Brumfield RC. Fundamental mechanics of dental bridges, 5th edn. In: Tylman SD, Tylman SG. St Louis: The CV Mosby Company; 1965
Howe DF, Denehy GE. Anterior fixed partial dentures utilising the acid-etch technique and a cast metal framework. J Prosthet Dent. 1977; 37:28-31
Djemal S, Setchell D, King P, Wickens J. Long-term survival characteristics of 832 resin-retained bridges and splints provided in a post-graduate teaching hospital between 1978 and 1993. J Oral Rehabil. 1999; 26:302-320
King PA, Foster LV, Yates RJ, Newcombe RG, Garrett MJ. Survival characteristics of 771 resin-retained bridges provided at a UK dental teaching hospital. Br Dent J. 2015; 218:423-428 https://doi.org/10.1038/sj.bdj.2015.250
Thoma DS, Sailer I, Ioannidis A, Zwahlen M, Makarov N, Pjetursson BE. A systematic review of the survival and complication rates of resin-bonded fixed dental prostheses after a mean observation period of at least 5 years. Clin Oral Impl Res. 2017; 28:1421-1432 https://doi.org/10.1111/clr.13007
Hannig C, Laubach S, Hahn P, Attin T. Shear bond strength of repaired adhesive filling materials using different repair procedures. J Adhes Dent. 2006; 8:35-40
Sasse M, Kern M. Survival of anterior cantilevered all-ceramic resin-bonded fixed dental prostheses made from zirconia ceramic. J Dent. 2014; 42:660-663
Dahl BL, Krogstad O, Karlsen K. An alternative treatment in cases with advanced localized attrition. J Oral Rehabil. 1975; 2:209-214
Botelho MG, Ma X, Cheung GJ, Law RK, Tai MT, Lam WY. Long-term clinical evaluation of 211 two-unit cantilevered resin-bonded fixed partial dentures. J Dent. 2014; 42:778-784 https://doi.org/10.1016/j.jdent.2014.02.004
Jepson NJ, Moynihan PJ, Kelly PJ, Watson GW, Thomason JM. Caries incidence following restoration of shortened lower dental arches in a randomized controlled trial. Br Dent J. 2001; 191:140-144
Smyd ES. Dental engineering as applied to inlay and bridge fabrication. N Y J Dent. 1951; 21:161-163
A contemporary approach to the provision of tooth-supported fixed prostheses part 2: fixed bridges where the abutment teeth require minimal or no preparation
A contemporary approach to the provision of tooth-supported fixed prostheses part 2: fixed bridges where the abutment teeth require minimal or no preparation Richard Ibbetson Dental Update 2024 45:2, 707-709.
Fixed tooth replacement is a central part of prosthodontic care for patients. The approach and options for treatment have changed due to the decrease in dental disease in the population and the impact of the osseo-integrated implant. Despite the impact of the dental implant, there remain indications for the use of tooth-supported fixed prostheses. The impact of improving oral health, the continued developments in resin-retained bridgework and the dental implant have reduced the indications for fixed prostheses retained by crowns. The last 30 years have seen a simplification in the design of fixed bridgework and this article describes the contemporary approach to this treatment modality. The second of this two part series discusses the influence of patient choice and the use of fixed bridges requiring little or no tooth preparation.
CPD/Clinical Relevance: To assist the reader in appreciating the principles of design for fixed bridgework whether supported by crowns or resin retainers.
Article
The first part of this two part series described the changes that have taken place in the design principles for tooth-supported fixed bridgework retained by crowns. It emphasized that there are fewer indications for these types of bridge due to the decrease in dental disease, the availability of effective, more conservative options and the use of dental implants. However, as is described in the first section of Part 2, the preference of the patient may influence the choice of prosthesis. The second part of this article will then describe the provision of tooth-supported fixed bridges that involve little or no tooth preparation.
Patient preference
Where a tooth-supported fixed prosthesis is indicated and the abutments are generally sound, resin-retained bridges are preferred, whilst recognizing that patient choice may be a factor limiting their use.
