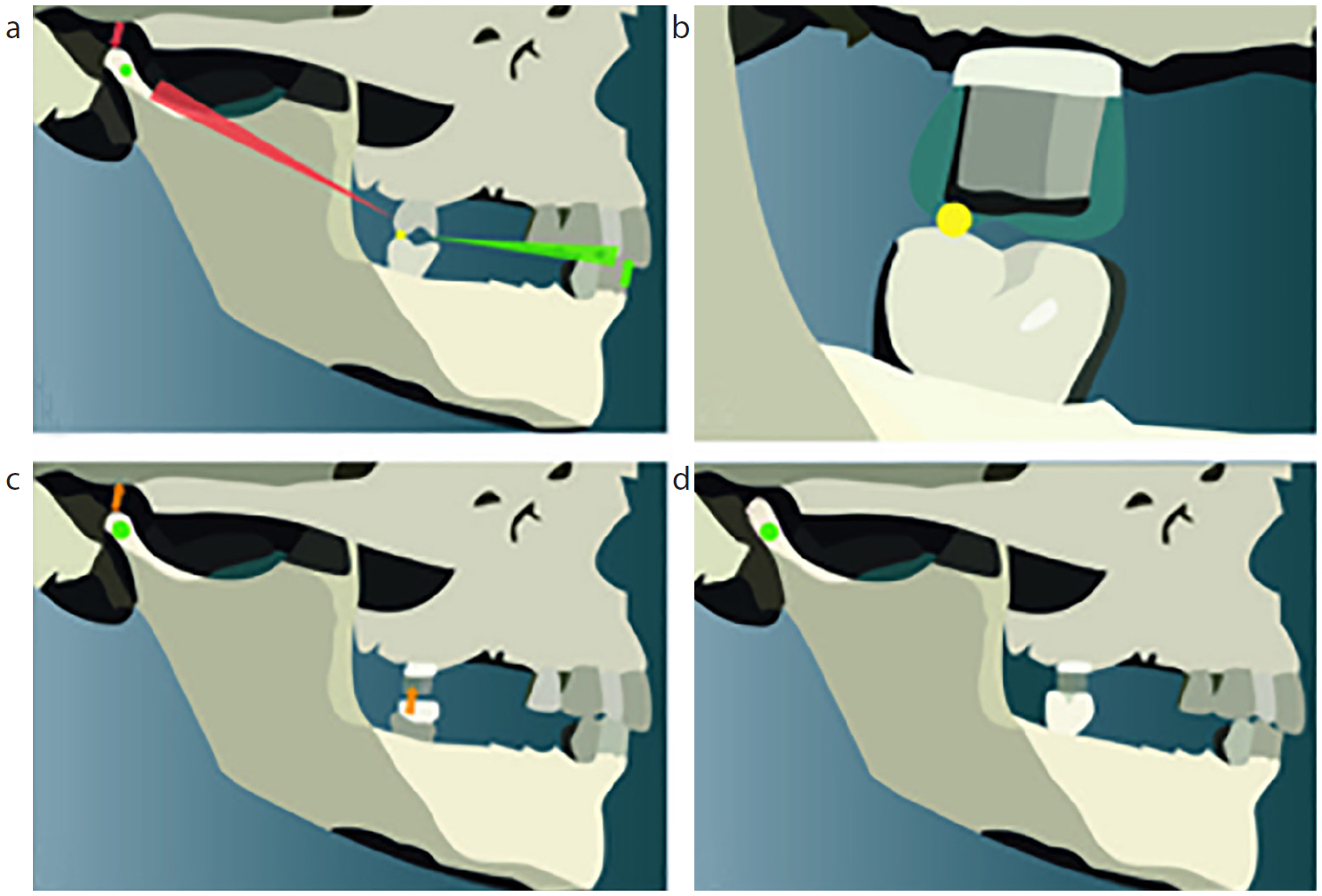
(a–d) Schematic diagram showing: 1. the deflective movement from RCP to ICP; 2. preparation of the tooth resulting in the loss of RCP; 3. space for the condyles to reposition superiorly; 4. condyles have repositioned and occlusal clearance has been lost.1 Diagram adapted from animated demonstration as part of Applied Occlusion by Wassell R, Naru A, Steele J, Nohl F.1
Operators may visualize this as a superior repositioning of the condyles into the glenoid fossa.1 Note that ICP may change following the repositioning of the deflective contact.
The clinical significance of this effect is that, despite removing occlusal tooth tissue in order to create space for the restorative material, further tissue may need to be removed. This lack of planning means the need to remove further tissue was not recognized in advance and incorporated into the decision-making process at the treatment planning stage. This could potentially force the operator into preparing the tooth more heavily and closer to the pulp. This may result in a loss of preparation height in an unplanned fashion; perhaps necessitating deep, sub-gingival margins as a result.
How to plan
Any restorative procedure requires planning. It is important to carry out a thorough occlusal examination for every patient that is to receive any occlusal coverage restoration, particularly for indirect restorations. This will aid the operator in determining several important features of occlusion that are to be included in the final restoration. These features include, but are not limited to:
Occluding contacts in ICP;
The location of RCP;
Lateral guidance patterns;
Antero/posterior guidance patterns.
