Scottish Government. A Healthier Future – Action and Ambitions on Diet, Activity, and Healthy Weight: Consultation. 2017. http://www.gov.scot/Publications/2017/10/1050 (Accessed April 2018)
Wright W, Turner S, Anopa Y, McIntosh E, Wu O, Conway DI, Macpherson LM, McMahon AD. Comparison of the caries-protective effect of fluoride varnish with treatment as usual in nursery school attendees receiving preventive oral health support through the Childsmile oral health improvement programme – the Protecting Teeth@3 Study: a randomised controlled trial. BMC Oral Health. 2015; 15
McMahon AD, Elliott L, Macpherson LM, Sharpe KH, Connelly G, Milligan I Inequalities in the dental health needs and access to dental services among looked after children in Scotland: a population data linkage study. Arch Dis Child. 2018; 103:39-43
Childsmile after 10 years part 2: programme development, implementation and evaluation Lorna MD Macpherson Jennifer Rodgers David I Conway Dental Update 2024 46:3, 707-709.
Authors
Lorna MDMacpherson
Professor of Dental Public Health, School of Medicine, Dentistry and Nursing, University of Glasgow
Childsmile is the national child oral health improvement programme for Scotland. It was developed as pilot studies from 2006/7, building on an established national supervised toothbrushing programme in nursery schools. By 2011, an integrated programme was in place in all NHS Boards across the country. The importance of a multi-agency, common risk factor approach is acknowledged and the programme continues to evolve through learning from the embedded process evaluation. The development and implementation of Childsmile has been associated with major improvements in child oral health. However, clear health inequalities remain and the future focus of the programme will aim to reduce further the social gradient of child oral health in Scotland.
CPD/Clinical Relevance: This paper describes the development, implementation and evaluation of Childsmile, utilizing the theories and approaches outlined in Part 1.
Article
Childsmile aims to improve the oral health of children in Scotland and reduce inequalities both in dental health and access to dental services. Programmes required to make a real impact can be difficult to implement without organizational and system level changes to support new ways of working and alterations in the philosophy of groups and individuals, embracing a multi-agency approach.
The programme follows the principles of supporting the wellbeing of children and young people in Scotland by offering the ‘right help at the right time from the right people’. This approach is known as Getting it Right for Every Child (GIRFEC) and supports young people and their families to work in partnership with the services that can help them.1