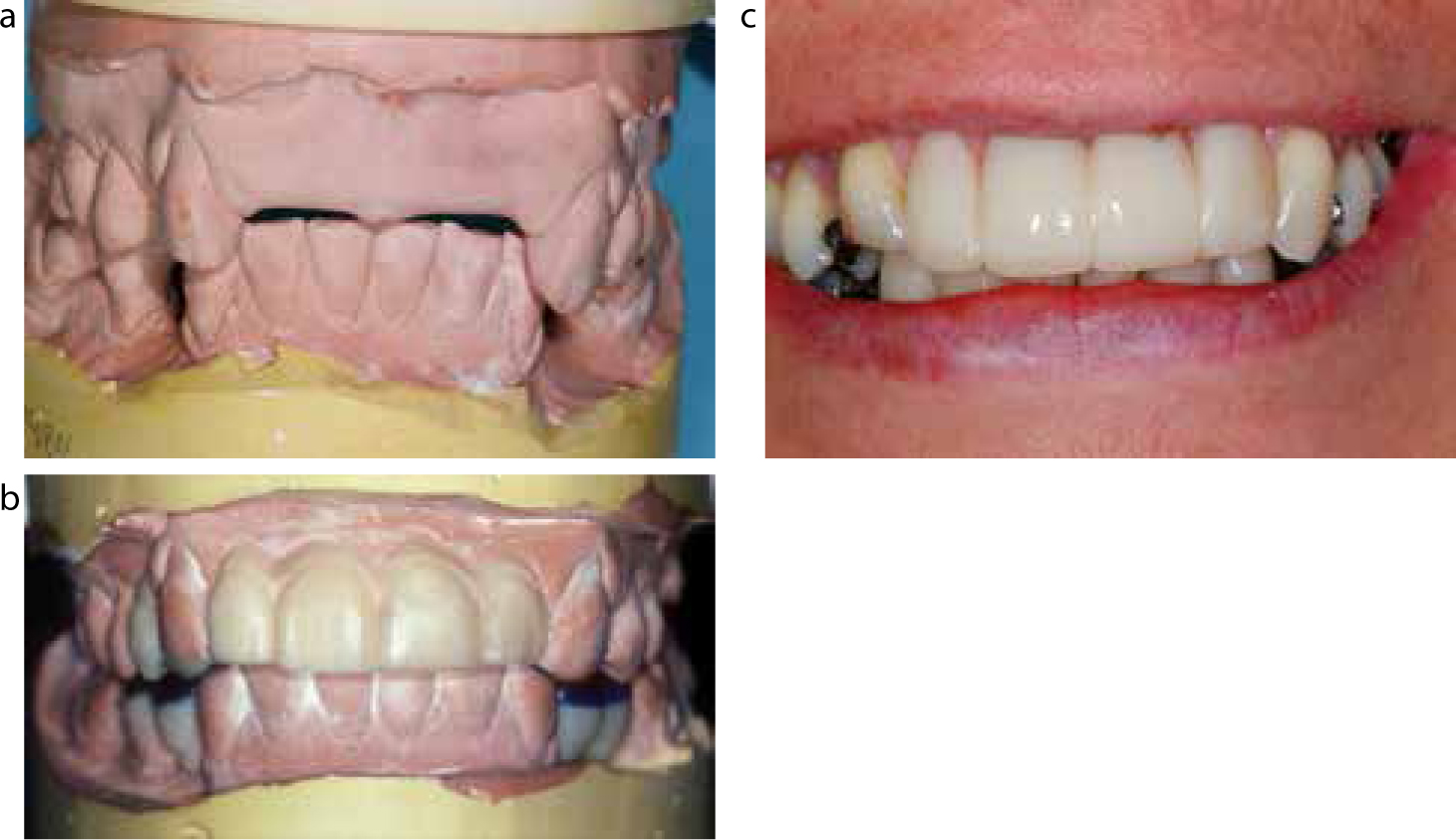
On very rare occasions, it may be necessary to use entirely sound teeth as the abutments for a fixed bridge retained by crowns, but this should be very much the exception rather than common practice. The patient whose anterior teeth are shown in Figure 1 had previous multiple episodes of peri-radicular surgery carried out on all four maxillary incisors over a number of years. The treatment had not been successful and the teeth were deemed too compromised and damaged to be retained. The most appropriate treatment from a dental perspective was the loss of the maxillary incisors, followed by the placement of two implants to retain a fixed prosthesis. However, the patient expressed a wish to avoid further surgery. With that in mind, the option of a resin-retained adhesive bridge was recommended, but the patient asked about the likelihood of debonding as she had a job that involved travelling overseas and public speaking and she was concerned about how she would manage if the prosthesis became loose or was lost, which is a potential complication. It was indicated that the only other alternative was a fixed bridge retained by full crowns and the disadvantages of this in terms of loss of tooth structure and damage to the abutment teeth long-term were explained. Nevertheless, as the risk of complete loss of cementation is improbable, she selected this option for treatment. The replacement of four missing incisors constitutes a relatively long span and control of loading is essential with a fixed-fixed design being indicated.
Figure 1. Palatal view showing four compromised maxillary incisors prior to their extraction.
The posterior occlusion was stable and the posterior dentition complete such that loading on the prospective prosthesis would be controlled.
Bridge designs of 20 or so years ago would often recommend the use of two abutments at each end of the span for longer span anterior bridges, as the pontics lie outside the inter-abutment axis and the use of double abutments was felt to ‘tie the bridge in’, minimizing the possibility of the entire prosthesis and abutments drifting anteriorly. This was the classical work of Brumfield, an engineer, who contributed a number of chapters in Tylman's Theory and Practice of Crown and Bridge Prosthodontics.1 However, an improved understanding of bio-mechanics and an appreciation of the undesirable aspects of double abutments have led to a single abutment at each end of the span being preferred. Double abutments create a fulcrum about the more mesial of the two abutments, with the more distal one being at increased risk of suffering a loss of cementation. Solitary abutments at each end of the span, with each having good crown height and appropriate retention and resistance form, will perform better than double abutments.
