McArdle LW, Renton T. The effects of NICE guidelines on the management of third molar teeth. Br Dent J. 2012; 213
McArdle LW, Renton TF. Distal cervical caries in the mandibular second molar: an indication for the prophylactic removal of the third molar?. Br J Oral Maxillofac Surg. 2006; 44:42-45
McArdle LW, McDonald F, Jones J. Distal cervical caries in the mandibular second molar: an indication for the prophylactic removal of third molar teeth? Update. Br J Oral Maxillofac Surg. 2014; 52:185-189
Falci SG, de Castro CR, Santos RC, de Souza Lima LD, Ramos-Jorge ML, Botelho AM Association between the presence of a partially erupted mandibular third molar and the existence of caries in the distal of the second molars. Int J Oral Maxillofac Surg. 2012; 41:1270-1274
Ozeç I HSS, Taşdemir U, Ezirganli S, Göktolga G. Prevalence and factors affecting the formation of second molar distal caries in a Turkish population. Int J Oral Maxillofac Surg. 2009; 38:1279-1282
Allen RT, Witherow H, Collyer J, Roper-Hall R, Nazir MA, Mathew G. The mesioangular third molar – to extract or not to extract? Analysis of 776 consecutive third molars. Br Dent J. 2009; 206:E23-587
Chang SW, Shin SY, Kum KY, Hong J. Correlation study between distal caries in the mandibular second molar and the eruption status of the mandibular third molar in the Korean population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 108:838-843
McArdle LW. NICE and the third molar debate. Faculty Dent J. 2013; 4:166-171
McArdle LW, Andiappan M, Khan I, Jones J, McDonald F. Diseases associated with mandibular third molar teeth. Br Dent J. 2018; 224:434-440
McArdle LW, Jones J, McDonald F. Characteristics of disease related to mesio-angular mandibular third molar teeth. Br J Oral Maxillofac Surg. 2019; https://doi.org/10.1016/j.bjoms.2019.02.002
Brickley MRT, Evans DJ, Edwards MJ, Armstrong RA, Shepherd JP. Prevalence of third molars in dental practice attenders aged over 35 years. Community Dent Health. 1996; 13:223-227
Hugoson AKC. The prevalence of third molars in a Swedish population: an epidemiological study. Community Dent Health. 1988; 5:121-138
Toedtling V, Coulthard P, Thackray G. Distal caries of the second molar in the presence of a mandibular third molar – a prevention protocol. Br Dent J. 2016; 221:297-302
McArdle LW, Patel N, Jones J, McDonald F. The mesially impacted mandibular third molar: the incidence and consequences of distal cervical caries in the mandibular second molar. Surgeon. 2018; 16:67-73
Dental Checks: Intervals Between Oral Health Reviews. 2004;
The prevention and management of distal cervical caries of the mandibular second molar Louis W McArdle Dental Update 2024 46:5, 707-709.
Authors
Louis WMcArdle
BDS, MSc, FDS RCS(Eng)
Senior Specialist Clinical Teacher and Honorary Consultant Oral Surgeon, Faculty of Dentistry, Oral and Craniofacial Sciences, King's College London, Floor 18, Guy's Tower, Guy's Hospital, London SE1 9RT, UK
Distal Cervical Caries (DCC) of the mandibular second molar has become a more frequent complication of third molar impaction as a direct consequence of the introduction of NICE's guidance on the management of wisdom teeth. NICE's tenet that disease free impacted third molars can be retained is contradicted by the development of DCC on the second molar as its diagnosis asks the simple question of why the impacted third molar was not removed before DCC occurred.
This paper aims to address the features of DCC associated with the second molar and outlines how dentists should address its diagnosis but, more importantly, how to recognize those at risk and how patients should be managed.
CPD/Clinical Relevance: Clinical management of impacted third molar teeth.
