Fisher SE, Lai CSL, Monaco AP. Deciphering the genetic basis of speech and language disorders. Annu Rev Neurosci. 2003; 26:57-80
Cambridge: Cambridge University Press; 1999
Mitchell PR, Kent RD. Phonetic variation in multisyllable babbling. J Child Lang. 1990; 17:247-265
Fenson L, Dale PS, Reznick JS Variability in early communicative development. Monogr Soc Res Child Dev. 1994; 59:1-185
Hoff E, Laursen B, Tardif T. Socioeconomic status and parenting, 2nd edn. In: Bornstein MH (ed). Mahwah, New Jersey and London: Lawrence Erlbaum Associates, Publishers; 2002
Hoff E. The specificity of environmental influence: socioeconomic status affects early vocabulary development via maternal speech. Child Dev. 2003; 74:1368-1378
Law J, Boyle J, Harris F. Screening for speech and language delay: systematic review of the literature. Health Technol Assess. 1998; 2:1-184
Kerosuo H, Hausen H, Laine T The influence of incisal malocclusion on the social attractiveness of young adults in Finland. Eur J Orthod. 1995; 17:505-512
Overby M, Carrell T, Bernthal J. Teachers' perceptions of students with speech sound disorders: a quantitative and qualitative analysis. Lang Speech Hear Serv Sch. 2007; 38:327-341
Nuttall NM, Steele JG, Evans D, Chadwick B, Morris AJ, Hill K. The reported impact of oral condition on children in the United Kingdom. Br Dent J. 2006; 200:551-556
Gherunpong S, Tsakos G, Sheiham A. The prevalence and severity of oral impacts on daily performances in Thai primary school children. Health Qual Life Outcomes. 2004; 2
Dhiman R, Singh P, Roy Chowdhury SK, Singla NK. Complete mouth rehabilitation of sub total congenital anodontia with indigenous implant supported prosthesis. J Indian Prosthodont Soc. 2006; 6:90-94
Snow K. Articulation proficiency in relation to certain dental abnormalities. J Speech Hear Dis. 1961; 26:209-212
Bankson NW, Byrne MC. The relationship between missing teeth and selected consonant sounds. J Speech Hear Dis. 1962; 27:341-348
Riekman GA, el Badrawy HE. Effect of premature loss of primary maxillary incisors on speech. Pediatr Dent. 1985; 7:119-122
Lamberghini F, Kaste LM, Fadavi S, Koerber A, Punwani IC, Smith EB. An association of premature loss of primary maxillary incisors with speech production of bilingual children. Pediatr Dent. 2012; 34:307-311
Gable TO, Kummer AW, Lee L, Creaghead NA, Moore LJ. Premature loss of the maxillary primary incisors: effect on speech production. J Dent Child. 1995; 62:173-179
Turgut MD, Genc GA, Basar F, Tekcicek MU. The effect of early loss of anterior primary tooth on speech production in preschool children. Turk J Med Sci. 2012; 42:867-875
Holan G, Needleman HL. Premature loss of primary anterior teeth due to trauma – potential short and long term sequel. Dent Traumatol. 2014; 30:100-106
Mattuella LG, Frasca LCF, Bernardi l, Moi GP, Fossati ACM, De Araújo FB. Tooth supported prosthetic rehabilitation in a 5-year-old child with early childhood caries. J Clin Pediatr Dent. 2007; 31:171-174
Bolan M, Cardoso M, Galato G, Vieira RS, Andriani W. Overdenture for total rehabilitation in a child with early childhood caries. Pediatr Dent. 2012; 34:148-149
Klockars T. Familial ankyloglossia (tongue-tie). Int J Pediatr Otorhinolaryngol. 2007; 71:1321-1324
Klockars T, Pitkäranta A. Pediatric tongue-tie division: indications, techniques and patient satisfaction. Int J Pediatr Otorhinolaryngol. 2009; 73:1399-1401
Suter VG, Bornstein MM. Ankyloglossia: facts and myths in diagnosis and treatment. J Periodontol. 2009; 80:1204-1219
Webb A, Hao W, Hong P. The effect of tongue-tie division on breastfeeding and speech articulation: a systematic review. Int J Pediatr Otorhinolaryngol. 2013; 77:635-646
Jocelyn LJ, Penko MA, Rode HL. Cognition, communication, and hearing in young children with cleft lip and palate and in control children: a longitudinal study. Pediatrics. 1996; 97:529-534