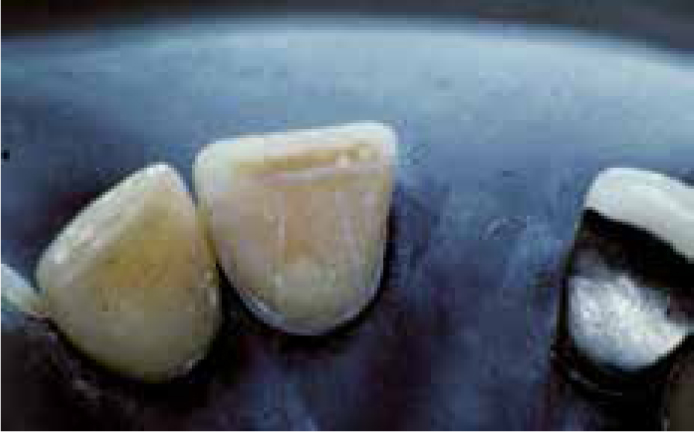
In this case, the maxillary canines were prepared to receive metal-ceramic retainers, with emphasis being placed on creating parallelism between the opposing axial surfaces. Where maxillary anterior teeth are prepared, maintaining appropriate form of the axial surface apical to the cingulum is of particular importance. As this wall is the shortest, it is frequently advisable to increase resistance form by decreasing the palato-labial rotational radius through the use of auxiliary preparation features in the form of axial grooves. The ideal location for these would be mesially and distally in the mid-proximal regions of the preparations. However, this location is better avoided as the tooth reduction is already significant to accommodate both the metal coping and the veneering porcelain. The position of the grooves is therefore best between the mid-proximal and mid-palatal regions of the preparations. The grooves are prepared parallel to the gingival half of the facial surface of the preparations and the two pairs of grooves in each preparation have a common path of withdrawal. These are prepared using a friction-grip 170 tungsten bur: more control and tactile feedback are available if a speed-increasing handpiece is used with an electric micro-motor or air motor rather than using a turbine. The preparations of the maxillary canines are shown in Figure 2. The palatal view of the fixed-fixed bridge following cementation is shown in Figure 3.
Figure 2.
(a, b) Preparation of maxillary canines as abutments for a fixed-fixed bridge to replace the maxillary incisors. Note the placement of axial grooves palato-proximally to increase resistance form.Figure 3. Palatal view of the completed fixed-fixed bridge replacing the four maxillary incisors retained by the maxillary canines.
The use of a fixed bridge with cemented crown retainers should be increasingly rare. The impact of the implant is significant whilst the continued development of the resin-retained bridge reduces both the need and the indications for tooth preparation. So rarely are ‘traditional’ fixed bridges used that consideration should be given to considering whether training in their preparation and provision is a postgraduate skill rather than one that should be taught as part of the undergraduate curriculum.
Planning fixed tooth replacement
Where fixed tooth replacement is planned, it should be part of the protocol to make study casts, mount these in a semi-adjustable articulator or one that is capable of receiving a face-bow transfer. The casts should then be waxed to give an indication of the final result (Figure 4). The information gained from this will alert the clinician to any intra-arch or opposing arch factors which may influence the outcome. It is also beneficial to be able to show the wax-up to the patient and should form part of the process of informed consent to treatment. The wax-up may also be used to create a silicone index which can be used to guide the preparations and construct the temporary bridge. A silicone index may also be used to construct at the chairside; a ‘dummy’ prosthesis using a bisacrylic temporary crown and bridge resin which can allow the patient to see the intra-oral effect of what is planned (Figure 5). Diagnostic waxing is frequently omitted in the provision of indirect restorations and this is commonly to the detriment of the tooth preparation and final result. The use of diagnostic waxing improves predictability of the outcome.
Figure 4. A diagnostic wax-up of a proposed bridge to replace a maxillary premolar and molar.Figure 5.
(a) Casts mounted in a semi-adjustable articulator. (b) Diagnostic wax-up of missing maxillary anterior teeth and right maxillary canine. (c) ‘Dummy’ prosthesis made using a silicone putty index of the wax-up and formed using bis-acrylic temporary resin directly in the mouth.
Tooth-supported fixed prostheses involving little of no tooth preparation
The development of resin-retained bridges,2 since their first description in 1977, has been one of steady progress. The resin-retained bridge offers a conservative, economical and relatively durable option for the replacement of missing teeth. The evidence indicates that they are most successful when used to replace a missing anterior tooth when the span is short, employing a cantilever design of one abutment with one pontic.3,4,5 Such a design places least demands on the operator and the technician. Resin-retained bridges used to replace multiple teeth and employing longer spans require great attention to detail, both clinically and in the laboratory, with a good understanding of the bio-mechanics of fixed bridge provision.