Article
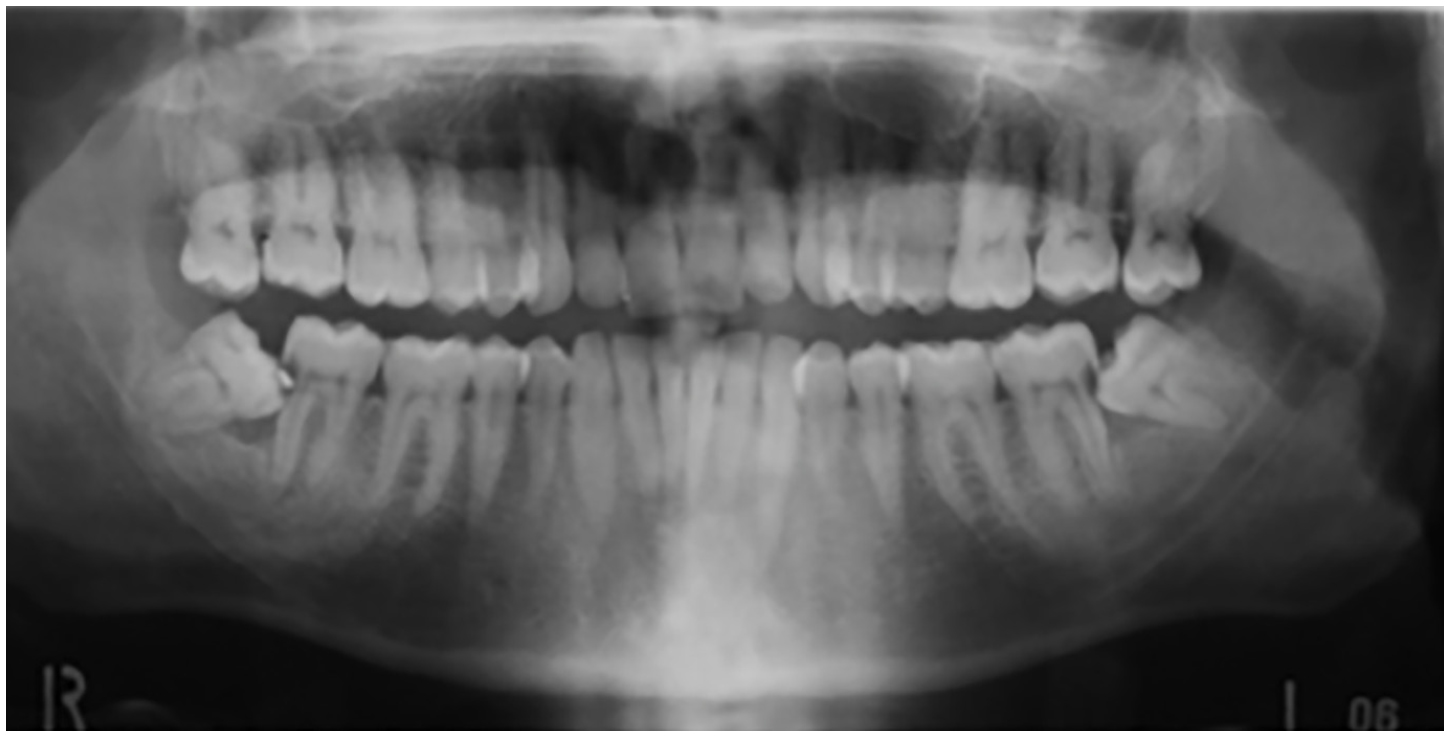
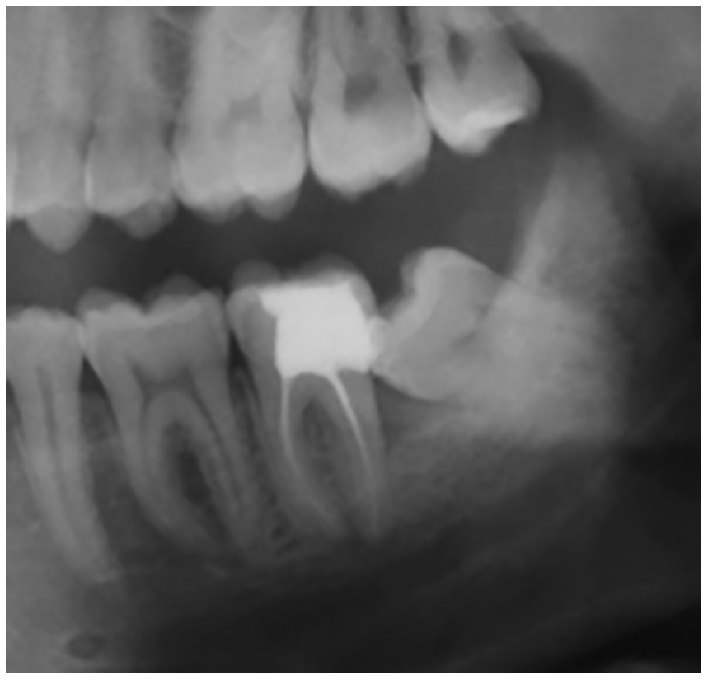
Since the introduction of NICE's guidance on the extraction of wisdom teeth in 2000, the mean age of patients having third molars removed has risen from 28 to 32 years of age.1, 2 In addition, there has been a notable change in the spectrum of disease affecting third molars, with a significant increase in caries-related disease associated with them.2 Distal cervical caries (DCC) of the mandibular second molar (Md2M) has become a more common feature associated with partially erupted mandibular third molar teeth (Md3M) (Figure 1).3, 4, 5, 6, 7, 8 Its occurrence will commonly indicate the surgical removal of the Md3M, not only to allow restoration of the Md2M but also to prevent recurrence of DCC. Md2M DCC is not seen in isolation, it only occurs in the presence of a partially erupted impacted third molar, predominantly mesio-angular impacted Md3M and, less commonly, with horizontally impacted Md3M.3, 4 Reflection and common-sense would invariably question why the Md3M was not removed before DCC could form on the second molar, as this would have prevented additional and preventable treatment. NICE's guidance on the management of impacted third molars proscribes the removal of asymptomatic or disease-free third molars.1 As a consequence, the removal of the Md3M before DCC forms on the second molar is ostensibly contra-indicated, although arguably the prophylactic removal of the Md3M would appear to have a strong indication in this instance. This paradox and the resultant conflict that NICE's guidance creates, namely DCC of the second molar, challenges NICE's orthodoxy and how dentists should manage the potential for this disease.9
Figure 1. Mesio-angular Md3M with Md2M DCC present.
This review paper will look at the significant features of DCC on the second molar and discuss the risk factors associated with it. In addition, it will outline the potential management strategies for patients who are at risk of this type of caries and discuss NICE's guidance when confronted with evidence that challenges it.
Distal cervical caries of the mandibular second molar
Distal cervical caries forms on the distal cervical area of the second molar in the region of the amelo-cemental junction (Figures 1 and 2). The unsuccessful eruption and subsequent partial eruption of the Md3M results in impaction of the third molar against the distal aspect of the second molar. This causes loss of the distal gingival collar of the tooth and exposure of the distal root surface to the oral environment. This anatomical defect is poorly accessible for adequate oral hygiene and, as a consequence, bacteria colonize the area, plaque formation results and caries can ensue. Second molar DCC can be difficult to diagnose clinically, as the carious lesion cannot easily be detected as it is low on the distal root surface, and visualization is impeded by the impacted Md3M itself. Diagnosis is often an isolated finding on radiographic review or when DCC becomes symptomatic for the patient.