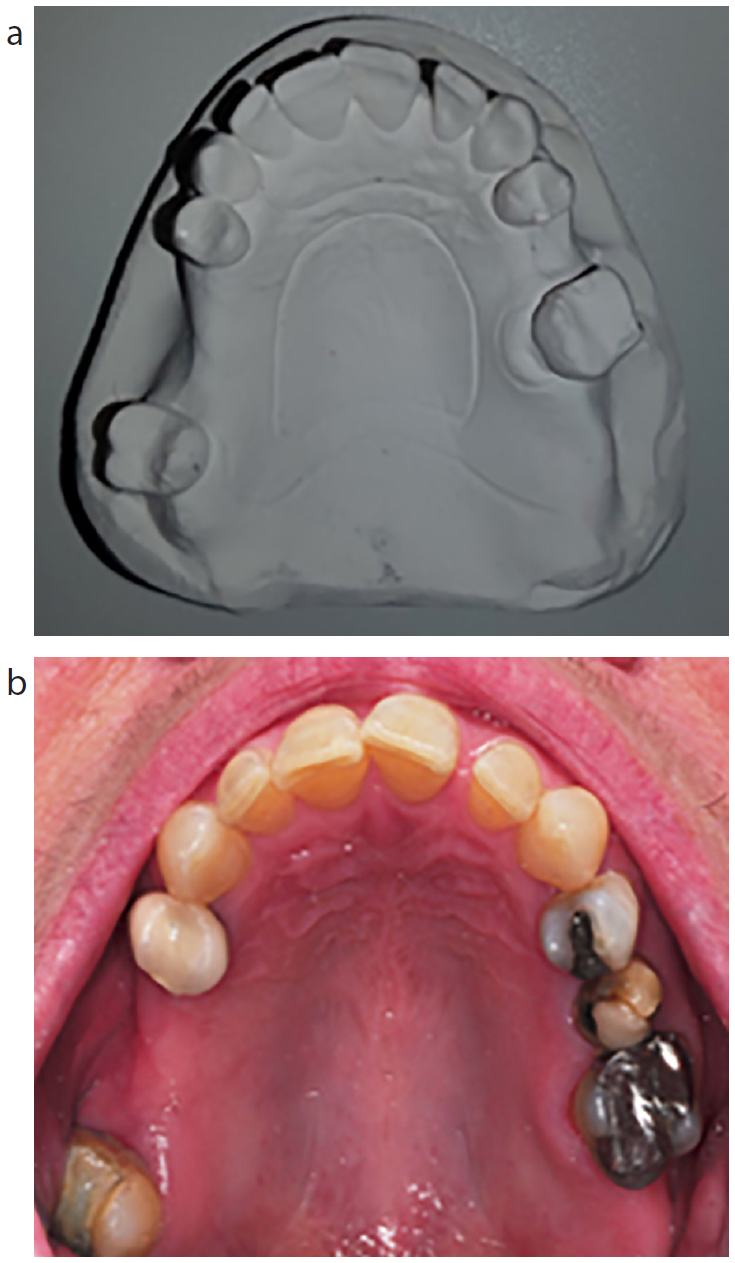
These checks should be carried out as a minimum. Readers are directed to the Clinical Guide Series (A Clinical Guide to Occlusion) compiled by Davies SJ and Gray RJM for a comprehensive approach to examining and recording a patient's occlusion.3, 5 The rationale behind the latter two features above is beyond the scope of this paper so will not be explored further. Clinical photography can be invaluable, and it is advised that occlusal contacts are marked, as it can be difficult to determine the restorative condition of the dentition from mounted stone casts (Figure 2). However, when used in conjunction with clinical photography, this suddenly becomes easier, since photographs will show the location and condition of restorations, as well as occlusal markings on teeth. These can be double checked and replicated on the articulated study casts. Figure 2 shows how the heavily restored state of a dentition can be masked on stone casts.
Figure 2.
(a, b) A pictorial depiction showing that the restorative state of teeth may not be obvious on study casts. For example, the heavily restored condition of the UL6 is not obvious on the stone model.
Identifying
To identify RCP, one needs to be able to manipulate the patient into centric relation. There are several accepted methods available for this, often used in conjunction with one another, including:
The construction of a lucia jig from self-cured acrylic or a prefabricated jig. These methods deprogram the mandible and force the condyles superiorly (Figure 3);
Through bimanual manipulation of the patient's jaw;
Through the use of a leaf gauge to allow closure slowly;
By using gothic arch tracing.
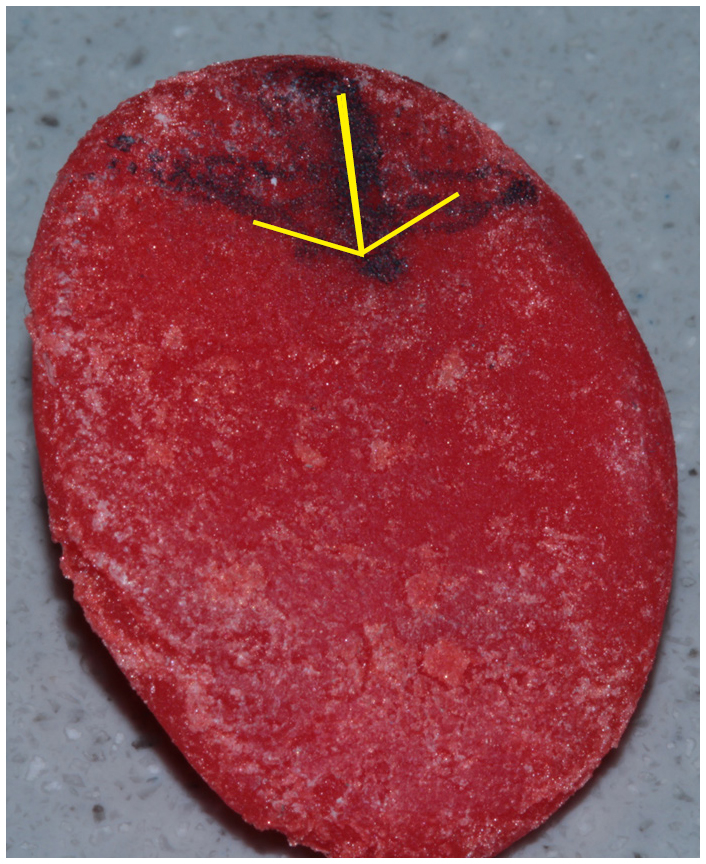
Figure 3. Custom lucia jig fabricated from DuraLay (Reliance) self-cured acrylic. The tip of the arrow represents centric relation.