The resin-retained bridge requires sound but not necessarily unrestored abutment teeth. The presence of existing restorations is not a contra-indication but any restorations should be of composite resin that has been relatively recently placed in order to ensure adhesion to the restorative material on cementation of the bridge.6 Composite resin that has been present in the mouth for some time undergoes water sorption and the bond strength of composite luting agents to old composite restorations will be lower. However, it has been shown that the presence of restorations in the abutment teeth is associated with a decrease in success rate.4
Resin-retained bridges have traditionally been constructed in cast nickel-chrome alloys: increasingly, alloys of chrome-cobalt are being used as a consequence of concerns over toxicity from the dust associated with grinding nickel-chromium alloys. A further factor driving the move towards chrome-cobalt is its ability to be milled as part of CAD-CAM fabrication of restorations. Nevertheless, the milled chrome-cobalt fitting surface is considerably smoother than a cast surface and is not as responsive to sandblasting, a necessary part of the preparation for cementation. The impact of these factors on bond strengths with surface-active composite luting agents is at present unknown.
Metal frameworks veneered with porcelain represent the most appropriate materials for resin-retained bridge construction, despite occasional limitations on the aesthetics produced by the metal retainers. There continue to be reports of the use of newer ceramic materials for constructing resin-retained bridges. Whilst leucite-reinforced porcelain provides a material with improved physical properties, the thickness of the retainers and the strength of the connectors are significant limiting factors. Figure 6 shows such an all-porcelain resin-retained bridge used to replace a missing maxillary canine in a young patient: however, the connector fractured soon after the bridge was fitted (Figure 7). It is noted that high success rates have been reported for zirconia frameworks used to provide resin-retained bridges7 and this may represent a possible avenue for development.
Figure 6.
(a) Anterior view of a one unit space mesial to the maxillary left canine. (b) Anterior view following cementation of a cantilever leucite reinforced adhesive bridge UL3 area.Figure 7. Anterior view of a the failed leucite reinforced cantilever resin-retained bridge following fracture through the connector mesial to UL3.
Principles of design
The design should be as simple as possible and should follow the principles outlined earlier in Part 1 of this paper. The framework should:
Cover as much of the abutment tooth or teeth as possible;
Be rigid;
Permit control of the occlusal contacts.
These are the same principles which apply to any type of fixed bridge.
Area of coverage of the abutments
Tooth preparation
At the time of the introduction of the Maryland Bridge, the concept of 180 degrees of axial surface coverage for posterior teeth was introduced. It is difficult to find the precise rationale for this but it was probably based on seeking to cover as much of the abutment as possible without significantly compromising the appearance of the tooth or interfering with the patient's mandibular closure into his/her intercuspal position. Simonsen, Thompson and Barrack8 were amongst the first to describe detailed principles of framework design and tooth preparation as being of benefit to facilitate axial and functional surface coverage by the framework. Grooves, rest seats and the creation of finish lines for their preparations of both anterior and posterior teeth were recommended. Most of these preparation features were designed not only to facilitate retention of the framework, but also to improve resistance form and also had the benefit of increasing rigidity in the framework. Figure 8 shows a posterior resin-retained bridge which follows these principles, whilst Figure 9 shows a maxillary central incisor to be employed at the abutment for a cantilever resin-retained bridge, where a rest seat has been prepared in the cingulum, a fine chamfer finishing line created and mesial and distal axial grooves placed. However, there never has been any clearly demonstrated benefit in tooth preparation and the advantages of little or no removal of tooth structure outweigh any of the theoretical benefits of tooth preparation. Despite the disadvantages of tooth preparation, some modification of the proximal surfaces of abutment teeth is frequently required to move the survey line further apically and facilitate the creation of connectors which have sufficient height to provide adequate resistance to torsion and bending. This is more the case when fixed-fixed designs are used but may also be needed for cantilevers to facilitate both connector height and the path of insertion of the prosthesis. Tooth preparation may also be necessary to create occlusal rest seats (Figure 10), which will provide resistance to apical displacement and flexure of the framework for a resin-retained bridge in the posterior part of the mouth. In order to act effectively, the rest seats should be adjacent to the pontic area. More recently available evidence suggests that preparation of the abutments for a resin-retained bridge is associated with an increased risk of failure.4
Figure 8.
(a) Occlusal view of a fixed-fixed resin-retained bridge circa 1983 following design principles described by Simonsen, Thompson and Barrack. (b) Lingual view of a fixed-fixed resin-retained bridge circa 1983 following design principles described by Simonsen, Thompson and Barrack.Figure 9. Palatal view of a maxillary central incisor prepared to receive a resin-retained cantilever bridge circa 1983 following design principles described by Simonsen, Thompson and Barrack.Figure 10. Rest seat prepared in a maxillary second premolar: the abutment for a resin-retained bridge.