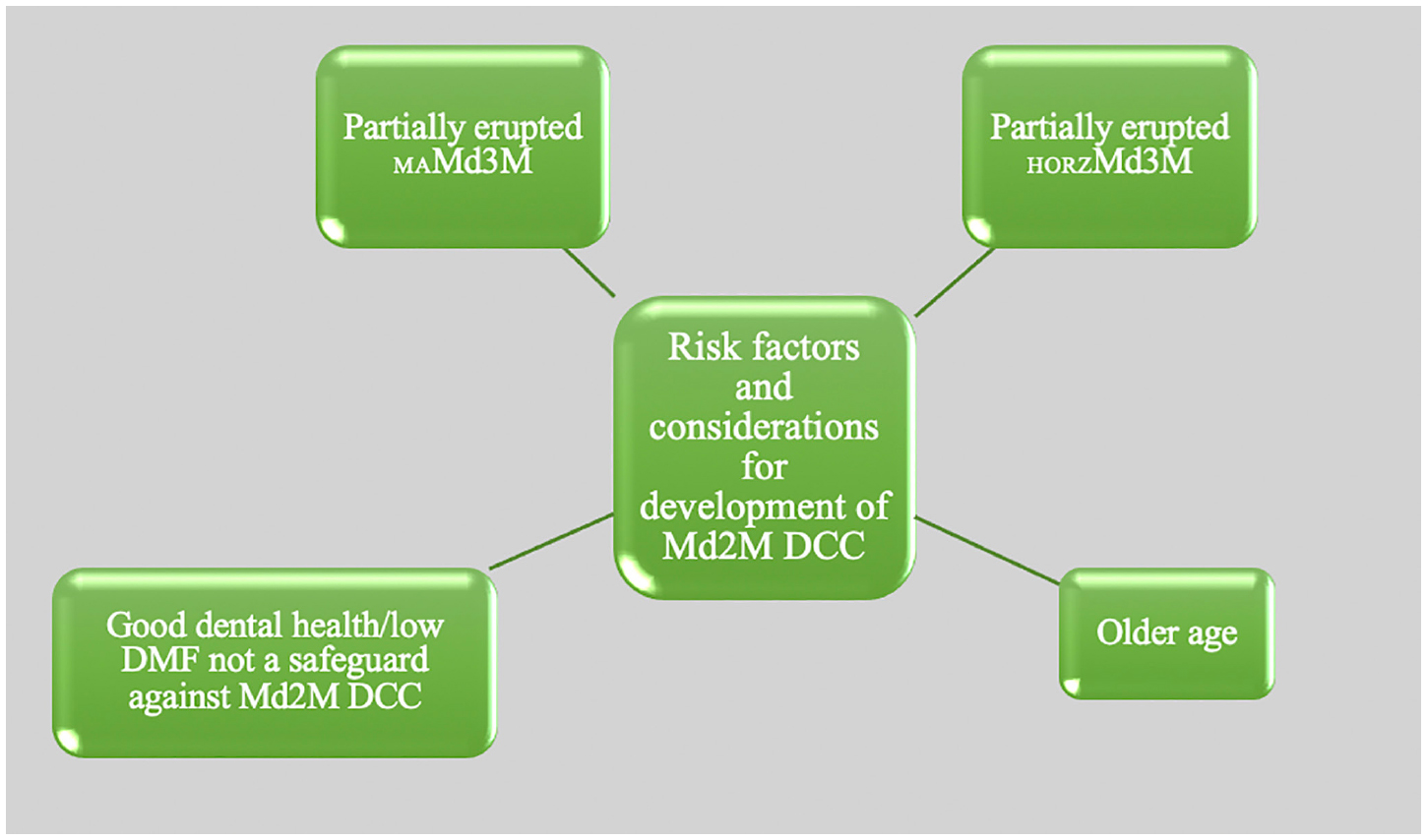
Figure 3. Primary risk factors and characteristics for Md2M DCC.
The principal risk factor for the development of DCC on the second molar is the partially erupted mandibular third molar. DCC is seen mainly in association with mesio-angular third molars, which contributes to 91% of cases of DCC on the second molar.10 It is also seen, to a lesser extent, in horizontal third molars but it has not been seen in association with other impacted third molars and never in the absence of a third molar.10 DCC of the second molar is now responsible for 44% of all mesio-angular third molars removed and 9% of all horizontal third molars removed.10 In contrast, unerupted mesio-angular and unerupted third molars do not give rise to DCC on the second molar as there is no soft tissue deficiency between the unerupted third molar and the second molar for oral bacteria to colonize. However, unerupted third molars should be reviewed to detect for distal pocket development on the second molar, which would act as a portal for bacteria to invade and colonize.
