Ellis J, Seymour R, Thomason JM Gingival sequestration of amlodipine and amlodipine-induced gingival overgrowth. Lancet. 1993; 341:(8852)1102-1103
Prisant LM, Herman W. Calcium channel blocker induced gingival overgrowth. J Clin Hypertens. 2002; 4:310-311
Nyska A, Shemesh M, Tal H Gingival hyperplasia induced by calcium channel blockers: mode of action. Med Hypotheses. 1994; 43:115-118
Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol. 1999; 4:1-6
Doong H, Dissanayake S, Gowrishankar T The 1996 Lindberg Award. Calcium antagonists alter cell shape and induce procollagenase synthesis in keloid and normal human dermal fibroblasts. J Burn Care Rehabil. 1996; 17:497-514
Monkman S, Ellis J, Cholerton S Automated gas chromatographic assay for amlodipine in plasma and gingival crevicular fluid. J Chromatogr B Biomed Appl. 1996; 678:360-364
Cune MS, Strooker H, van der Reijden WA Dental implants in persons with severe epilepsy and multiple disabilities: a long-term retrospective study. Int J Oral Maxillofac Implants. 2009; 24:534-540
Silverstein LH, Koch JP, Lefkove MD Nifedipine-induced gingival enlargement around dental implants: a clinical report. J Oral Implantol. 1995; 21:116-120
Lang NP, Wilson TG, Corbet EF. Biological complications with dental implants: their prevention, diagnosis and treatment. Clin Oral Implants Res. 2000; 11:146-155
Chee WW, Jansen CE. Phenytoin hyperplasia occurring in relation to titanium implants: a clinical report. Int J Oral Maxillofac Implants. 1994; 9:107-109
Bevilacqua L, De Biasi M, Lorenzon MG Volumetric analysis of gingival crevicular fluid and peri-implant sulcus fluid in healthy and diseased sites: a cross-sectional split-mouth pilot study. Open Dent J. 2016; 10
Mombelli A. Microbiology and antimicrobial therapy of peri-implantitis. Periodontology 2000. 2002; 28:177-189
Mellado-Valero A, Buitrago-Vera P, Solá-Ruiz MF, Ferrer-Garcia JC. Decontamination of dental implant surface in peri-implantitis treatment: a literature review. Med Oral Patol Oral Cir Bucal. 2013; 18:e869-e876
Bassetti M, Schär D, Wicki B Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: 12-month outcomes of a randomized controlled clinical trial. Clin Oral Impl Res. 2014; 25:279-287
Mavrogiannis M, Ellis J, Thomason J The management of drug-induced gingival overgrowth. J Clin Periodontol. 2006; 33:434-439
Nakou M, Kamma JJ, Andronikaki A Subgingival microflora associated with nifedipine-induced gingival overgrowth. J Periodontol. 1998; 69:664-669
Marshall R, Bartold PM A clinical review of drug-induced gingival overgrowth. Aust Dent J. 1999; 44:219-232
Hall E. Prevention and treatment considerations in patients with drug-induced gingival enlargement. Curr Opin Periodontol. 1997; 4:59-63
Mesa FL, Osuna A, Aneiros J Antibiotic treatment of incipient drug-induced gingival overgrowth in adult renal transplant patients. J Periodont Res. 2003; 38:141-146
Renvert S, Roos-Jansåker AM, Claffey N. Non-surgical treatment of peri-implant mucositis and peri-implantitis: a literature review. J Clin Periodontol. 2008; 35:305-315
Amlodipine-induced gingival overgrowth in the peri-implant region: a review and case report Neil MacBeth Stephen Sterlitz Graeme Bryce Dental Update 2024 46:3, 707-709.
