
References
McGeown M, O'Connell A Management of primary molar infra-occlusion in general practice. J Ir Dent Assoc. 2014; 60:192-198
Antoniades K, Kavadia S, Milioti K, Antoniades V, Markovitsi E Submerged teeth. J Clin Pediatr Dent. 2002; 26:239-242
Petcu A, Maxim A, Pasareanu M, Savin C Relevance of primary molars in development of occlusion in mixed dentition. Rom J Oral Rehabil. 2009; 1:16-19
Noble J, Karaiskos N, Wiltshire WA Diagnosis and management of the infraerupted primary molar. Br Dent J. 2007; 203:632-634
Sidhu HK, Ali A Hypodontia, ankylosis and infraocclusion: report of a case restored with a fibre-reinforced ceromeric bridge. Br DentJ. 2001; 191:613-616
Kurol J Infraocclusion of primary molars: an epidemiologic and familial study. Community Dent Oral Epidemiol. 1981; 9:94-102
Steigman S, Koyoumdjisky-Kaye E, Matrai Y Submerged deciduous molars in preschool children: an epidemiologic survey. J Dent Res. 1973; 52:322-326
Kurol J, Koch G The effect of extraction of infraoccluded deciduous molars. A longitudinal study. Am J Orthod Dentofacial Orthop. 1985; 87:46-55
Via WF Submerged deciduous molars: familial tendencies. J Am Dent Assoc. 1964; 69:127-129
Teague AM, Barton P, Parry WJ Management of the submerged deciduous tooth: 1. Aetiology, diagnosis and potential consequences. Dent Update. 1999; 26:292-296
Shalish M, Peck S, Wasserstein A, Peck L Increased occurrence of dental anomalies associated with infraocclusion of deciduous molars. Angle Orthod. 2010; 80:440-445
Parisay I, Kebriaei F, Varkesh B, Soruri M, Ghafourifard R Management of a severely submerged primary molar: a case report. Case Reports in Dentistry. 2013;
Mishra SK, Jindal MK, Singh RP, Stark TR, Hashmi GS Submerged and impacted primary molars. Int J Clin Pediatr Dent. 2010; 3:211-213
Bacetti T A controlled study of associated dental anomalies. Angle Orthod. 1998; 68:267-274
Jenkins FR, Nichol RE Atypical retention of infraoccluded primary molars with permanent successor teeth. Eur Arch Paediatr Dent. 2008; 9:51-55
Lai PY, Seow WK A controlled study of association of various dental anomalies with hypodontia of permanent teeth. Paediatr Dent. 1989; 11:291-196
Bjerklin K, Kurol J, Valentin J Ectopic eruption of maxillary first permanent molars and association with other tooth and developmental disturbances. Eur J Orthod. 1992; 14:369-375
Cobourne MT, Fleming SP, DiBiase T, Ahmed SOxford: Wiley-Blackwell, John Wiley and Sons Ltd; 2012
Ekim SL, Hatibovic-Kofman S A treatment decision-making model for infraoccluded primary molars. Int J Paediatr Dent. 2001; 11:340-346
Hobkirk J, Gill DS, Jones SP, Hemmings KW, Bassi GS, O'Donnell AL, Goodman JROxford: Wiley-Blackwell; 2010