Laine T. Associations between articulatory disorders in speech and occlusal anomalies. Europ J Orthod. 1987; 9:144-150
Leavy KM, Cisneros GJ, LeBlanc EM. Malocclusion and its relationship to speech sound production: redefining the effect of malocclusal traits on sound production. Am J Orthod Dentofacial Orthop. 2016; 150:116-123
Caniklioglu C, Oztürk Y. Patient discomfort: a comparison between lingual and labial fixed appliances. Angle Orthod. 2005; 75:86-91
Verrastro AP, Stefani FM, Rodrigues CR, Wanderley MT. Occlusal and orofacial myofunctional evaluation in children with primary dentition, anterior open bite and pacifier sucking habit. Int J Orofacial Myology. 2006; 32:7-21
Warren JJ, Bishara SE, Steinbock KL, Yonezu T, Nowak AJ. Effects of oral habits' duration on dental characteristics in the primary dentition. J Am Dent Assoc. 2001; 132:1685-1693
Patient Information Leaflet. Dummy and Thumb Sucking Habits. 2013;
Barbosa C, Vasquez S, Parada M The relationship of bottle feeding and other sucking behaviors with speech disorder in Patagonian preschoolers. BMC Pediatrics. 2009; 9
Broad FE. Further studies on the effects of infant feeding on speech quality. NZ Med J. 1975; 82:373-376
This article outlines how sounds are produced and how speech and language develop, in the child. The assessment of speech by a speech and language therapist is briefly described. It then discusses the evidence for an impact of occlusion, and the loss or absence of teeth on speech. In summary, there is a possibility that the loss, absence or malalignment of teeth may affect speech, but unfortunately the evidence base is weak.
CPD/Clinical Relevance: Dental care professionals should understand the development of speech and how dental health potentially affects speech.
Article
Language is the human ability to learn and use complex methods of communication. It allows humans to structure thinking and reasoning, and contributes to human identity. Communication exists in many forms, for example: written, heard, read, gestural and non-verbal. Speech (spoken language) is one way to express language and can be described as a mechanism of conveying thoughts into words by producing sounds. This article will focus on the relationship between verbal communication and dentistry.
Speech production
The aetiology of speech disorders is complex and multifactorial, however, it is well documented that the development of speech and speech disorders have a genetic component. Four chromosomal regions on chromosomes 2, 13, 16 and 19 have been identified as being potentially involved in common forms of speech impairment. One of the first genes implicated in speech and language disorders was FOXP2, which regulates several other genes that have also been implicated in these disorders. This gene is found on chromosome 7 and has been definitely linked to language production, but only in relation to an extremely rare speech and language disorder (monogenetic inheritance). It does not appear to be involved in the more common forms of language impairment and further research is needed into the complex genetic basis of speech disorders.1
Acquiring and producing spoken language involves a complex combination of neurological pathways that control the tongue, lips and other vocal apparatus. Specific areas of the brain, notably Broca's and Wernicke's areas, are important for linguistic perception, the decoding of speech sounds, and the mechanical production of speech. Spoken language relies on the physical ability to produce sound waves that travel through air and are capable of vibrating the eardrum. The organs (speech apparatus) that produce these sounds by manipulating the airstream are the lungs, larynx, and the upper vocal tract (throat, mouth, palate and nose).
