Moreinis SA. Avoiding perforations during endodontic access. J Am Dent Assoc. 1979; 98:707-712
Fuss Z, Trope M. Root perforations: classification and treatment choices based on prognostic factors. Endod Dent Traumatol. 1996; 12:255-264
Yildirim G, Dalci K. Treatment of lateral root perforation with mineral trioxide aggregate: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 102:55-58
Mente J, Hage N, Pfefferle T, Koch MJ, Geletneky B, Dreyhaupt J Treatment outcome of mineral trioxide aggregate: repair of root perforations. J Endod. 2010; 36:208-213
Bargholz C. Perforation repair with mineral trioxide aggregate: a modified matrix concept. Int Endod J. 2005; 38:59-69
Main C, Mirzayan N, Shabahang S, Torabinejad M. Repair of root perforations using mineral trioxide aggregate: a long-term study. J Endod. 2004; 30:80-83
Biodentine™ Active Biosilicate Technology™. Product Information Leaflet 2009.
Benenati FW, Roane JB, Biggs JT, Simon JF. Recall evaluation of iatrogenic root perforations repaired with amalgam and gutta-percha. J Endod. 1986; 12
Mannocci F, Vichi A, Ferrari M. Sealing ability of several restorative materials used for repair of lateral root perforations. J Endod. 1997; 23:639-641
Behnia A, Strasseler HE, Campbell R. Repairing iatrogenic root perforations. J Am Dent Assoc. 2000; 131:196-201
Baek SH, Plenk H, Kim S. Periapical tissue responses and cementum regeneration with amalgam, SuperEBA and MTA as root-end filling materials. J Endod. 2005; 15:444-449
Pitt Ford TR, Torabinejad M, McKendry DJ, Hong CU, Kariyawasam SP. Use of mineral trioxide aggregate for repair of furcal perforations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 79:756-763
Torabinejad M, Hong CU, Pitt Ford TR, Kettering JD. Cytotoxicity of four root-end filling materials. J Endod. 1995; 21:489-492
Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literaturer review – Part III: Clinical applications, drawbacks, and mechanism of action. J Endod. 2010; 36:400-413
Mente J, Leo M, Panagidis D, Saure D, Pfefferle T. Treatment outcome of mineral trioxide aggregate: repair of root perforations – long-term results. J Endod. 2014; 40:790-796
Bachoo IK, Seymour D, Brunton P. A biocompatible and bioactive replacement for dentine: is this a reality? The properties and uses of a novel calcium-based cement. Br Dent J. 2013; 214
Kvinnsland I, Oswald RJ, Halse A, Gronningsaeter AG. A clinical and roentgenological study of 55 cases of root perforation. Int Endod J. 1989; 22:75-84
Ghoddusi J, Sanaan A, Shahrami F. Clinical and radiographic evaluation of root perforation repair using MTA. N Y State Dent J. 2007; 73:46-49
Lin L, Chen MY, Ricucci D, Rosenberg PA. Guided tissue regeneration in periapical surgery. J Endod. 2010; 36:618-625
Camelo M, Nevins ML, Schenk RK. Clinical, radiographic and histologic evaluation of human periodontal defects treated with Bio-Oss and Bio-Gide. Int J Perio Rest Dent. 1998; 18:321-331
Richardson CR, Mellonig JT, Burnsvold MA, McDonnell HT, Cochran DL. Clinical evaluation of Bio-Oss a bovine derived xenograft for the treatment of periodontal osseous defects in humans. J Clin Periodont. 1999; 26:421-428
Peetz M. Characterization of xenogenic bone material. In: Boyne PJ (ed). Chicago: Quintessence; 1997
Tsesis I, Rosen E, Tamse A, Taschieri S, Del Fabbro M. Effect of guided tissue regeneration on the outcome of surgical endodontic treatment: a systematic review and meta-analysis. J Endod. 2011; 37:1039-1045
Stoecklin-Wasmer C, Rutjes AW, da Costa BR, Salvi GE, Juni P, Sculean A. Absorbable collagen membranes for periodontal regeneration: a systematic review. J Dent Res. 2013; 92:773-781
A 43-year-old male reported with pain and swelling in the maxillary anterior region as a result of iatrogenic perforation of his right maxillary central incisor tooth. After attempted internal repair, surgical management was required due to repair material extrusion. Removal of the extruded material preceded repair of the perforation site with biosilicate cement which had a short initial setting time. The set repair material then allowed Guided Bone Regeneration (GBR) to be performed to reduce the risk of recession in a single surgical process. At 24-month recall, the patient was asymptomatic with no clinical or radiographic evidence of ongoing disease. Additionally, the patient presented with excellent aesthetics after surgical management.