Kokich VO Congenitally missing teeth: orthodontic management in the adolescent patient. Am J Orthod Dentofacial Orthop. 2002; 121:594-595
Bhatia SN, Leighton BCOxford: Oxford University Press; 1993
Gill DOxford: Wiley-Blackwell, John Wiley and Sons Ltd; 2008
Van der Beek MCJ, Hoeksman JB, Prahl-Anderson B Vertical facial growth and statural growth in girls: a longitudinal comparison. Eur J Orthod. 1996; 18:549-555
Kurol J, Thilander B Infraocclusion of primary molars and the effect on occlusal development. A longitudinal study. Eur J Orthod. 1984; 6:277-293
Kurol J, Thilander B Infraocclusion of primary molars with aplasia of the permanent successor. A longitudinal study. Angle Orthod. 1984; 54:283-294
Tieu LD, Walker SL, Major MP, Flores-Mir C Management of ankylosed primary molars with premolar successors: a systematic review. J Am Dent Assoc. 2013; 114:602-611
Soxman JA Infraocclusion of primary molars. In: Soxman JA (ed). Oxford: John Wiley-Blackwell, Wiley and Sons Ltd; 2015
Ostler MS, Kokich VG Alveolar ridge changes in patients congenitally missing mandibular second premolars. J Prosthet Dent. 1994; 71:144-149
Linqvist B Extraction of the deciduous second molar in hypodontia. Eur J Orthod. 1980; 2:173-181
Management of infra-occluded primary molars
From Volume 45, Issue 7, July 2018 | Pages 625-633
Article

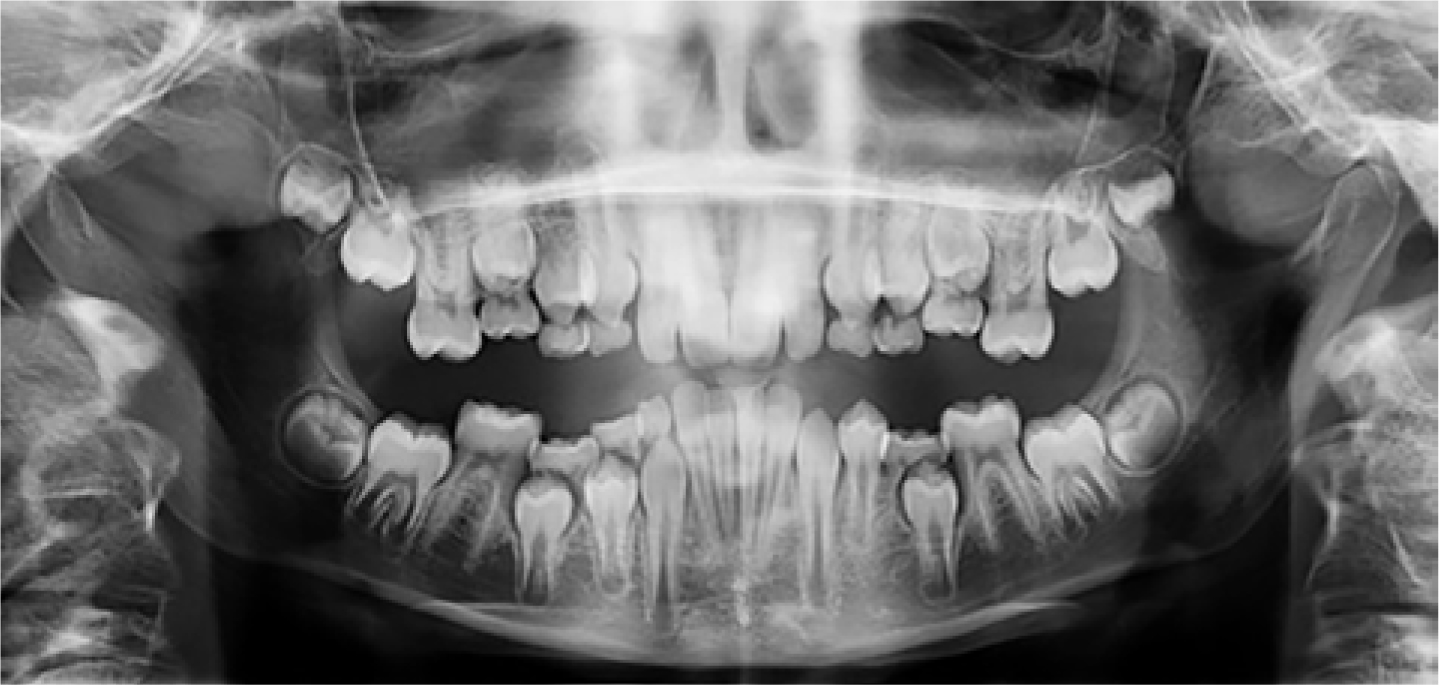
Infra-occlusion occurs when the eruptive mechanism of a tooth fails, which leads to the tooth failing to maintain its vertical position relative to the adjacent teeth.1 The marginal ridges of the infra-occluded tooth are below the marginal ridges of the adjacent teeth and the tooth lies below the occlusal plane2 (Figure 1). Infra-occlusion can affect both the primary and permanent dentition.3 It predominantly affects mandibular primary molars, with the mandibular second primary molar being most commonly affected followed by the mandibular first primary molar.4 The incidence of infra-occluded primary molars has been reported to range from 1.3–8.9%,5,6 however, some reports suggest that it can be as high as 38.5%.7 The incidence varies with patient age, but most frequently develops in the mixed dentition between the ages of 8–9 years old.4,8,9

Infra-occluded teeth have also been referred to as ‘submerging teeth’. However, the term ‘infra-occluded’ is more accurate as the position of the tooth is due to a failure of eruption rather than movement away from the occlusal plane.4
Aetiology