Speech sounds are categorized into vowels and consonants, which differ due to the presence or absence of contact or friction in the upper vocal tract. They vary in quality depending on the degree of lip opening, the position of the soft palate and the placement of the tongue within the oral cavity. Vowels are those sounds produced with vibration of the vocal cords with shaping of the airstream, whereas consonants are produced by impedance of the air stream. Some speech sounds involve release of airflow through the nasal cavity (nasals or nasalized sounds). Other sounds are defined by the way the tongue moves within the mouth (eg rhotics, or ‘r’ sounds), which are characterized by how the tongue is positioned relative to the airstream.2
As the oral cavity includes the speech apparatus, there are many links between dentistry and the learning and production of speech. For example, there are certain speech sounds that directly involve teeth, and hence any changes to these teeth can lead to changes in speech. These include: ‘f’ and ‘v’ sounds, known as labiodental speech sounds, which are articulated with the upper front teeth touching the lower lip; ‘n’ (nasal alveolar plosive) and ’t’, ‘d’ and ‘l’ sounds (oral alveolar plosive), which are articulated with the tongue resting behind the upper anterior teeth; ‘s’ and ‘z’ sounds (oral alveolar fricative), which are created by a narrow opening between the incisal edges of anterior teeth; and ‘th’ sounds (interdental) which are formed with the tip of the tongue against the teeth.
Theories of speech and language development
There are many theories as to how language develops. The Environmental/Empiricist theory is based around the belief that children learn language by imitation and linguistic input from the environment around them. In contrast, the Nativist theory is centred on a belief that a large amount of what the child needs to be able to learn language is an innate faculty and that we are born with a set of rules about language. Other theories include Piaget's theory of cognitive development, which considers language development to be a function of cognitive development.
Children generally speak fluently by the age of 5. There are many stages involved in speech development (Table 1). The first is the pre-linguistic stage, which is the process of language development that starts in the months before a baby speaks his/her first word. Usually, below 1 month, babies generally only make crying or gurgling noises. Aged 1–3 months, babies can laugh and coo (making repetitive vowel sounds). Consonant sounds generally appear from age 6–7 months, when the baby has developed the muscle control needed to combine a consonant with a vowel sound. From 6 months, there is an increase in vowel/consonant combinations. This is known as ‘babbling’. Most babbling involves repetition of the same syllables (eg ‘dadada’ or ‘nananana’).3 Babbling is an important part of the preparation for spoken language. It is easy for adults to imitate, which then develops turn taking skills which may help the child to learn language, and it is more similar to adult speech. There are generally two different types of babbling; babbling with rising intonation, indicating that infants expect a reply, and babbling with falling intonation, indicating that they require no response.
Age
Speech Development
Stage
0–3 months
Recognizes tones/voices, coos and gurgles if content, cries if distressed
Pre-linguistic
6 months
Babbles – short sounds/use of consonants, eg da da, begins to understand emotion in voices
Pre-linguistic
9 months
Imitates simple words, starts to recognize own name, pointing, may understand simple words
Pre-linguistic
12 months
Strings together vowels and consonants to make repetitive sounds, understands more than he/she can say, responds to simple instructions, first words
Pre-linguistic
24 months
Can use simple sentences, ask simple questions, understands more
Linguistic
36 months
Speech can be understood by strangers, longer sentences
Linguistic
Usually the first sign that the child understands individual spoken words (receptive language) is evident from the age of 9 months. At this stage, children begin to make meaningful gestures and babbling becomes more understandable. Usually, by the age of 12 to 13 months, children will speak their first words.4 By 24 months, children are able to put words together and make simple sentences and by 30 months children are able to form longer sentences. From the age of 3 years, the majority of what a child says can be understood by others. Most children, by the age of 5 years, can use sounds effectively and have the ability to understand and use well-formed sentences.
The linguistic environment to which children are exposed can affect development, and some studies have shown that children exposed to less varied language in their early years do not seem to catch up later in terms of vocabulary. Firstly, interacting with others is important for speech development and the more interactions that occur, the richer the speech content will be. Additionally, the amount and quality of language a child hears has been shown to vary with social background. Studies by Hoff and co-authors5,6 looked at the causes and consequences of socioeconomic status (SES) on parent-child speech. These studies found that mothers from high SES have longer conversations with their children, and are more responsive to their children's contributions, whilst socially deprived families have been shown to talk and read less to their children, and use simpler vocabulary. However, Law and co-authors7 highlighted that the opportunity to communicate or interact with children has a greater effect on speech than poverty in itself.
