
References
Bilateral dentigerous cysts: an updated literature review and report of a case with associated root resorption
From Volume 45, Issue 11, December 2018 | Pages 1063-1082
Article

A dentigerous cyst is an epithelial-lined cavity which surrounds the crown of an unerupted tooth at the cemento-enamel junction.1, 2 It is considered benign and is developmental in nature.3 Dentigerous cysts are the second most common odontogenic cysts following radicular cysts,4 with evidence suggesting that they account for 25% of all odontogenic cysts.5
Dentigerous cysts develop due to the accumulation of fluid between the reduced enamel epithelium and enamel of an unerupted tooth or within the enamel organ.6 The erupting tooth exerts pressure on the impacted follicle which obstructs venous outflow. This results in a serum transudate across the capillary wall causing elevated hydrostatic pressure and therefore pooling of fluid. This causes separation of the follicle from the crown, leading to formation of the cyst.6, 7 Given this mechanism, dentigerous cysts generally materialize during tooth development in young patients, with peak incidence in the second to fourth decades of life.3 The teeth most frequently associated with such cysts are mandibular third molars, followed by maxillary canines.4
The dentigerous cyst most commonly presents as a solitary lesion.2 Multiple dentigerous cysts with bilateral presentation have been associated with several conditions which involve unerupted teeth, such as mucopolysaccharidosis type VI (Maroteaux Lamy syndrome) and cleidocranial dysplasia.2, 8, 9, 10 The current literature asserts that bilateral presentation in a non-syndromic patient is extremely rare, with a review by Kaushik et al citing only 43 published cases of non-syndromic bilateral dentigerous cysts worldwide up to the year 2013.11
Radiographically, dentigerous cysts appear as a unilocular radiolucency with a well-defined, sclerotic margin which is attached to the cervical area of an unerupted tooth and encompasses the crown.4 Whilst histological features of dentigerous cyst have been shown in radiographically normal follicles,12 the view is held that, on radiographic examination, a follicular space of approximately 3−4 mm is considered normal, however, if this is enlarged and greater than 5 mm then a cystic lesion is assumed to be likely.2
The diagnosis of a dentigerous cyst often stems from an incidental finding within primary care, as the majority of patients are asymptomatic.3 However, they may become symptomatic if infected. Treatment of neighbouring teeth may also be affected, as these cysts have also been associated with displacement or resorption of teeth in close proximity. Therefore, the general practitioner may wish to delay any major restorative treatment until the cyst has been treated. Root resorption is often mild; however, severe root resorption of adjacent teeth has been reported.13, 14 Less frequent complications may include displacement and obliteration of the maxillary antrum and nasal cavities, paraesthesia of the inferior alveolar nerve, or metaplastic and dysplastic changes.15
As there is potential for the cyst to increase in size, and for the aforementioned complications, surgical removal of the lesion and involved teeth is often indicated. Alternatively, decompression of the cyst may be considered in order to attempt to salvage the involved teeth or adjacent delicate structures. Hence, it is prudent that a referral be made for specialist care.
The purpose of this study is to remind practitioners of the presentation, radiographic investigations and surgical management of bilateral dentigerous cysts, and to assess the frequency of associated adjacent tooth resorption, which may impact on treatment plans. This article will also add to the current literature by describing the management of a 42-year-old male with no known syndromes, who presented with bilateral dentigerous cysts.
Materials and methods
A literature search was performed to review all published case reports of bilateral dentigerous cysts. The databases Ovid EMBASE, Ovid MEDLINE, PubMed, Cochrane and search engine Google Scholar were searched using a combination of controlled vocabulary and free-text terms (see Table 1 for search strategy). In order for a study to be included, the following criteria were applied:
| Ovid EMBASE 1974–2016 Sept 09 | Ovid MEDLINE 1946–2016 Sept 09 | PubMed 2016 Sept 09 | Cochrane Sept 2016 | Google Scholar |
|---|---|---|---|---|
| ((Dentig*) OR follicular*) AND cyst*) AND (jaw* OR mandib* OR maxilla*)) NOT ovar* |
Dentig* |
Dentigerous follicular |
||
| 490 articles |
483 articles |
965 articles |
2 articles |
875 articles |
Note:
= truncation of associated word.
