White DA, Tsakos G, Pitts NB, Fuller E, Douglas GV, Murray JJ Adult Dental Health Survey 2009: common oral health conditions and their impact on the population. Br Dent J. 2012; 213:567-572
Larato DC. Intrabony defects in the dry human skull. J Periodontol. 1970; 41:496-498
Tal H. The prevalence and distribution of intrabony defects in dry mandibles. J Periodontol. 1984; 55:149-154
Wouters FR, Salonen LE, Hellden LB, Frithiof L. Prevalence of interproximal periodontal intrabony defects in an adult population in Sweden. A radiographic study. J Clin Periodontol. 1989; 16:144-149
Tomasi C, Koutouzis T, Wennstrom JL. Locally delivered doxycycline as an adjunct to mechanical debridement at retreatment of periodontal pockets. J Periodontol. 2008; 79:431-439
Matuliene G, Pjetursson BE, Salvi GE, Schmidlin K, Bragger U, Zwahlen M Influence of residual pockets on progression of periodontitis and tooth loss: results after 11 years of maintenance. J Clin Periodontol. 2008; 35:685-695
Ower P. BPE Guidelines: British Society of Periodontology Revision 2016. Dent Update. 2016; 43:406-408
Davies KJ, Drage NA. Adherence to NICE guidelines on recall intervals and the FGDP(UK) Selection Criteria for Dental Radiography. Prim Dent J. 2013; 2:50-56
Tsitoura E, Tucker R, Suvan J, Laurell L, Cortellini P, Tonetti M. Baseline radiographic defect angle of the intrabony defect as a prognostic indicator in regenerative periodontal surgery with enamel matrix derivative. J Clin Periodontol. 2004; 31:643-647
Cortellini P, Carnevale G, Sanz M, Tonetti MS. Treatment of deep and shallow intrabony defects. A multicenter randomized controlled clinical trial. J Clin Periodontol. 1998; 25:981-987
Matthews DC. Prevention and treatment of periodontal diseases in primary care. Evid Based Dent. 2014; 15:68-69
Cobb CM. Non-surgical pocket therapy: mechanical. Ann Periodontol. 1996; 1:443-490
Renvert S, Nilveus R, Egelberg J. Healing after treatment of periodontal intraosseous defects. V. Effect of root planing versus flap surgery. J Clin Periodontol. 1985; 12:619-629
Nibali L, Pometti D, Chen TT, Tu YK. Minimally invasive non-surgical approach for the treatment of periodontal intrabony defects: a retrospective analysis. J Clin Periodontol. 2015; 42:853-859
Froum SJ, Coran M, Thaller B, Kushner L, Scopp IW, Stahl SS. Periodontal healing following open debridement flap procedures. I. Clinical assessment of soft tissue and osseous repair. J Periodontol. 1982; 53:8-14
Nyman S, Lindhe J, Rosling B. Periodontal surgery in plaque-infected dentitions. J Clin Periodontol. 1977; 4:240-249
Nyman S, Gottlow J, Karring T, Lindhe J. The regenerative potential of the periodontal ligament. An experimental study in the monkey. J Clin Periodontol. 1982; 9:257-265
Karring T, Nyman S, Lindhe J. Healing following implantation of periodontitis affected roots into bone tissue. J Clin Periodontol. 1980; 7:96-105
Nyman S, Karring T, Lindhe J, Planten S. Healing following implantation of periodontitis-affected roots into gingival connective tissue. J Clin Periodontol. 1980; 7:394-401
Polson AM, Proye MP. Fibrin linkage: a precursor for new attachment. J Periodontol. 1983; 54:141-147
Haney JM, Nilveus RE, McMillan PJ, Wikesjo UM. Periodontal repair in dogs: expanded polytetrafluoroethylene barrier membranes support wound stabilization and enhance bone regeneration. J Periodontol. 1993; 64:883-890
Wikesjo UM, Nilveus R. Periodontal repair in dogs: effect of wound stabilization on healing. J Periodontol. 1990; 61:719-724
Wikesjo UM, Lim WH, Thomson RC, Hardwick WR. Periodontal repair in dogs: gingival tissue occlusion, a critical requirement for GTR?. J Clin Periodontol. 2003; 30:655-664
Kao RT, Nares S, Reynolds MA. Periodontal regeneration – intrabony defects: a systematic review from the AAP Regeneration Workshop. J Periodontol. 2015; 86:(2 Suppl)S77-104
Esposito M, Grusovin MG, Papanikolaou N, Coulthard P, Worthington HV. Enamel matrix derivative (Emdogain(R)) for periodontal tissue regeneration in intrabony defects. Cochrane Database Syst Rev. 2009; (4)
Farina R, Simonelli A, Minenna L, Rasperini G, Trombelli L. Single-flap approach in combination with enamel matrix derivative in the treatment of periodontal intraosseous defects. Int J Periodontics Restorative Dent. 2014; 34:497-506
Troiano G, Laino L, Zhurakivska K, Cicciu M, Lo Muzio L, Lo Russo L. Addition of enamel matrix derivatives to bone substitutes for the treatment of intrabony defects: a systematic review, meta-analysis and trial sequential analysis. J Clin Periodontol. 2017; 44:729-738
Castro AB, Meschi N, Temmerman A, Pinto N, Lambrechts P, Teughels W Regenerative potential of leucocyte- and platelet-rich fibrin. Part A: intra-bony defects, furcation defects and periodontal plastic surgery. A systematic review and meta-analysis. J Clin Periodontol. 2017; 44:67-82
Sculean A, Nikolidakis D, Nikou G, Ivanovic A, Chapple IL, Stavropoulos A. Biomaterials for promoting periodontal regeneration in human intrabony defects: a systematic review. Periodontol 2000. 2015; 68:182-216
Takei HH, Han TJ, Carranza FA, Kenney EB, Lekovic V. Flap technique for periodontal bone implants. Papilla preservation technique. J Periodontol. 1985; 56:204-210
Cortellini P, Tonetti MS. Improved wound stability with a modified minimally invasive surgical technique in the regenerative treatment of isolated interdental intrabony defects. J Clin Periodontol. 2009; 36:157-163