The most common cause of infra-occlusion is thought to be ankylosis. Ankylosis is an anomaly which occurs due to failure of the periodontal ligament to separate the root from the alveolar bone, leading to cementum and dentine being resorbed and replaced by bone, and resulting in fusion of the root and the bone. Consequently, the affected primary tooth remains static whilst the adjacent teeth continue to erupt, with continued vertical skeletal growth and occlusal development.2,10,11 The exact cause of ankylosis remains unknown, although factors such as traumatic injury to Hertiwg's epithelial root sheath, deficient local vertical bone growth, disturbance in local metabolism and local inflammation have been suggested.3,5,12 Other aetiological factors of infra-occluded primary molars include impaction, absence or an ectopic position of the permanent successor.13 Additionally, a genetic cause has also been suggested due to the increased incidence of ankylosis in siblings.6,9
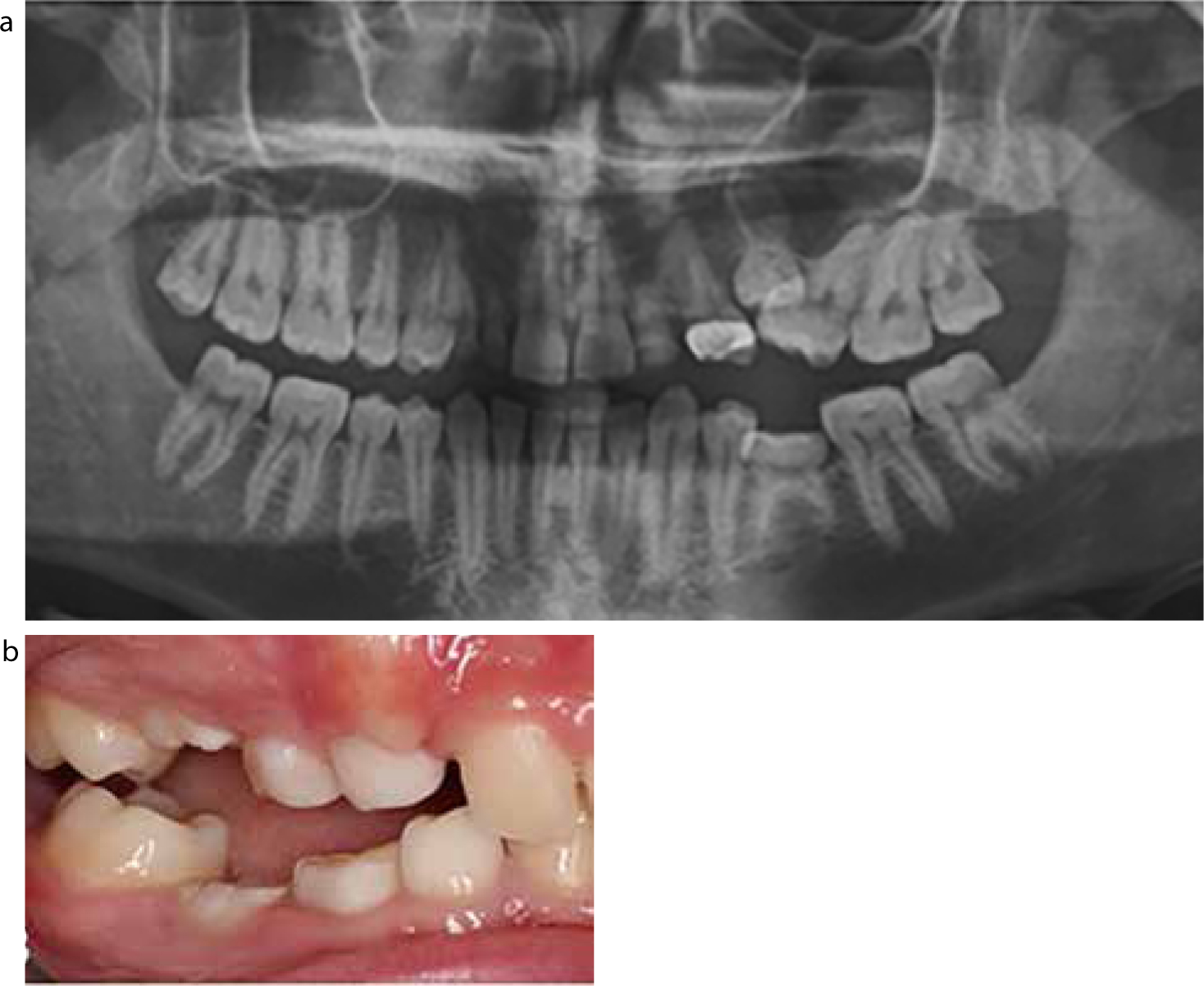
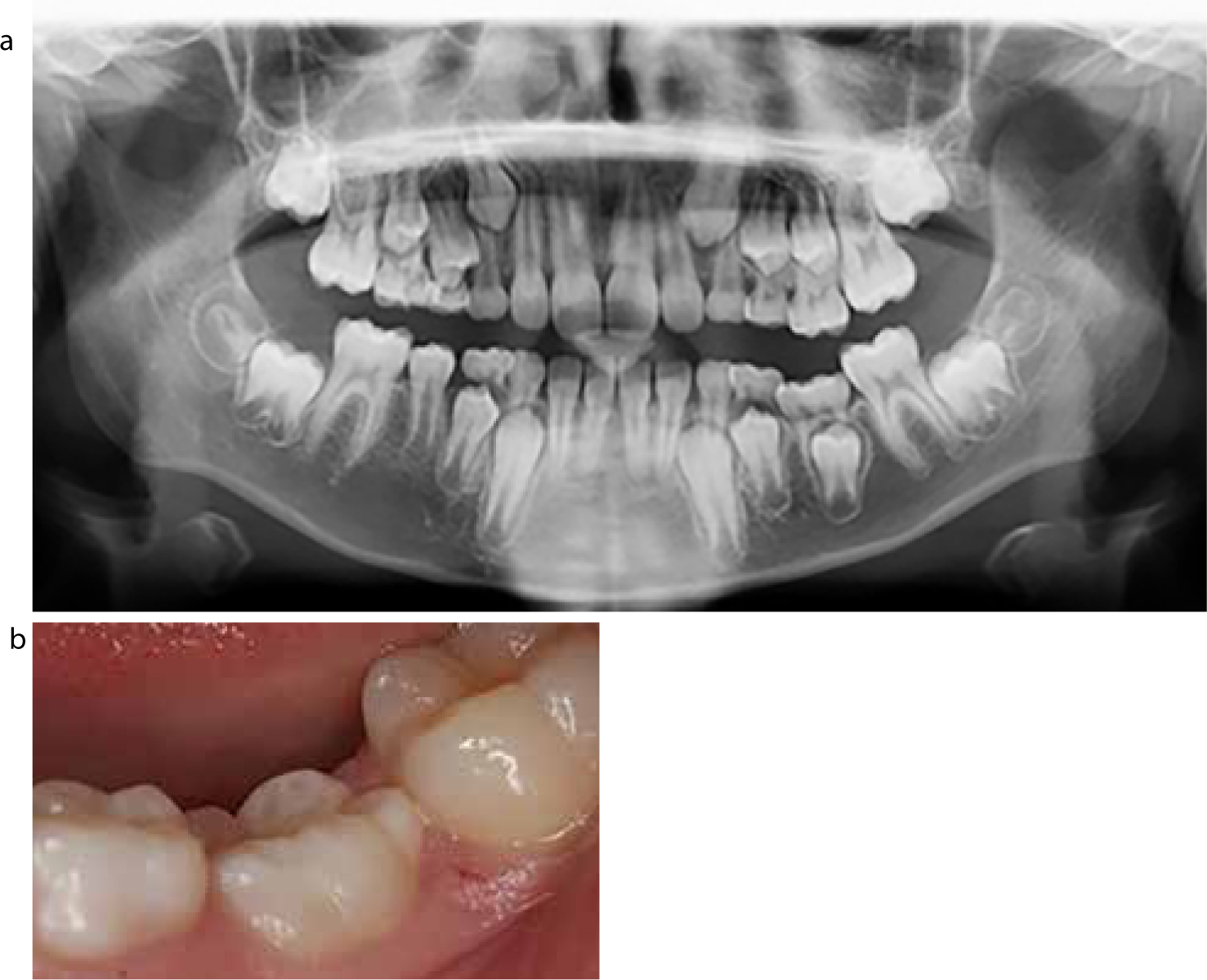
Infra-occluded primary molars have been associated with other dental anomalies, including peg-shaped lateral incisors, enamel hypoplasia, ectopic eruption of first permanent molars and the palatal displacement of maxillary canines.11,14 Another factor thought to play a role in infra-occlusion is hypodontia, with up to 65.7% of patients with missing permanent premolars having infra-occluded primary molars15,16 (Figure 2). The high prevalence of infra-occlusion in patients with hypodontia suggests a possible common aetiological mechanism.17

Classification
The severity of infra-occlusion can be classified according to the level of the occlusal surface of the infra-occluded tooth relative to the adjacent teeth. The following classification is commonly used:18
Severely infra-occluded teeth occur more commonly when there is hypodontia of the permanent successor.5
Diagnosis
Early recognition of infra-occluded teeth is important because it can facilitate appropriate and timely management and thus prevent long-term complications from arising. Diagnosing infra-occluded primary molars is predominantly based on the clinical findings. The infra-occluded tooth will be below the occlusal plane, with the marginal ridges of the infra-occluded tooth below those of the adjacent teeth1,2 (Figure 1). If the tooth is ankylosed it may be immobile and may give a characteristic metallic sound on percussion, however, it is important to use these diagnostic tools with caution.4,5 The high-pitched percussion tone can be subjective and is only present when at least 20% of the root surface is ankylosed, therefore it can be an inconsistent diagnostic tool and should not be used in isolation.19 A lack of mobility can also be unreliable because at least 10% of the root surface needs to be ankylosed before mobility is affected.19