The titles and abstracts of the articles retrieved from the search strategy were reviewed by two authors (APM and ZY). The full text articles were reviewed for those that reported bilateral dentigerous cysts in the title or abstract. In addition, the reference lists of all relevant articles were manually searched to identify any further reported cases. Full text articles were retrieved for any titles or abstracts that were unclear. The included full text articles were then assessed to record the presenting symptoms, the imaging modality used during investigation, the treatment performed, and to identify cases that had associated root resorption. Any queries were resolved by discussion and agreement between both authors (APM and ZY).
Results
Outcome of the literature search
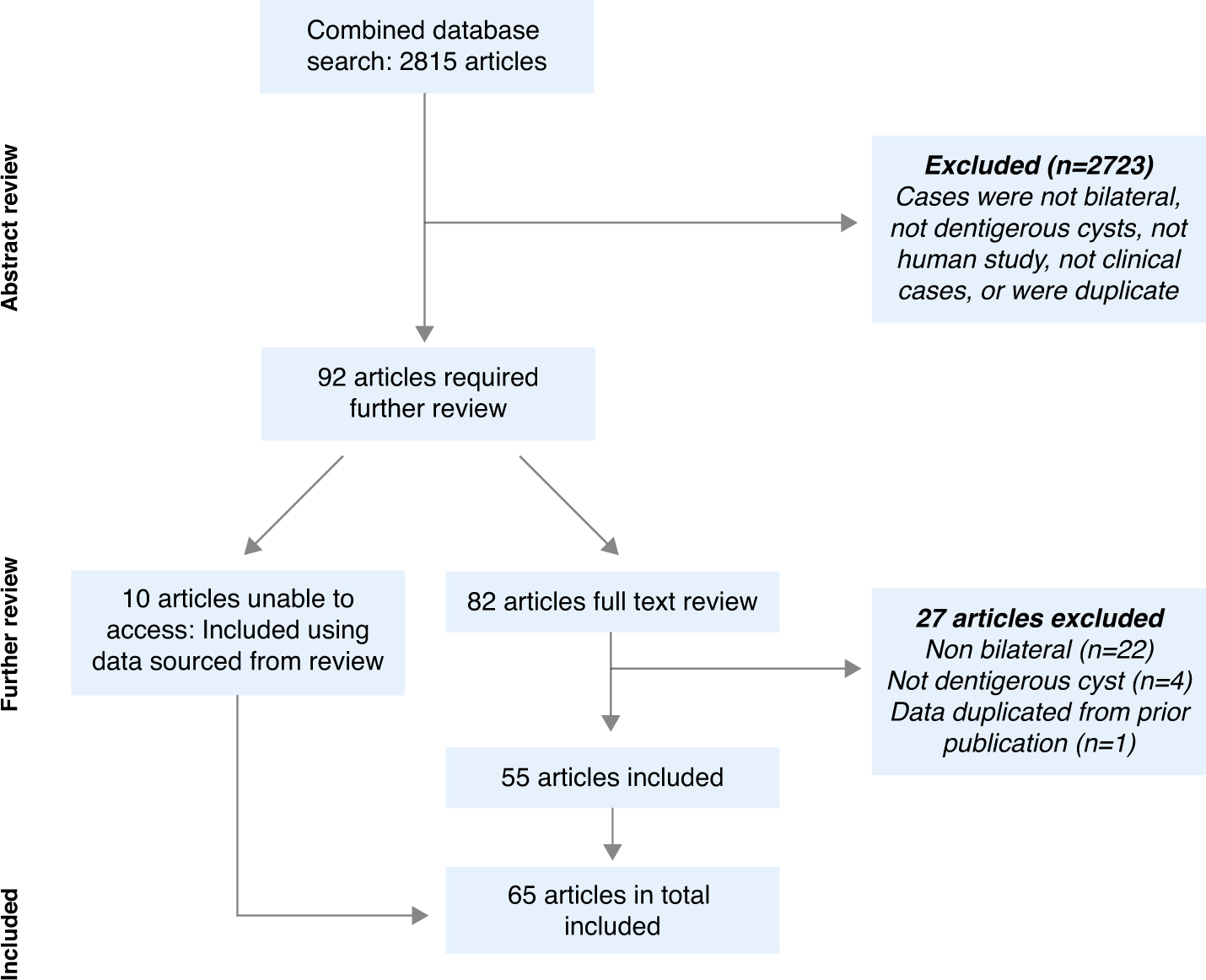
The literature search resulted in 2815 journal articles being identified (Table 1). Abstracts of these articles were reviewed and those that did not meet the inclusion criteria were removed, as well as duplicates. Further searching of reference lists resulted in a total of 92 articles requiring further review; 82 articles were accessed for full text review; 27 were subsequently excluded resulting in 55 articles. For 10 articles, the full text was not accessible and case data were taken from references Freitas et al4 and Cura et al,27 as indicated in the appendix. Therefore, in total, 65 articles met the inclusion criteria and described a total of 77 cases. A flowchart of the review is illustrated in Figure 1 and a summary of the included articles can be found in the appendix.