Trombelli L, Farina R, Franceschetti G, Calura G. Single-flap approach with buccal access in periodontal reconstructive procedures. J Periodontol. 2009; 80:353-360
Liu S, Hu B, Zhang Y, Li W, Song J. Minimally invasive surgery combined with regenerative biomaterials in treating intra-bony defects: a meta-analysis. PLoS One. 2016; 11
Graziani F, Gennai S, Cei S, Cairo F, Baggiani A, Miccoli M Clinical performance of access flap surgery in the treatment of the intrabony defect. A systematic review and meta-analysis of randomized clinical trials. J Clin Periodontol. 2012; 39:145-156
Cortellini P, Stalpers G, Mollo A, Tonetti MS. Periodontal regeneration versus extraction and prosthetic replacement of teeth severely compromised by attachment loss to the apex: 5-year results of an ongoing randomized clinical trial. J Clin Periodontol. 2011; 38:915-924
Intrabony periodontal defects present a clinical challenge in the treatment of periodontal disease and maintenance of compromised teeth. The management of such defects ranges from non-surgical mechanical debridement to modern minimally invasive regenerative surgery. The incidence of intrabony defects is discussed along with prognosis and likely outcomes of various treatment options.
CPD/Clinical Relevance: Vertical or intrabony (IB) defects are a common occurrence in patients suffering from advanced periodontal disease. Primary care practitioners must be aware of possible treatment options in order to make suitable referrals when initial phases of treatment prove unsuccessful.
Article
Periodontal disease management is taking ever greater importance in dental professionals' daily lives, as caries prevalence reduces from 48% of teeth in 1998 to 26% in 2009.1 The number of adults retaining teeth into old age is increasing and, as such, a significant proportion of these patients will present with periodontal pathology: in 2009, 19% of 55–64 year-olds presented with pockets of 6 mm or more;1 35% of all 55–64 year-olds in 1988 were registered as edentate; whereas the figure for this age group had reduced to just 5% in 2009.
Patterns of destruction of tissue, and particularly bone, due to periodontitis are well established, and are classified dependant on the location of the base of the pocket relative to the alveolar bone crest. Generally, periodontal bone loss follows the pattern of horizontal bone loss, but a significant proportion of sites will present with a vertical defect, also known as an intrabony defect. A bacteria-induced ‘dysbiosis’ affecting the inflammatory pathways within the periodontal tissues can lead to osteoclastic activation and destruction of bone. If this pattern occurs to leave a ‘trough’ around the tooth, with the base of the defect apical to the surrounding bone crest, it is termed an ‘intrabony’ or ‘angular’ defect.
Prevalence
Studies examining human skulls have stated that the prevalence of intrabony defects around teeth ranged from 4.1%–9.4%,2,3 whereas radiographic assessments of an adult population in Sweden have found that prevalence may reach as high as 32% of individuals.4 The presence of such anatomical features can lead to difficulties in conventional periodontal management of deep pockets,5 with intrabony defects reducing the likelihood of pocket closure, along with other factors such as presence of plaque and furcation defects. The presence of such defects may perpetuate deep periodontal pockets due to the difficulties in subgingival biofilm removal.
The risk of tooth loss due to periodontal disease is known to increase, not only as a result of anatomical factors such as intrabony defects, but also with the depth of the periodontal pocket present.6 Matuliene et al demonstrated the increased risk of tooth loss with greater depth of pockets: for example a 6 mm pocket tooth has an 11 times greater odds of loss than a tooth with a 3 mm pocket or less.6 Deep pockets, particularly with unfavourable anatomy, such as the intrabony defect, therefore demand treatment to avoid depletion of the dentition.
Identification of defects
As part of a thorough clinical assessment, a detailed history should be obtained from the patient to help determine the risk for periodontal disease. The recent British Society of Periodontology ‘Good Practitioner’ guidelines present the recommended interpretation of a Basic Periodontal Examination (BPE) score.7 Once a BPE score of 3 (pocket between 3.5 and 5.5 mm) is reached, that sextant should undergo a course of non-surgical periodontal therapy, before a 6 point periodontal chart is obtained 8–12 weeks following treatment. Any score of 4 (6 mm pocket and above) should initiate a full mouth periodontal charting both before and after the initial phase of treatment. Whilst such periodontal probing and charting will indicate the presence of residual pockets, radiographic assessment using intra-oral radiographs will indicate the pattern of bone loss and the type of defect. The FGDP guidelines from 2013 describe the need for vertical bitewings with pocketing of less than 6mm with little recession, whereas in cases of deeper pockets and more evidence of loss of attachment, a periapical should be considered.8 Panoramic radiographs can be considered when large numbers of intra-oral periapicals are required.