In 2001, the first national initiative, which now forms part of the Childsmile programme, commenced. Ad-hoc toothbrushing projects, already operating in some regions of Scotland, were consolidated into a national supervised programme, available to all nursery schools across the country. A more comprehensive approach to child oral health improvement (Childsmile) was developed as pilots from 2006, following the publication of a Scottish Executive Action Plan in 2005.2 The plan included new investment for improving child oral health, and successive government administrations have continued to fund and support the development of the programme.
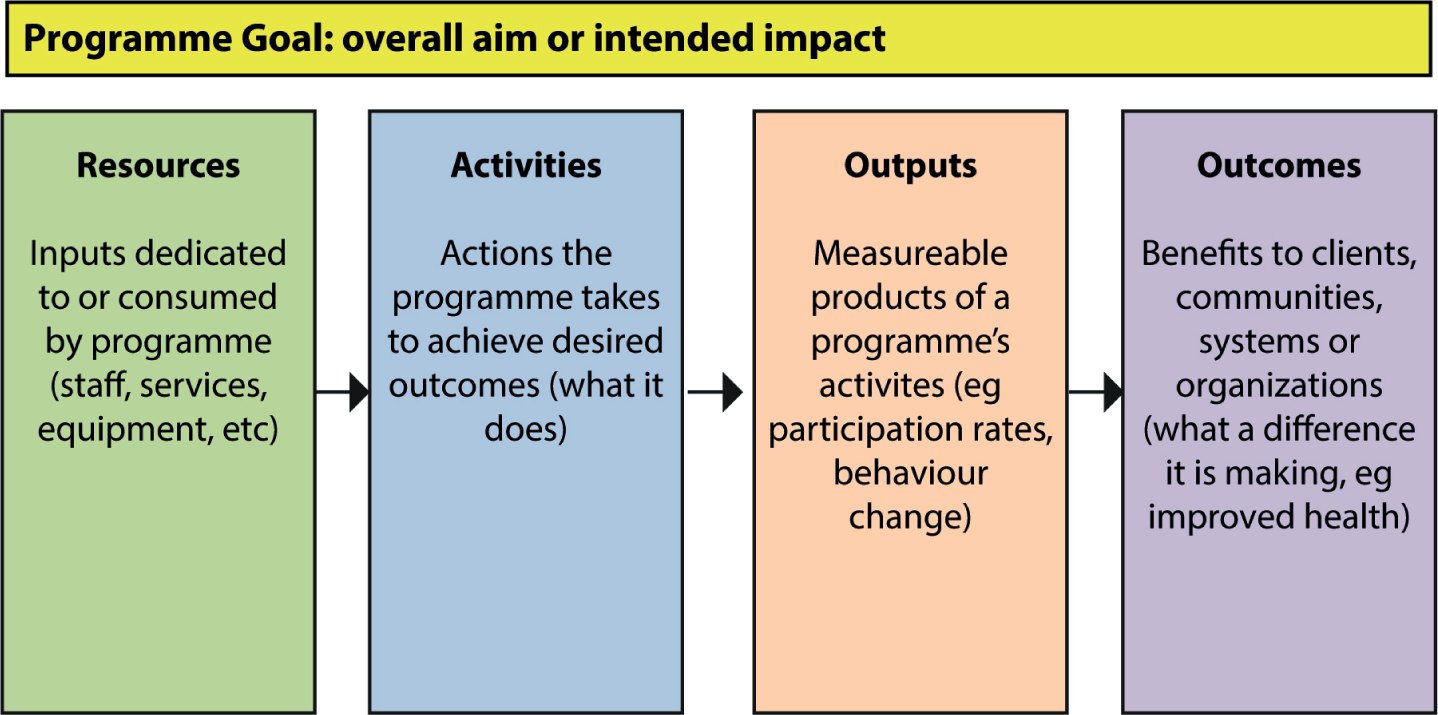
The programme was designed and is evaluated using a theory-based approach. A theory-based approach explicitly, and at the outset, considers the mechanism of change and the context in which the programme is delivered.3 Logic models were developed following multi-stakeholder input. These identified the evidence-based health improvement activities and approaches (outlined in Part 1) which were considered to be associated with long-term improvement in child oral health, health and social outcomes. This was context specific to the Scottish population, taking into account the availability of resources, organizations and structures available for programme implementation. Service- and behaviour-change intermediate outcomes which would be required to achieve the health outcomes were also identified. The design of a typical logic model is shown in Figure 1.
Figure 1. Typical logic model.
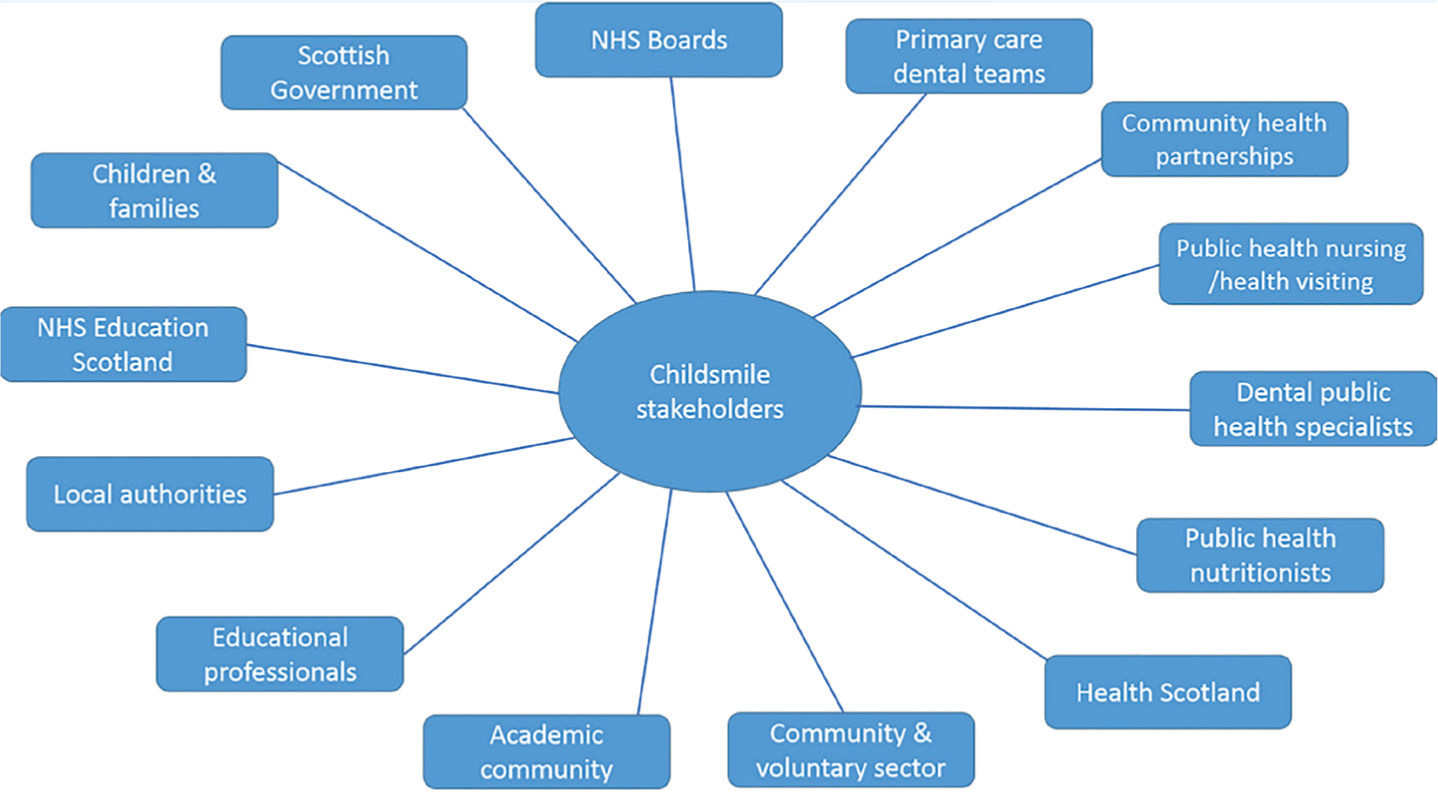
Since 2011, Childsmile has been delivered as an integrated programme in all (n = 14) Health Board areas throughout Scotland. It is a complex public health intervention involving many stakeholders (Figure 2), creating a broad coalition and collaboration with common goals. The programme has developed and delivers oral health improvement interventions both within and outside traditional dental clinical settings – in education establishments, community settings, other healthcare settings (integration to Health Visitor Early Years Pathway), and children's homes.
Figure 2. Childsmile stakeholder map.
Programme outline
The main features of the Childsmile programme, and its position within the upstream/downstream continuum are shown in Table 1. These are also represented in Figure 3.
Upstream
Influencing Public Health Policy at national level:
Contribute to development of healthy food & drink regulations in education settings
Change to national primary dental care contract for children (prevention-orientated)
Midstream
Oral Health Training for wider workforce:
Training to national standards for nursery and school staff
Guidance for Health Visitors
Supervised toothbrushing in nursery and school settings
National standards: universal in nurseries; targeted in schools
Universal and targeted provision of toothbrushes/paste
National contract: distribution via education, health and other community settings
As part of a more upstream approach to health improvement, the programme is involved in advocacy for, and involvement in, development of national strategies, policies and regulations relating to diet and nutrition. This includes membership of a multidisciplinary working group which developed government regulations relating to healthy eating in schools.4 It also supports the common risk factor approach relating to non-communicable diseases and promotes integration of oral health into national strategies and policies relating to sugar control and obesity.5
Other regulatory and policy changes include successfully lobbying the General Dental Council for a change in the scope of practice of dental nurses in the UK. This was to enable appropriately trained dental nurses to apply fluoride varnish as part of community-based public health programmes and in dental practice settings. A change has also been made to the dental primary care payment system in Scotland to promote a more preventive orientated focus in the Scottish General Dental Service6 and national policy has been developed and implemented in relation to supervised toothbrushing and fluoride varnish application (FVA) programmes within child education settings.
At the community level, some components of the programme are available to all children (universal), while others are targeted to more socio-economically deprived areas based on the Scottish Index of Multiple Deprivation (SIMD).7 The SIMD is an area-based index comprising data on multiple sources of deprivation (eg income, education, employment levels) and ranks these small areas (called data zones) of which there are n = 6976. These data zones are grouped into fifths for the purposes of targeting. This approach follows the principles of proportionate universalism, ie the programme is universally available, not only for the most disadvantaged, but is also able to respond to the level of presenting need. The multi-agency programme is implemented in a number of different community settings.