When infra-occlusion is detected clinically, radiographs are indicated to confirm the presence or absence of the permanent successor.1 Periapical radiographs or dental panoramic radiographs (DPTs) can be used, each with their own merits. Figure 2 shows a patient with infra-occlusion of URDE, ULDE, LRDE and LLDE associated with hypodontia of LR45, UR34 and UL34, whilst Figure 3 shows a patient with infra-occlusion of the upper and lower Es with all the permanent successors present.
When a primary molar is retained, even when it is not infra-occluded, there will be a natural step in the occlusal plane due to the crown height of the primary molar being less than that of the adjacent permanent teeth.20 If the primary molar is infra-occluded, this step will increase as the adjacent teeth continue to erupt whilst the primary molar remains static. Angular bony defects may develop in the interproximal bone surrounding the infra-occluded tooth due to a cessation of vertical bone formation normally associated with eruption.10,21Figure 4 shows a bony angular defect between the infra-occluded LLE and the LL6. The presence of this angular bony defect can also aid in the diagnosis of infra-occlusion. Radiographic assessment may also show a lack of well-defined periodontal ligament and lamina dura and fusion of the root of the infra-occluded tooth with the surrounding alveolar bone.10 However, the latter may not be visible if the area of fusion is small or located on the buccal or lingual aspect of the affected tooth.

DPT radiographs are useful in assessing infra-occluded teeth relative to the adjacent teeth and to check for the presence or absence of the permanent successor (Figures 2 and 3). It may be easier to locate a permanent successor on a DPT than a periapical radiograph, due to the larger field of view: this is pertinent if the primary tooth is severely infra-occluded or the permanent tooth is ectopic. Due to the association of infra-occlusion with other dental anomalies, DPTs can also be useful in detecting any other dental anomalies that may be present.1
It is important to record the position of infra-occluded teeth accurately at each appointment so that the amount of infra-occlusion and any progression over time can be monitored. Infra-occlusion can be recorded clinically with direct measurements using the marginal ridges of the adjacent teeth as a reference, supplemented by clinical photographs or serial study models.1
The progression of infra-occlusion is related to the amount of vertical skeletal facial growth remaining, which is in turn related to patient age and gender.21 Distance and velocity growth curves for vertical facial growth show that there is an acceleration of vertical facial growth, and therefore tooth eruption, during puberty and that growth continues for longer in males than females.20,22 (Figure 5).