An intrabony defect can be assessed using these tools and specific factors relating to this, such as defect depth, width, angulation and morphology may influence the treatment choice and outcome in the long-run. Tsitoura et al looked at the baseline defect angle and compared it with the outcome of treatment.9 Narrow defects, with a small angle between the defect wall and the root surface, performed better in terms of CAL gain. Deeper defects tend to show greater clinical improvements following surgery, however, this has been shown to be a simple result of the defect magnitude, rather than any difference in the regenerative potential of deep versus shallow defects.10
When should a referral be considered?
The competent and skilled dentist should be aware of the necessity, on occasion, to seek specialist advice and treatment for complex issues in various disciplines. Periodontology will be managed mainly in the primary care setting, particularly moderate chronic periodontal disease, which should respond well to high quality non-surgical management. The SDCEP guidance ‘Prevention and treatment of periodontal diseases in primary care’ states that BPE scores of 1–3 should be managed in primary care.11 If a score of 4 is recorded, and this patient fails to respond to non-surgical management, referral may be considered. Patients with a BPE score of 4 plus a modifying condition such as diabetes, or those with a diagnosis of aggressive disease, should be referred. Local guidelines are commonly available from NHS Health Board websites stating the restorative or periodontal departmental criteria for acceptance. Importantly, patients should demonstrate a positive attitude towards oral hygiene in order to be accepted for specialist treatment.
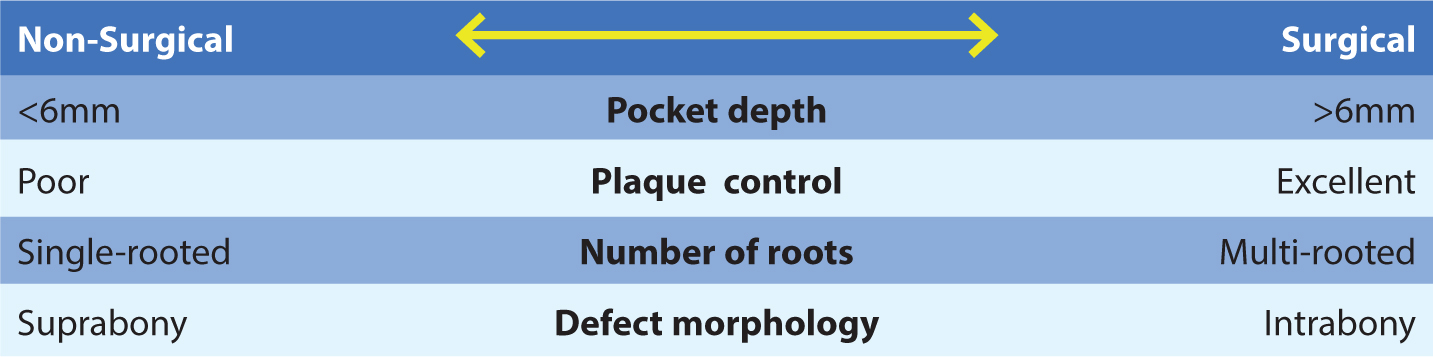
A detailed periodontal assessment, including pocket depths, clinical attachment loss, furcation pathology, bleeding on probing, plaque scores and radiographic assessment, will allow the practitioner to determine the complexity of the case and the likelihood of the diseased site responding to the available treatment. Intrabony defects reduce the likelihood of treatment success and, along with level of plaque control, pocket depth, tooth type and patient motivation, should form a basis of a potential need to refer for specialist advanced treatment (Figure 1).