Speech assessment
There are many variables that can affect the development and ability of speech and language. This article will now go on to explain some of these in relation to dentistry. It is important for dental professionals to be aware of typical speech and language development, and the various factors that can affect it. Additionally, if there are concerns, dental professionals should refer children for help and support.
Speech assessment helps to identify speech and language delays and impairments in young children and different tools are available for speech assessment. Speech and language therapists in the UK commonly use the CLEAR Phonology Screening Assessment (Figure 1). This screening assessment covers all the 44 phonemes (a single ‘unit’ of sound that has meaning) of English in all relevant syllable positions, ie initial, middle and final positions in the word. The CLEAR Phonology Screening Assessment comes with two record sheets separating the single phonemes from the two phoneme cluster combinations. To evaluate speech, children are shown a picture and asked to say what they see. The words used are examples of those phonemes that they are expected to be able to say at any given age: two, three, four and five or above years of age. The child is tested on the words for his/her age and younger years. For example, if a child is three years of age, the words come from the two and three year age word categories and, similarly, if the child is seven years old, assessment is made from the two to five year categories, allowing the full range to be tested. Table 2 demonstrates the words used at the lower (2+) and upper age brackets (5+).
Figure 1. CLEAR Phonology Screening Assessment.
Approximate Age
Sound
Target Words
Initial
Middle
Final
2+
p
Pencil
Teapot
Sheep
b
Boat
Baby
Crab
m
Mouse
Dummy
Drum
n
Knot
Banana
Lion
w
Window
Flower
h
House
5+
r
Rabbit
Mirror
3
Treasure
θ
Thumb
Path
ð
Feather
Interface of dentistry and speech
Impact of oral health and malocclusion on speech
A lack of confidence in their teeth or pain may make patients reluctant to speak. Studies have shown that children with straighter teeth are thought to be friendlier, of a higher social class, more popular and more intelligent.8 A study by Overby et al examined teachers' perceptions of children with speech sound disorders and concluded that intelligibility and speaker pitch appeared to be speech variables that influence teachers' perceptions of children's school performance.9 Nuttall et al examined the Children's Dental Health Survey 2003 and found that, for a small group of children, caries was reported to impact on oral function, self-confidence and a child's emotions, and highlighted the need for the nature of dental care to be considered in this patient group.10 They suggested that these children have potentially a greater need for intervention than those children who are not so affected by their oral condition.
Caries not only has a psychological impact, but also a physical impact. Gherunpong et al conducted a study to examine oral health-related quality of life in Thai primary school children.11 It was a cross-sectional study of 1126 children aged 11–12 and results showed that 11.8% of patients with toothache reported an impact on speech production. If caries has led to abscess formation that has spread extensively, patients may present with a ‘hot potato’ voice. Here speech has a defect in resonance and appears muffled due to space occupying lesions (dental abscess). This should of course resolve with treatment of the abscess.