There are several other techniques, and the operator should use a technique with which they are familiar and which produces an accurate and reproducible result.6
To mark RCP accurately, one technique which is proposed is as follows:
The patient is placed in the supine position;
The patient is instructed that his/her jaw will be moved by the operator, and the patient is encouraged to relax;
The patient's jaw is then manipulated into centric relation and the jaw is eased to close;
The patient is asked to take note of where his/her teeth first touch, and to point in the general direction of where they felt contact;
The location of where the patient noticed contact should be documented in the notes;
The procedure is repeated. This time, the dental assistant will hold articulating paper passively in the area where the patient noted the original RCP, which will mark up the location of first contact in centric relation.2
Articulating study casts
Even if the tooth to be prepared is not the RCP contact, accurate recording of the patient's occlusion and the use of articulated study casts will improve the accuracy of the restoration and reduce chairside adjustment. Once the operator has determined that RCP is to be occlusally restored, particularly with indirect work, certain procedures should be followed. Accurate upper and lower impressions should be taken. Once poured and cast, models should be mounted and articulated in centric relation; it should be possible to locate ICP as well. To relate the casts, an inter-occlusal centric relation record may be taken in a rigid-setting thermoplastic material, such as Beauty Wax® (Moyco) (Figure 4), which may be refined with a material such as TempBond® (Kerr) (a self-curing temporary cement). There should be no tooth-tooth contact through the wax at this point, as CR is a tooth apart position, and any contact may result in an involuntary deviation from the terminal arc of closure due to proprioceptive feedback from the periodontium.6 Finally, a facebow record should be sent with the inter-occlusal record for more accurate articulation and jaw relation, by relating the maxillary cast to the condyles in an anatomically appropriate position.1, 7 Once mounted on a