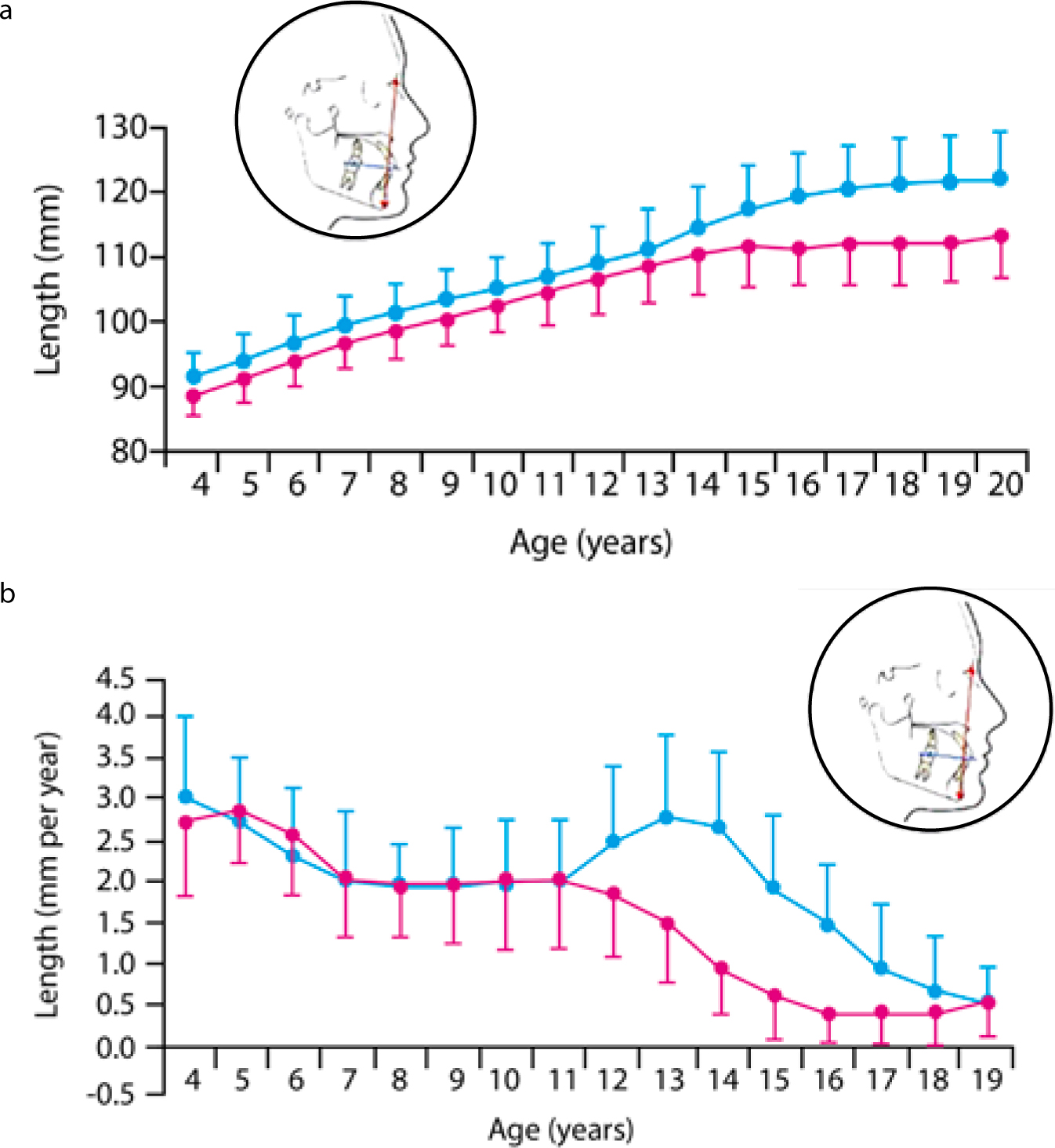
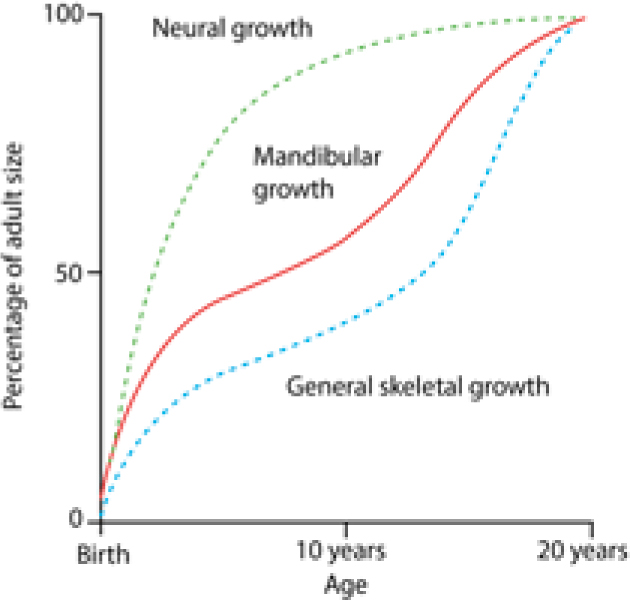
There is a correlation between the timing of facial growth and an individual's growth in stature23 (Figure 6). Orthodontists therefore commonly use standing height measurements, plotted on growth charts, to estimate the remaining amount of skeletal growth.24 These growth charts can, in turn, be used to predict the likely progression of the infra-occlusion.24 It is important to appreciate that the progression of infra-occlusion affects the prognosis of affected teeth. Severely infra-occluded teeth in patients with substantial remaining facial growth have a poorer prognosis than mildly infra-occluded teeth in patients with limited remaining growth.