Supervised toothbrushing programme
Every 3- and 4-year-old child attending nursery (whether it is a local authority, voluntary or private nursery) is offered free, supervised toothbrushing. National toothbrushing standards8 have been developed and are closely followed, on a daily basis, by nursery staff. Oral health personnel from the Public Dental Service are available to provide training and support. The products (toothbrush and 1450 ppm F toothpaste) are provided by a nationally procured contract to ensure consistency and cost-savings across Scotland.
Supervised toothbrushing continues for many children into the first two years of primary school (5–6 year-olds), targeted to schools situated in areas with the highest level of deprivation in each Health Board.
To promote home toothbrushing, every child is also provided with a Dental Pack (containing a toothbrush and a tube of 1450 ppm F toothpaste) on at least six occasions by the age of 5, initially by the health visitor and then via nursery. Children also receive a free-flow feeder cup by one year of age.
Fluoride varnish in nursery and school programme
This delivers, via nursery and primary schools, the application of fluoride varnish to the teeth of children aged 3 to at least 8 years who are identified as living in the most deprived areas. It covers a minimum of 20% of children from each Health Board.
Educational establishments are targeted in order of those with the highest proportion of children living in the most deprived local quintile as defined by the Scottish Index of Multiple Deprivation (SIMD).7 Twice-yearly fluoride varnish applications are provided by Childsmile dental nurses. These Extended Duty Dental Nurses (EDDNs) have been trained by NHS Education for Scotland in fluoride varnish application technique. As part of the process, children who require further assessment and possible dental care are identified and their parents receive a letter informing them of their child's dental need.
Community interventions involving Health Visitors and Dental Health Support Workers
Every newborn child in Scotland is linked to Childsmile via the universal child health surveillance system within the Universal Health Visitor Early Years Pathway.9 Health Visitors see all children and their parents/carers on a regular basis between birth and 5 years. Health Visitors provide advice on oral health, distribute a Dental Pack, and encourage dental attendance from a young age. Where they feel additional support may be required to promote oral health, they make a referral to a community-based Dental Health Support Worker (DHSW).
DHSWs are embedded within the more disadvantaged communities and offer peer support to families with young children in the family home. They work closely with health visitors, dental practices, and the Public Dental Service (who co-ordinate and administer the nursery and school components of the programme). They are aware of, and engage with, agencies in their local communities which can help to support family life and parenting skills, eg access to healthy foods, promoting coping skills/self-esteem, and thus facilitate and enable the implementation of positive child oral health promoting behaviours. The DHSWs can also provide support to these groups and assist them to incorporate oral health into their activities and, additionally, can undertake social prescribing to link families into these organizations, as deemed appropriate at an individual level.
DHSWs provide the following:
Tailored support and advice to promote and enable oral health in the family home;
Linking to dental services and facilitating child attendance at a dental practice;
Engaging with and signposting/linking to other community organizations and initiatives via social prescribing (eg food co-operatives, infant feeding programmes, parenting skills classes, debt management advice agencies).
Dental primary care
In 2011, payments were introduced into the NHS primary dental care contract in Scotland for preventive items of care, including fluoride varnish, and advice to support and enable plaque control via toothbrushing with a fluoride-containing toothpaste and promoting healthy eating in the family home.6
This programme of preventive care should be tailored to meet the needs of the individual child, and be delivered by any appropriately trained dental team member. The clinical care includes twice-yearly fluoride varnish applications from two years of age and, as children age, there are opportunities for fissure sealant applications on first permanent molar teeth.
A major aim of the programme is to replace very brief, standardized ‘health education’ messages with meaningful, tailored support for families. Identification of social needs which can best be met by other community groups and organizations should be identified and linking to such organizations and groups promoted, as appropriate.
To facilitate this type of working within dental primary care, undergraduate students at the University of Glasgow are now learning the principles of social prescribing and how to identify and be aware of local community-based services around their paediatric outreach teaching centres, which could support the oral health of the patients they see.
Evaluation
An integrated theory-based evaluation, funded by the Scottish Government, has been an important feature of the programme from its outset. This work is underpinned by the logic model and robust national data monitoring systems (including a bespoke Childsmile IT system designed by the Health Informatics Centre, University of Dundee). The evaluation work is both process- and outcome-orientated in nature.