Authors
NeilMacBeth
BDS, MSc, FFGDP, MGDS, MFGDP, MFDS, FDS(Rest), Consultant in Restorative Dentistry, Defence Primary Health Care Centre for Restorative Dentistry, Evelyn Woods Road, Aldershot, GU11 2LS, UK
Surgeon Commander (D) Graeme Bryce Royal Navy, Consultant in Restorative Dentistry, Centre for Restorative Dentistry, Defence Primary Health Care (Dental), Evelyn Woods Road, Aldershot, GU11 2LS
Gingival overgrowth is a known side-effect of the antihypertensive drug amlodipine, but the risk of mucosal overgrowth around dental implants has been less well documented. This article discusses the role of calcium channel blockers in drug-induced mucosal overgrowth around dental implants and describes the preventive and surgical management of the case.
CPD/Clinical Relevance: The report describes the management of a patient with an implant-supported restoration who presented with peri-implantitis and drug-induced mucosal overgrowth. The review discusses how amlodipine and other medications, commonly associated with drug-induced gingival overgrowth, impact on the management of implant patients.
Article
Introduction
Drug-induced gingival overgrowth (DIGO) around teeth
Several different medications have been reported to induce gingival overgrowth,1 with the three most common being: anticonvulsants, immunosuppressants and calcium channel blockers (CCBs). Despite differences in the pharmacological actions of each protagonist group, they are similar in that they alter the host tissue response, resulting in an increase in collagen synthesis and cellular changes within the connective tissue. The prevalence of gingival overgrowth varies, with a reporting incidence of 50% for phenytoin (anticonvulsant), 25–30% for cyclosporine (immunosuppressant), 5–20% for nifedepine and 3% for amlodipine (CCBs).2 The incidence of gingival overgrowth is three times higher in males,3,4 with the difference attributed to the effect of testosterone on fibroblast proliferation and collagen stimulus.5 The influence of plaque as an associated factor in gingival overgrowth is well established and acknowledged in the Armitage classification of periodontal disease.6
Calcium channel blockers and gingival overgrowth
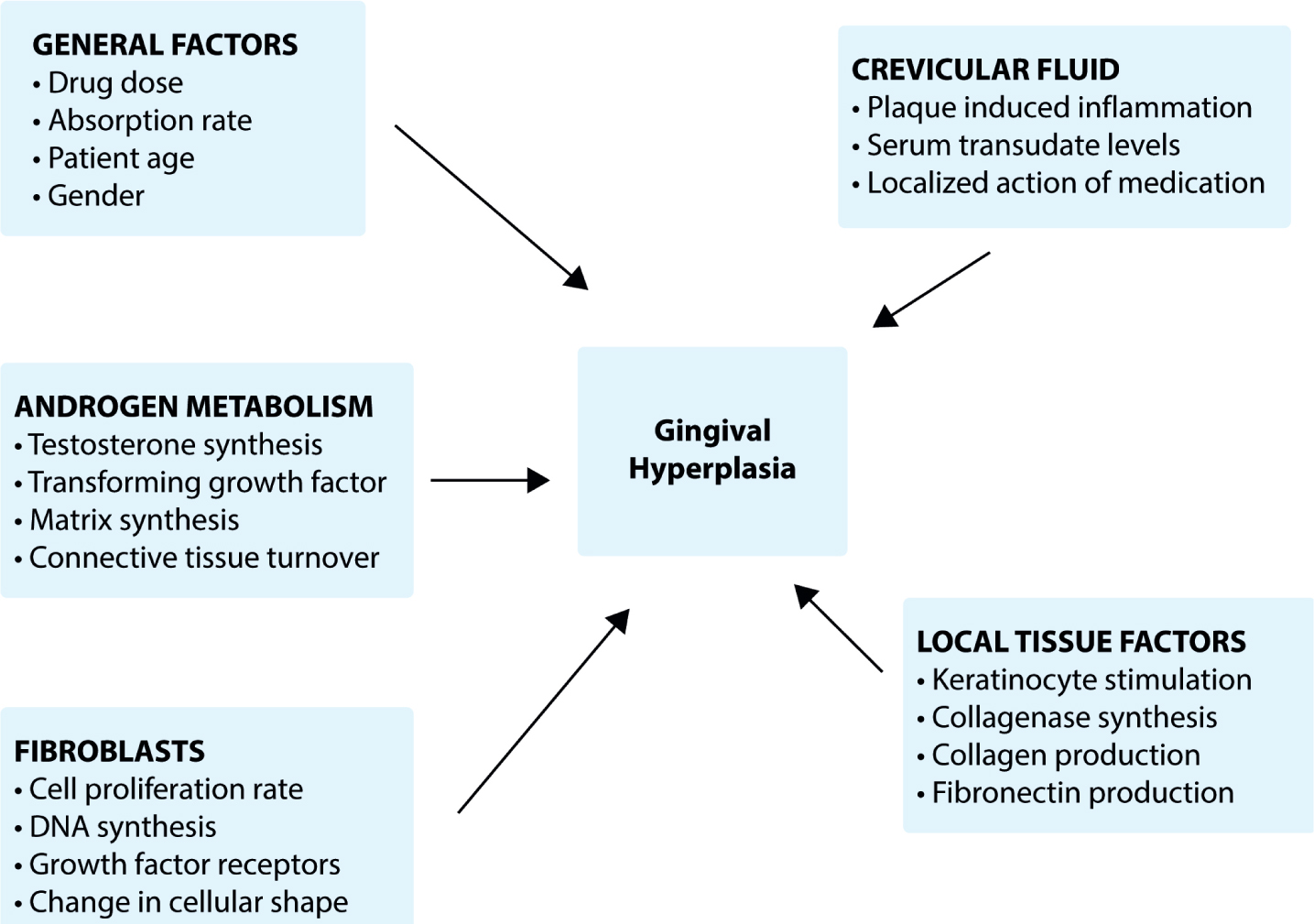