Complications
There are many possible complications of infra-occluded primary molars, which can affect the infra-occluded tooth itself, the developing occlusion and the permanent successor, if present.23 These are summarized in Table 1.
| Feature | Consequence |
|---|---|
| Infra-occluded primary molar | Delayed exfoliation |
| Permanent successor | Delayed eruption or impaction |
| Developing occlusion | Potential site for developing malocclusion |
If left untreated, infra-occluded primary molars can cause an increased risk of occlusal disturbances, including tipping of the adjacent teeth, deviation of the dental centre line to the affected side and inhibition of vertical development of the adjacent teeth due to tension in the transeptal fibres of the periodontal ligament which interconnect the teeth5,23 (Figure 7).

The extent of tipping of the adjacent teeth can be related to the severity of the infra-occlusion, as illustrated in Figure 8 which shows two different patients. The first has a severely infra-occluded ULE and severe tipping of the adjacent teeth (Figure 8a). The second patient has milder infra-occlusion of the LRE and URE and subsequently less tipping of the adjacent teeth (Figure 8b).
Teeth opposing infra-occluded teeth can over-erupt, or a localized lateral open bite can develop if the opposing teeth do not over-erupt or maintain contact with the infra-occluded tooth.4 Additionally, infra-occluded teeth may be at an increased risk of periodontal disease and caries, due to difficult access for adequate oral hygiene.
Infra-occluded primary molars due to ankylosis are usually associated with a lack of adjacent alveolar bone development (Figure 9). This may be problematic if extractions are indicated or if any future restorative treatment is required, such as implant-supported restorations.

Infra-occluded teeth can have delayed exfoliation.1,8,25 If the permanent successor is present, the infra-occluded primary tooth usually exfoliates naturally, but is typically delayed by approximately 6 months.8,25 If the permanent successor is absent, the infra-occluded tooth can be retained for many years, even into adulthood. The prognosis of the infra-occluded primary molar will then depend on its root length, the severity of the infra-occlusion and the rate of progression of the infra-occlusion related to vertical facial growth and the eruption of the adjacent teeth. The rate of progression of infra-occlusion when the permanent successor is absent has been found to be, on average, 0.5 mm (+/- 0.26 mm) per year in one report.26
As well as the rate of progression of infra-occlusion, the prognosis of infra-occluded primary molars depends on caries, recession, tooth wear and the rate of root resorption. Root resorption of infra-occluded primary molars when the permanent successor is absent has been found to be, on average, 0.4 mm per year in one study.26
Management
Early diagnosis of infra-occlusion plays a pivotal role in its management and is important to prevent complications from arising. Factors which are important to consider when treatment planning patients with infra-occluded primary molars include:1,12
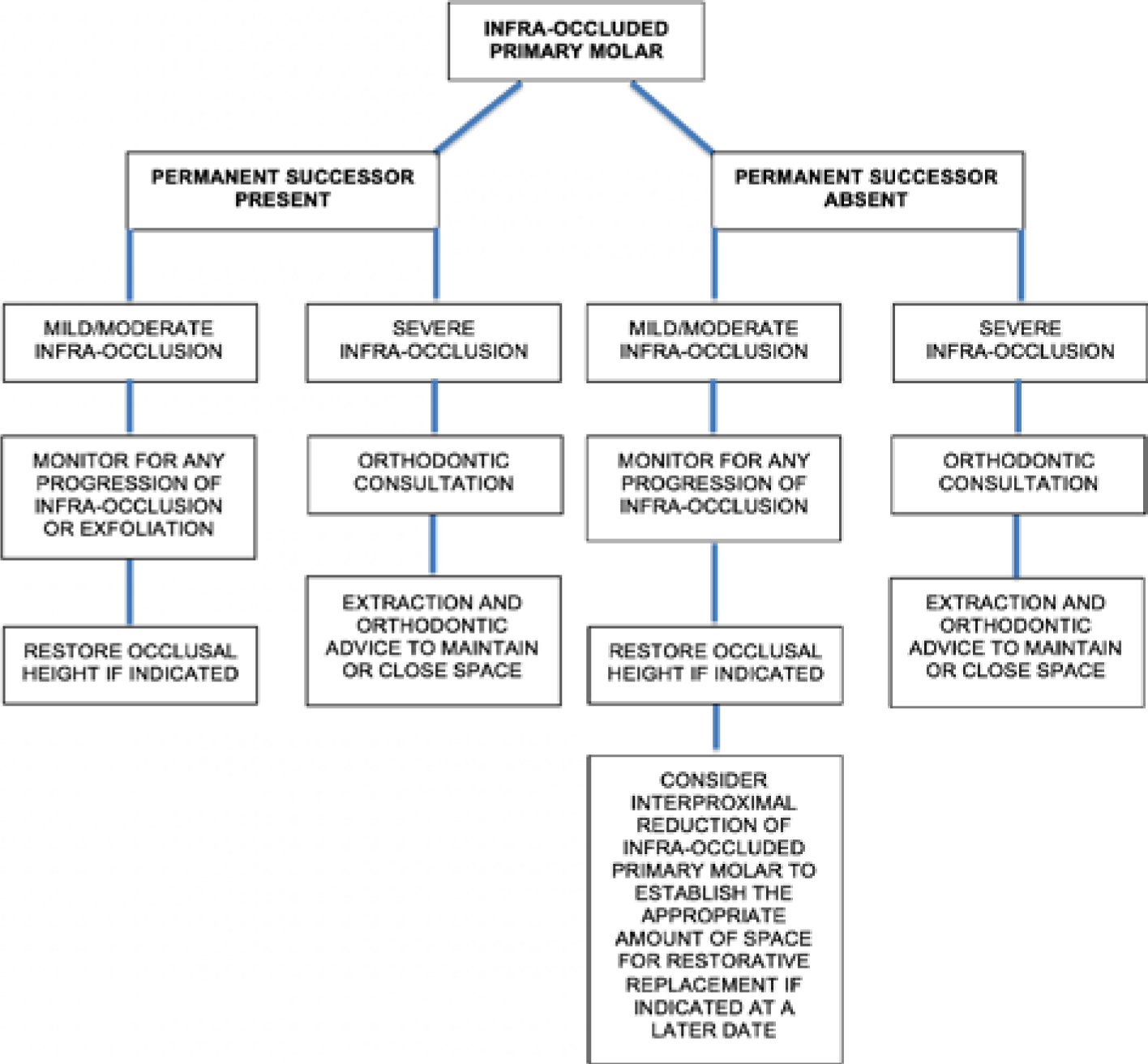
The management of infra-occluded primary molars is influenced by the presence or absence of the permanent successor. A flowchart depicting the main decisions for the management of infra-occluded primary molars can be seen in Figure 10.