semi-adjustable articulator in centric relation, the inter-occlusal record may be removed from between the casts, and the RCP can be confirmed to be the same as what was established intra-orally.5 Ideally, casts should be duplicated, as adjustments will be made on them. Producing an accurate centric relation record is very important, as the operator and technician must know exactly where RCP is located. Additionally, casts must be treated with the utmost care to avoid damaging RCP. When mounted in centric relation, upon opening and closing the upper member of the articulator, RCP will be the only contact, so it is easy to damage this surface, which is another indication to duplicate the casts.
Figure 4. Centric relation record fabricated from Beauty Wax® (Moyco). The V-shaped notch at the anterior aspect also permits the placement of a lucia jig in conjunction with the wax record.
Testing slides and pivots
With accurately articulated models, the operator can go on to assess the deflective pattern of movement from RCP to ICP. The direction of the deflection can be assessed, and it should be noted whether the movement is:
The horizontal and vertical vector should be evaluated and noted.
This will aid in the assessment of the discrepancy between RCP and ICP. The operator may make a sectional matrix of the cast (or this may be done intra-orally at the patient's last visit), and he/she can then perform a trial adjustment of RCP on the proposed tooth on the cast. The matrix can be sectioned and placed upon the tooth to assess the level of occlusal reduction (Figure 5). With only a small level of occlusal reduction, RCP will remain on the same tooth as the mandible is permitted to progress further along the RAC (with the condyles in centric relation) as it has not been deflected out of this position by the original RCP.1
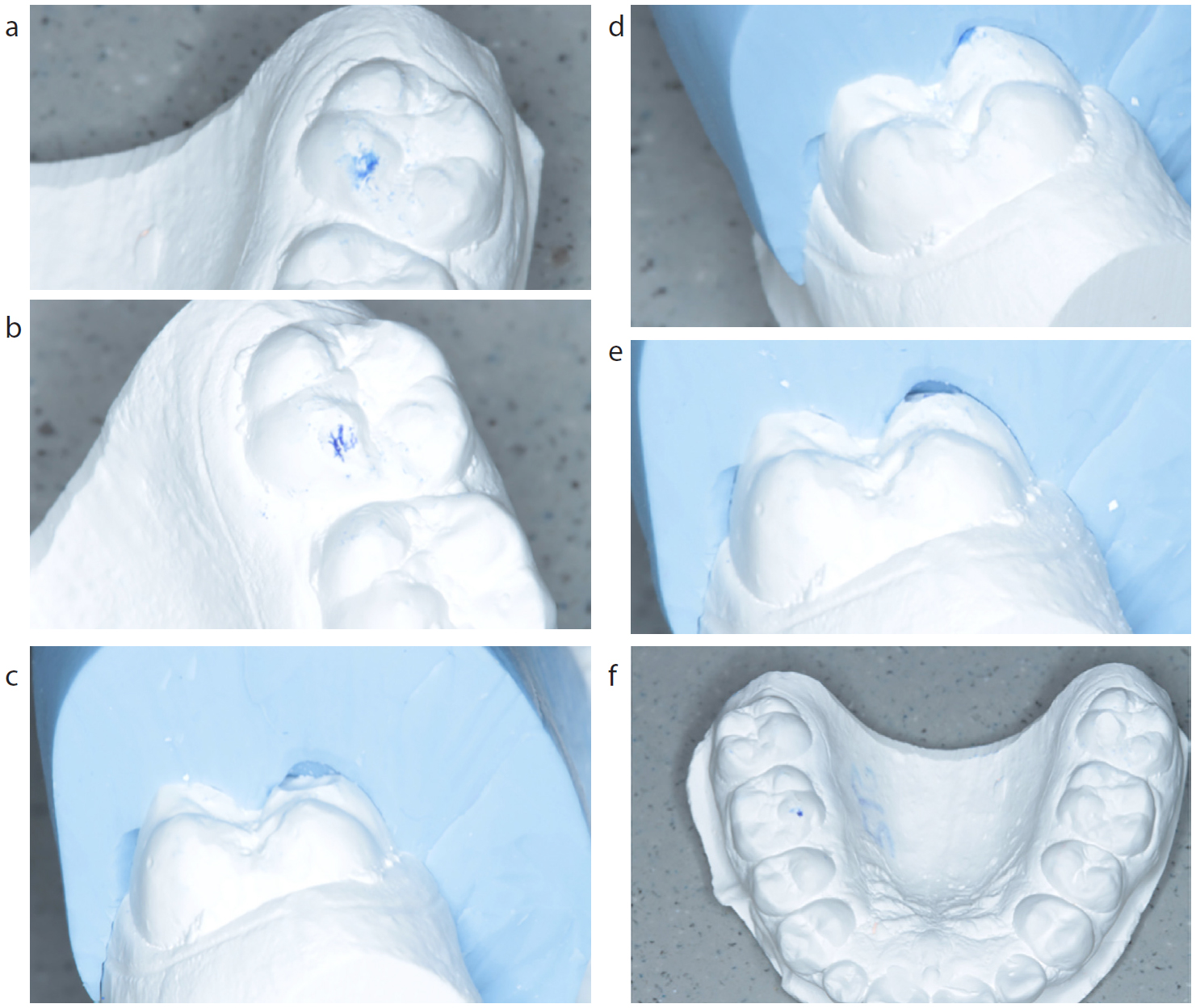
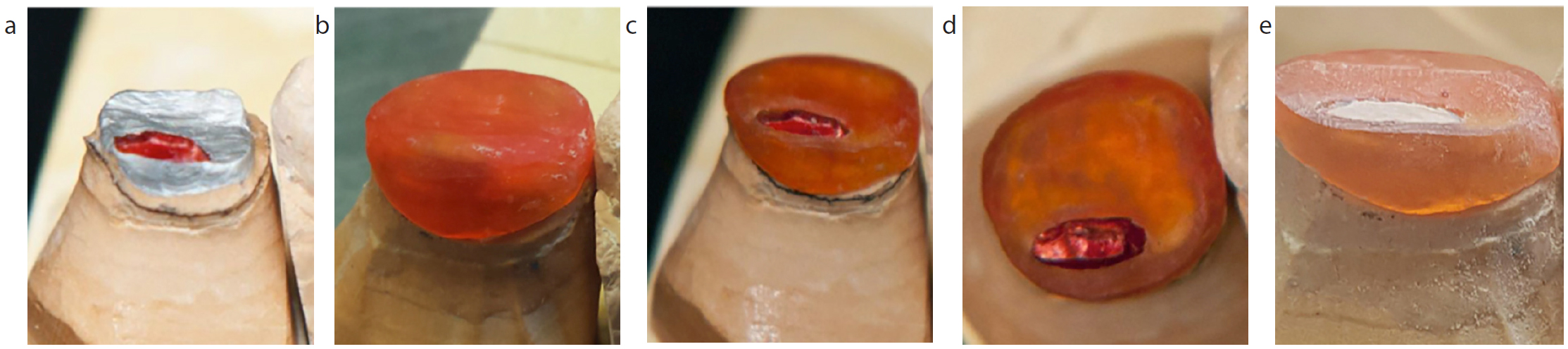
Figure 5. Schematic views depicting: (a, b) RCP marked on the cast (UR7); (c) silicone index created as a depth reduction gauge; (d, e) approximately 1 mm reduced from RCP (RCP remains in the same location as before); (f) approximately 2 mm reduced from RCP (RCP has now relocated to a different tooth (UL6)).