Demographic details of patients and site of the cysts were included when the information was available in the articles. The average age was 20.4 years, and included 31 females and 43 male patients, with three not specifying gender. Out of the 55 cases that described the presenting symptoms, 16 patients (29%) were asymptomatic, 32 (58%) presented with swelling and 12 (22%) presented with pain (Table 2). The radiographic investigations used to aid diagnosis in the 77 cases reviewed are illustrated in Table 3. Plain film radiography was the most common investigation, with the use of panoramic radiographs reported in 65% of cases. Conventional CT imaging was used in 21% of cases, with three more recently published cases reporting the use of CBCT (4%).
| Presenting symptom | Number of cases (%) |
|---|---|
| Swelling | 32 (58%) |
| Asymptomatic | 16 (29%) |
| Pain | 12 (22%) |
| Intra-oral discharge | 4 (7%) |
| Maligned teeth | 1 (2%) |
| Retained deciduous teeth | 1 (2%) |
| Sensitivity | 1 (2%) |
| Spacing | 1 (2%) |
| Trismus | 1 (2%) |
| Not reported | 22 (40%) |
| Radiograph | Number (%) |
|---|---|
| Panoramic | 50 (65%) |
| CT | 16 (21%) |
| Periapical | 13 (17%) |
| Occlusal | 10 (13%) |
| CBCT | 3 (4%) |
| MRI | 1 (1%) |
| Lateral Oblique | 5 (6%) |
| Occipitomental (Waters view) | 2 (3%) |
| Cephalogram | 1 (1%) |
In the literature, the main complication seen was resorption of adjacent teeth, which was reported in 12 cases (16%), with six of these cases (8%) describing resorption of the permanent dentition. Further complications included four cases (5%) of obliteration of the maxillary sinuses, three cases of displacement of adjacent roots (4%), three cases of displacement of adjacent developing teeth (4%), and one case (1%) of transient paraesthesia of the mental nerve.
The management of the reviewed cases of bilateral dentigerous cysts is outlined in Table 4. The majority of cases were treated with enucleation alone (73%), however, 17% of cases were managed with marsupialisation, and a further six cases were treated by a combination of these surgical techniques. The choice of marsupialisation appeared to depend on the size and extent of the cyst, the proximity to vital structures, the risk of pathological fracture, and the desire to avoid damage to the developing permanent teeth.
| Treatment | Number (%) |
|---|---|
| Enucleation | 56 (73%) |
| Marsupialisation | 13 (17%) |
| One cyst marsupialised contralateral cyst enucleated | 3 (4%) |
| Staged: marsupialisation then enucleation at later date | 3 (4%) |
| No treatment – spontaneous regression | 2 (3%) |
Case report
A healthy 42-year-old male presented to the Oral Surgery department of Birmingham Dental Hospital following referral from his dentist. His main complaint was of an episode of discharge in his oral cavity two months prior. In addition, he reported a one-week episode of left-sided facial swelling occurring one month previously. The patient denied any altered sensation of the inferior alveolar nerve region bilaterally, or any other symptoms. On examination there was no swelling, alveolar expansion or discharge noted.
A panoramic radiograph revealed horizontally impacted and unerupted lower right (LR) and lower left (LL), both of which had radiolucencies associated with their crowns (Figure 2). On the right side this had caused resorption of the LR7 roots, whereas on the left, the distal root of the LL6 was affected along with both the roots of the LL7.