CPD/Clinical Relevance: Comprehensive management of endodontic perforations, especially in the anterior dentition, should stretch beyond tooth survival and include the need to maintain and improve the patient's aesthetics.
Article
A lateral perforation is an iatrogenic injury that may occur during endodontic treatment. Such perforations are artificial openings in the root canal wall that result in a communication between the pulp space and periodontal tissue. Although a perforation may occur due to resorption processes or caries, the most frequent cause is iatrogenic in nature. Planning for endodontic access should be as precise as possible.1 When this is not the case, it may occur during access preparation, instrumentation of the root canal anatomy or during post space preparation. This may predispose to hypochlorite accidents, cause inflammation of the periodontal tissue, infection and eventual loss of the tooth.2
The management strategy for perforations depends on a number of factors, including perforation size, accessibility of perforation, periodontal condition, patient motivation, strategic importance of tooth, quality of the root canal therapy and operator factors, including experience. The main options for treatment are:
Non-surgical repair (internal repair);
Surgical repair (external repair);
A combination of non-surgical and surgical repair; or
Location of the perforation plays a role in prognosis, as those that do not communicate with the gingival sulcus, and are surrounded by healthy periodontium, usually have a favourable prognosis. Other factors affecting prognosis include time of treatment, size and location.2 Many authors have suggested that small perforations have a more favourable prognosis and are more amenable to direct and immediate sealing with a decreased likelihood of periodontal breakdown. As the size of the defect increases, so does the potential for an overfilling during the repair procedure and creating an inadequate seal.4
Should repair of the perforation be attempted, the choice of repair material is an important factor in the prognosis of the endodontically treated tooth with a perforation defect, regardless of treatment modality. Prognosis is affected by the biocompatibility and sealability of the repair material. It has been highlighted that quality of the seal of the defect is correlated to improved prognosis of the tooth.5
A number of materials have been used for the repair of root perforations including amalgam, Intermediate Restorative Material®, zinc oxide eugenol, Super EBA™, Cavit®, gutta-percha, glass ionomer cement, resin-modified glass ionomer cement, composite resin and Mineral Trioxide Aggregate (MTA).6
Although MTA has emerged as the benchmark repair material, other calcium silicate cements have been developed to overcome MTA's disadvantages. In 2009, a new calcium silicate-based material was released named Biodentine™ (Septodent, France). Biodentine™ is an inorganic, non-metallic compound presented in a capsulated powder and liquid form. The powder phase consists of tricalcium silicate, calcium carbonate and zirconium dioxide and the liquid phase combines calcium chloride, water and a water-reducing agent.7 It has several endodontic indications, including management of root perforations.
Periodontal inflammation, as a consequence of lateral perforation, may lead to bone loss, pocketing or recession, which has the greatest impact in the aesthetic zone. It has been suggested that complex bony defects may be regenerated during endodontics or periodontal surgery using graft materials. This procedure, known as Guided Tissue Regeneration (GTR), may improve the outcome of such cases, although the evidence base is sparse.
The purpose of this article is to demonstrate the combined use of a calcium silicate cement (Biodentine™) and the GTR technique in the comprehensive management of a lateral perforation with an associated complex periodontal bony defect.
Case report
A 43-year-old male patient was referred by his dentist to a large teaching hospital with a suspected perforation in 2010. This may have occurred during endodontic treatment or post preparation to the upper right central incisor. The patient's medical history was non-contributory.