Figure 1. Guidance for treatment of residual periodontal pockets: factors which may lead the clinician to follow further non-surgical therapy, or consider the use of a surgical approach to treatment.
Non-surgical management (NSM)
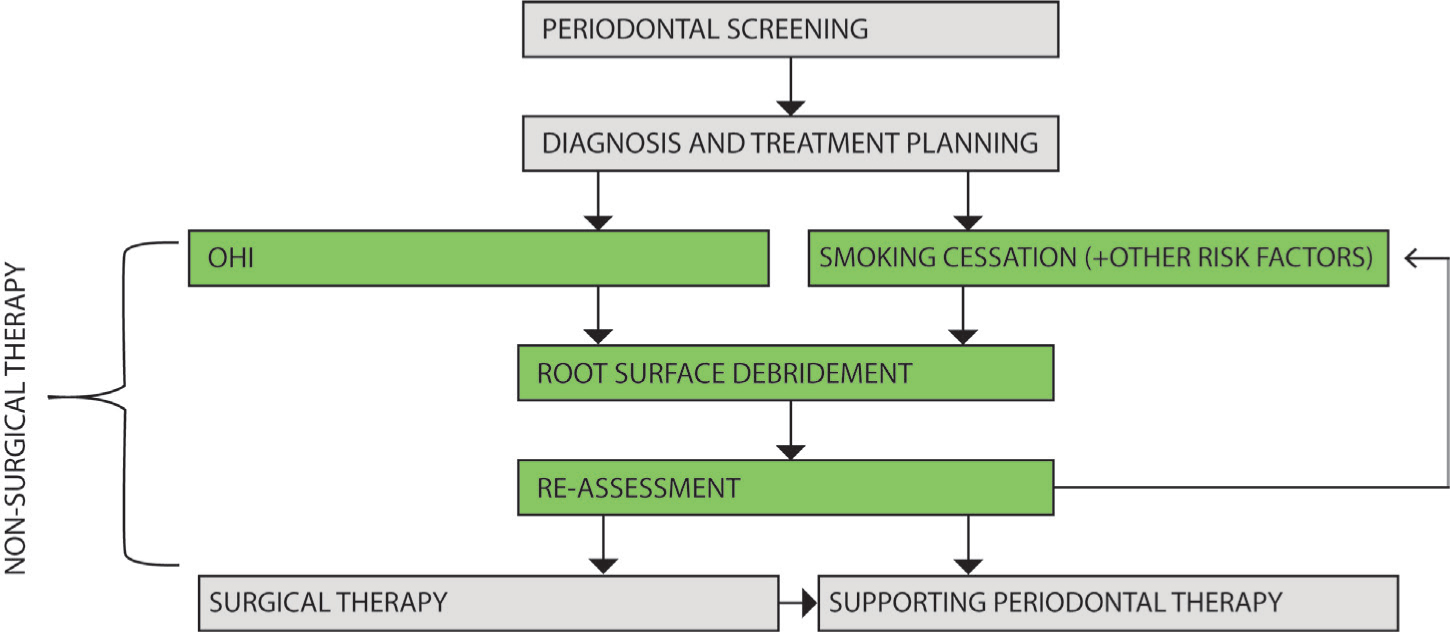
Non-surgical means of disrupting and controlling the bacterial biofilm, which may initiate periodontal tissue destruction, is the mainstay treatment for periodontal disease, and has been refined and optimized to minimize the need for more advanced treatment.12 A course of periodontal treatment is, by convention, initiated with at least one course of non-surgical treatment (Figure 2). Studies assessing the benefit of NSM of IB defects demonstrated a variety of improvement in clinical attachment gain from 0.8 mm13 to 2.8 mm.14 The modern concepts promote a minimally invasive strategy which involves:
Thorough supra- and subgingival debridement;
Use of a magnification system;
Prevalent use of an ultrasonic device with ultra-thin tips and mini gracey-curettes; and
Caution to preserve soft tissue integrity. These factors are likely to optimize this method of treatment.
Figure 2. Conventional pathway of periodontal disease management. Adapted from the BSP ‘Good Practitioner's Guide to Periodontology’: (www.bsperio.org.uk).
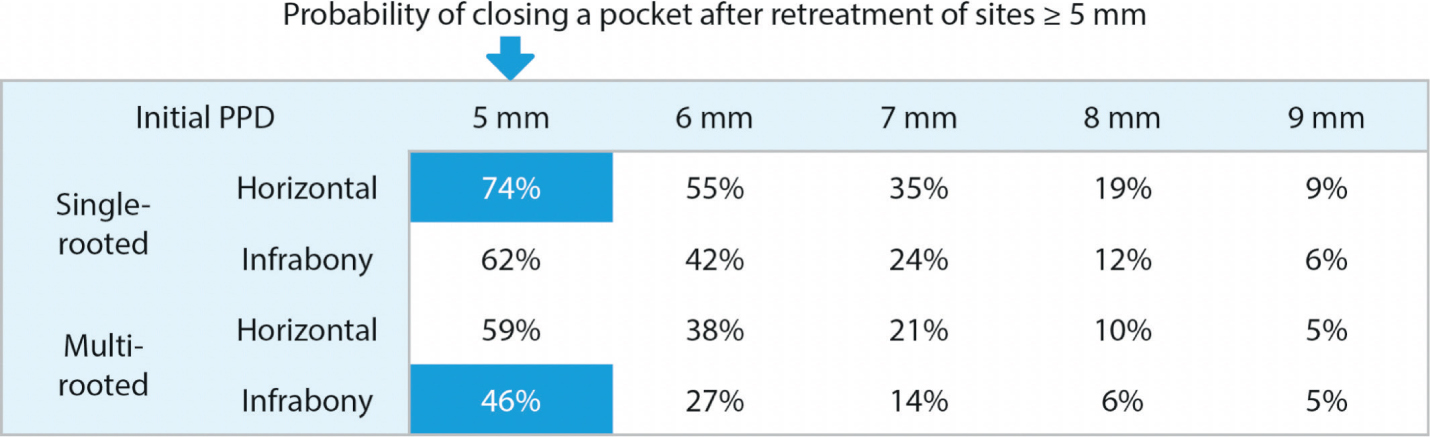
What are the chances of success in a second round of non-surgical management? The likelihood of pocket resolution (ie 4 mm or less) has been studied in re-treatment of periodontal defects (following one initial course of NSM) by Tomasi et al.5 This included the effect of variables such as single versus multi-root, absence or presence of plaque, and intrabony versus horizontal lesion. In favourable conditions, ie single root, horizontal defect and 5 mm pocket, the probability of closing a pocket is as high as 74% for re-treatment with mechanical debridement alone. However, in a less favourable scenario such as a multi-rooted tooth with an intrabony defect, and with just 1 mm more pocket depth of 6 mm, the probability of closure plummets to 27% (Figure 3). This study emphasizes the need to avoid a ‘one-size fits all’ treatment, and that careful diagnosis can predict the success of treatment.