Calcium channel blockers, prescribed for the treatment of coronary hypertension and angina, prevent calcium ion flow through trans-membranous voltage gated channels, into the intercellular structure of cells. The resulting ionic imbalance reduces the activation of the intercellular actin-myosin complex of the smooth muscle cells and inhibits muscular contraction. The precise action of CCB on the gingival tissues is complex, with cellular interactions resulting in altered fibroblast shape, proliferation rate, DNA synthesis and increased numbers of growth factor receptors (Figure 1).7 This stimulation of fibroblasts results in increased collagen production with subsequent thickening of the connective tissue layer of the gingivae.
Figure 1. Reported actions of CCB on gingival tissues.
Clinically, CCB-induced gingival overgrowth has been characterized by interdental papilla enlargement, inflammation and the formation of fibrotic gingival lobules, which may extend into the coronal and free gingival areas. The severity of overgrowth has been associated with general factors that include: the administered dose, rate of absorption and older age-groups. Plaque-induced inflammation may also directly affect the severity of overgrowth as serum-derived levels of CCB are 290 times higher in the crevicular fluid, when inflammation is present.8
Mucosal overgrowth around implants
Mucosal overgrowth around an implant-supported restoration has been previously reported,9,10 with associated causative factors including ill-fitting and poorly contoured prostheses and the presence of implant mucositis or peri-implantitis.11 The incidence of drug-induced mucosal overgrowth (DIMO) at implant sites is less well reported, although isolated case reports have identified the prescription of nifedipine and phenytoin as a contributory factor.10,12 The commonality that exists between the peri-implant sulcular fluid,13 microbiota and inflammatory mediators, at both inflamed peri-implant and tooth-sites,14 presents the likelihood that inflammatory mediators and CCBs synergistically act to develop a similar environment for the promotion of both DIGO and DIMO.
Case presentation
This case report describes amlodipine-induced mucosal overgrowth at an implant site and its contribution to the development of peri-implantitis. A 45-year-old Tanzanian male received dental implant therapy to rehabilitate his traumatically lost upper and lower incisors. Implant fixtures positioned in the UR2, UR1, UL1 UL2, LR1 and LR2 sites (Brånemark Mk III, Nobel Biocare, Ca USA) were used to support fixed maxillary and mandibular bridges superstructures. Treatment was undertaken using strict operative and prosthetic protocols, with the maintenance schedule including oral hygiene instruction (OHI), a preventive regimen with the dental hygienist and a biannual clinical review with prosthetic staff.