Clinical crown height
The area of coverage will also be influenced by the available clinical crown height. Resin-retained bridges are not immediately suitable when this is in short supply as it clearly limits the enamel available for bonding and the height of the connectors. This contra-indication may be altered by pre-operative surgical crown lengthening. As a guide for maxillary anterior teeth, the vertical wall apical to the cingulum should be available for coverage by the retainer. Extension of the framework onto the approximal surface that will be adjacent to the pontic is also a pre-requisite as it will allow the appropriate dimensions to be established for the connector and also provide a degree of resistance form. There is also frequently the opportunity to extend the framework onto the incisal edge of maxillary anterior teeth without major detriment to the aesthetics of the final result (Figure 11). The metal is angled palatally, which minimizes visibility from a direct anterior view. The framework should also be extended as far into the embrasure away from that adjacent to the pontic as can be achieved without tooth preparation. Increased coverage of the abutment by the retainer provides improved security for the prosthesis.3
Figure 11.
(a) Palatal view of a fixed-fixed resin-retained bridge showing maximal coverage of the abutments. (b) Labial view of the resin-retained bridge replacing the maxillary central incisors.
Thickness of retainers
It is generally considered that the thickness of an adhesive retainer should be a minimum 0.7 mm, which appears able to give good rigidity when a nickel-chrome or chrome cobalt framework is employed. Longer spans with consequently greater demands on the retainers require an increased thickness of metal coverage of the abutments. Previously, accommodating retainers of these thicknesses without interfering with the patient's closure into his/her intercuspal position was frequently not possible. However, the use of relative axial tooth movement9 has facilitated the use of these more robust and rigid frameworks. It has also encouraged more extensive coverage of the abutment with the metal framework, as increased area of coverage provides greater security for the prosthesis. This is associated with increased survival of the prostheses.3
Designs of resin-retained bridges
Designs of resin-retained bridges are:
Cantilever;
Fixed-fixed;
Hybrid.
Cantilevers
These are the simplest design and are indicated when replacing a single missing anterior tooth when the span is short (Figure 12) and are the design of choice in this situation. However, cantilevers are increasingly being employed in the replacement of missing posterior teeth.
Figure 12.
(a) Occlusal view of a cantilever resin-retained bridge replacing a maxillary lateral incisor using the adjacent canine as the abutment. (b) Palatal view of two separate resin-retained bridges replacing the maxillary lateral incisors using the central incisors as abutments.
Cantilevers are, from an engineering perspective, mechanically unsound but they perform well as resin-retained bridges in the anterior region because the abutment is either unrestored or only lightly restored. Neverthless, the framework should cover as much of the palatal or lingual surface of the abutment as possible and be extended onto the approximal surface to provide connector height and perhaps some resistance form. Where possible, the closure contact and the excursive contacts should be maintained on the retainer. The risk of failure is increased when the intercuspal contact lies at or close to the junction between the framework and the tooth. The occlusal scheme should provide intercuspal contacts on the retainer and the pontic but, in excursive movements, the pontic should be free of contact with the antagonist teeth.
The situation in the posterior part of the mouth is different, as loading of the teeth is greater than anteriorly. There is an increasing trend to extrapolate the finding that the cantilever performs the best of all resin-retained bridge designs by extending its application to the posterior part of the mouth (Figure 13). There may be justification for this where a small tooth is cantilevered from a larger one, such as a single premolar which uses a molar as the abutment. However, employing such designs for replacing a missing molar using another molar as the abutment seem unwise as the loads will be relatively high, which may result in adverse effects on the prosthesis or the abutment. Resin-retained bridges benefit from maximal coverage of the abutment with the metal framework, and cantilevered units place more demands on the retention and resistance form provided by the abutment. There is a lack of clinical data reporting the performance of posterior cantilever resin-retained bridges: the small amount of recent work published comes from Botelho et al.10 Their work indicates that short span posterior resin-retained bridges can be successful but the success rate is lower than in the anterior region.
Figure 13.
(a) Two cantilever resin-retained bridges replacing missing maxillary first premolars. Note the anterior resin-retained bridges are of fixed-fixed design to provide post-orthodontic retention (courtesy of Miss K E Harley). (b) Labial view of the resin-retained bridges replacing the maxillary lateral incisors and first premolars (courtesy of Miss K E Harley).
The use of a distal facing resin-retained cantilever has gained some popularity and its use may be justified if its provision avoids the need for a free-end saddle removable partial denture.11 However, these bridges carry a higher risk of failure of which both the operator and patient should be aware. Furthermore, there can be little indication for adjacent pontics where one is a distal-facing cantilever and the other a mesial-facing cantilever. In this instance, a fixed-fixed design, whilst demanding excellent coverage of the abutments and good rigidity in the framework, remains the design of choice.