It is incumbent on the operator to decide how much occlusal reduction is acceptable for the tooth to be prepared. It is important to consider whether this tooth has sufficient occlusal height to preserve resistance and retention form for an indirect restoration, or whether the pulp may be compromised. It is important to consider the effect of excessive tooth preparation on:
Two scenarios can therefore arise, and the operator must consider:
Where minimal occlusal reduction is necessary, the deflective RCP contact can be relocated to another tooth/teeth. RCP may become coincident with ICP, hence this scenario may be akin to a re-organization case. The objective in this case is to shift RCP away from the tooth to be prepared in order to allow an unhindered preparation, without the worry of losing occlusal clearance. This scenario is more likely when patients have most of their teeth and there is only a small vertical slide into ICP. If the new RCP is suitable, this reduction can be replicated intra-orally. Further tooth preparation can then be undertaken with normal considerations as to the requirements of the restoration. Breaking this process into two appointments is advised.5, 8 The operator should take into consideration the changes in jaw relationship once RCP has been removed. For example, if there is originally a large horizontal: vertical vector, removal of RCP may result in distal positioning of the mandible and loss of protrusive guidance.8 Moreover, the operator should be satisfied with the suitability of the new RCP. If, for example, the new RCP in Figure 2 was situated on the disto-buccal cusp of the upper left first molar, a thin, unsupported cusp, the operator may consider preparation of this new deflective contact with the intention of relocating it elsewhere (see ‘When little occlusal reduction is required’).
Where an unacceptably excessive level of reduction is required to move RCP to another tooth, making it unfavourable to relocate it elsewhere, a conformative approach is favoured, as the original contact needs to be maintained (see ‘When significant occlusal reduction is required’).
How to execute
When little occlusal reduction is required
If minimal occlusal reduction is required to move RCP onto a different tooth, generally the case becomes simpler to manage. It is important to consider the new location of RCP. The operator must be happy that this new deflective contact is suitable, and will be able to support the loads involved. If the new RCP ends up on a thin, unsupported cusp, on the outside of a large MOD amalgam restoration (as an example), the operator may not be comfortable leaving the initial deflective contact on this tooth. In such a case, the operator should practise removal of the sequential RCPs on the casts until they