At 18-months post treatment completion, the patient was diagnosed with coronary hypertension and prescribed a regimen that included amlodipine (10 mg) medication. At the 24-months review appointment, the patient presented with a discharge from an area of soft tissue enlargement around the LR1 implant abutment. He reported difficulty in cleaning the area due to gingival enlargement.
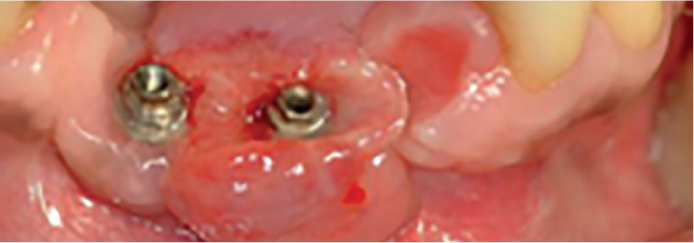
At presentation, an erythematous and oedematous mucosal overgrowth (15 x 20 mm in diameter) was present at the abutment level of the LR1 and LR2 implant fixtures (Figure 2). The enlarged tissue obliterated the embrasure and sub-pontic areas of the implant bridge, with expansion and ulceration of the tissue labio-lingually beyond the margins of the prosthesis (Figure 3).
Figure 2. Intra-oral view showing the appearance of the DIMO lesion extending around the fit surface of the patient's implant-supported fixed bridge.Figure 3. Intra-oral view showing the extent of the DIMO lesion post-removal of the bridge.
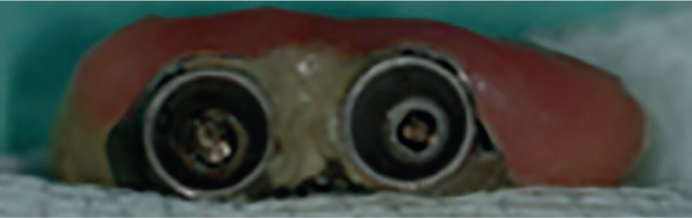
A full mouth 6-point pocket chart recorded probing depths of less than 4 mm in all dentate areas, with the presence of 8-and 5-mm suppurating pockets on the labial and interproximal surfaces of the LR1 and LR2 implants, respectively. Plaque and gingivitis scores were low but heavy calculus deposits were noted in a concavity present in the ridge lap pontic surface of the bridge (Figure 4).
Figure 4. The presence of calcified deposits on the fit-surface of the bridge.
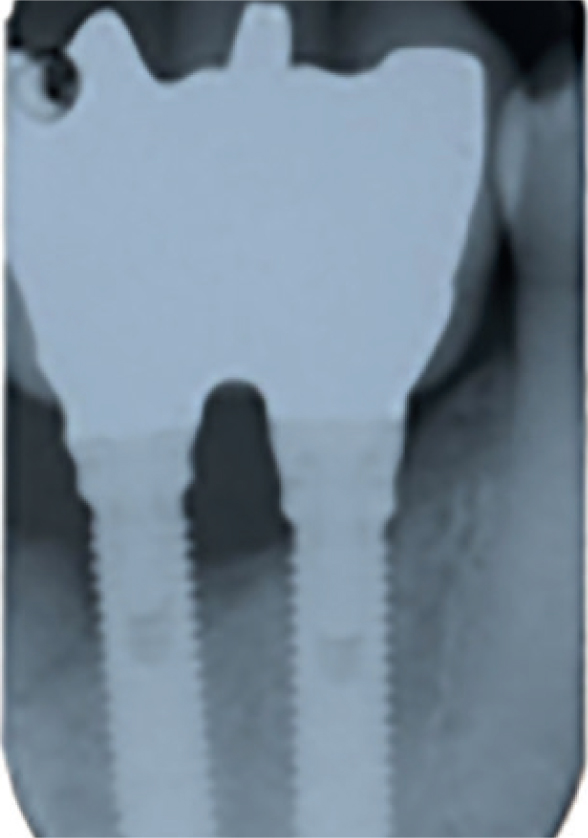
A periapical radiograph (Figure 5) revealed saucerized bone loss extending to the sixth thread of the LR1 implant. The patient was diagnosed with peri-implantitis of the LR1 implant in combination with amlodipine-induced mucosal overgrowth around the prosthetic structure.