Process
The in-depth, mixed-methods process evaluation assesses how closely the programme is operating according to how it was envisioned initially, ie whether the anticipated changes in service provision and behaviours, necessary for child oral health improvement, have occurred. This includes, for example: activity levels for fluoride varnish applications in education and dental practice settings; dental registration and attendance rates; toothbrushing activity; DHSW and other community-based early years' activity. Where necessary, research is conducted to investigate the barriers and facilitators for the implementation of component parts of the programme. Identification of these factors can facilitate ongoing refinement to enhance programme delivery still further.
Outcomes
Outcomes from the programme are being investigated mainly via a pioneering big data linkage project. This involves linking multiple routine administrative national health and education datasets to create a birth cohort to evaluate the complex multiple interventions of Childsmile with a range of health and education outcomes. An economic evaluation, investigating the cost-effectiveness of the programme and its components, accompanies this work. Furthermore, an embedded, randomized control trial of the nursery fluoride varnish programme – Protecting Teeth @ 3 trial10 – has recently been completed.
Outcomes
Child oral health improvement
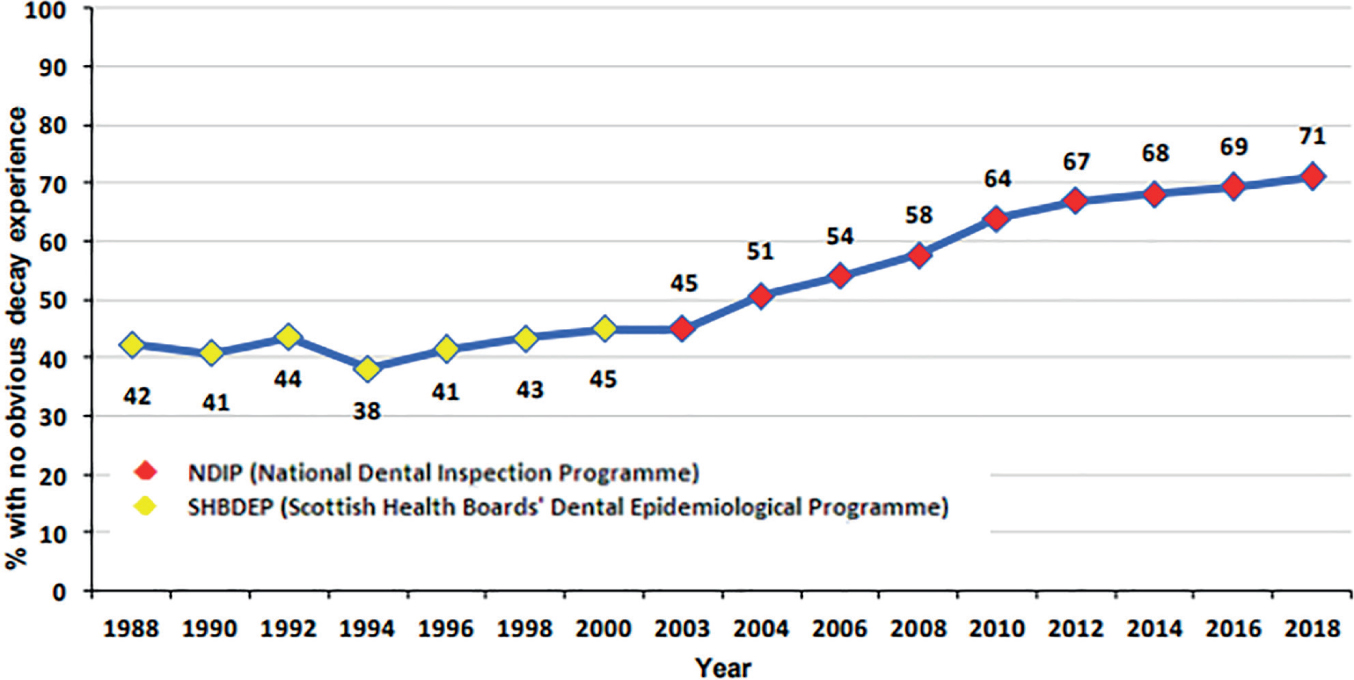
The National Dental Inspection Programme (NDIP) data show substantial improvements in dental health for both 5- and 11-year-olds over time.11,12 More than two-thirds (71%) of 5-year-old children had no obvious decay experience in their primary teeth in 2018 (d3mft = 0) (Figure 4). This is a large improvement in comparison with 45% back in 2003. There has been a parallel continuing decline (improvement) in the mean number of decayed, missing and filled primary teeth from 2.76 in 2003 to 1.14 in 2018. Similar improvements are observed for 11-year-olds, with an improvement from 53% with no obvious caries experience in 2005 to 77% in 2017; and the mean D3MFT decreased from 1.29 in 2005 to 0.49 in 2017.