Permanent successor present
The main aim of treatment of infra-occluded primary molars when the permanent successor is present is to achieve normal eruption of the permanent successor.20
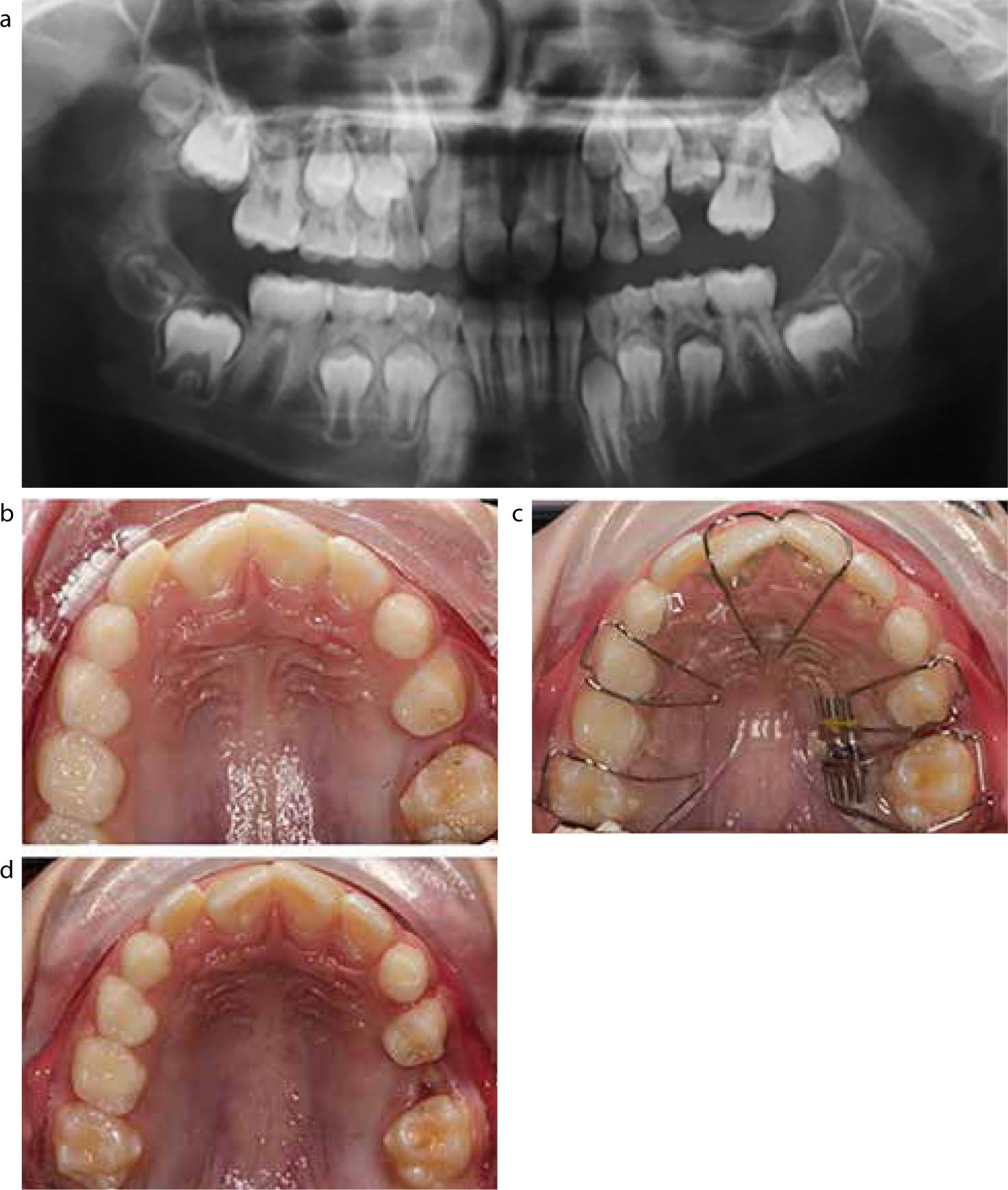
When the permanent successor is present, 96.7% of infra-occluded primary molars exfoliate naturally with normal eruption of the permanent successor, with a delay of up to six months compared to the contralateral, non-infra-occluded primary molars.8,25 General dental practitioners (GDPs) are well placed to monitor mild to moderately infra-occluded primary molars where the permanent successor is present. These teeth can be monitored at 3–6 monthly intervals and often require no intervention.1Figure 11 shows a patient with an infra-occluded LLE where the LL5 was present. The LLE was monitored and it exfoliated naturally and the LL5 erupted with no disturbances to the patient's overall occlusion.