Fixed-fixed designs
The indications for a resin-retained bridge supported by abutments at each end of the span are no different from those where crowns are used as the retainers. These are employed for longer spans and, on occasions, when permanent retention is required, the latter occurs most frequently after orthodontic treatment, particularly for patients affected by hypodontia where tooth replacement is required (Figure 14). For example, where space has been created for a maxillary lateral incisor, there is the risk that the approximal contact between the lateral incisor pontic and the central incisor may be insufficient to maintain the position of the canine used as the single abutment. This can allow movement of the canine with the pontic ‘slipping’ its approximal contact (Figure 15). The fixed-fixed resin-retained bridge presents greater difficulties because the retainers cover only part of the abutment teeth. Data indicate that one significant factor in outcomes is the amount of coverage of the abutments.3
Figure 14. A fixed-fixed resin-retained bridge for the replacement of a missing maxillary lateral incisor where post-orthodontic fixed retention was required.Figure 15. Occlusal view of a resin-retained bridge replacing a maxillary lateral incisor in a younger patient who had received orthodontic treatment. The approximal contact between the pontic and central incisor was insufficient to maintain the position of the teeth.
The important principle for fixed-fixed resin-retained bridges is that the framework should have good rigidity: this means a minimum thickness of 0.7 mm in non-precious metal, whilst there must be adequate crown height to provide good coverage of the axial surfaces. The management of the occlusal contacts is a further essential requirement.
There are parallels to be drawn with the now rarely used fixed bridge retained by cemented partial veneer crowns. These were described by Smyd in the early 1950s.12 It was stated that rigid frameworks were essential and the occlusal contacts on the elements of the fixed bridge must be controlled. The greatest risk for an otherwise mechanically sound fixed-fixed bridge is the abutment tooth being pushed out of the framework and becoming uncemented, either by contacts on mandibular closure or tooth-to-tooth contacts on excursive movements of the mandible. Figure 16 shows an old example of a fixed-fixed resin-retained bridge using perforated retainers from the early 1980s, which illustrates this point. The nature of the occlusal contacts with little overjet and a deep overbite restricted the thickness of the framework and limited its rigidity. In order to accommodate closure into the intercuspal position, the area of coverage by the framework has been compromised. Lastly and significantly, the lack of coverage allows the canine antagonist to move readily and frequently from the framework onto the abutment tooth. This eventually fatigues the bond of the framework to the tooth as it is repeatedly stressed, leading to a loss of cementation. The benefits of increased occlusal coverage are greater security for the retainers,3 and this is not difficult to achieve for anterior bridgework. However, there may be some significant compromise to aesthetics where extensive occlusal coverage is employed and this is increasingly likely in the mandibular arch.
Figure 16.
(a) Facial view in the intercuspal position showing deep overbite and minimal overjet. (b) An inadequate perforated Rochette bridge (circa 1980) replacing the maxillary lateral incisor and of fixed-fixed design.
Figure 17 shows an appropriately designed framework for an anterior fixed-fixed resin-retained bridge replacing three maxillary incisors. There is extensive coverage of the abutment teeth from the axial wall apical to the cingula extending almost onto the incisal edges. The framework is extended into the pontic areas to provide increased resistance and permit good height in the connectors: further coverage has been achieved by extending the framework onto the distal surface of UR3 and UL2. The only tooth preparation was minor modification of the mesial of UR3 and UL2 to create guide planes, which facilitated the connector height. The framework is 0.7 mm thick in a nickel-chrome alloy. Placement of the bridge prevents full mandibular closure but relative axial tooth movement, both of the bridge and its antagonists and the posterior teeth, will predictably re-establish full intercuspal contact within weeks or months. An example of a posterior fixed-fixed bridge replacing two maxillary premolars is shown in Figure 18. This demonstrates partial coverage of the occlusal surface of the maxillary molar to give increased security.
Figure 17. An appropriate design for a fixed-fixed resin-retained bridge replacing three maxillary incisors. Note the extent of the coverage of the abutment teeth.Figure 18. A posterior fixed-fixed resin-retained bridge replacing two maxillary premolars. (More coverage might have been beneficial for the molar tooth).
Fixed-fixed resin-retained bridges usually require some degree of tooth preparation of the axial surfaces adjacent to the pontic area in order to move the survey line further apically to allow greater coverage of the axial surfaces and sufficient connector height to provide a more rigid framework.