Figure 5. Peri-apical radiograph of the lower dental implants with bone loss evident to the sixth thread of the LR1.
Initial treatment involved reshaping the mucosal fit-surface of the implant bridge, to improve access for single-tufted brushes and Superfloss® (Proctor & Gamble Limited, OH, USA) OH measures (Figure 6). Non-surgical debridement (NSD) of the implant surface was undertaken, under local anaesthesia, using titanium implant scalers (Hu-Friedy, IL, USA) and rubber polishing cusps. In addition, Dentomycin® topical gel (2% minocycline, Henry Schein Holdings Limited, Kent, UK) was applied to the peri-implant pockets at 1-week intervals for 3-weeks. The patient's general medical practitioner was contacted, requesting a change in the patient's hypertensive medication.
Figure 6. The fit-surface of the bridge following recontouring to improve access for oral hygiene measures.
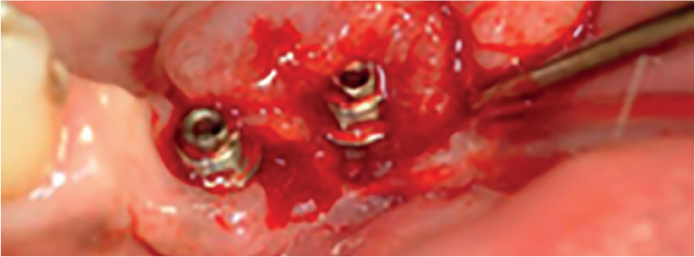
At 3-month review, the mucosal ulceration, bleeding and suppuration had resolved, with the pocketing around the LR1 implant fixture reduced from 8- to 6-mm. The mucosal overgrowth had not decreased in size. Surgical excision of the overgrowth was then undertaken concomitantly with apical repositioning of the tissue to achieve pocket reduction (Figure 7). A sample of tissue was sent for histopathological examination. In the immediate post-operative period, healing abutments were placed on the implants. Following stabilization of the peri-implant mucosal health, the original implant-supported bridge was further reshaped and then refitted in conjunction with OHI reinforcement (Figure 8).
Figure 7. Intra-oral view showing the resection of mucosal overgrowth prior to apical repositioning of the tissues.Figure 8. Intra-oral view showing oral hygiene demonstration using single-tufted brush.
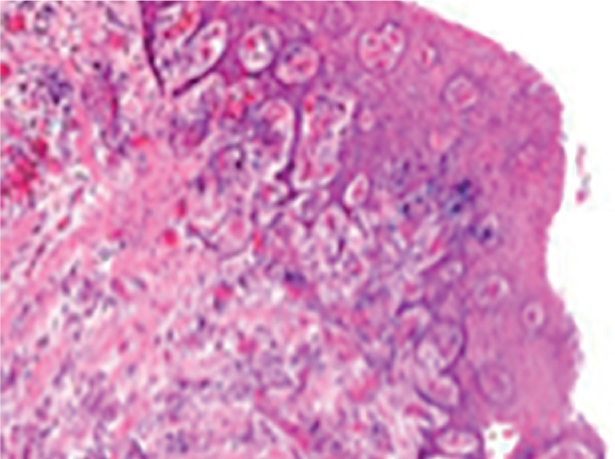
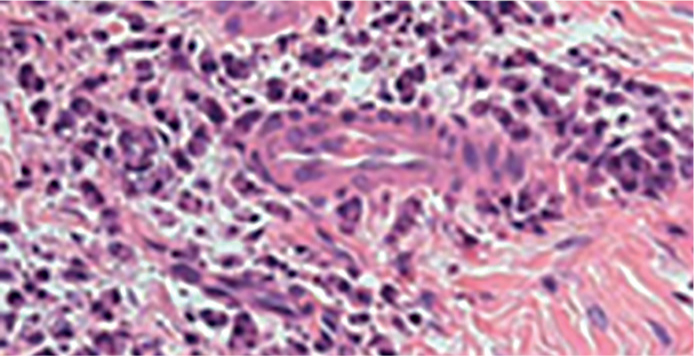
The histopathogical report of the excised tissue described reactive hyperplasia of the connective tissue, dense infiltration of the lamina propria by a chronic inflammatory cell population (predominantly lympho-plasmacytes) and an acanthotic parakeratinized epithelium surface, which had elongation of the rete ridges (Figures 9 and 10). These findings were consistent with the histopathological features observed in CCB-related gingival overgrowth.5
Figure 9. Histological view of resected mucosal overgrowth, with evidence of elongated rete ridges.Figure 10. Histological view of resected mucosal overgrowth, at increased magnification, showing dense infiltration of lympho-plasmacytes.