Figure 4. National Dental Inspection Programme, 2018: Trends in the proportion of primary 1 (five-year-old) children in Scotland with no obvious decay experience (d3mft = 0).11
Nursery toothbrushing
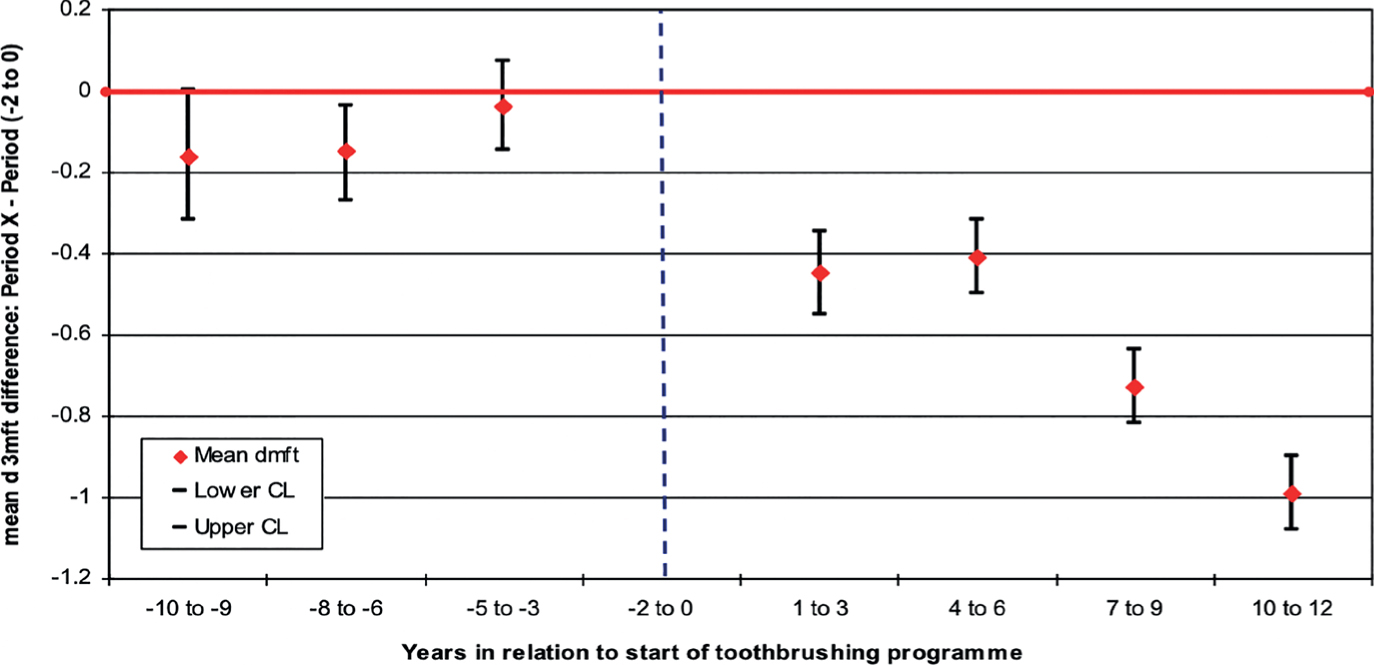
A Scotland-wide population study has shown an association between the roll-out of the Childsmile national nursery toothbrushing programme and a reduction in dental decay in five-year-old children (Figure 5), with the aggregated slope of uptake in toothbrushing across Health Boards being significantly correlated with the slope in the reduction of mean d3mft.13
Figure 5. Mean d3mft for 5-year-olds in Scotland in relation to commencement of nursery toothbrushing. Note: Year 0 is a year before the start of nursery toothbrushing intervention (dotted vertical line). Period (-2 to 0) is a reference period.
