Shah NP, Katsarelis H, Pazianas M, Dhariwal DK. Periodontal disease, dental implants, extractions and medications related to osteonecrosis of the jaws. Dent Update. 2015; 42:878-889
Sidhu HK. Denosumab, an alternative to bisphosphonates but also associated with osteonecrosis of the jaw – what is the risk?. Dent Update. 2015; 42:436-440
Personal Communication, Dental Protection. 2016;
Pemberton MN. Developing patient safety in dentistry. Br Dent J. 2014; 217:335-337
Taking a comprehensive medical history is a prerequisite for treating every patient. This paper will explore the current requirements and suggest how computerized practices might efficiently achieve them. It is suggested that practices consider their patient journey and information flow and a medical history form is presented which should facilitate the process. Audit and monitoring provide a means for continual improvements.
CPD/Clinical Relevance: Improving the process of taking and recording medical histories will save clinical time and improve patient safety.
Article
Taking a comprehensive medical history (MH) is a prerequisite for treating every patient, yet many medical history forms (MHF) and the processes used in practices may be outdated. In a busy dental practice it can be challenging to find the time to discuss and record a MH thoroughly, but obviously any errors or omissions could have potentially serious consequences,1,2 The relevance of particular medical conditions to dentistry are covered in detail in a recent paper and therefore will not be discussed further here.3 Confidentiality is an absolute requirement throughout the MH process but is outside the scope of this paper; obviously indiscreet discussion of medical details should be avoided. This paper will focus on the current requirements and consider the process and practicalities of taking a MH in a busy computerized practice.
Current requirements
The GDC states that ‘You must make and keep complete and accurate patient records, including an up-to-date medical history, each time that you treat patients’.4
The CQC states that you must carry out… ’An assessment of the patient which must include a current or updated medical history’.5
The Faculty of General Dental Practitioners guidance is specifically cited by the CQC. It says that ‘…the medical history must be recorded and updated as necessary…a clinician should work through the questionnaire in collaboration with the patient… Once complete, the form should be signed and dated by the patient and clinician unless the software does not permit this…’6
Dental Protection says that ‘… it is good policy to take a full medical history every time a patient is examined and the use of a medical history form provides an excellent way of recording this information. It is important, however, that the patient is not left to complete the medical history form; whoever is carrying out the examination should go through all the questions with the patient to ensure they fully understand them’7
The information flow
Traditionally, a MH has often been taken verbally by the clinician, with little or no involvement of other members of staff. Whilst simple and effective, this is particularly time consuming and probably no longer realistic in modern general practice. In computerized practices, taking a MH now usually involves multiple members of the dental team. Practice-wide software allows for delegation, but each member of staff must perform his/her role well to avoid either omissions (errors) or duplication (time wasted so less efficient).
For example, patients may update their contact details on the MHF. At some point in the practice's process, the contact details must be checked against that which is recorded in the software and amended. It may be that this is done by the dental nurse or by the receptionist, but if not done, perhaps because each assumes the other has, then the new data will be missed.
In order to consider how best to organize the MH process, it can be helpful to consider how the information flows through the practice. The flow of data from patient to practice will vary, but is often similar to the following outline. The receptionist will generally identify who requires a MHF. The MHF is given to patients to complete in the waiting room when they arrive for their appointments. When called through into the surgery, the form comes with the patient and the clinician transfers the information to his/her dental software, in discussion with the patient. The form is then taken back to reception to be scanned to the software file then shredded.
Reception
The receptionist is usually the person to give the paper MHF to the patient on a clipboard. The receptionist should consider: can this patient understand and complete this form? Can he/she read? Can he/she read this size of print? Does he/she understand written English, or would he/she prefer another language? Should a parent or carer complete it instead? Common sense, courtesy, experience and training all have their role in helping a busy receptionist quickly and tactfully ask the right questions and provide solutions. For example, a large-print, two-page version of the MHF should be available, and the receptionist should make this available to those who require it. Multiple language MHFs are available8 and the digital copies should be kept on the reception computers, for printing as and when required. Although these are a different format (see below), ensuring that the patient understands the basic questions is paramount.