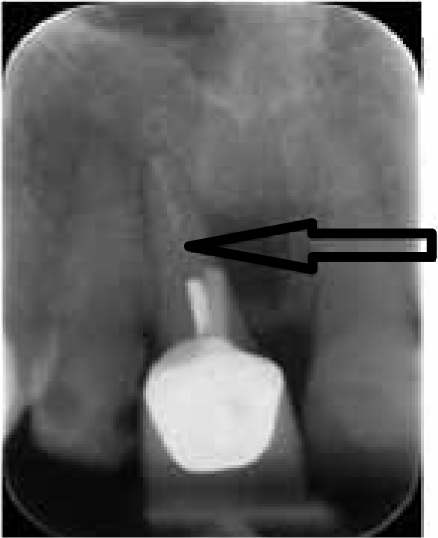
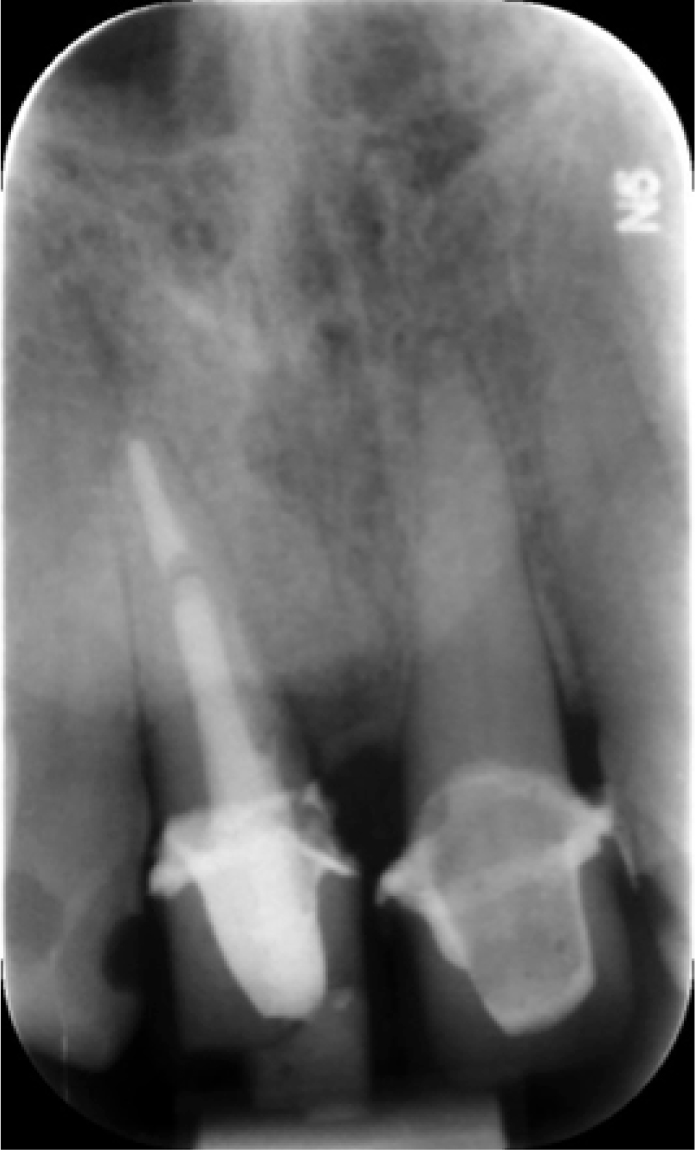
The patient complained of a ‘blood blister’ which would frequently increase in volume then ‘burst’ in the sulcus adjacent to the tooth in question. Clinical examination revealed a draining sinus adjacent to the UR1. Radiographic review indicated a fractured metallic post within the canal which appeared off centre. Additionally, a root filling was present beyond the length of the post which appeared poorly condensed. A radiolucency associated with the mesial aspect of the root was present (Figure 1).
Figure 1. Pre-operative periapical radiograph demonstrating lateral radiolucency and post which is not in the long axis of the tooth (arrowed).