At the 4-months review, the peri-implant mucosa was noted to be pink and healthy, with a 3 mm band of attached keratinized mucosa present and implant probing depths recorded at less than 3 mm (Figures 11 and 12). The patient was then placed on a 4-month maintenance programme, to monitor the mucosal health and to provide prophylactic scaling and further OH instruction.
Figure 11. Review of implants at 4-months with healthy peri-implant tissues and probing depths within normal limits.Figure 12. Review of prosthesis in situ.
Discussion
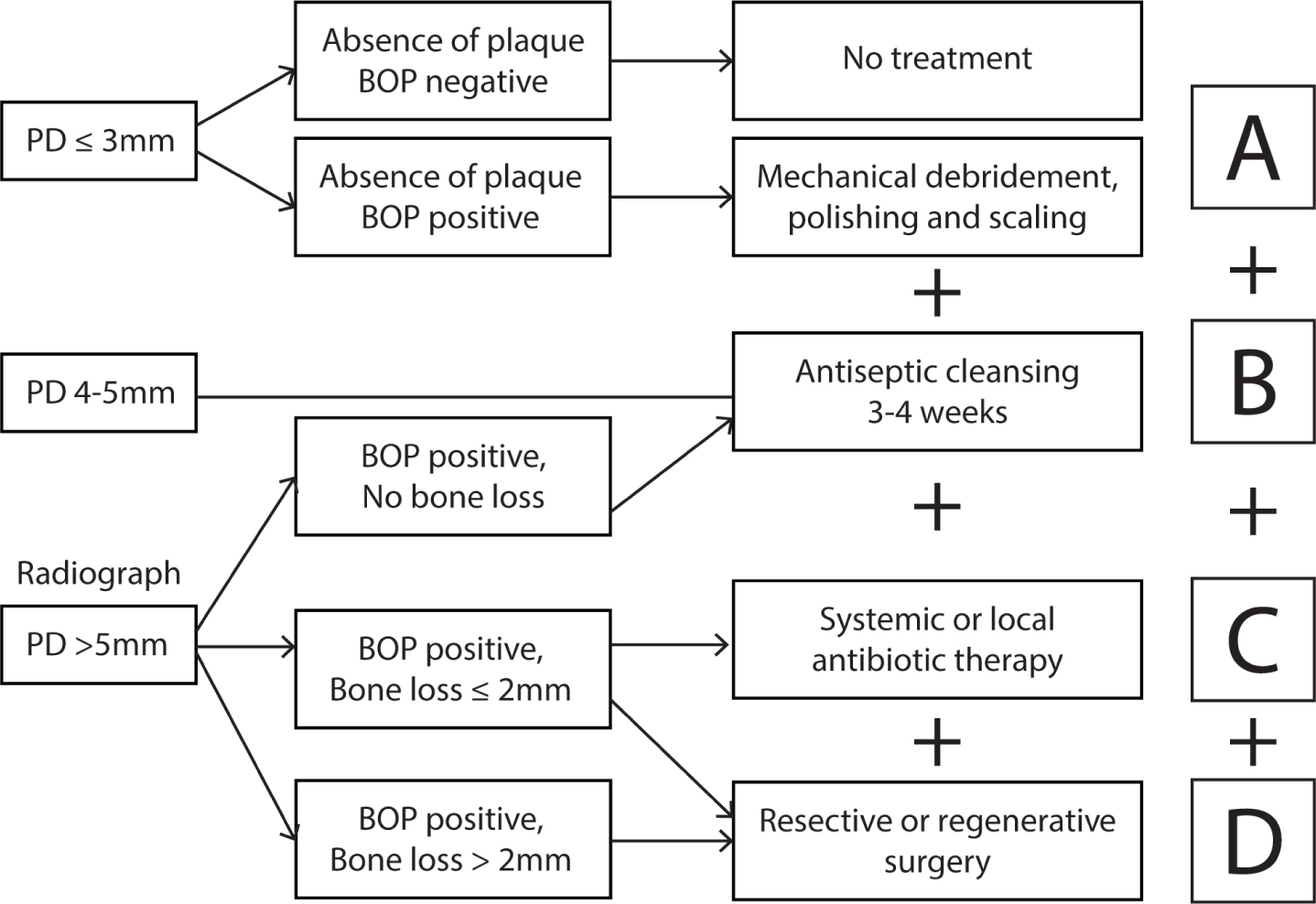
The management of this case required established treatment protocols for both peri-implantitis and DIGO/DIMO. The Cumulative Interceptive Supportive Therapy (CIST)11 is a regimen based on targeting the treatment of clinical findings around dental implants that include: the presence/absence of plaque, bleeding on probing, pocket depth and peri-implant bone loss.15 To summarize, initial phases of the strategy focus on ensuring optimal plaque control, in combination with NSD and/or antibiotics or disinfectant agents (Figure 13).11 Surgical approaches, such as open flap debridement, resective or regenerative surgical approaches are reserved for pocket depths >5 mm that have failed to respond to non-surgical therapies.
Figure 13. CIST protocol.
Laser therapy has also been considered as an alternative to antibiotics as a non-surgical means of decontaminating dental implant surfaces,16 without damaging the surface.14 However, despite the elimination of bacteria and inflammation, clinically relevant reduction of probing depths has been shown to be minimally effective at 12-months.17 In addition, diode lasers without the application of a photosensitizing substance may result in an unacceptable increase in implant body temperature.16