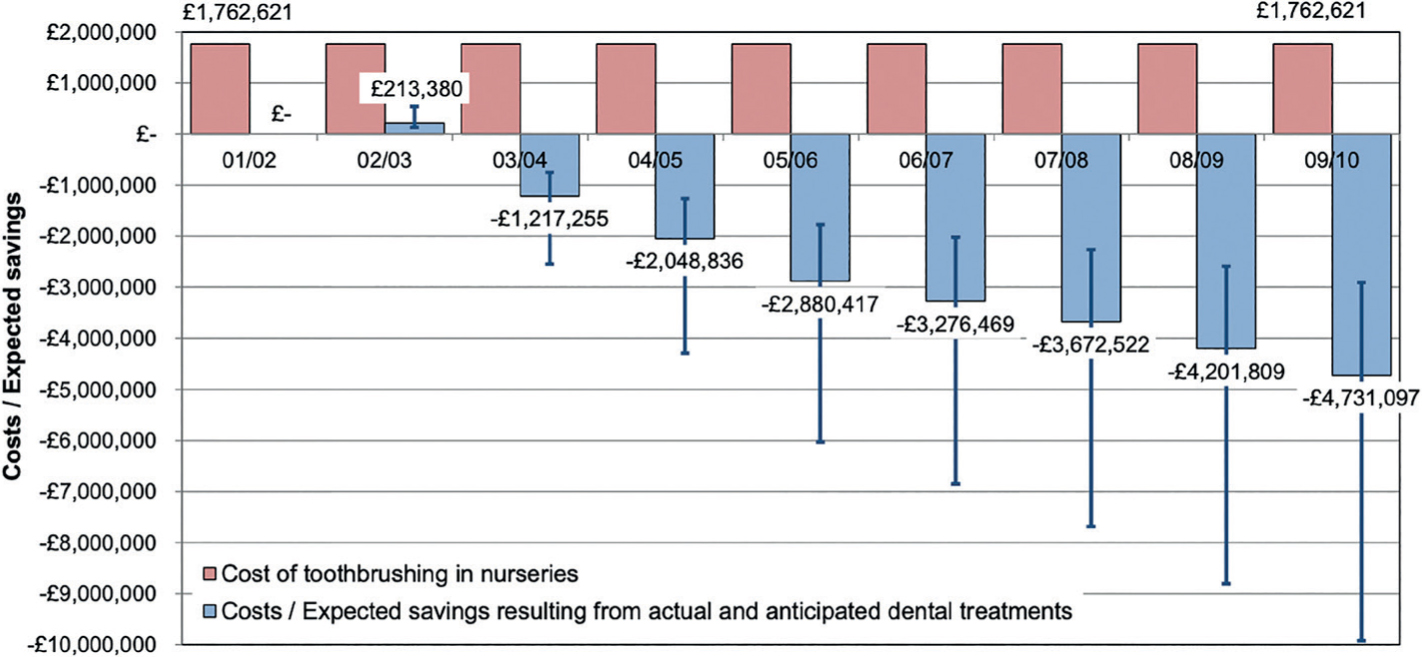
A further study compared the cost of providing the Scotland-wide nursery toothbrushing programme with associated estimated National Health Service (NHS) cost savings from improvements in the dental health of 5-year-old children: through avoided dental extractions, fillings and potential treatments for decay.14
The study (Figure 6) indicated that the estimated cost of the nursery toothbrushing programme in Scotland was around £1.8 million per year. The estimated NHS costs associated with the dental treatments for five-year-old children decreased over time such that eight years into the toothbrushing programme, the expected savings were more than two and a half times the costs of the programme implementation. This is a good example of preventive spend, with funding for this aspect of the programme resulting both in health gain and also in reduced treatment costs for the NHS.
Figure 6. Annual cost of nursery toothbrushing programme and costs/expected savings resulting from actual and anticipated dental treatments in comparison with 2001/02 dental treatment costs. Adapted from Anopa et al 2015.14
Ongoing challenges
Introduction of new approaches always requires a period of transition, with different groups and individuals varying in their rate and level of adoption of new ways of working. The process evaluation helps to identify and address issues related to the perceived relevance, feasibility and interest of stakeholders in this public health programme. Many dental professionals are most comfortable working in the more traditional, clinical, downstream areas of activity and the challenge is to enhance the public health approach further within dental primary care, and to increase multi-agency community-based and upstream activities, both of which are likely to have more reach and impact among those most in need of support. This will include working more closely across primary care, as well as facilitating patient access to local support services that may assist vulnerable families.15 Such services can involve welfare, debt and community food initiatives delivered via both public sector agencies (eg social care) and also the third or voluntary sector (including charity, community groups).
