Algaithy RA, Qualtrough JE. Pulp sensibility and vitality tests for diagnosing pulpal health in permanent teeth: a critical review. Int Endod J. 2017; 50:135-142
Kqiku L, Sivic E, Weiglein A, Stadtler P. Position of the mental foramen: an anatomical study. Wien Med Wochenschr. 2011; 161:272-273
Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol. 1965; 20:340-349
Siqueira JF, Rocas IN. Microbiology and treatment of acute apical abscesses. Clin Microbiol Rev. 2013; 26:255-273
Levitan ME, Himel VT. Dens evaginatus: literature review, pathophysiology, and comprehensive treatment regimen. J Endod. 2006; 32:1-9
An apical abscess associated with a caries free and unrestored tooth (virgin tooth) is uncommon. This may present diagnostic challenges and risk in general dental practice. The following report illustrates the diagnostic challenges and the initial management of pain in the case described.
CPD/Clinical Relevance: Patients presenting with endodontic pain should be examined carefully, with particular reference to radiographic exposure of suspect teeth. Dentists should come to a presumptive diagnosis only after such careful examination and not make assumptions based on either a tooth of apparent integrity or, alternatively, heavily restored in nature.
Article
This is a case report of a patient presenting in pain of two-weeks' duration localized to the lower right premolar region. Whilst the LR5 was heavily restored, the adjacent unrestored LR4 was tender to percussion. This case report presents the clinical management of diagnosis and treatment of an apical abscess at an apparently sound virgin premolar tooth. The authors discuss how they made a differential diagnosis and the likely reasons for disease arising.
Case report
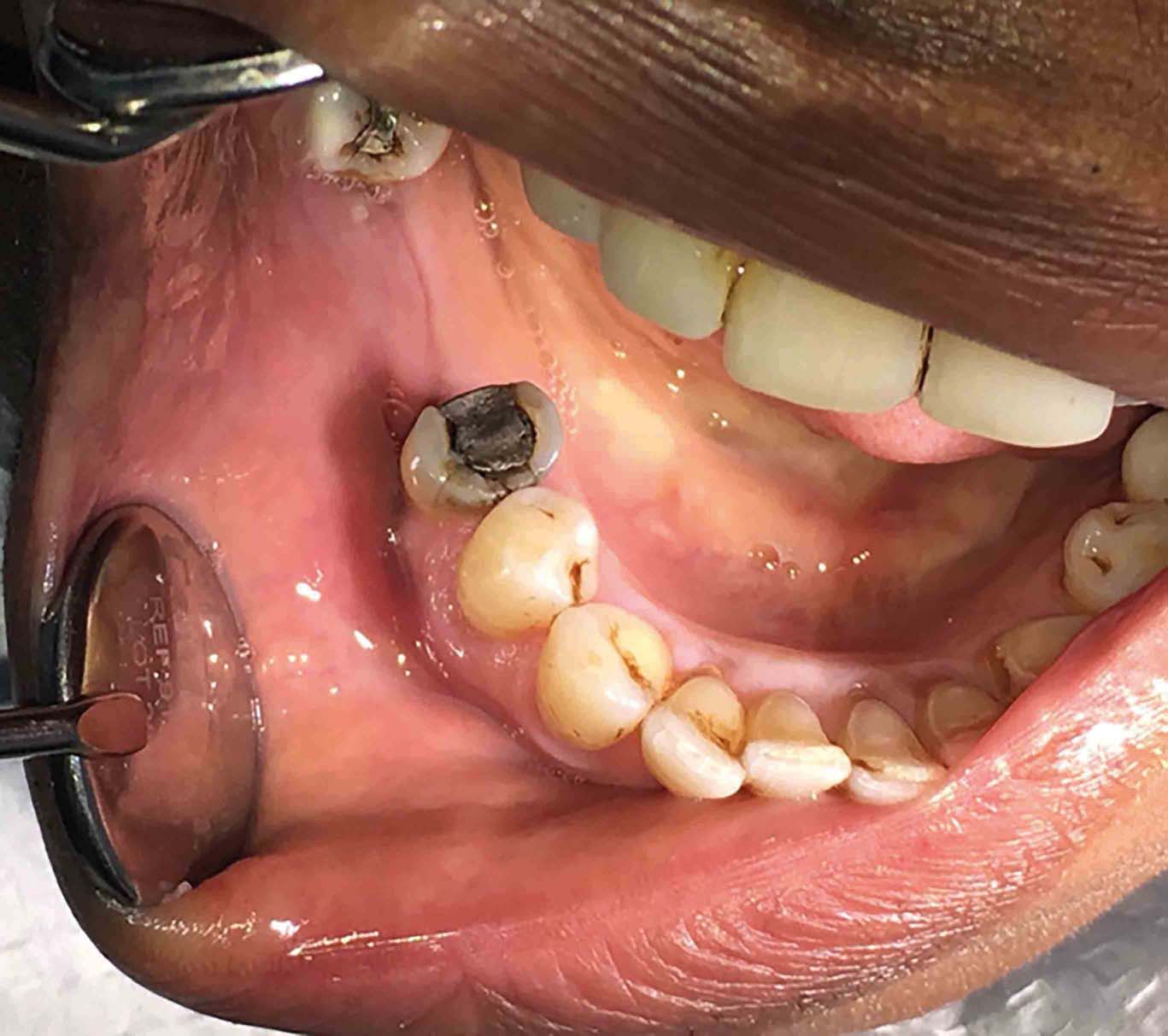
A 67-year-old female patient with type II diabetes presented with a constant dull ache localized to the LR45. The pain radiated through the right-hand side of the mandible, keeping the patient awake at night. There was no associated suppuration or sinus tracts. The LR5 had a large distal occlusal (DO) amalgam and was not tender to percussion. The virgin LR4 was tender to percussion. The patient could not differentiate the pain between the two teeth. The LR4 appeared free from any restoration or dental caries (Figure 1). Clinical examination did not reveal discoloration of either tooth. There was no mobility nor was there any periodontal pocketing greater than 3 mm. Sensibility testing with both ethyl chloride and electric pulp tester of the LR45 showed a positive but not exaggerated response at LR5 and no response at LR4.