In a similar vein to peri-implantitis, DIGO can be managed by both non-surgical and surgical techniques.18 Non-surgical techniques involve the withdrawal or substitution of the affective medication, instigation of enhanced oral hygiene measures, NSD19,20 and enrolment within a periodontal maintenance programme. However, as in this case, changing the affective medication may fail to correct the mucosal overgrowth; a problem that has been previously reported with DIGO, especially with patients on long-term medication regimens.21 Other non-surgical techniques proposed to reduce gingival overgrowth include the use of chlorhexidine gluconate mouthwash22 and antibiotics, such as azithromycin and metronidazole.23
The failure of the non-surgical phases of this patient's therapy to eliminate pockets or mucosal overgrowth mirrors the uncertainty of the effectiveness of these procedures to manage both conditions.18,24 In this case, a surgical approach aimed at resecting the mucosal overgrowth and inflamed peri-implant collar achieved pocket reduction and improved the access for patient-led oral hygiene. The subsequent prognosis for the implants and prosthesis was judged to be good.
Conclusion
Patients taking calcium channel blockers may be susceptible to mucosal enlargement around dental implants and should be advised of the risks and managed appropriately when it occurs;
The cause of peri-implantitis/DIMO is often multi-factorial and requires careful assessment to achieve an accurate diagnosis;
The implementation of the CIST protocol led to effective management of peri-implantitis and DIMO in the presented case.