Effects of missing teeth on speech
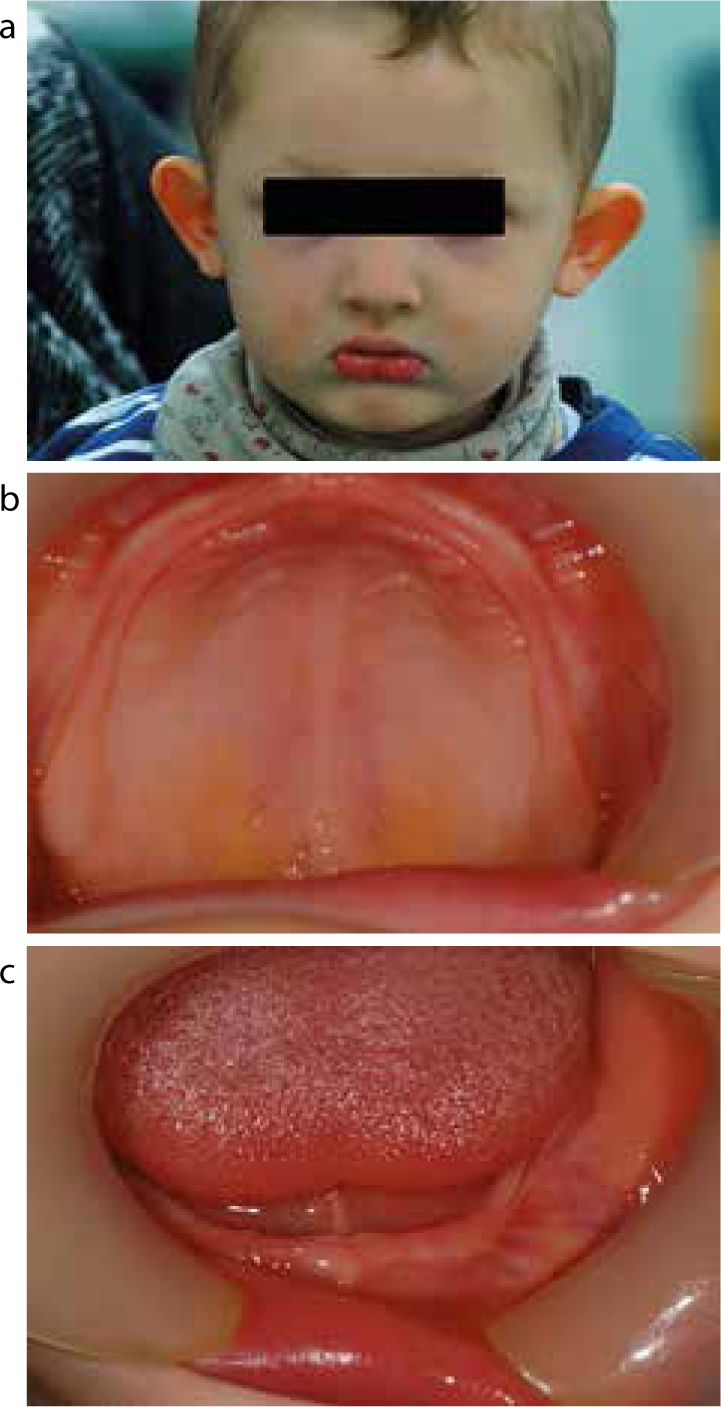
There are many case reports in the literature of patients with anodontia reporting speech problems, alongside reports showing that providing a prosthesis improves speech. In 2006, Dhiman et al presented a case of subtotal congenital anodontia.12 In this case, the patient complained of improper speech and, indeed, on examination the patient had poor phonetics, with escape of air orally during pronunciation of certain sounds such as ‘Vee’, ‘Aff’ and ‘Ash’. The patient had developed an inherent tendency to speak with minimum mouth opening. The patient complained of low self-esteem and, after construction of a prosthesis, felt that their self-esteem had improved along with their speech. This highlights the impact missing teeth can have on speech and the importance of consideration of intervention. Anecdotally, the authors report that the speech of the patients that they have treated is influenced by the absence of teeth. Figure 2 shows a 30-month-old boy with absent teeth due to ectodermal dysplasia, as an example of a relatively common condition associated with severe hypodontia or anodontia.
Figure 2.
(a) Extra-oral (b, c) and intra-oral views of a 30-month-old boy with absent teeth due to ectodermal dysplasia.
Effects of tooth loss on speech
Teeth play an important role in the course of producing certain sounds; they act as a functional landmark for the tongue. Teeth, along with the tongue and lips, obstruct and modify airflow between the incisal edges for articulation of consonants. The anterior teeth are important for the pronunciation of some sounds, especially the ‘s’ sound.