Figure 3. Multilevel assessment of probability of pocket closure, and the influence of intrabony anatomy, pocket depth and the great reduction in likelihood of re-treatment success of mechanical debridement, eg highlighted 5 mm pockets. With permission from Professor Cristiano Tomasi and the Journal of Periodontology.5
Surgical management
Conventional surgery
Polson and Heijl15 and Froum et al16 have shown that successful treatment with a conventional periodontal access flap can lead not only to successful pocket resolution but, given the right conditions, bring out the innate regenerative potential of the periodontal apparatus. Polson and Heijl showed a mean of 2.5 mm of bone regeneration using a conventional modified Widman flap (MWF) approach to surgical periodontal therapy of intrabony defects. These studies emphasized the absolute pre-requisite for success of excellent pre-operative and post-operative plaque control. Without this, any attempts at treatment will fail, regardless of how well they are performed.17
Guided tissue regeneration (GTR) principle
A classic series of in vivo experiments from the 1980s18,19-20 demonstrated the regenerative potential of the periodontal ligament cells. They demonstrated that cells from the periodontal ligament have the capacity to regenerate the periodontal attachment, including the formation of new cementum with inserting collagen fibres and alveolar bone, whereas gingival connective tissue and bone do not. These studies went on to suggest that occluding unfavourable cell types from defects, guided tissue regeneration would lead to optimal periodontal regeneration. A significant body of research data undertaken since this early work by Polson and Proye,21 Haney et al22 and Wikesjo et al23,24 have shown that, although tissue occlusion may play an important role, the key factors leading to successful periodontal regeneration include:
Wound (or clot) stability;
Space provision;
Primary intention healing;
Defect characteristics; and
Innate potential for regeneration.
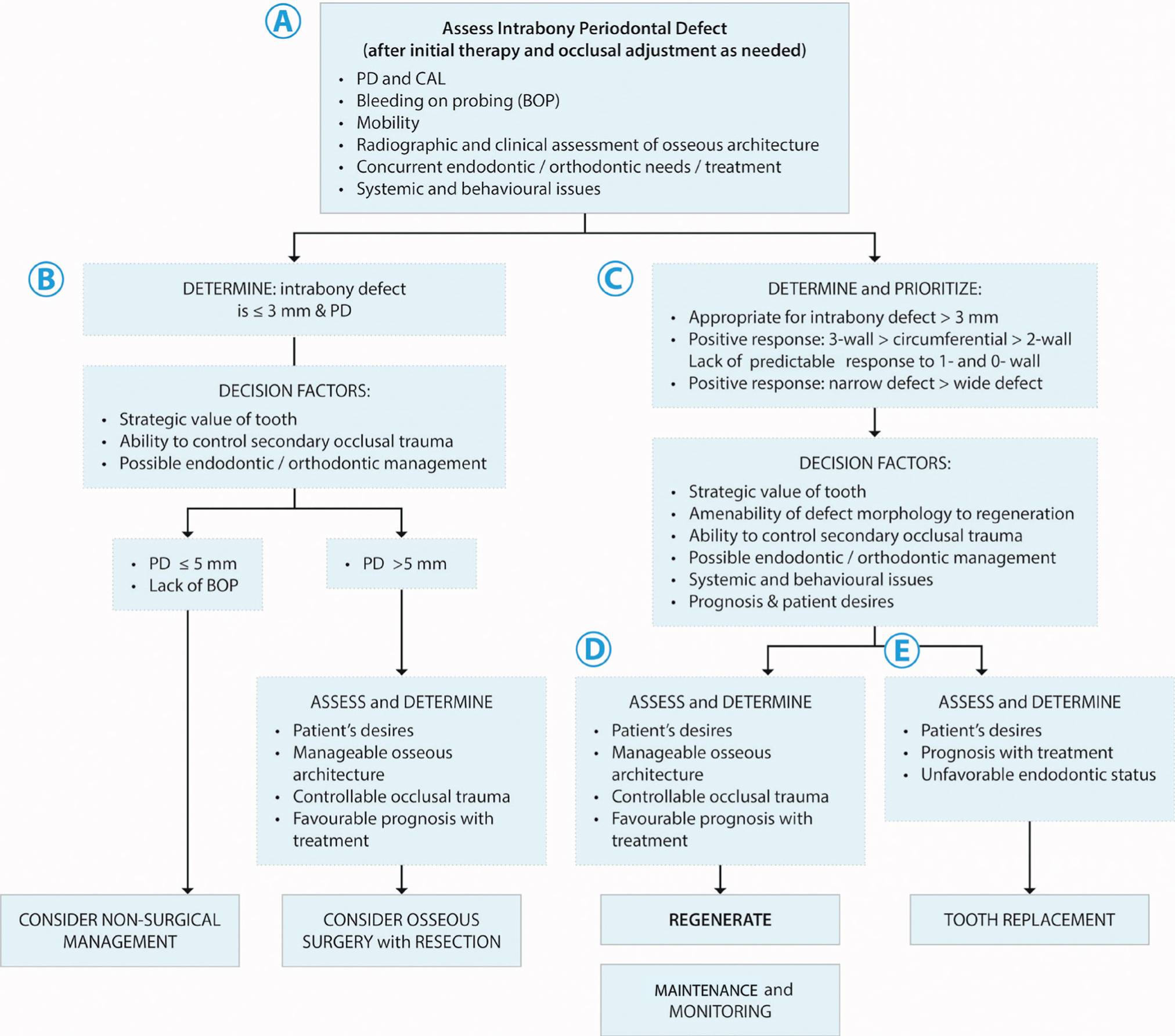
Clinically, the technique of GTR has been successfully validated over numerous clinical trials summarized by systematic reviews.25,26 A clinically relevant benefit above traditional open flap debridement/modified Widman flap (MWF) surgery has been demonstrated with improved reduction in pocket depths, attachment gain and reduced recession. Careful case selection is critical and an example decision tree (Figure 4) can help guide clinicians when determining which sites require specific treatment.