Dental health
Patients who develop second molar DCC tend to have better dental health than average. Studies have shown that the dental health of patients with DCC, as measured by DMFT scores, are approximately 50% less than the average when compared with the adult dental health survey of 1998 and 2009.3, 4 Approximately 70% of patients with DCC have a DMFT of 5 or less and 21% have a DMF score of 0.3, 4 Paradoxically, patients with good dental health are not excluded from DCC forming, as those seemingly at minimal risk of tooth decay are those who should not be overlooked from consideration of the potential for DCC (Figure 2)
Age
Age is an important factor in relation to Md2M DCC, not in the direct development of the disease, but due to the fact that more people retain their third molars later into life as a consequence of the proscription of early prophylactic removal.2 As a consequence of NICE, the spectrum of disease attributed to impacted third molar removal has changed; patients are now older on average with dental caries, in general, becoming more prevalent in third molars.2 In relation to the second molar, the longer a mesio-angular third molar is retained, the greater the potential outcome of DCC forming. The older patients are, the more likely they become susceptible to this type of disease, as evidence demonstrates that the incidence of DCC in older age groups increases.11 Second molar DCC is primarily a disease of older patients, with the mean age of patients presenting with DCC being 32.7 years of age.10 In contrast, the mean age of patients requiring third molar removal due to pericoronitis is 27.5 years. For mesio-angular Md3M, which has the highest incidence of DCC, the mean age of patients is 32.8 years and, for pericoronitis, is 25.5 years. Ominously, the incidence of DCC increases with age, with over 60% of mesio-angular third molars removed in over 30s due to DCC of the second molar.11
Risk – will all mesio-angular mandibular third molars cause DCC of the second molar?
Not every mandibular second molar associated with a partially erupted mesio-angular or horizontal third molar will result in DCC. However, it is not the case that only some second molars will be at risk: hypothetically, all mesio-angular and horizontal third molars will have the potential to cause DCC. The reason we do not see DCC in all cases is that DCC is a late consequence of third molar retention and, in most cases, the partially erupted third molar will be removed before DCC can affect the second molar. Approximately 60% of all impacted third molars are removed before the age of 30 years, with pericoronitis accounting for 65% of all third molars removed in patients below this age.10 Consequently, a large number of patients who could otherwise succumb to DCC become eliminated from the ‘at-risk group’ before DCC can result because their third molar is removed before it can form. In addition, those patients who retain a partially erupted mesio-angular third molar demonstrate an increasing prevalence of DCC as they become older, suggesting that the longer the third molar remains retained, the likelier it will be to result in DCC and the need for third molar removal.11 As patients age, the total number retaining an impacted third molar will continually diminish, as third molar disease will eventually occur resulting in its removal. It is estimated that 80% of all patients with impacted third molars will require removal by the time they are middle-aged.10,12,13
Management
Prevention of second molar DCC and treatment of DCC
All partially erupted mesio-angular or horizontal third molars have the potential to cause DCC on the second molar and, consequently, these types of impacted third molar cannot be ignored. As stated, the DCC lesion can be difficult to detect clinically and, although it has been suggested that regular review and radiographic assessment of patients at risk of DCC should be undertaken to aid in diagnosis of those at risk, this approach is counter-productive.14 The location of DCC is deep on the root surface of the second molar and, consequently, routine bitewing radiographs may omit this area on the image. Radiographic monitoring has one significant limitation as, once the caries has established itself, then the removal of the third molar is indicated to permit restoration and to prevent re-occurrence of the DCC. In effect, an opportunity has been missed to prevent the formation of DCC. Early restoration may ensure the longevity of the second molar, however, 40% of all second molars with DCC end up being removed as a consequence, which results in avoidable and expensive costs. It has been estimated that the overall cost of treating DCC of the second molar is in the region of £27million/annum.15
As stated, the majority of patients who succumb to DCC have better than average dental health as measured by DMF.3, 4 NICE's guidance on dental recalls would notionally afford patients with low DMFT scores the longest recall period of 24 months between dental examinations owing to their relatively good dental health.16 This may again be counter-productive in that, if DCC becomes established in a second molar, then its progression may go unchecked for some time, resulting in a more extensive lesion that may require root canal treatment or even extraction.