Snow studied the relationship between the articulation of six consonant sounds and the primary maxillary incisors In 438 children with a mean age of seven years, and found that a large proportion of children with missing or abnormal teeth articulated sounds incorrectly compared to those with an intact dentition.13
Bankson and Byrne studied the relationship between the exfoliation of primary teeth and the production of an ‘s’ sound. A sample size of 444 children, with a mean age of 73 months, was tested before and after loss of the primary teeth. The results showed that the most affected sound after tooth loss was an ‘s’ sound.14
Riekman and El Badrawy conducted a small retrospective study with no control to evaluate the long-term effects on articulation in a small sample of 14 children who had their primary maxillary teeth extracted at an early age, between two and four years of age. They found that 40% of the total sample displayed a degree of speech distortion, with 20% of them having a severe speech impairment for which corrective therapy was required.15 Lamberghini et al showed that loss of the upper front incisors caused issues with the pronunciation of the following – ‘f, v, t, d, n, s, z, l and th’.16
Factors that may influence the effects of tooth loss on speech
Factors that may influence the effects of tooth loss on speech include:
Age;
Compensation ability; and
Premature loss of primary incisors.
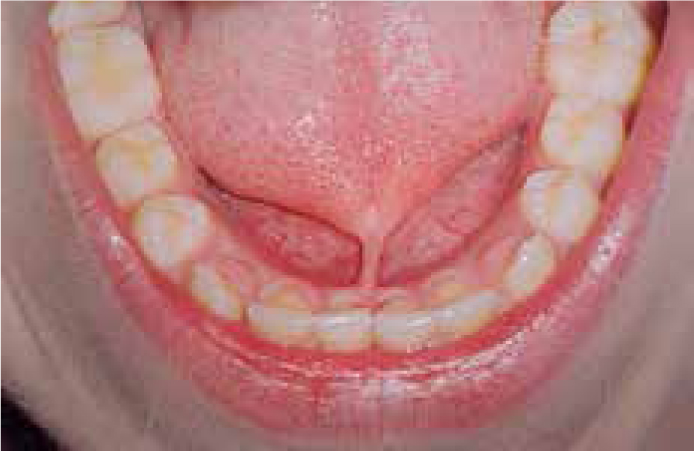
Age: at time of tooth loss age has been considered to be an important factor in the acquisition of correct sound articulation. Figure 3 shows a young child who has lost his upper incisors due to early childhood caries. The age range of three to seven is a critical period for the development of normal and correct sounds. Riekman and El Badrawy reported that patients who lost teeth before the age of 3 were more affected, stating that minor residual effects may occur if such extractions are performed in children younger than 3 years of age.15 On the other hand, Gable et al reported in a controlled study that loss of maxillary incisors in children with an age younger than five years is unlikely to cause defective articulation. They also found that the number of articulation errors that occurred in the children decreased with age.17
Figure 3. A young child who has lost his upper primary incisors due to early childhood caries. The evidence is unclear if this affects speech.
Compensation ability: Speech may not be distorted by the premature loss of teeth; this may be related to the child's ability to compensate for the loss of teeth during the time of exfoliation of primary teeth and eruption of permanent successors. This compensation occurs with the adjustment of the airstream by positioning the tongue and lips to articulate the correct speech sounds. Gradual changes may occur in the crowns of teeth with early childhood caries (ECC); teeth may have lost most of their original form and consequently their role in articulation. This gradual change is relatively slow and therefore allows for a degree of compensation and adaptation of articulation, unlike sudden tooth loss occurring in traumatic dental injuries (Figure 4). Turgut et al conducted a study to investigate whether early primary anterior tooth loss affected articulation in preschool children with ECC. They found that tooth loss did not influence articulation. It also showed that children under 5 years of age have an ability to compensate and correct their articulation of speech sounds despite the early primary anterior tooth loss.18
Figure 4. Early loss of primary teeth due to trauma. Speech distortion is unlikely and if it occurs is likely to be transient (parent's fingers used for retraction).
Premature loss of primary incisors: Holan and Needleman reviewed the short-and long-term possible consequence of premature loss of primary incisors following traumatic dental injuries. They concluded that any potential resultant speech distortion, such as lisping, is unlikely to develop; however, if speech impairment occurs, it is unlikely to be permanent and has a strong tendency to correct with the eruption of permanent successors.19
Restore or extract?