A receptionist may identify those patients who should fill out a new paper MHF. During their conversations with patients they may pick out key details, such as a change of address or recent serious illness. They also should check each patient's file to see when the last paper MHF was done (time interval discussed later). Good team communication and training are essential to avoid a clinician having to wait for a patient to fill out the MHF.
The receptionist is usually responsible for scanning the MHF to the patient's software file. Training should be considered to ensure efficiency in time and digital memory: full colour, high resolution scans are unnecessary! The paper MHF needs either storage or safe disposal, usually shredding. Data protection guidelines need consideration but are beyond the scope of this paper.
Medical history form
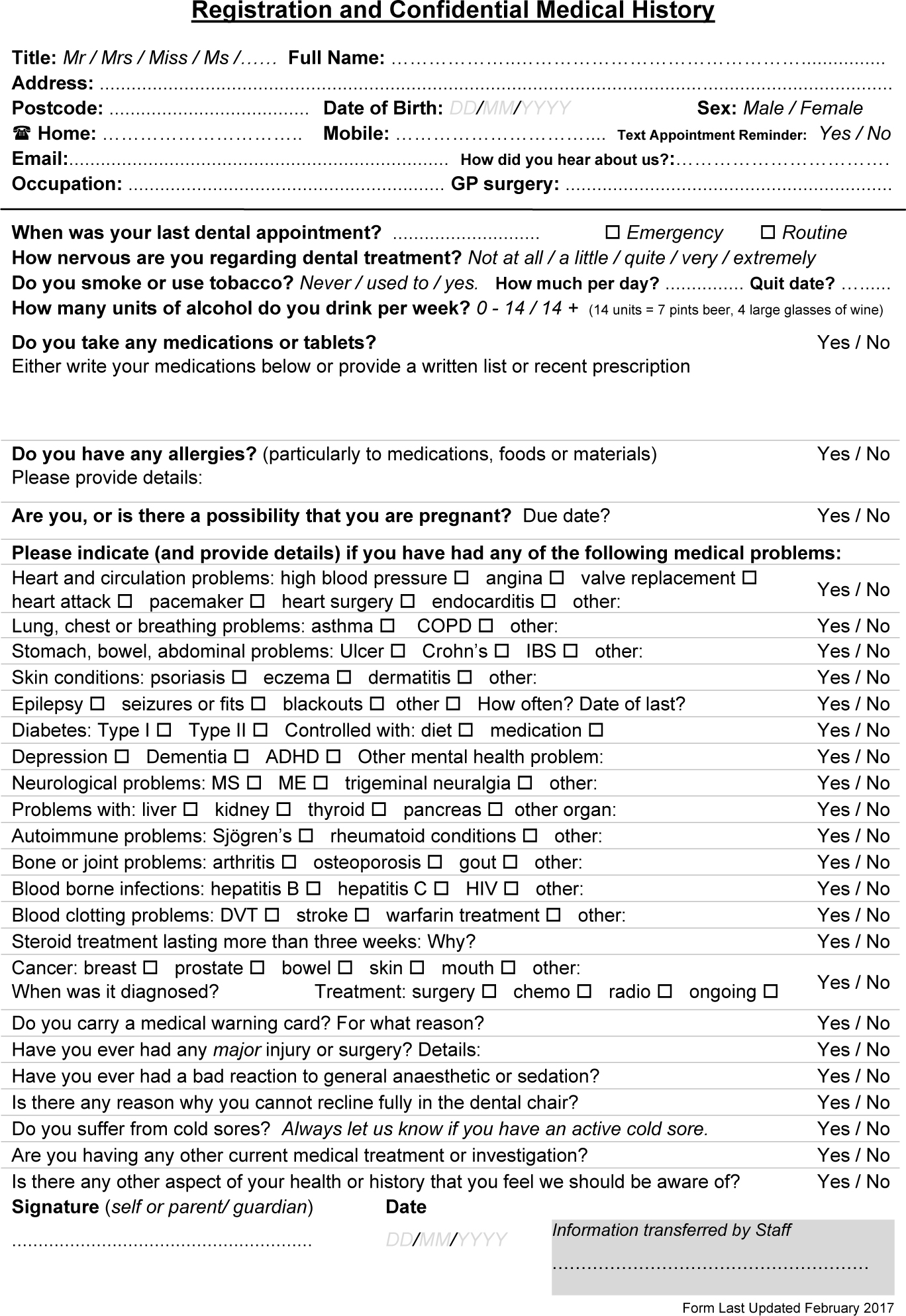
Several model MHFs are in common usage but it could be argued that many of the questions in these forms are obsolete or irrelevant. For example, a form has been suggested that does not specifically ask about a history of cancer,9 which is surely universally regarded as relevant information.10 A new form (Figure 1) is suggested which aims to question the patient in a systematic way and is designed to optimize the information flow. Many practitioners will have their own opinions regarding the suggested form, perhaps additions or alterations; but no single form is ‘correct’ or will appease everyone. It is suggested that this MHF is a starting point which can be modified according to the requirements of each practice.
Figure 1. This medical history form is available from the author in a format which can be edited to allow easy adaptation, ie inclusion of your logo. (Email: richard@gwynnedental.co.uk)
Regarding the overall design of the MHF, brevity is essential in order to keep the form on a single A4 page to improve logistics. Paper, printing, storing, scanning, digital memory and shredding all take time and money; if two pages are required, then obviously the administrative burden increases. Most computerized practices use office printers and scanners which are not designed for speed or large volumes, so scanning alone can engage a receptionist for long periods.
The font size, handwriting spaces and number of questions have to be carefully balanced in order to enable most people to read and write on the form comfortably, yet sufficiently question the MH. Font sizes 10 to 12 are recommended, which are fairly standard in business and of a size most individuals can comfortably read.11 More space could be given for handwriting, eg for medications, but usually, if more than a few are listed, a patient will give a copy of a prescription. Consider the size of the clipboard clip upon which the MHF will be given to the patient: check the writing is clear of the area covered.