If the occlusion is not stable (eg over-eruption; tipping of adjacent teeth), whilst awaiting eruption of the permanent successor, it can be beneficial to restore the occlusal height of the infra-occluded tooth. This can be completed using composite or stainless steel crowns.1 There is no evidence that building up an infra-occluded molar will reverse ankylosis.
The extraction of infra-occluded primary molars when the permanent successor is present may be indicated if the tooth is severely infra-occluded, with tipping of the adjacent teeth causing space loss and occlusal disturbances.25 Other indications for extraction include:
In severe cases, uprighting of the teeth adjacent to the severely infra-occluded tooth may be required to facilitate access for extraction of the infra-occluded tooth (Figure 12). Teeth can be uprighted using a removable appliance (finger spring or expansion screw design) or a sectional or full fixed appliance.
If extraction is indicated prior to the eruption of the permanent successor this can result in space loss.23 The use of a space maintainer to maintain arch length until the permanent successor erupts should therefore be considered. Space maintainers can either be fixed or removable in design. Fixed space maintainers include the band and loop or lingual/transpalatal arch. Removable space maintainers can be simple acrylic partial dentures or orthodontic retainer appliances. Removable appliances can usually be worn nights only to maintain tooth position.
Where the permanent successor is ectopically displaced, the management strategy may involve extraction of the infra-occluded primary molar, with surgical exposure of the permanent successor, if it is easily accessible. Bonding a gold chain and applying traction to the permanent successor, with a fixed appliance, may result in favourable movement.
In cases of severe infra-occlusion, severely ectopic permanent successors, space loss or occlusal disturbances, the patient should be referred to a specialist orthodontist for a full assessment and treatment planning.
Permanent successor absent
When a patient presents with an infra-occluded primary molar without a permanent successor, a decision needs to be made whether to retain or extract the infra-occluded primary molar.1 When treatment planning these patients, as well as the general factors to consider for infra-occluded teeth, it is also important to consider the overall malocclusion of the patient and any need for orthodontic treatment.1 Referral to a specialist orthodontist is advisable to facilitate treatment planning.10
Mild to moderately infra-occluded teeth, without a permanent successor in uncrowded arches where there is minimal remaining vertical facial growth, may be retained and monitored for any progression of the infra-occlusion.23 In the absence of ankylosis, primary molars without permanent successors may function for many years before exfoliation. The tooth may be maintained, preserving alveolar bone until facial growth is complete and some form of tooth replacement can be placed, if necessary. In such cases, the mesial and distal interproximal surfaces of the mandibular primary molar can be reduced to establish the appropriate amount of space for tooth replacement.28 Restoration of the occlusal surface may also be beneficial to prevent tipping of adjacent teeth, over-eruption of opposing teeth and to restore any loss of function.1
Extraction of the infra-occluded tooth may be warranted if the tooth is severely infra-occluded with subsequent occlusal disturbances. If the infra-occluded tooth is to be extracted, an orthodontic opinion should be sought to decide if the space is to be maintained and possibly restored, or closed. This will depend on the patient's presenting malocclusion. For example, if crowding is present elsewhere in the arch, extraction of the infra-occluded tooth may be indicated and the resulting space used as part of an overall orthodontic treatment plan.1
The extraction of infra-occluded primary molars when no permanent successor is present has also been advocated to prevent vertical bony defects worsening as infra-occlusion progresses.21 Extraction of the infra-occluded tooth allows the alveolar bone to develop occlusally as the adjacent teeth continue to erupt.29 It has also been advised to extract the infra-occluded primary molar early to achieve spontaneous space closure and therefore no alveolar defect in this area.30 At present, however, there is no research evidence to support this approach.
When extraction is the preferred treatment option for an infra-occluded primary molar, it is important to note that such teeth can be difficult and traumatic to extract and are more prone to fracture due to the ankylosis. Using an atraumatic extraction technique, including luxation to disrupt the bony union between the alveolus and the ankylosed tooth, should be considered before forceps are used to deliver the tooth. Surgical extraction may be necessary in teeth which are severely infra-occluded, or where access is impeded.1 However, surgical extraction can be destructive to the surrounding bone and lead to complications with space closure or future restorative treatment. Additionally, consideration needs to be made when surgically extracting infra-occluded primary second molars as there may be a risk of damage to the mental nerve, resulting in temporary or permanent paraesthesia.
Conclusion
In general, the management of infra-occluded primary molars depends on the severity and progression of infra-occlusion, the presence or absence of the permanent successor, as well as the patient's preference for the different treatment options. When the permanent successor is present, and the infra-occlusion is mild or moderate, the infra-occluded tooth usually has a good prognosis. When the permanent successor is absent and the infra-occlusion is mild or moderate, it is usually preferable to monitor the affected tooth or restore the occlusal surface, if required. When infra-occlusion is severe, the most appropriate option may be to extract the affected tooth. Successful management is dependent upon early diagnosis, good communication between the patient and the clinician and referral for an orthodontic opinion, where appropriate.