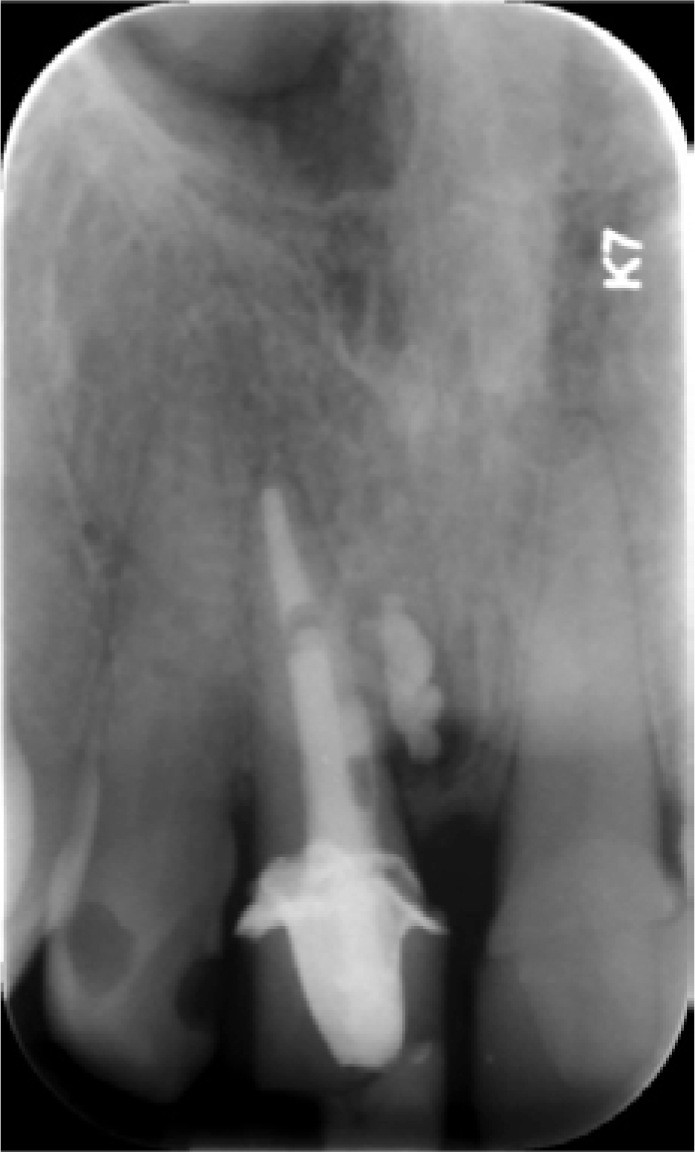
A diagnosis of periradicular periodontitis associated with a root perforation was made. Initial treatment was to attempt orthograde root retreatment and internal perforation repair using MTA. This approach was taken in light of the poorly condensed root filling. During this procedure it was noted, through tactile inspection of the root canal system, that the perforation was located on the proximal surface of the root. This procedure resulted in extrusion of MTA during post placement owing to the large size of the pre-existing perforation. The patient's signs and symptoms continued. Clinical and radiographic examination confirmed a persistent sinus and radiolucency surrounding the MTA (Figures 2 and 3). At this stage, the patient was referred for specialist assessment and management.
Figure 2. A radiographic view following endodontic retreatment and definitive post in situ. Note the extruded repair material lateral to the tooth. Orthograde repair of the perforation resulted in extrusion of material lateral to the tooth.Figure 3. View of the anterior maxilla at follow-up after attempted internal repair; buccal swelling can be seen (arrowed).
Treatment options were then discussed with the patient, including extraction or surgical exploration of the area. As the patient wished to save the tooth, endodontic surgery was planned and written informed consent was obtained.