Figure 4. A decision tree regarding intrabony defects and the related pockets. The management may range from non-surgical, through surgical management to extraction. With permission from Dr Richard Kao and the Journal of Periodontology.25
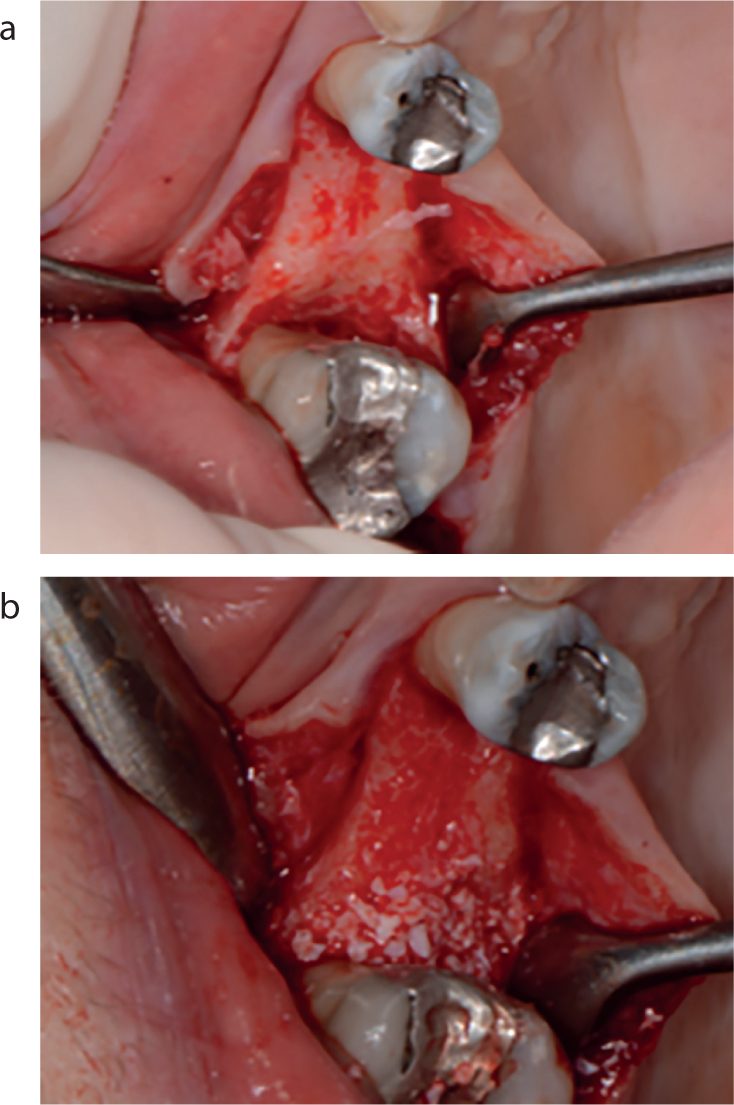
Grafting materials can be used in such situations, especially in combination with non-supporting resorbable membranes, in order to provide space provision as well as an osteoconductive or inductive scaffold dependant on the material of choice (Figure 5).
Figure 5.
(a, b) Intrabony crater on the mesial surface of the maxillary right second molar. The defect is debrided and granulation tissue removed, with deproteinized bovine bone mineral used to provide an osteoconductive matrix for the blood clot within the defect.
Biologics
An increased understanding of the cellular and molecular mechanisms underpinning tissue regeneration has led to increased interest in isolating particular proteins and cell signalling molecules, in order to optimize clinical regenerative techniques.
Enamel matrix derivative (EMD, Emdogain) is a biomaterial developed with enamel matrix proteins which may adhere to the surface of the debrided root within a periodontal defect and encourage regeneration of the periodontal tissues. The precise mechanism of action of this treatment is not wholly clear due to the multitude of proteins and growth factors present in the material. The biomaterial is postulated to mimic the events during the formation of the periodontal ligament. The presence of enamel matrix proteins may in fact encourage cementum formation and eventually complete periodontal regeneration.
Again, clear clinical benefit has been demonstrated above traditional periodontal surgical methods,27,28 with 1.1mm more clinical attachment gain and 0.9mm more pocket reduction than open flap debridement.