Considering the implications discussed, it is debatable whether any intervention is needed with regards to early loss of teeth above and beyond what a clinician would normally do. Many patients who require early loss of teeth are precooperative and are hence undergoing a general anaesthetic. Extraction is therefore often the chosen treatment due to its predictability as clinicians are reluctant to place restorations, which may have a questionable prognosis.20
There are reports in the literature of the use of overdentures in cases of early loss of primary teeth due to caries. Reported benefits included maintaining diet, re-establishing masticatory function, improving speech, and facial aesthetics in the patient.21,22 However, these are self-selecting case reports and this is not the experience or practice of most dentists treating children, where, in fact, children appear to adapt to the loss of teeth quickly. However, there is a real lack of high quality research on the effects of loss of teeth, despite this being a common procedure.
Tongue-tie
There are several definitions of a tongue tie (also known as ankyloglossia) but Klockars states that it is a congenital anomaly characterized by an abnormally short lingual fraenum. Prevalence has been quoted as 4–10% of the population, with a familial pattern.23
Currently there is no consensus regarding the indications, timing and method of surgical repair. Klockars et al undertook a study which looked at 317 patients undergoing release of tongue-ties and found that the most common indication for intervention, based on a questionnaire of patients or guardians, was indeed speech/articulation problems (64%).24 Suter and Bornstein undertook a review of the literature to look at the diagnostic criteria, indications, need for treatment and treatment options. They concluded that it is debatable as to which tongue-ties need to be removed and which can be monitored. They conclude that more high quality randomized trials must be undertaken to improve the evidence base.25
Tongue-ties can cause issues with breastfeeding, eating, dental hygiene, uncontrolled salivation, social issues and speech and communication (Figure 5). In terms of speech, tongue-ties can cause problems with the pronunciation of sounds such as t, d, s, z, l, n, sh and th as these all involve the use of the tongue tip. Speech can also sometimes sound blurred, drawled or slow due to tongue-ties impeding speech.
Figure 5. Patient presenting with an obvious tongue-tie. Tongue-ties can cause issues with breastfeeding, eating, dental hygiene, uncontrolled salivation, social issues and communication.
In 2013, Webb et al published a systematic review on the subject of tongue-tie division and the effect on breastfeeding and speech articulation. They concluded that surgical repair does provide benefits in breastfeeding, but that most evidence to suggest an association between speech problems and ankyloglossia was of low quality.26
Tongue thrust
Tongue thrusts are described as being endogenous (rare) or adaptive (more common) with differing aetiologies. This paper will only deal with the latter adaptive form. Tongue thrusts may occur as an adaptation of speech, to enable the patient to produce the desired sounds. The tongue thrust may then subsequently affect the occlusion. If a space is left between the anterior incisors because of the tongue thrust, sounds such as ‘s, z’ can be articulated too far forwards. This can be perceived as a ‘lisp’. Speech therapy can be unsuccessful in these cases as there is no barrier for the tongue.
Cleft lip and palate (CLP)
Cleft lip and palate can have a huge impact on speech articulation and speech and language therapy monitoring is essential for this patient group (Figure 6). Some patients with CLP make sounds too far back in their mouths or indeed create sounds in their throat instead. One theory as to why this occurs is that, when patients are babies and learning to talk, they try to stop air going through their nose so that they can make the sounds as expected in their mouths. As the yet unrepaired cleft palate does not function properly, they use the back of the tongue instead to try and create a barrier to the nose. This causes the tongue to become stronger at the back and to become relatively retro-placed, which can affect speech in the long term.
Figure 6. The presence of cleft lip and or palate has a very significant effect on speech development.
Cleft lip and palate patients can often also have problems in relation to hearing, which may hinder the development of speech. Jocelyn et al found that children with CLP had significantly lower scores on tests of cognition, comprehension, and expressive language abilities than matched control children at 12 and 24 months of age, and also had a higher frequency of middle-ear disease.27
Orthodontics and Occlusion
A Class I occlusion is deemed ideal for English articulation. If you deviate from a Class I or ideal jaw relationship, it has been shown that patients can get articulation errors. This is suggested to be caused by the fact that the tongue, teeth and lips are in incorrect positions.