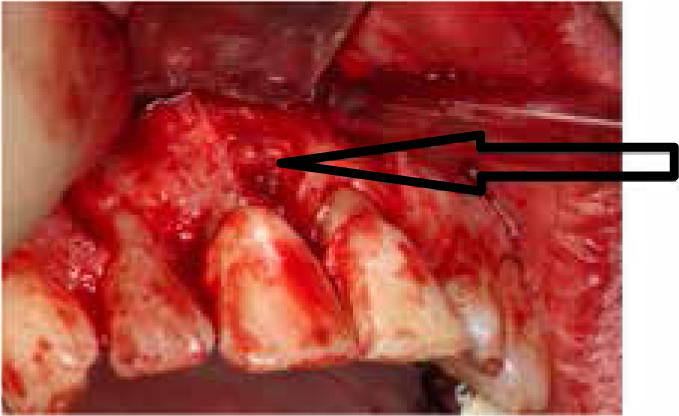
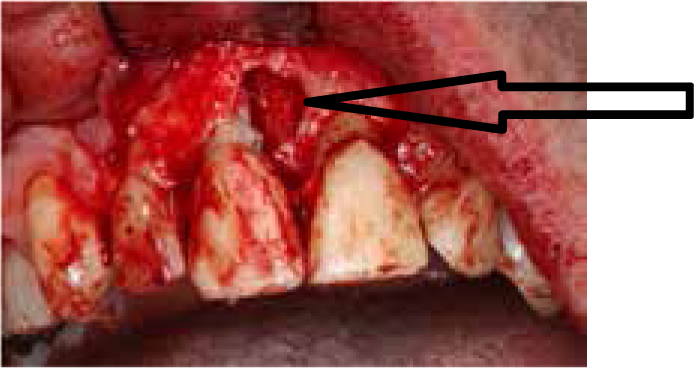
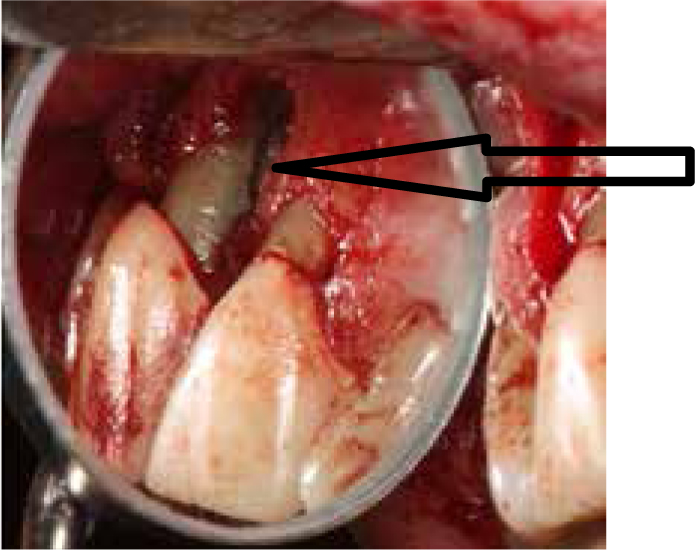
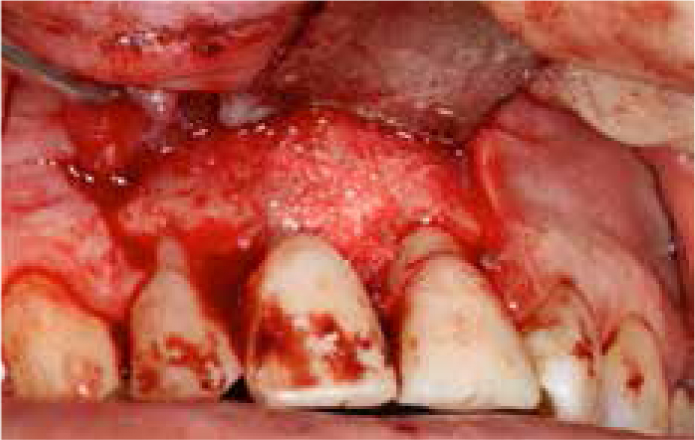
During the presurgical assessment it was again noted that there was no periodontal pocketing of concern. After the administration of local anaesthesia with 6.6 ml of 2% lignocaine with 1:80.000 adrenaline (Lignospan Special, Septodont, Saint Maur des Fosses, France), a buccal, 3-sided mucoperiosteal flap, extending from the distal aspect of tooth UR2 to the distal aspect of tooth UL1, was raised. A mesial bone defect filled with granulation tissue was apparent. The tissue which had filled in the bone site and excess reparative material was removed with hand currettes (Figures 4 and 5). A large mesial perforation was visible, with an operating microscope and a complex periodontal defect, revealing that a communication between the lateral bone loss and marginal bone level was present (Figure 6).
Figure 4. View after reflection of mucogingival flap displaying granulation tissue (arrowed).Figure 5. View after curettage of tissue. Note communication between mesial bony defect and crestal bone loss (arrowed).Figure 6. View showing the mesial perforation site following preparation with ultrasonic tips (arrowed).
The orthograde filling and repair material within the perforation site was inspected and found to be insufficient, displaying voids marginally. The material was removed from the site with the assistance of ultrasonic KiS Tips (Obtura Spartan Endodontics, Illinois, USA).