The MHF is commonly used in practice to obtain and update a patient's contact details, so these are included at the top of the form. Whilst a separate contact detail and medical form could be designed, and might be preferred in some practices, most prefer to use a single combined form. The title includes ‘registration’ to reflect this dual purpose.
Tobacco and alcohol use are necessary social history components and are included. Most model MHF ask numerically how many units of alcohol are consumed each week. However, the precise number is not important; the question is intended to identify those individuals for whom advice would be appropriate. The latest Government guidelines suggest a weekly limit of 14 units per week for both men and women, hence this is the threshold we should use.12 The recommended question simply asks whether the weekly alcohol intake is above or below this threshold; the former should trigger appropriate advice.
Some practitioners may question some of the implications and categorizations of the questions. For example, it may be felt that ME (also known as Chronic Fatigue Syndrome) is a psychiatric not physical condition. As it is considered by most sufferers and support groups to be physical, it seems reasonable loosely to classify it as a neurological condition.13 It is not the purpose of the MHF to debate controversies. As it stands, the form will generally be understood by patients and most conditions are identified by an appropriate question.
The question regarding cold sores is worthy of specific mention as few patients tend to advise before an appointment that they have an active lesion. Adding the text ‘Always let us know if you have an active cold sore’ has been a reasonably successful patient education tool, even though the actual yes or no response to the question is of limited value.
Discussion
The taking of a MH is not the completion of a paper form by the patient. The signature of the patient does not absolve the responsibility of the dentist or staff to check that the patient understood and correctly filled out the MHF. The MH, as envisaged by the official guidance, is the process. There is no requirement actually to have a MHF at all; the form merely provides a framework for the discussion with the patient.