Hybrid designs
The situation is sometimes encountered where one abutment is sound or is lightly restored but the second abutment requires a crown or already has one. It is an attractive option to combine a crown as one retainer and an adhesive retainer for the relatively unrestored tooth. However, it is important that appropriate principles are employed in its design with an awareness that these hybrid designs may have higher failure rates.3 All the data indicate that loss of retention is more likely with an adhesive retainer rather than one that is a cemented crown. It is therefore an important requirement that the resin-bonded retainer should be retrievable without having to sacrifice the entire prosthesis. This means that a hybrid bridge of this type must incorporate a movable connector to allow retrieval of the adhesive component. There is a further consideration, which is the position and function of the movable connector. In a fixed-movable bridge using cemented crowns as the retainers, the movable connector should be housed in the distal of the minor abutment (the more anterior tooth). Furthermore, the female should be part of the more anterior retainer with the male component in the mesial of the pontic. This is to ensure that the movable connector is fully seated under axial loading. As a consequence, the most appropriate type of hybrid bridge is where the tooth with a crown retainer is the more anterior, with the resin-bonded retainer attached to the more distal tooth. This also allows the movable connector to be housed within the normal contour of the crown on the minor abutment.
Figure 19 shows a resin-retained bridge replacing a maxillary first premolar which then failed and was lost. There was already a crown on the maxillary canine which required replacement on aesthetic grounds. In the new prosthesis shown in Figure 20, a hybrid design was chosen: the retainer at UL3 contains the female component of the movable connector in its distal surface. The resin-bonded major retainer with extensive occlusal coverage is placed on the maxillary second premolar and the male-component of the movable connector is in the mesial of the pontic. The position of the movable connector and the location of the male and female components are clearly shown and will result in axial loading seating the components fully. The resin-bonded retainer on the maxillary second premolar has extensive occlusal coverage to provide increased security. It can be seen from the buccal view of the bridge (Figure 21) that there is no display of metal.
Figure 19. Occlusal view showing absence of the maxillary first premolar: the previous cantilever resin-retained bridge had been lost and the crown on the canine required replacement on aesthetic grounds.Figure 20. Occlusal view of the hybrid design employed. The crown is the minor retainer and the adhesive retainer, the major.Figure 21. Buccal view of the completed hybrid bridge replacing the maxillary left first premolar.
Cementation
Cementation of a fixed bridge is an important part of the clinical procedure and it is frequently not given the attention that it deserves. In respect of resin-retained bridgework, the cementation procedure is a critical part of the procedure of providing a bridge: the clinical stages are demanding for both the operator and the dental nurse. Therefore a description of the procedure is included.
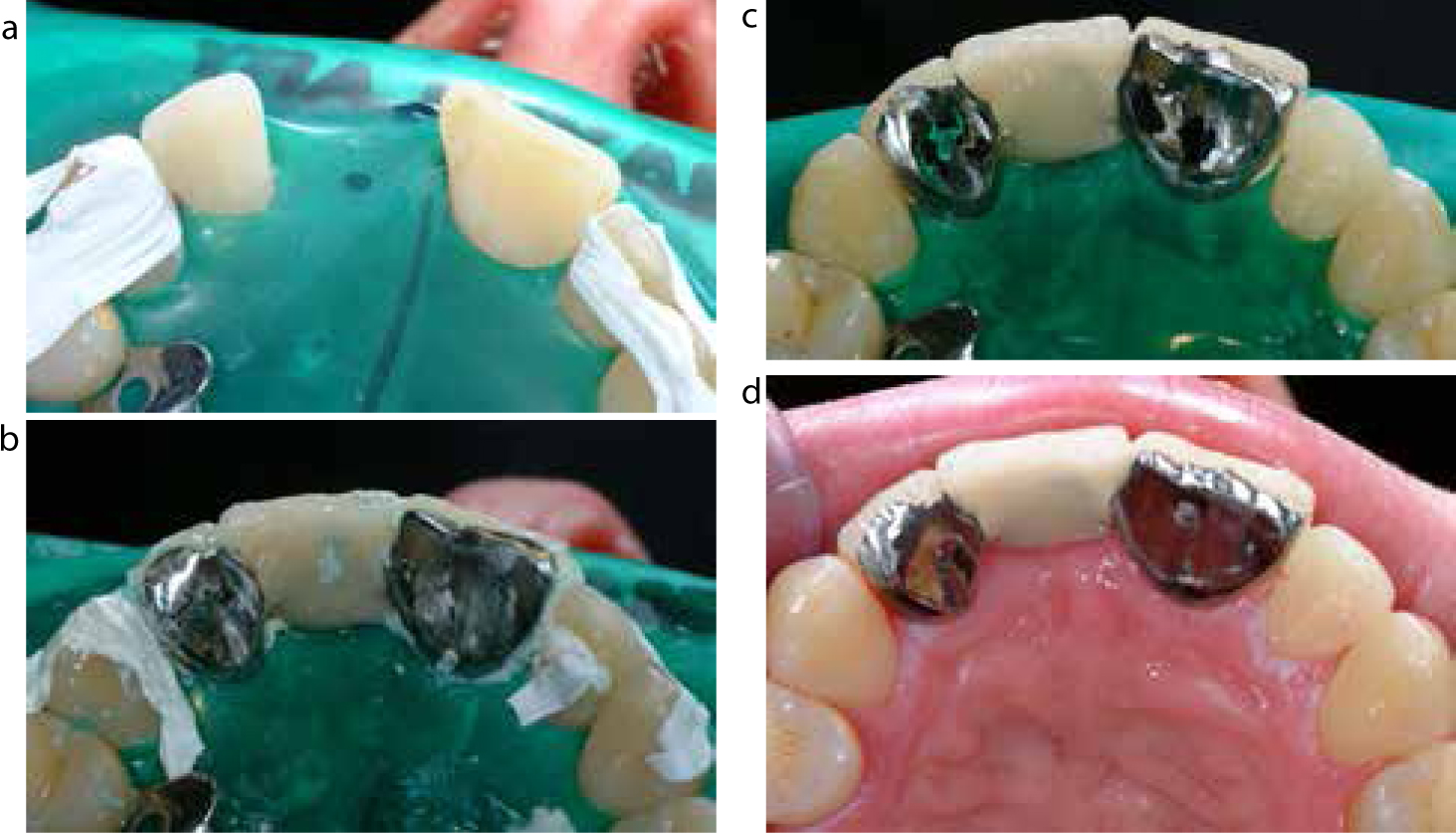
Frameworks for resin-retained bridges need not only demonstrate good marginal fit but must also be well-adapted to the abutments. Even without tooth preparation, the retainers should locate easily and positively on the abutments. If this is not the case at try-in, it is likely that the framework is not well adapted. This in turn will result in an increased thickness of the composite resin-luting cement. Increased film thicknesses will give lower bond strengths. Cementation is a clinically demanding procedure; not only must the framework fit and adapt well, but it must be accompanied by a careful cementation procedure. Rubber dam isolation, while apparently frequently