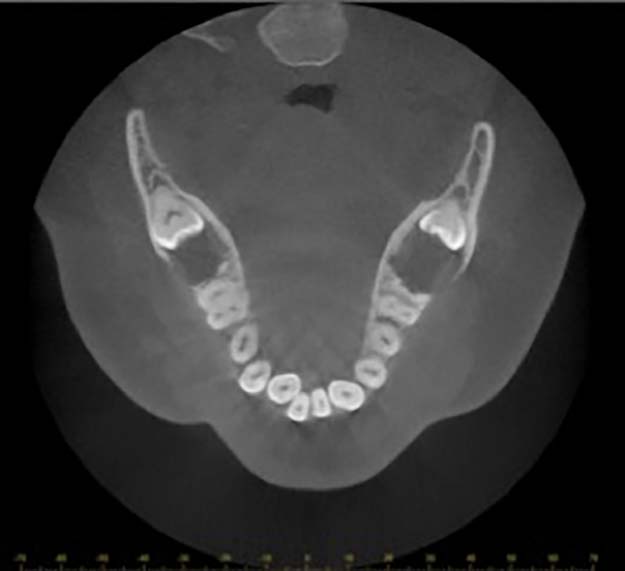
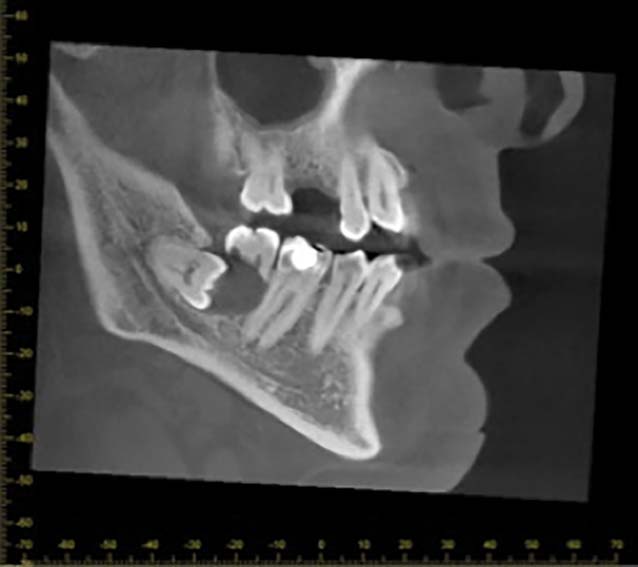
Cone beam computed tomography (CBCT) supported these findings and suggested that the radiolucency on the right side had caused expansion of both the buccal and lingual plates, with apparent perforation of the plate seen buccal to the LR7. The radiolucency on the left side had also caused some buccal and lingual bony expansion. In both cases, the inferior alveolar nerve was not intimately involved with the third molar or the radiolucency (Figure 3). The appearance on CBCT was indicative of a solid lesion, such as an ameloblastoma, and therefore biopsy was indicated.
The surgical procedure was performed under local anaesthetic and consisted of raising a mucoperiosteal flap on the right side, over the region seen as radiolucency on the radiograph. Clinically, a perforation of the buccal cortex was seen and a purulent discharge was noted. The LR7 was extracted and a sample of the lining of the cavity was obtained. Both were sent for histopathological analysis. The results of the biopsy revealed no evidence of malignancy or ameloblastoma, with appearances in keeping with an inflamed dentigerous cyst.
Following discussion of the results with the patient, he elected to undergo surgical removal of the LR8 and enucleation of the associated cyst, followed by surgical removal of the LL678 with enucleation of the associated cyst. This was performed over two visits, uneventfully.
The histological findings following enucleation of both lesions supported a diagnosis of bilateral inflamed dentigerous cysts.
At clinical review 3 months postoperatively the patient demonstrated good soft tissue healing, with no further symptoms and no paraesthesia. Radiographic review at 12 months, and again at 24 months post-surgery showed evidence of bony infill at the sites of extraction and enucleation, suggesting good healing (Figures 4 and 5).


Discussion
Dentigerous cysts are the second most frequently occurring cyst of the jaw, accounting for approximately 25% of odontogenic cysts.5 Whilst rare, the literature search found 65 articles which described 77 reported cases of bilateral dentigerous cysts in non-syndromic patients.