FGDP and Dental Protection suggest that the dentist should ‘work through the form with the patient’. This need not imply that we stand over patients whilst they fill it out as it would render the form irrelevant and would take far too much time in surgery. The wording of the guidance should be interpreted more practically to suggest that a discussion needs to take place during which the answers on the form are considered and the patient's comprehension checked. This, in turn, can provide an opportunity to pick out specific issues raised on the form. An example is asthma, which is commonly ticked but without further written details. Further questioning is required to elucidate the severity.
The MH discussion must take place between a trained staff member and the patient. Usually, this would be the clinician (assisted by a nurse) and the patient, once they have entered the surgery for their examination or treatment. This is when the medical history is actually taken and recorded. Many MHFs will be incomplete or have irrelevant information. For example, a patient may have forgotten that he/she takes a medication – but the fact that they ticked the box for a condition should trigger a question from the clinician.
A common problematic example is bisphosphonates and similar medications. The use of these are well known to have long-term potential side-effects,14 (Figure 2) so it may seem appropriate to have a specific question and yet the form in Figure 1 purposefully does not.
Figure 2. Spontaneous bisphosphonate-related osteonecrosis of the lower left lingual mandible.
Firstly, wording a specific question is difficult, as few patients know that they have taken ‘bisphosphonate’ by that name or what it is for, and there are new different drugs being introduced with similar side-effects.15 Secondly, tablet forms like alendronic acid are taken weekly, so are often forgotten when listing otherwise daily medication. Thirdly, the lengthy half-life of these drugs and increasing cancer survival rates means that a patient in future may have had a single infusion of a potent bisphosphonate decades ago which still has significance. If a specific question on the form is marked as ‘no’ then we may be tempted to assume that it is correct: however, for the above reasons the author believes that the only way to check for bisphosphonates reliably is to watch for ‘red flags’, such as osteoporosis or cancer treatment, and to question the patient in detail.
Exploring the information given by the patients is essential to clarify exactly what they mean and therefore the impact upon treatment. For example, patients may declare that they are ‘allergic’ to local anaesthetic (LA). In the vast majority of cases, this reflects a reaction to the adrenaline vasoconstrictor and not a true allergy, and careful questioning can determine the precise nature of the issue. Appropriate precautions might vary from simply noting to be careful with LA technique (a single incident of probable intra-vascular injection), ensuring the use of non-adrenaline LA (notable side-effects such as tremors or heart palpitations), or complete avoidance for a true allergic reaction to a component of the LA (rash, skin test result).
Recording
Software such as Exact (Software of Excellence) or R4 (Kodak) includes an easily accessible MH page which should be used as the day-to-day reference. The format of the questions in this software MHF should be updated to reflect accurately the paper version, facilitating efficient information transfer by avoiding ‘hunting’ for the correct question. Usually, a separate notes section can be filled out with particular highlights such as ASA status of the patient.3
It should be remembered that more information is not always better. Irrelevant information should not be transferred into the software MHF as it creates clutter and makes it harder to see the important information quickly. This is especially relevant when using software that prevents deletions from the medical notes, as unnecessary data cannot then be removed. For example, the clinician will want to avoid having to search for ‘takes warfarin’ amongst commentary such as ‘hospitalized age 5 for tonsillectomy’ for an octogenarian. Some practices have a process where receptionists transfer the MHF from paper to software – but they are unlikely to be qualified to decide what is relevant and they may not be in a position to discuss details easily with the patient.
Ensuring that the information is transferred correctly from paper to software is a crucial step so, at the bottom of the form is a greyed box for the initials of the staff member who transferred the information. This would usually be the person typing the software MHF, typically the dental nurse, or the dentist who has overall responsibility. Exactly who does what will depend on how the particular dental team works and what user information the software records, but incorporating a means of tracing the responsible individual should encourage accuracy and accountability.
What and when
The guidelines are unequivocal: a MH must be checked each and every time we see a patient. However, the process may differ, depending on circumstances. It is obvious and reasonable that, for a new patient, or where a patient reports substantial changes, a MHF and discussion should take place.