are satisfied that RCP is in a suitable position. Note that this may result in a full mouth occlusal re-equilibration. Intra-oral photography can be especially useful here, since it is difficult to distinguish the coronal nature of tooth/restorative structure from study casts, as mentioned previously. Once the operator is comfortable with the new RCP, or has decided toward a full mouth re-equilibration, provided he/she has obtained suitable consent from the patient, then he/she may carry out the same adjustments intra-orally as made on the cast. Preparation for the occlusal coverage restoration may follow at a separate appointment.5
When significant occlusal reduction is required
Four techniques will be explored to manage the case in the event of significant occlusal reduction. The names of each technique are purely colloquial and are not referred to in the literature.
1. The ‘Island Technique’
This is a technically challenging procedure. Once the exact location of RCP (the specific position on the tooth itself) has been established intra-orally, it should be re-confirmed on articulated study casts. RCP should be at exactly the same point, and a high level of accuracy is required for this technique to be successful.
Operative appointment 1:
The marked RCP point with articulating paper should be noted.
Tooth preparation may commence as usual, however, care must be taken not to prepare wherever RCP has been marked. On the other hand, this area must be kept as small as possible, without compromising and shifting the deflective contact. This maintained area will likely appear as a pillar protruding from the prepared tooth. There should be no undercut along this pillar, in order to facilitate laboratory work and the accurate removal of the temporary restoration (Figures 6 and 7).
Impressions may be taken as normal of the prepared tooth; a dimensionally stable material should be used with detailed surface accuracy. With digital impression taking, it is possible to take a pre-operative scan, and a post-preparation scan, which the laboratory can use to reproduce the original tooth anatomy.
A temporary restorative material should be placed; this will help to maintain the integrity of the pillar supporting RCP. Other authors have also suggested that a heat- and pressure-cured resin is favourable due to its superior mechanical properties.8 It is recommended that a sectional matrix of the tooth before preparation is employed, and a resin-based material can be placed into the matrix and held over the prepared tooth to fabricate the temporary restoration.
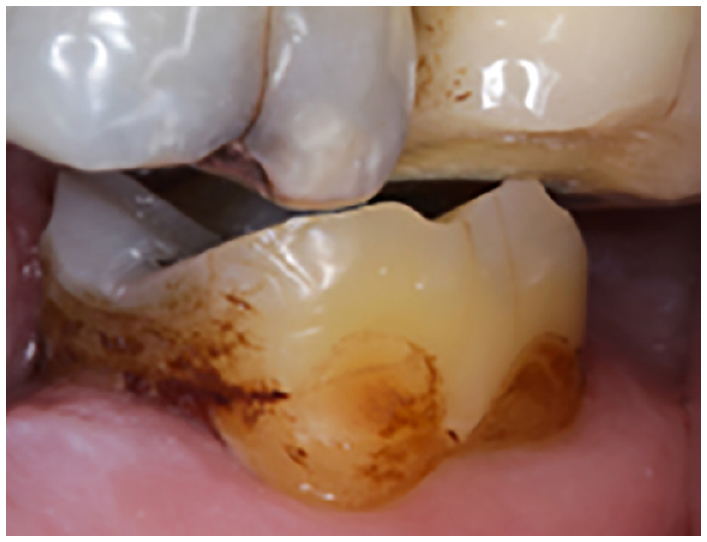
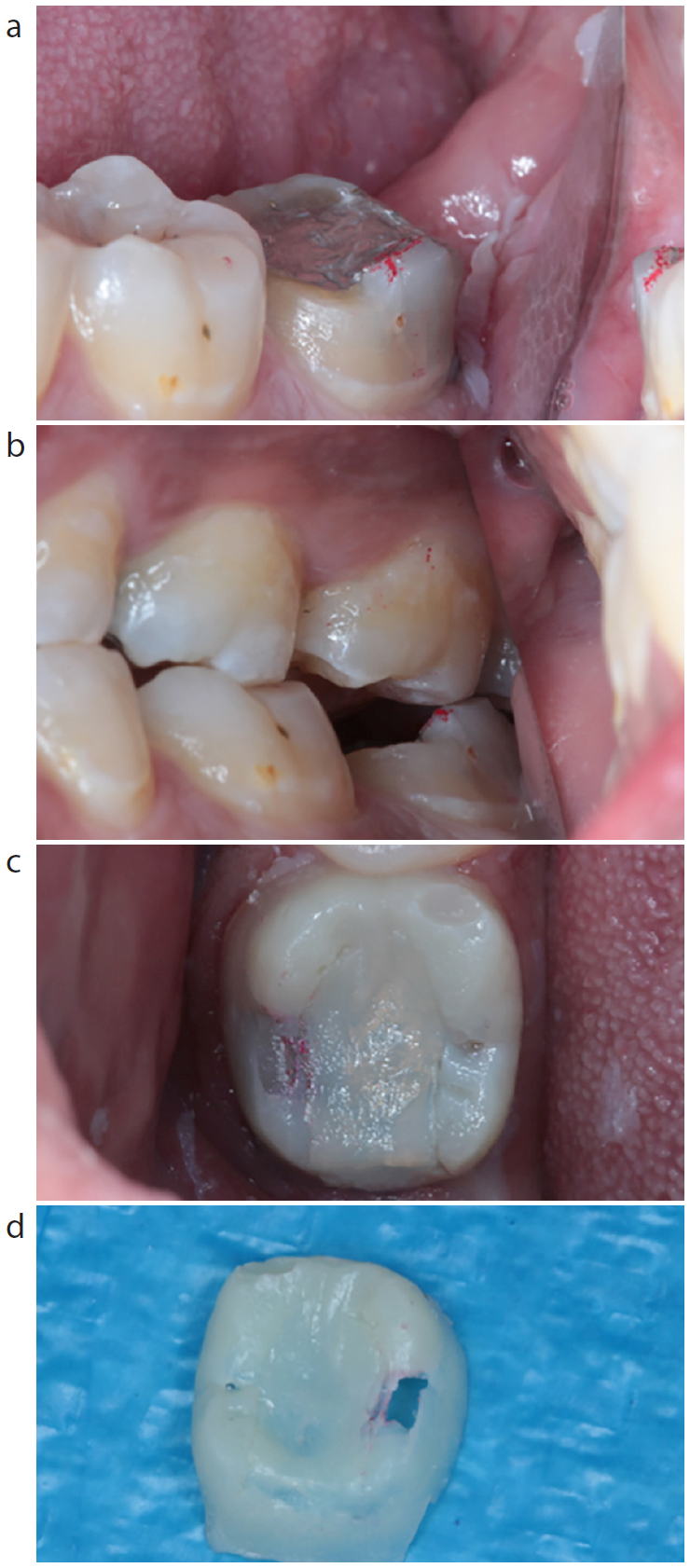
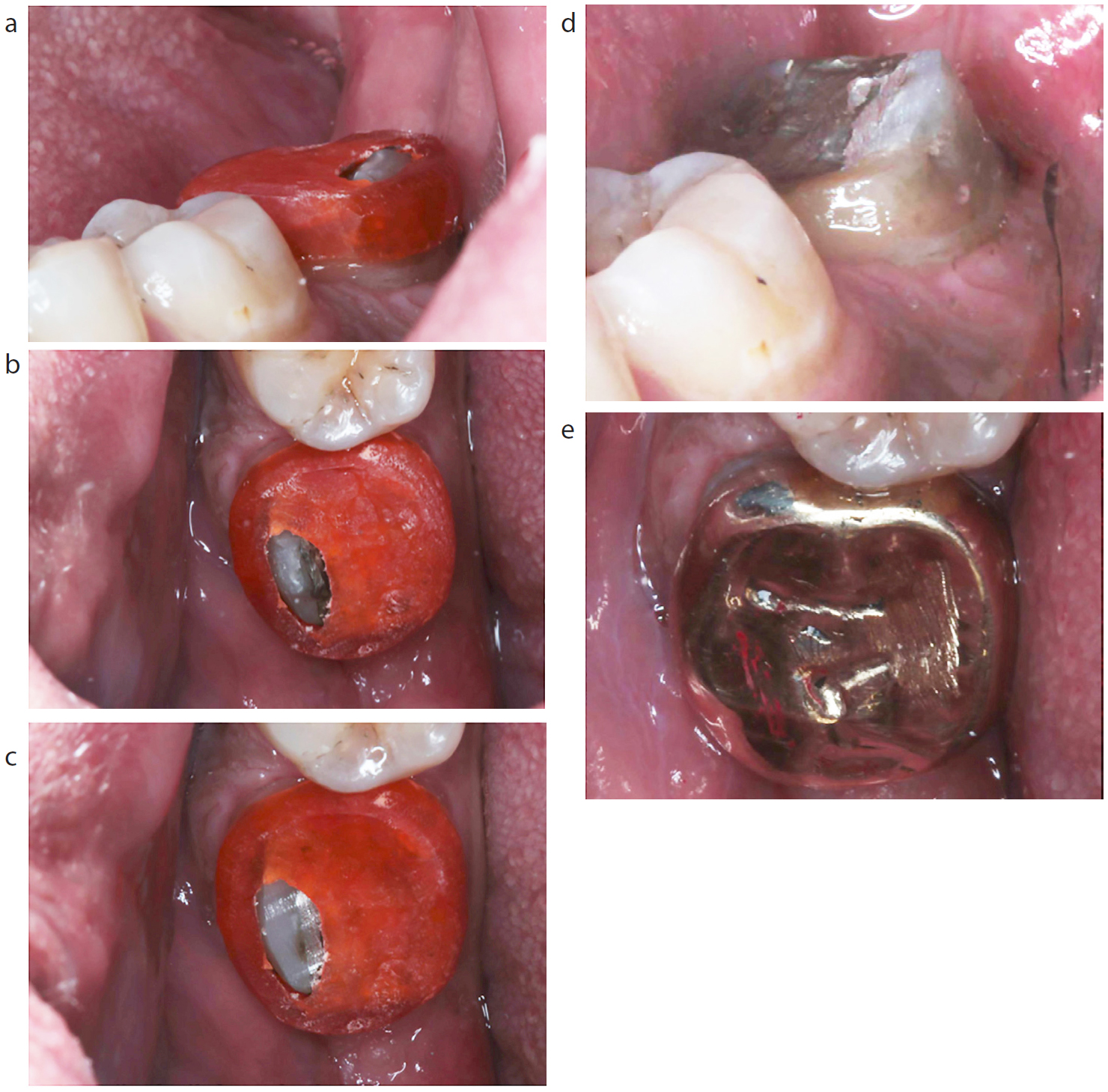
Figure 6. Example of a partial preparation form when using the ‘Island Technique’.Figure 7.