This type of cyst is most frequently associated with mandibular third molar teeth and is more prevalent in males than females, as supported by this search which revealed 58% of cases occurring in male patients.71, 72, 73
Dentigerous cysts are often an incidental finding (demonstrated by the 29% of cases which were described as asymptomatic upon presentation) following radiographic examination. However, of those symptoms that did occur, swelling (58%) and pain (22%) were the most commonly reported.
The first-line imaging modality seen in the literature to diagnose dentigerous cysts is plain film radiography, with a panoramic radiograph being the investigation of choice for multiple cysts. This is a simple and widely available investigation which can be accessed by dental practices, the results of which can guide the justification of further imaging. Computed Tomography has also been used to analyse extensive cystic lesions, providing the detail required to differentiate between cystic, solid or fibro-osseous lesions, as well as accurate information on the size, likely origin, content, bony margins and anatomical relationships to other structures, such as the maxillary sinuses or inferior dental canal.56 In the current case report a panoramic radiograph was the initial investigation performed, and was followed by a CBCT. This is supported by more recent literature which has illustrated the emerging role of CBCT in evaluating cystic lesions of the jaw, that may allow decreased radiation exposure and cost when compared to conventional CT imaging.14, 27, 39
Within the literature and the case report discussed, resorption of adjacent roots is an important complication that may occur with dentigerous cysts, which could ultimately result in loss of the affected teeth. It is therefore important that practitioners refer in a timely manner so that diagnosis and treatment may begin promptly. Although the literature review has identified that root resorption of the adjacent permanent teeth is a rare feature (8% of cases), the result will be of particular consequence to patients, their function and the treatment options available to the general practitioner. Further complications described in the literature included displacement of adjacent roots or developing tooth germs, obliteration of the maxillary sinuses and damage to the inferior alveolar nerve.
Where underlying medical syndromes exist the prevalence of such cysts are increased and clinicians should be aware of such conditions, which may render a patient at higher risk of undergoing cystic change. However, in the absence of underlying syndromes the mean age of presentation was 20.4 years, although 64% of cases were under the age of 18. There was a broad variance in age of presentation, with the oldest patient being 81 years of age and the youngest just three years old.
Where multiple dentigerous cysts were reported, 76% of cases consisted of patients with two dentigerous cysts. In the remaining 24% of cases, the number of cysts identified were n = 3 (7%), n = 4 (10%), n = 5 (3%) and n = >5 (4%).
When adequately treated dentigerous cysts do not recur,3 although with inadequate treatment they may persist. Of note there have been reported cases in which the cysts have transformed into more aggressive lesions. Hence, when assessing patients on their routine check-ups, it is important to remain vigilant in the assessment of the treated cystic regions. A third of ameloblastomas are thought to be derived from cystic lining and, although extremely rare, there have been reported incidents of mucoepidermoid and squamous cell carcinomas which have been shown to arise from the lining of dentigerous cysts.74 Enucleation of the cystic lining is therefore often the preferred surgical treatment modality for dentigerous cysts, as demonstrated in the current case report and in 73% of cases reviewed. However, if the cyst is extensive and encroaches upon vital anatomical structures, or there is risk of pathological fracture, then marsupialisation may be considered. This will also act to preserve the developing permanent teeth. In these cases, close review of the patient post-operatively will be required, with consideration of a staged approach; initial marsupialisation followed by enucleation at a later date.
Conclusion
This review of the literature and case report aims to outline the key features of dentigerous cysts, as well as highlight the rarer associated features. Given the potential severity of the signs, symptoms and sequelae from this limited number of reported cases, the importance of effective diagnosis, referral and management with appropriate follow-up of such cases is discussed.
There are limited cases of bilateral dentigerous cysts in non-syndromic patients reported within the literature. Though often asymptomatic, these lesions can present with pain and swelling and may also be associated with more serious features, including root resorption of the adjacent teeth. Although such features may be more associated with aggressive lesions, such as an ameloblastoma, the review has shown that the dentigerous cyst should also be considered in the differential diagnosis.
In light of evidence suggesting the potential transformation of dentigerous cysts into more sinister lesions, it is likely that specialist intervention will consist of surgical enucleation as the definitive treatment option. The size of the cyst and proximity to associated anatomical structures will determine if a period of marsupialisation, to allow for decompression, is required prior to enucleation. It is essential that histopathological analysis is undertaken to allow definitive diagnosis.