For routine patients, how often should a new MHF be done? Many practices suggest that a paper MHF should be done by every patient at every examination, sometimes with apparent reference to the CQC or other authority. It can be argued that this is inaccurate (who demands this? See ‘Current requirements’) and counter-productive, as it is unlikely to increase data accuracy and may reduce patient co-operation, increasing the risk of errors.
Although new paper MHFs are useful as an overview, a downside is that previous errors and irrelevant information may have to be sifted through again. Also, if patients are asked to fill out a form repeatedly, they are likely to become irritated. They will often refuse – ‘I did one last time!’ or may only partly complete the form as they think we already have the information.
A better approach, suggested by the FGDP6 is that, at every routine examination, the clinician should verbally check with the patient what is recorded on the software MHF. For other visits when this has recently been done, such as planned treatment appointments, the patient can simply be asked whether there have been any changes to his/her health. Both of these discussions should be recorded in some way, that is, the clinical notes should reflect that the MH has been checked and updated. In the absence of substantive changes to the patient's MH, the paper MHF should be used only after an appropriate interval, say, 2 years; this could be agreed as a practice policy.
Some systems allow the old MHF or software MHF to be printed off and checked by the patient. As with the paper MHF, checking and signing the form is not a substitute for the discussion process. It may lead to a repeat of the filtering of the patient's written information or having to explain the terminology within the medical notes. It may have an administrative burden, such as finding the old document, printing, checking it is legible, etc. Overall, it seems less efficient than simply having a discussion to check the MH details.
Sometimes a child may attend for examination or treatment without a parent or guardian present. Assuming that the child is considered Gillick competent for the purposes of treatment, the child may be also considered competent to provide a medical history.16 It would be sensible to make sure that the language used in discussion with the child is age appropriate and care must be taken to check understanding.
The process of taking a MH does not have to be burdensome or time consuming. The process should be done as quickly as can be safely achieved, bearing in mind that, in busy surgeries, 30 or more patients may be seen a day. A good MHF and a brief conversation with the patient will usually suffice for a healthy individual. If the process is not easy, quick and efficient then staff and patients can become frustrated, increasing the scope for errors.
Monitoring
Once a MHF and process has been created, monitoring is key to ensure efficiency. For example, any updates to a MHF should be piloted to check the result is as expected: do patients understand and respond in the desired way?
Staff meetings are an ideal time to discuss processes as problems can be raised by all members of the team and solutions found. Clinical near misses should be routinely discussed and recorded,17 and problems with a MH should be treated in a similar way.
Consideration should be given to all aspects of the patient journey. Having an agreed policy for common or foreseeable problems ensures that staff know how to handle situations, eg how will a visually impaired patient have the MH taken? Staff should be encouraged to reflect on how well they coped with such challenges, with a view to streamlining the process in the future.
Clinical audit may provide a useful framework for monitoring many aspects of the MH process. For example, if clinical records were audited, a check could be made to ensure that the scanned MHF is accessible and signed by the staff – surprisingly often the scan is illegible or the data file corrupted.
The future
Technological advancements will almost certainly substitute paper with touch screens as long as the data can be integrated and edited easily. Clearly, this will reduce the logistical burden somewhat but, no matter how effective the MHF, it can never replace the need for discussion with the patient.
Improved dental software MHFs should be designed with safety and efficiency as primary goals. For example, some existing software prevents out-of-date or incorrect information from being hidden or modified (not deleted, as an audit trail is important), which contributes to the ‘clutter’ and prevents the important information from standing out. Also, it would be useful for reception to have a simple means of identifying which patients are due (time interval) a MHF without having to search each file manually. Simple time-saving modifications, when extrapolated over a busy multi-surgery practice, could make a significant difference to efficiency overall.
Conclusion
Carrying out a medical history may seem a simple task but creating an efficient flow of information through the practice is vital to keep the process rapid and error-free. It is suggested that practices consider their patient journey, information flow and roles of staff. Monitoring of errors, problems and near-miss incidents will facilitate fine tuning of the process.