Laine looked at the associations between articulatory disorders in speech and occlusal anomalies. He concluded that incorrect sound production occurs in occlusal anomalies, which affect the position of the tongue and hyoid bone, decrease the posterior intermaxillary space, or affect the size and shape of the front of the mouth. This therefore includes crossbites, anterior open bites, and Class II and III malocclusions.28 He found an association between an anterior open bite and a laterally or too anteriorly produced ‘s’ sound. A more recent study by Leavy et al in 2016, looking at malocclusion and its relationship to speech production generally, concurred. They concluded that an anterior open bite as little as 2 mm can cause speech production errors, and that the more severe the malocclusion, the more likely it is that a speech error will occur.29
Several orthodontic appliances can also affect the speech, although this effect is transient and resolves relatively quickly. Caniklioglu and Oztürk compared patient discomfort with lingual and labial fixed appliances. In relation to speech they found that speech difficulty was the most severe problem for the lingual group. Most patients, however, reported that any speech problem was resolved at the end of 30 days.30
As previously discussed, certain malocclusions can affect speech and some orthodontic treatment can temporarily affect normal articulations, as with decompensation for the treatment of Class III malocclusions using orthognathic surgery. This means that speech can also be affected due to the change in occlusion during orthodontic treatment, and it is important for clinicians to be aware of this and warn patients of this potential when appropriate.
Non-nutritive sucking
Anecdotally, speech and language therapists often prefer thumb-sucking as opposed to dummy use, as children tend to take the thumb out to play and a lot of speech development happens during play. This is in contrast to orthodontists who tend to favour dummy use over thumb-sucking, as it tends to be easier to stop. As previously stated, an AOB or Class II malocclusion can cause a person to misarticulate. It has long been known that non-nutritive sucking can cause the above, as it can cause proclination of the upper incisors and retroclination of the lower incisors and restricts their development. It also causes posterior crossbite and a narrowed maxillary dental arch.31 Effects of the habit depend on duration and intensity. Prolonged habits have been shown to lead to greater problems, in particular when continued for over 48 months.32
The British Orthodontic Society advises that, if the habit stops by the age of 7, when the adult teeth begin to appear, then the teeth can normally correct themselves with growth. It states that, if a child digit sucks for more than 6 hours per day, problems can occur in terms of malocclusion.33
Infants' feeding and sucking behaviours were investigated by Barbosa et al in a total of 128 three-to five-year-old children.34 They found that prolonged periods of sucking habits are related to speech disorders as they lead to myofunctional disorders, reduced oro-motor abilities and reduced oral awareness. The use of a pacifier beyond the age of three was found to have a negative impact on speech. They also found that the early start of bottle-feeding, under the age of nine months of age, may have an impact on speech development. This impact occurs due to the effect of sucking on the developing dentition, especially the upper labial segment alignment and the possible anterior open bite and posterior crossbite development. In bottle-feeding, only the buccinator muscles and the orbicularis oris muscle of the mouth are exerted and other muscles are not stimulated, so correct muscle activity is not promoted. Breastfeeding was found to decrease the risk of malocclusion in comparison.34 Broad concluded that sucking during breastfeeding promotes proper development of the oral motor structures and the correct muscle activity.35 Therefore, this will again be predicted to benefit normal speech development but there are no studies to confirm this.
Conclusion
The development of speech has been shown to be very complex, with many variables that may influence its development. As many of these are related to the oral cavity, dentists must be aware of normal development, and potential influences there may be on speech development, so that all patients can receive optimum care, support and referral when needed. Although this article focuses on speech, this is just one way of expressing language.
The absence, loss or malalignment of teeth has been shown to have an effect on speech but, unfortunately, many of these studies involve small convenience samples with limited follow-up. It is likely that, in most instances, children are able to adapt to change, without intervention. However, there is a need for larger studies to investigate the loss of teeth and any potential effect on speech or its development.