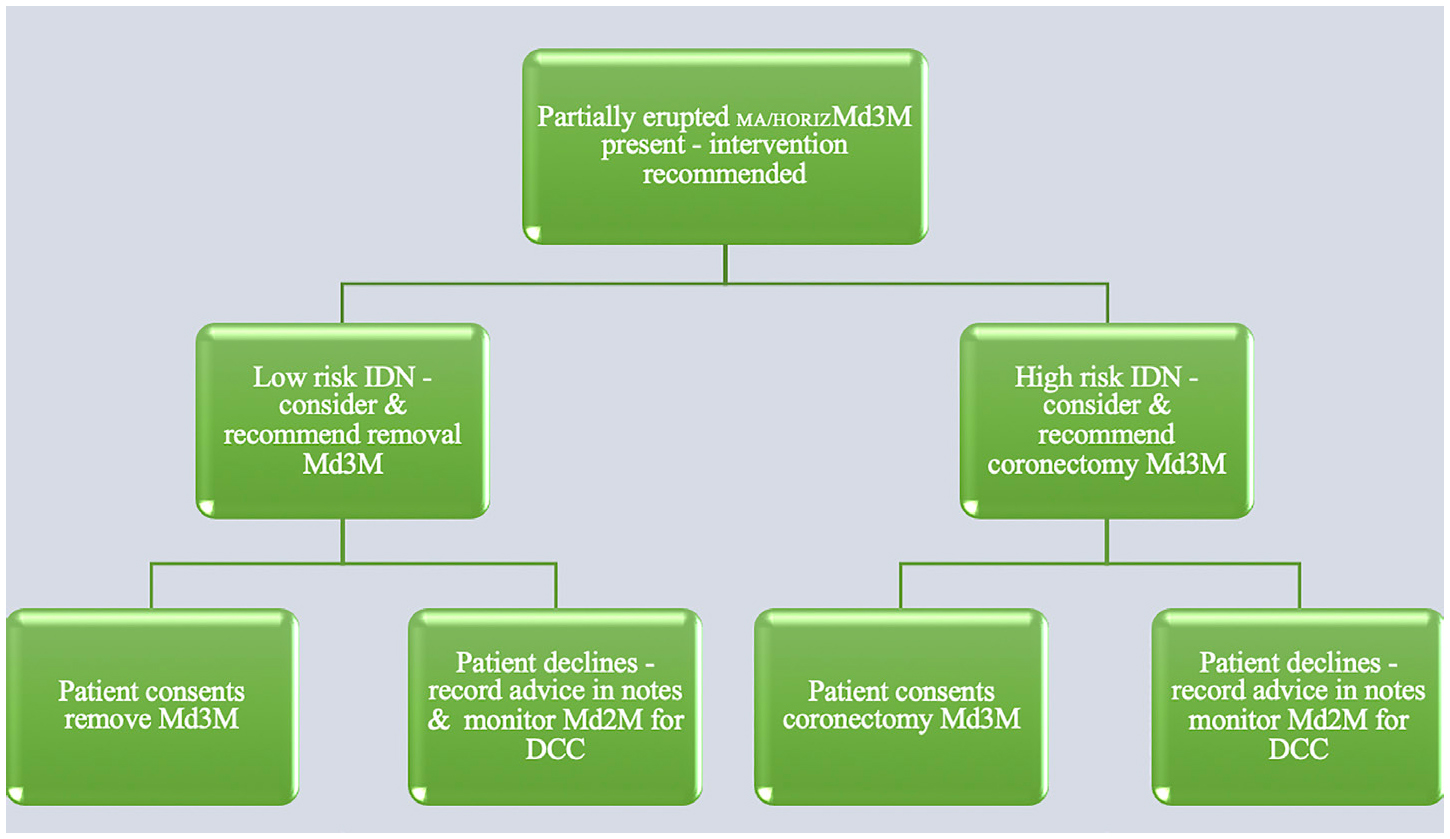
In terms of overall patient management, this poses a problem in that the potential development of DCC would suggest that consideration should be given to the prophylactic removal of the mesio-angular or horizontal third molar before DCC can occur, contrary to NICE guidance. In managing patients with an asymptomatic partially erupted mesio-angular or horizontal third molar, both the dentist and the patient need to appreciate that there is material risk of DCC forming due to the long-term retention of these types of third molars. A discussion should be had with the patient regarding the potential of DCC of the second molar occurring, the relative complexity of restoring this tooth or the possible need for its removal, and the added necessity for third molar removal as well. In the opinion of the author, all partially erupted mesio-angular or horizontal third molars pose this risk and all should be considered and recommended for prophylactic removal. It is always a patient's right to decline advice or treatment, however, the dentist has a duty to patients to put their interests first and advise them accordingly (Figure 4). Retaining an impacted mesio-angular or horizontal third molar that has the risk of contributing to disease on adjacent teeth, with the potential long-term loss of the second molar, cannot be overlooked, even if NICE's guidance proscribes us from recommending removal of such an otherwise asymptomatic tooth.