A lateral cavity was irrigated with saline and the Biodentine™ (Septodont, Saint Maur des Fosses, France) was mixed as per the manufacturer's instructions.7 A single-dose container of liquid was squeezed into a capsule containing a single dose of powder. The capsule was closed and placed in a mixing device (Silamat, Ivoclar Vivadent, Liechtenstein) at a speed of 4000–4200 rotations/min for 30 seconds. The mixed material was then loaded into a Lee Block® (G Hartzell & Son, Concord, Calfornia, USA) and packed into the perforation site with a carver to ensure a good seal. The material was smoothed and allowed to set for 12 minutes, as directed by the manufacturer8 (Figure 7).
Figure 7. View with Biodentine™ repair in situ on mesial aspect of root.
Bio-Oss Collagen® (Geistlich, Geistlich Pharma AG, Switzerland) is a mixture of bovine bone with 10% porcine collagen to improve handling characteristics. A xenograft bone substitute graft material (Bio-Oss Collagen® block, Geistlich, Geistlich Pharma AG, Switzerland) was prepared by mixing with saline solution and surrounding blood. The walled bony defect was then packed with grafting material by applying in situ and modelling to the defect (Figure 8).
Figure 8. View of Bio-Oss® adapted to bony defect.
Bio-Gide® (Geistlich, Geistlich Pharma AG, Switzerland), a bilayer, xenograft porcine collagen membrane, covered the bone graft material, with the porous surface of the bilayer material facing the bone. The flap was then repositioned and six interrupted, monofilament, non-absorbable, Novafil™ (Covidien, Mansfield, MA, USA) sutures placed (Figure 9).
Figure 9. View of replaced flap with monofilament sutures stabilizing the closure of the surgical site.
A fortnight following surgery, the sutures were removed and a post-operative radiograph taken. The patient reported minimal pain and discomfort and the site appeared to be healing well.
Laboratory-fabricated provisional composite crowns were cemented one month after surgery. Following a seven-month period of unincidental healing, the provisional crowns on the upper central incisors were replaced with definitive crowns (Figure 10). The patient returned for review one year post-surgery and radiographic review showed healing, with no evidence of radiolucency surrounding the root. At one year review, the patient was asymptomatic and showed no evidence of periapical disease and no further bone loss. There was no recession and periodontal probing revealed no pocketing greater than 2 mm. The post-operative photographic and radiographic views at 24 months showed an excellent aesthetic outcome with minimal evidence of previous surgery and healthy periradicular tissues (Figures 11 and 12).
Figure 10. Radiograph at seven months post-surgery displaying no evidence of periapical disease and no deterioration in bone height. Provisional crowns are in place.Figure 11. Radiograph at 24 months post surgery illustrating healing with definitive coronal restorations cemented.Figure 12. View of anterior maxilla 24 months post surgery with minimal evidence of surgical intervention.
Discussion
The ideal material for root perforation repair should be non-toxic, capable of providing an adequate seal, non-resorbable, radio-opaque, bacteriostatic and encourage fibroblastic activity.8-11 In the past decade, MTA has been a popular material for the repair of perforation defects. MTA is a calcium silicate-based cement. Many studies have documented the biocompatible nature of MTA.12,13 In addition, its ability to set is not affected by the presence of moisture, such as body fluids, including blood.14 The biocompatibility of MTA, the ability of this material to seal root perforations effectively,3,5 and its setting properties in the presence of moisture are important characteristics that may result in greater success rates when used for treating perforations. MTA appears to provide a biocompatible and long-term effective seal for root perforations in all parts of the root.6
In a study of 16 cases by Main et al, the success of perforation repair with MTA was demonstrated over 12–45 months. No radiolucencies developed in cases which were absent of lesions prior to repair. Additionally, evidence of bony infill was seen in all cases presenting with an initial radioluency.6 In a study of 64 teeth by Mente et al, perforations repaired over a 12-year period with MTA showed an 86% healing rate, both clinically and radiographically.15 However, MTA also has some disadvantages, including long setting time (2 hours 45 minutes), discoloration potential, difficult handling characteristics, high material cost and the difficulty of its removal after setting.14
Biodentine™ is a newer calcium silicate cement with properties similar to MTA. The material does, however, display some improvements over MTA specific to repair of root perforation, namely improved handling and much quicker setting time at 12 minutes.16
The indications for Biodentine™ are similar to those for MTA, namely that it may be used for temporary enamel restoration, permanent dentine restoration, deep or large carious lesions, deep cervical or radicular lesions, pulp capping and pulpotomy. Uses in the root include perforation repair, internal/external resorptions, apexification and retrograde surgical filling.7 There has also been a suggestion that, where MTA cements are currently the material of choice, Biodentine™ may have additional benefits.