Figure 1. Showing a virgin LR4 alongside LR5 with a DO amalgam.
A periapical radiograph was taken which revealed a periapical radiolucency associated with the LR4 (Figure 2). The authors considered that they could not exclude that the periapical radiolucency was a superimposition of mental foramen on the apex of the LR4 and exposed a sectional OPG attempt to clarify the situation (Figure 3). The OPG film confirmed that the position of the right mental foramen and the radiolucency at the apex of LR4 were discrete. A diagnosis was made of pulpal necrosis and acute periapical periodontitis of the LR4. This was explained carefully to the patient and also that the situation was unusual given the unrestored nature of the tooth. The authors expressed the view that there was some diagnostic uncertainty in light of this and the confounding heavily restored nature of the adjacent LR5. Pulpal extirpation of the LR4 was proposed and the risks and benefits of that treatment discussed. The patient consented and careful attention was paid to the pulpal anatomy whilst gaining initial access. Upon deroofing the pulp chamber, pus began to ooze from the canal system, confirming the diagnosis of an apical abscess. Rubber dam was placed, the tooth was cleaned and shaped with hand files and irrigated throughout with sodium hypochlorite. The canal was dried with paper-points and a non-setting calcium hydroxide paste was placed. The tooth was restored coronally with glass ionomer cement. The patient re-attended at two weeks with resolution of symptoms and root canal treatment progressed uneventfully.
Figure 2. Periapical radiograph showing an apical radiolucency associated with the LR4.Figure 3. Right-hand OPT confirming the position of the mental foramen.
Discussion
The presentation of pulpal and apical pathology at an apparently sound tooth is unusual and created diagnostic uncertainty because an adjacent heavily restored lower premolar seemed more likely.
The importance of the sensibility and special tests have been highlighted as this provided important information as to the vitality of the LR45. The LR4 was tender to percussion whereas the LR5 was not. In the authors' experience, such tenderness to percussion is very often diagnostic, although where multiple adjacent teeth are tender this can confuse. The unrestored nature of LR4 confounded this somewhat.
The heavily restored nature of LR5 suggested that this as a more likely candidate for loss of vitality; percussion, radiographic and vitality testing suggested that the LR4 was the cause of the patient's symptoms. If these tests were not carried out on the assumption that the LR5 was the cause, or if the apex of the LR4 had been missing from the periapical radiograph, the treatment which subsequently followed would have been unnecessary and detrimental to the patient. Although laser Doppler tests are referred to as the gold standard for assessing pulp vitality, this is a laboratory tool in the main. Where this is not available to hand, a combination of electric and thermal testing gives valuable diagnostic information.1
The most common place to find the mental foramen is between the first and second mandibular premolar (37.8%). Variations do occur, including the mental foramen being in line with the long axis of the first premolar (1.5%), which could have been the case for this patient, hence the need for further investigation via OPT.2 Where the teeth in question are lower premolar teeth, the proximity of the mental foramen should be borne in mind and the possibility that this may mimic or mask apical pathology. In this case, the mental foramen and apical pathology were discrete. Had these been coincident, this would have been a particularly challenging diagnosis to make.
For an acute apical abscess to form, the root canal system needs to be infected.3 The aetiology of this apical abscess associated with a virgin tooth was uncertain.
There was no caries at the tooth nor history of caries (a restored tooth). Bacterial aetiology is most often the cause of loss of vitality at lower premolar teeth, in the authors' experience. There was no history of trauma to the dentition; this could be a potential reason for the formation of a periapical abscess, although this is unusual at lower premolars.4 A high pulp horn or dens evaginatus is a recognized phenomenon at lower premolar teeth.5 This could have meant an undetected pin-point exposure previously. This would allow the bacteria to enter the root canal system and thus allow for abscess formation. Such an exposure might be occult to clinical examination and diagnosis would be radiographic and after exclusion of other causes. The pulpal anatomy of the premolar in question, however, appeared relatively normal.
Any micro fractures present that were unable to be seen, or the presence of accessory canals, could provide the necessary cover required for bacteria to enter the root canal system. Micro-organisms from the gingival sulcus are able to pass through these canals via the periodontal membrane and/or following periodontal debridement in some instances.6 This tooth, however, had good bony support and the authors considered this unlikely.
Following trauma to the tooth, transient bacteria from the bloodstream could be attracted to a pulp in a process called anachoresis. During this process there is no exposure of the pulpal system, however, a marked inflammatory process is present.6 This is a pathological mechanism of theoretical interest in the authors' view and the more common causes of pulpal necrosis should be excluded in the first instance.
Ultimately, the cause of pulpal necrosis here was unknown.
Conclusion
An apical abscess associated with a virgin premolar tooth is an unusual occurrence. The presentation here should raise awareness for dental practitioners that visually sound teeth may, on occasion, present with endodontic pathology. Where there is an adjacent heavily restored tooth, this can create diagnostic uncertainty; such teeth are more commonly the source of endodontic problems. Careful clinical and radiographic examination with judicious use of sensibility testing should resolve most uncertainty and, on this occasion, meant a successful outcome. As always, clinical judgement is paramount on occasions where conflicting diagnostic evidence is present.