ignored, gives control of the operating field and also, importantly, control of the excess cement when the bridge is seated (Figure 22). The framework should be freshly sandblasted with 50 micron alumina and steam cleaned prior to cementation. This should ideally take place immediately prior to cementation: if it is delayed by 24 hours, as much as 40% of the bond strength can be lost due to excessive build-up of oxide on the fitting surface of the non-precious alloy.13 The abutment or abutments must be carefully isolated from the adjacent teeth; the use of PTFE tape for this purpose is advantageous. Clearly, the manufacturer's instruction for the composite resin-luting cement should be followed and, after loading the retainer(s) with cement, the bridge should be seated and held firmly in position. Whilst access at this point can be limited, if the dental nurse is able to use a disposable brush or sponge to clear as much excess cement as is possible, this will speed the post-cementation clean up. If the cement is dual cure, the cement should be exposed to light, where possible, although the operator's fingers frequently limit access. If an oxygen-excluder is provided by the manufacturer, this should be applied over all exposed margins of the retainers with the bridge held firmly in place against the abutments until it has cured. Once cured, wash away the oxygen excluder, if supplied, and then, if possible, leave the bridge for a further few minutes to ensure that the cement is fully cured. Minimal finishing should be carried out post-cementation as there are stresses within the composite cement film and at the interfaces between the cement and tooth and the cement and retainer. The safest way to remove excess cement is to fracture it away carefully using a sickle scaler held parallel to the margin. Rotary finishing at this appointment should be avoided, if possible, as any heating is likely to damage the bond and has been known to cause the cement lute to fail immediately. Additional finishing, if necessary, should be delayed by at least 24 hours to allow some water sorption by the cement which, in turn, reduces the stresses: rotary finishing procedures should include the use of water spray to minimize heat production.
Figure 22.
(a) Rubber dam isolation prior to cementation of a maxillary resin-retained bridge. (b) Immediately following cementation showing excess cement controlled by the rubber dam. (c) Bridge following careful removal of excess cement with hand instruments. (d) The bridge at the end of the cementation procedure.
The occlusion should be checked prior to discharging the patient, together with instruction and rehearsal on how to clean the retainers and beneath the pontic. If relative axial tooth movement is being employed to accommodate the thickness of the retainers, advise patients that they are likely to be a little uncomfortable occlusally for a couple of days and after that they should notice little, apart from the fact that their other teeth will not contact properly. Very few patients have difficulty in adapting to this occlusal disturbance and, over time, in the vast majority of patients, full occlusion is re-established.
Conclusions
Fixed tooth replacement using teeth as abutments remains an important element of fixed prosthodontics. However, the need for bridges using crowns as the retainers has diminished due to the reduction in dental disease, the use of dental implants and the continued development and performance of resin-retained bridges. Designs of tooth-supported fixed prostheses have changed as a result of continuing improvements in the understanding of bio-mechanics and the slow accumulation of useful clinical data on outcomes. Bridge designs have simplified, but a sound appreciation of the requirements underpinning their use is still required. The resin-retained bridge should be the type of prosthesis considered first when a tooth-supported replacement is necessary. Whilst their mode of attachment to the teeth is different from those bridges retained by crowns, there is commonality in the principles upon which their use is based.