Cautions for the use of Biodentine™ include its radio-opacity being very similar to dentine, making its detection difficult. It has been suggested that its handling characteristics are not much improved over MTA, displaying similar slumping during placement. Additionally, as it is a newer product, many clinical follow-up studies are yet to be published.
During management of perforations, especially in the aesthetic zone, perforation repair and endodontic healing may not be the only consideration. Prevention of clinical attachment loss and recession associated with the perforation site is also of significant importance. Studies suggest that, if a perforation is not immediately sealed, even within a non-infected root canal system, secondary periodontal inflammation will occur.17,18 Any bony defect which may arise due to the perforation should also be managed. This may include the use of bone grafts and GTR. The ability of bone grafts to induce new bone formation has been suggested. However, new PerioDontal Ligament (PDL) and cementum regeneration in periapical surgery has not been shown to benefit from the use of bone grafts.19
A common material for bone grafting is xenograft material. Xenografting is the transplantation of cells, tissues or organs from one species to another. In this context, the xenograft material of interest is bone substitutes. One such product is Bio-Oss® (Geistlich, Geistlich Pharma AG, Switzerland). Bio-Oss® is a grafting material that has been used as a bone substitute for several years with its use documented since the 1990s.20,21 The material is characterized as deproteinized bovine bone mineral and has a wide variety of applications. One of the suggested favourable qualities of Bio-Oss® is that its structure closely resembles human bone.22 It contains wide interconnecting pores that acts as a scaffold and could promote migration and attachment of cells and vascularization. Bio-Oss® is strongly hydrophilic and the particles stick to each other when combined with blood at the surgical site.
The technique for directing the growth of new bone and gingival tissue at sites having insufficient volumes or dimensions of bone is known as guided tissue or guided bone regeneration. GTR is the method for prevention of migration of the epithelial cells along the cemental wall of the root surface. Preventing this migration favours repopulation of the defect by cells from the PDL and bone. This concept is based on the assumption that periodontal ligament cells have the potential for regeneration of the attachment apparatus of the tooth. In order to prevent the migration of these epithelial cells, a membrane is used. Membranes can be categorized as either degradable, such as collagen, the major benefit of these being that there is no need for retrieval. The alternative type being non-degradable, these must be removed within three to six weeks and include Millipore™ (Billerica, Massachusetts, USA), Teflon membrane and Goretex™ (WL Gore & Associates Inc, Flagstaff, Arizona, USA). Clinically, the best application of membrane barriers in periapical surgery appears to be in combined endodontic-periodontal or large periapical lesions communicating with the alveolar crest.19,23 In these cases, PDL and cementum are lost so that there is an increased likelihood of apical migration of the junctional epithelium along the denuded root surface, which may lead to recession. The aim of the membrane barrier is to allow selective repopulation of the defect with cementum, periodontal ligament and bone. Increasingly, the use of absorbable collagen xenografts, which contain collagen derived from porcine origin, have become popular used as a barrier membrane. Bio-Gide® is such a product. The membrane is degraded enzymatically.24 The product has a natural bilayer and a recent systematic review supports the clinical efficacy of GTR procedures with collagen membranes.25 The membrane is additionally strongly hydrophilic and adheres well, often without the need for suturing.
In this case report, Bio-Oss Collagen® was used to prevent collapse of the Bio-Gide® membrane. It is believed that this prevented epithelial down growth of the gingival epithelium and favourable healing of the defect with bone and periodontal ligament tissue. Biodentine™ was favoured for the external perforation repair as it was allowed to set prior to Bio-Oss® placement, owing to its short setting time. The author's experience is that MTA in the same situation would have been displaced, owing to its long setting time, when the Bio-Oss® was placed.14
Conclusion
In this report, a case was presented which involves management of a lateral perforation managed with a newer calcium silicate cement and guided bone regeneration in a one stage process. This allowed successful healing of the defect and resolution of the patient's symptoms without compromising the long-term aesthetics of the anterior dentition. The authors believe that this treatment modality could become a popular technique for comprehensive patient management of similar cases in the future.