Taking into account the key factors governing successful regeneration, a solution alone such as Emdogain cannot successfully regenerate unfavourable conditions alone. The mechanical stability of grafts in combination with this bioactive compound have been used in less favourable (eg 1-walled) defects28 to develop a combination approach of different strategies to improve overall outcomes for patients. A recent systematic review addressed the issue of treating intrabony defects with bone substitute alone, or in combination with Emdogain. The included studies demonstrated no significant difference, however, this review states that defect morphology is not detailed in the data assessment, thereby not allowing subgroup analysis of the benefits of control and test groups in different defects with varying anatomical morphology (eg one or three-walled).29
This area of regeneration research is moving quickly, with compounds such as platelet-derived growth factor and bone morphogenic proteins being assessed independently of, and in combination with, grafting materials. A recent systematic review assessing the use of platelet rich fibrin (patients' own blood spun in a centrifuge to isolate beneficial compounds) in the surgical treatment of intrabony defects showed a significant clinical benefit above open flap debridement.30
The overall aim is to refine regenerative techniques, and those which show promise in cellular studies are further assessed in vivo and clinically validated.31,32
Current strategies: minimally invasive surgery
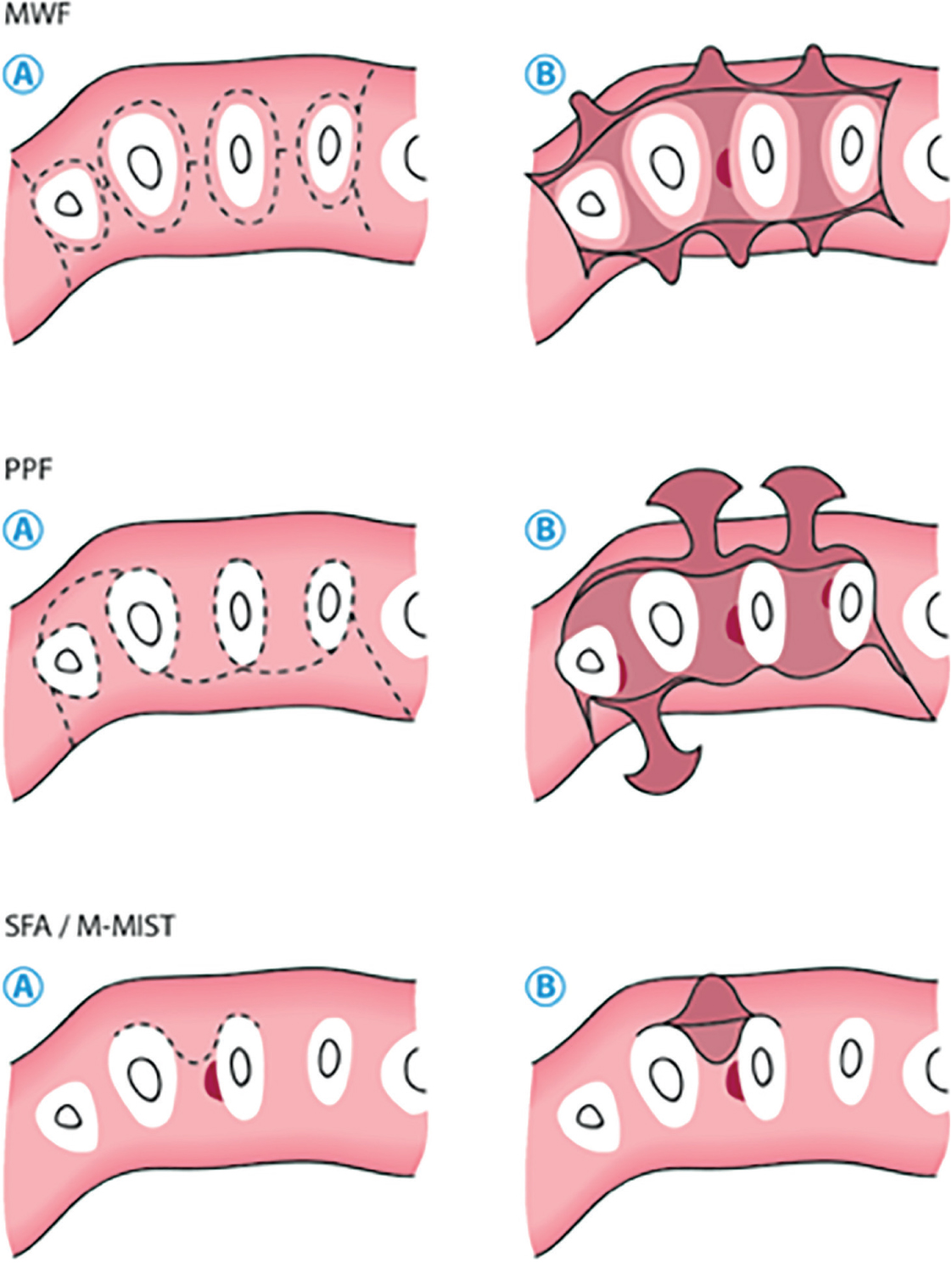
With the advent of microsurgical techniques and minimally invasive flap designs, the outcomes of regenerative treatment of intrabony defects have been refined and improved, both to optimize treatment outcomes but also improve patient comfort. Papilla preservation flaps (PPF) were first presented by Takei et al32 (Figure 6), and have been developed towards a ‘single-flap’ (SFA) or ‘Modified-minimally invasive surgical technique’ (M-MIST) (Figure 7).33,34 These approaches, with suitable supportive mattress sutures, allow the ideal conditions for regeneration to be achieved: a stable clot, primary intention healing, blood supply and space maintenance.
Figure 6. Papilla preservation flap (PPF) in surgical periodontal treatment.Figure 7. Schematic diagram representing incisions and flap designs for traditional periodontal surgery through papilla preservation and ‘single-flap’ (SFA) or ‘Modified-minimally invasive surgical technique’ (M-MIST).
A systematic review recently assessed the clinical outcomes of such minimally invasive surgery, treating intrabony defects with and without biomaterials (such as grafts and EMD).35 Interestingly, there appeared to be no additional benefit of biomaterials, above and beyond the minimally invasive surgery. This perhaps emphasizes the importance of creating the correct environment, and utilizing the innate potential of the periodontal tissues, rather than relying on biomaterials to achieve the desired outcomes.
Furthermore, Graziani et al, in systematically reviewed data on access flap treatment of IB defects, provided a meta-analysis and separated conventional surgical approaches from modern ‘conservative’ surgical approaches, such as those mentioned (Figure 7), and demonstrated improved outcomes in pocket depth reduction and clinical attachment gain with modern flap designs.36 Clearly, the flap design and surgical approach has a major impact on the outcomes measured following treatment.