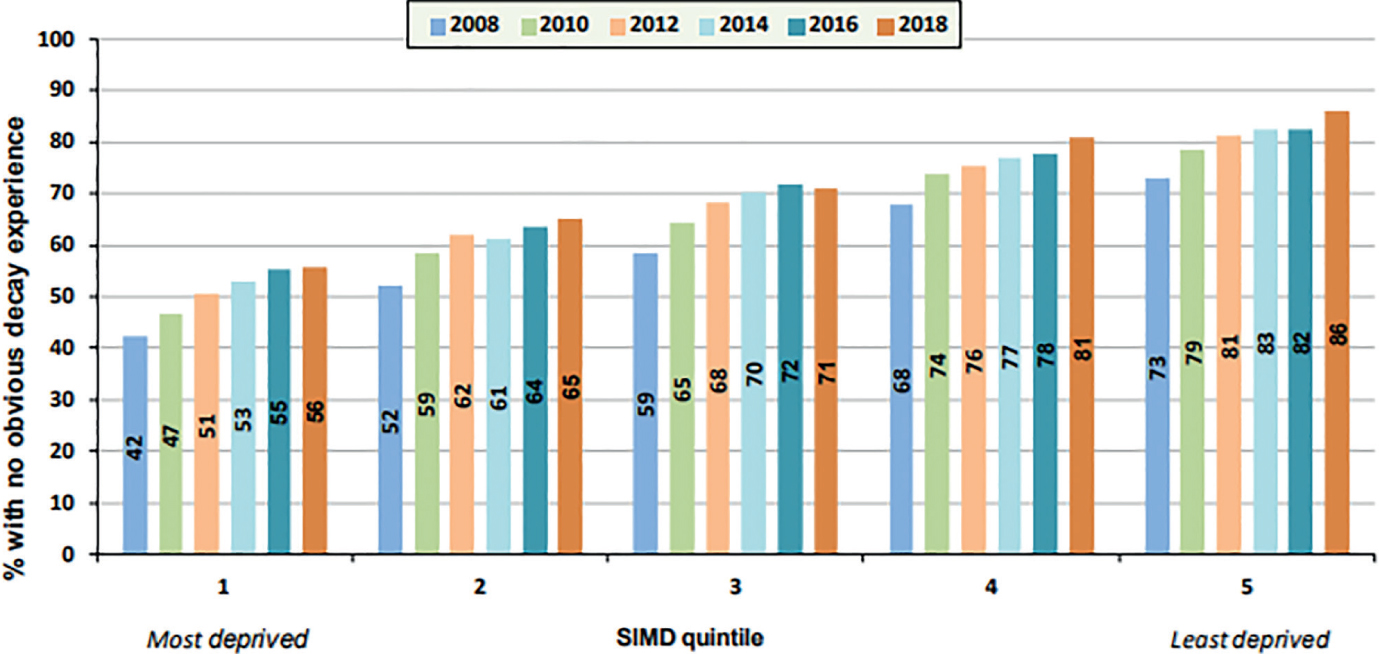
Health inequalities remain a significant challenge. Figure 7 shows data for the proportion of five-year-old children with no obvious decay experience by the Scottish Index of Multiple Deprivation (SIMD) quintiles.11 Quintile SIMD1 is the most deprived and quintile SIMD5 is the least deprived. Despite improvement in all groups, there are clear and persistent inequalities in child dental health over time, indicating that tackling child dental health inequalities should remain the clear focus for the programme.
Figure 7. National Dental Inspection Programme, 2018: Proportion of Primary 1 (five-year-old) children in Scotland with no obvious decay experience by SIMD quintile.11
Conclusions
The Childsmile programme has had significant achievements and been associated with major improvements in child dental health over time. However, socioeconomic inequalities persist, with children from the most deprived backgrounds bearing the greatest disease burden. A new national Oral Health Improvement Plan has recently been published16 and with it will be opportunities for the programme to develop further.
It is envisioned that the future work of the Childsmile programme will include the following:
Optimizing the delivery of the existing programme, through lessons learned from the evaluation;
Expanding community engagement work, including further work with the third (voluntary) sector and social prescribing/linking with ongoing community-based initiatives;
An increased focus on vulnerable groups (eg children looked after by the state17); and
Expanding the upstream work relating to influencing policy and programmes, particularly in relation to sugar control as part of a common risk factor approach and the Non-Communicable Disease (NCD) agenda of the WHO.