(a–d) Example of a preparation for a gold full veneer crown (FVC) when using the ‘Island Technique’. Note the prominence of the unprepared RCP and the perforation in the temporary crown.
By using this technique, RCP will now appear as an island in the temporary material; the temporary crown will appear to have a hole in it. The crucial point to consider here is that an occlusal stop has been maintained (the ‘island’), hence there will be no condylar repositioning.1, 8
Laboratory Stage 1:
Once cast, the working model should be checked and re-articulated. Articulation in centric relation will give a good understanding of the nature of deflection, however, ICP must also be achievable from the articulation.
Prior to fabricating the definitive restoration, the technician must determine how much of the ‘RCP pillar’ – the occlusal stop – should be removed to create the ideal shape for the prepared tooth. This will ideally be on the prescription from the dentist, who should also take into account restorative material properties.
Before removal of the stop, a coping made from a stable and rigid-setting material (such as DuraLay Pattern Resin (Reliance)) should be moulded around the occlusal stop at the desired height and shape of the final tooth preparation form.
The technician can now remove all stone from above the coping on the die (Figure 8). Alternatively, the coping may be simply placed over the entire tooth surface, and perforated in situ over the island (Figure 9). The technician can then continue preparation of the island and coping together until the desired tooth preparation form is achieved.
The coping can now be removed and what will remain is the shape of the final preparation form. The restoration may now be contoured and fabricated as normal.8
Figure 8.
(a–e) A laboratory schematic depicting the stages prior to crown preparation – RCP is marked up; DuraLay is placed over RCP; the coping is perforated such that RCP is protruding from it; RCP is cut flush with the coping.Figure 9. A depiction of the ‘Island Technique’ preparation and subsequent DuraLay coping within the laboratory. Diagram adapted from Failure in the Restored Dentition: Management and Treatment by Wise MD, Laurie A.8
Figure 10.
(a–e) Schematic example of ‘Operative appointment 2’ when employing the ‘Island Technique’. Initially, RCP is protruding from the DuraLay coping, however, is reduced level with the coping. The crown is then cemented in place. Articulating marks illustrate that RCP has been maintained in the same position as prior to tooth preparation.
When the patient returns for the fit appointment, the temporary restoration may be removed carefully without damaging any of the tooth structure present.
The same rigid coping used in the laboratory to reduce the occlusal stop should be placed over the tooth.
Any of the maintained occlusal stop protruding from the coping can be removed. From this point, the patient should not be permitted to occlude to avoid superior repositioning of the condyles; the use of a bite prop is strongly encouraged.
The matrix can now be removed from the tooth, and what will remain is a replica of what tooth structure the lab fabricated the restoration on.
The restoration may then be tried, adjusted and cemented in place.8
2. ‘Maintenance of the Condylar Relationship Technique’
Once RCP has been established, the operator may decide to carry on preparing the involved tooth in a usual manner, however, certain factors must be considered first. This technique involves replicating as well as possible the same deflective pattern of RCP–ICP in the final restoration as was originally present intra-orally. This requires skill from both the clinician and the technician. Again, with the advent of digital impression taking, it may be advisable to take a pre-operative scan and a post-preparation scan, such that the final restoration can be fabricated to replicate the original tooth anatomy. The operator should also be confident in constructing a well-fitting temporary restoration that mimics the previous occlusal anatomy and dimensions exactly and will not de-cement between appointments.8 Proper preparation design should be a priority, as it will encourage a stable temporary restoration.12 Occlusal considerations should also be taken into account regarding the temporary restoration, including elimination of unfavourable excursive interferences.5
Operative appointment 1:
The patient must not be permitted to occlude throughout the appointment (perhaps a mouth prop will help) until a temporary restoration has been cemented in place. This will allow the operator to prepare the tooth as usual, and will also have avoided superior repositioning of the condyles. Occlusal reduction may be assessed via the use of a silicone index, as previously described.