Summary
The boundaries of what is possible have been questioned by Cortellini et al.37 This study showed remarkable results in sites which may be considered ‘hopeless prognosis’ teeth (bone loss to or beyond the apex). Even with such severe loss of attachment, sites have been regenerated with astounding radiographic bone gain of 8.5 mm and pocket reduction of 8.8 mm. In this study, periodontal regeneration was compared with prosthetic replacement, and success rates of the treatment group compared favourably with control. Very careful case selection was emphasized by the authors, as well as the need to follow strict maintenance programmes.
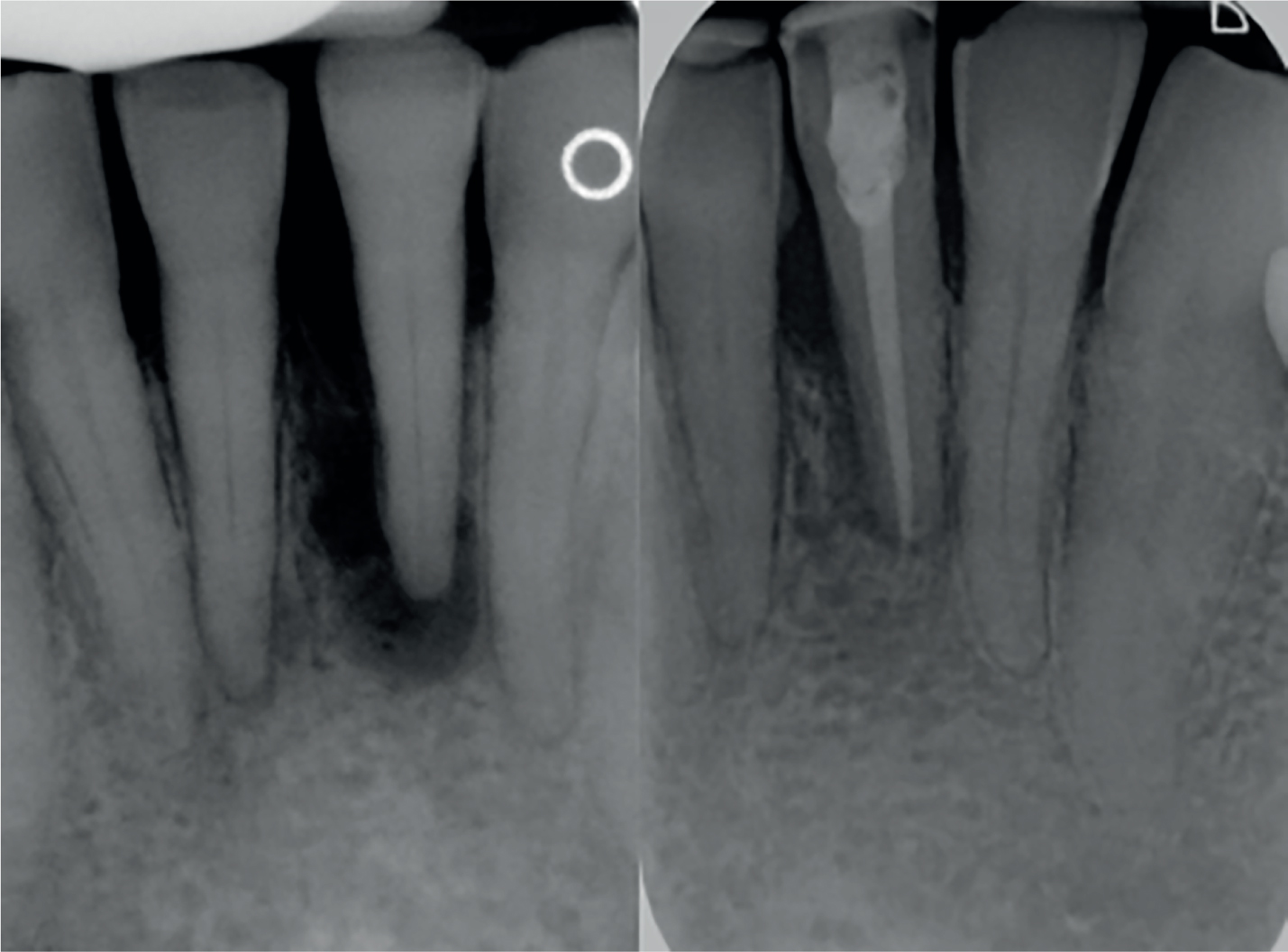
The clinicians in this study utilized minimally invasive flap designs, resorbable and non-resorbable membranes, bone graft materials and EMD. Utilizing the vast wealth of research on this topic, this data has shown a glimpse of what might be possible in the treatment of teeth which were previously consigned to the ‘bucket’ (Figure 8). Despite the emergence of dental implants, dentists must strive to maintain patients' dentitions for as long as possible as life expectancy rises. Implants replace missing teeth, not functional teeth.
Figure 8. Intrabony defect with endodontic lesion. After initial endodontic therapy followed by periodontal treatment, the defect resolved and clear bony infill has occurred, changing the prognosis of this tooth dramatically.
Thankfully, improvements in non-surgical treatment protocols and advances in surgical management mean that, more than ever before, dentists and specialists are able to maintain a dentition compromised by severe periodontal disease.