Figure 4. The dentist has a duty of care to patients to put their interests first and advise them accordingly, however, it is always a patient's right to decline advice or treatment.
Where indicated, patients should be advised of the relative risk of DCC and consideration be given to early intervention, In most cases, this would indicate the removal of the third molar, however, the nature of the intervention and the material risks of removal must also be considered. Post-operative surgical morbidity, in terms of pain and recovery, are generally self-limiting; surgical complications such as alveolar osteitis and infection can be relatively common post-extraction, though treatment is relatively simple. More significantly, the relative risk of inferior dental nerve (IDN) and lingual nerve (LN) injury needs to be considered and correctly assessed – there is no advantage in securing the long-term health and retention of the second molar but causing permanent IDN or LN injury as a consequence. In confirmed high risk cases for IDN injury, coronectomy may be an appropriate intervention to ensure longevity of the second molar whilst minimizing the risk to the IDN. Indeed, no intervention may be decided upon if IDN injury risk is high and acceptance that the loss of the second molar may be an ultimate but acceptable consequence. The possible long-term loss of the second molar will be, by far, a better outcome than third molar removal and permanent nerve injury.
Consent can be a complex process and it is important that patients understand the nature and outcomes for any treatment intervention. However, they also need to understand the outcomes of no treatment. Where no treatment may result in consequent disease and more complex treatment at a later stage, then patients should be informed of this risk and the potential outcomes. The Montgomery vs Lanarkshire Health Board case emphasized the notion of material risk and the value that a patient may place on the relative risks of an intervention,17 however, this principle is also true in terms of the material risk of non-intervention and, consequently, it is the dentist's duty-of-care to inform a patient of the relative material risks of non-intervention too. In this way, patients can make an informed choice related to risk and possible treatments. It is equally important that, when identifying risk, any discussion with the patient related to risk is recorded in the clinical notes. In the face of the evidence, failure to appreciate risk and to document decisions related to it could be misinterpreted as clinical ignorance or, at worst, as supervised neglect. Relevant documentation will support the clinician if patients question the reasons for not intervening early with a third molar when posing a risk to a now carious and unrestorable second molar.
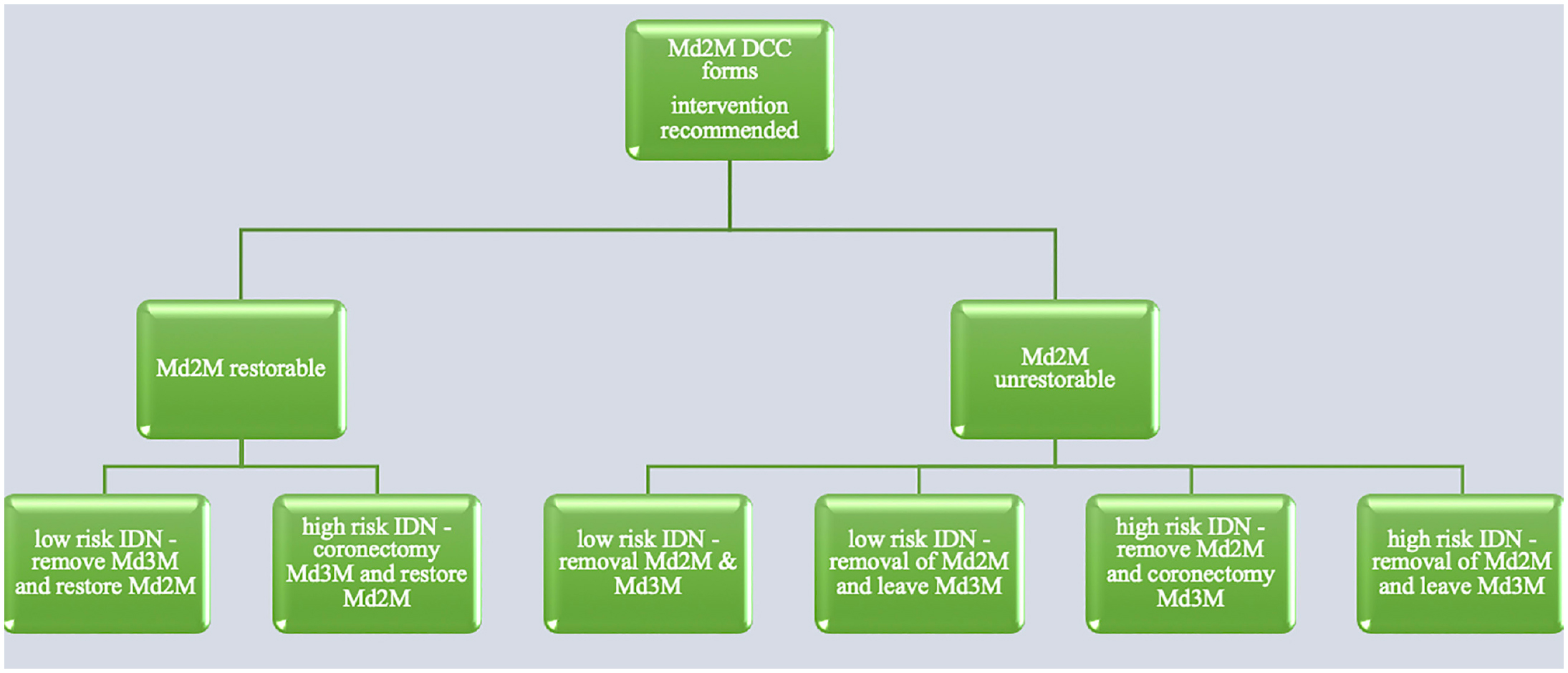