Fabrication of a temporary restoration using a sectional matrix method as described in the previous technique is favourable, as it will likely maintain the original deflective occlusal pattern prior to preparation.8
Some operators will choose to make the temporary restoration in supra-occlusion, in an attempt to prop the condyles further, and this may make adaptation to the final restoration easier, and may also create extra occlusal space through intrusion of the tooth and its antagonist. However, there is a higher risk that the temporary restoration will de-cement due to the unusually high loads involved. There is little literature to support or oppose this technique, however, so the technique is not to be recommended.13 The consequence of de-cementation of the temporary restoration is that there will no longer be any occlusal stop on the tooth in question, hence the condyles will be free to reposition, thereby losing inter-occlusal space.
Laboratory stage 1:
The original casts should be examined to determine the deflective pattern from RCP to ICP.
The goal is to obtain a final restoration which best mimics this pattern.
One such method of doing so is by using a matrix of the original tooth to hold wax. This may then be placed on the prepared model, which would, in an ideal world, create a shape identical to the original tooth with an identical slide, however, in practice this may not be identical right away.
The technician then has the ability to adjust and add to the wax to create a similar deflective pattern.
The technician can then burn out the wax and replace with the final restorative material in a furnace.
Alternatively, digital impressions may be employed here, and the final restoration may be fabricated in correlation to the original tooth anatomy that was obtained from the pre-operative scan.
Operative appointment 2:
The patient again should not be permitted to occlude once the temporary restoration has been removed.
The final restoration may then be trial fitted, and the deflective pattern should be examined to see if it is both similar/the same as previously and to make sure that it is suitable and that the patient is comfortable with it.
Once the deflective pattern has been deemed acceptable, the restoration may be cemented in place.
Table 2 shows a comparison between the two aforementioned techniques.
Island Technique
Maintenance of Condylar Relationship Technique
Temporary restoration will automatically mimic the RCP-ICP slide due to the maintenance of the occlusal stop
Temporary restoration design is simpler, and is mainly dictated by the occlusal stop
Comfortable for the patient – little clinicaltime required where they are not permitted to occlude
Temporary restoration de-cementation is not catastrophic as condylar repositioning would not be permitted
Ideal restoration preparation design can be carried out intra-orally, rather than being reliant on the technician
Less scope for lab stage induced errors (iereliance on the final restoration only rather than on the acrylic coping too)
Scope to intrude opposing tooth with a high temporary restoration (little evidence)
Ability to assess how the patient adapts to a slightly different RCP-IC slide
3. ‘Increased OVD and Relative Axial Tooth Movement Technique’
This technique is less favoured due to its lack of predictability, however, has some merit. This technique will often be used if the temporary restoration de-cements or if the patient is permitted to bite down without a temporary restoration:
The operator will prepare the tooth as normal, and may or may not permit the patient to occlude. Once the patient has occluded (either during the appointment or following failure of the temporary restoration), the condyles will have repositioned and occlusal clearance will be lost.
The ‘Dahl principle’ is employed by placing a thin metal restoration on the occlusal surface of the prepared tooth.
Essentially this restoration will then be perceived to be in supra-occlusion at an increased occlusal vertical dimension (OVD), however, despite the bite feeling propped open by the restoration, the occlusion will re-establish full arch contacts as previously through the Dahl principle. This will likely be as a result of intrusion of the restored tooth and through minute extrusion of the rest of the teeth.13
This approach may also be used as a ‘get out of jail’ attempt for poorly planned cases, whereby the tooth has been prepared without adequate consideration of RCP, however, success will vary, and the validity of the principles employed in this technique are still debated widely. Evidence relating to the complications of utilizing the Dahl principle is somewhat lacking, however, some operators may be concerned regarding pulpal symptoms, periodontal issues, temporo-mandibular issues and root resorption.13
4. ‘Regaining Lost Space Technique’
It is important that the patient should be informed of complications and difficulty when restoring a tooth involved in RCP. This should extend to warning the patient that it may be necessary to reduce the tooth opposing the one planned for indirect restoration. It is important to state this to the patient before any invasive procedure is carried out, and full informed consent should be obtained and documented. This technique involves creating necessary inter-occlusal clearance by reducing the height of the opposing tooth to the one due to be restored. Moreover, if the temporary restoration fails and de-cements, the patient's condyles will reposition. Thus, at the fit appointment, it may be necessary to adjust the opposing tooth in order to create sufficient space for the restorative material. It is much easier to inform the patient about the need to reduce the opposing tooth if he/she has been warned and consented previously.
Conclusion
It is clear that there are significant concepts to understand and plan when considering restoration of a tooth involved in the Retruded Contact Position. A decision always needs to be made whether re-organization is desirable or whether conforming to the existing occlusal scheme is the favoured approach. It is important to realize the deflective patterns and movements that occur, and plan around the issues that may arise. This will then allow the operator to employ the particular techniques most suited to the patient and the operator's experience. It is also worth noting that a lot of the time, this issue may not be apparent, and will not always occur. This is likely because the tooth preparation will remove the deflective contact, which will be moved to another tooth. However, by planning ahead, restorative treatment will be delivered in a controlled fashion. It will also allow the operator to assess the suitability of the new RCP that is established and if it has moved to a suitable location.5 It can be seen that thorough occlusal planning and treatment technique are arguably the most important parts of the restoration of a tooth contributing to RCP. Planning ahead will allow the operator to manage the case appropriately, and warn the patient of the complexities involved.