NICE presents us with a paradox when faced with DCC of the second molar. The early, prophylactic loss of the third molar will prevent DCC from forming but this is contrary to NICE's guidance where removal is indicated only in the presence of disease. NICE guidance does need to be reviewed and improved but NICE's guidance is not solely a list of clinical indications for third molar removal. NICE supports any decision related to third molar management as the guidance clearly states that it is just that – guidance – it is not a guideline nor a treatment algorithm. Unfortunately, non-clinical stakeholders, such as the NHS and private commissioners of care, have been misinterpreting the guidance in a monochrome manner to justify fiscal policies of saving money and not focusing on the needs and benefits of the individual patient. With finite amounts of resources, the general objective is to optimize resources and minimize cost, where possible, and third molar management is easy prey to such a policy. As NICE states, ‘…NICE guidance does not override the individual responsibility of health professionals to make the appropriate decisions in the circumstances of the individual patient and in consultation with the patient.’ The circumstances of individual patients and their informed choices should ultimately dictate their management and treatment, not NICE's deficient list of treatment indicators. For those patients who become diagnosed with DCC, restoration or extraction of the second molar is indicated (Figure 5). Where restoration is planned, the third molar will have to be removed to facilitate restoration. Attempting to restore the second molar with the third molar still present can result in a compromised restoration and leave the second molar at risk of further DCC (Figures 6 and 7). If the second molar is unrestorable, or if the patient chooses removal, then consideration may be given to retaining the third molar, especially if the risk of IDN injury is high. Often the second molar can be restored, however, access can be difficult due to the relative depth of the DCC on the root, restricting positioning of a matrix band distally to a good margin for a restoration. Endodontic treatment of the second molar is often indicated as caries can rapidly penetrate into the pulp, resulting in more extensive and expensive treatment. Long-term approximately 40% of second molars associated with DCC are lost.15
Figure 5. Optional treatments for patients diagnosed with distal cervical caries (DCC), ie restoration or extraction of the second molar is indicated.Figure 6. Restored DCC on Md2M.Figure 7. Previously restored Md2M with secondary DCC.
Conclusion
Distal cervical caries of the second molar has become a common disease related to impacted third molars and the relative risks for patients acquiring the disease are well established. DCC is ultimately a preventable disease and eliminating the detrimental effect of the third molar on the second molar will prevent this disease from occurring. Consideration, therefore, needs to be given to patients who are at risk of DCC forming, advice on prevention and early intervention should be considered and discussed and, where clinicians and patients consider and agree that early removal is indicated, then treatment should be undertaken accordingly.