Kayser AF, Witter DJ, Spanauf AJ. Overtreatment with removable partial dentures in shortened dental arches. Aust Dent J. 1987; 32:178-182
Craddock HL, Youngson CC, Manogue M, Blance A. Occlusal changes following posterior tooth loss in adults. Part 2. Clinical parameters associated with movement of teeth adjacent to the site of posterior tooth loss. J Prosthodont. 2007; 16:495-501
Tonetti MS, Cortellini P, Graziani F, Cairo F, Lang NP, Abundo R Immediate versus delayed implant placement after anterior single tooth extraction: the timing randomized controlled clinical trial. J Clin Periodontol. 2017; 44:215-224 https://doi.org/10.1111/jcpe.12666
Pjetursson BE, Brägger U, Lang NP, Zwahlen M. Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clin Oral Implants Res. 2007; 18:97-113
Salinas TJ, Eckert SE. In patients requiring single-tooth replacement, what are the outcomes of implant- as compared to tooth-supported restorations?. Int J Oral Maxillofac Implants. 2007; 22:71-95
Ante IH. The fundamental principles of abutments. Michigan State Dent Soc Bull. 1926; 8:14-23
Nyman S, Lindhe J. Prosthetic rehabilitation of patients with advanced periodontal disease. J Clin Periodontol. 1976; 3:135-147
Laurell L, Lundgren D. Influence of occlusion on posterior cantilevers. J Prosthet Dent. 1992; 67:645-652
Laurell L, Lundgren D. Periodontal ligament areas and occlusal forces in dentitions restored with cross-arch bilateral end abutment bridges. J Clin Periodontol. 1985; 12:850-860
Laurell L, Lundgren D. A standardized programme for studying the occlusal force pattern during chewing and biting in prosthetically restored dentitions. J Oral Rehabil. 1984; 11:39-44
Brumfield RC. Fundamental mechanics of dental bridges, 5th edn. In: Tylman SD, Tylman SG (eds). St Louis: The CV Mosby Company; 1965
Shillingburg HT, Sather DA, Wilson EL, Cain JR, Mitchell DL, Blanco LJ, Kessler JC, 4th edn. (authors/eds). Boston: Quintessence Int; 2012
Smyd ES. The mechanics of dental structures. J Am Dent Assoc. 1952; 44:187-193
Smyd ES. Dental engineering as applied to inlay and bridge fabrication. N Y J Dent. 1951; 21:161-163
Biancu SI, Ericsson I, Lindhe J. The periodontal ligament of teeth connected to osseointegrated implants. An experimental study in the beagle dog. J Clin Periodontol. 1995; 22:362-370
Shillingburg HT, Fisher DW. Nonrigid connectors for fixed partial dentures. J Am Dent Assoc. 1973; 87:1195-1199
Djemal S, Setchell D, King P, Wickens J. Long-term survival characteristics of 832 resin-retained bridges and splints provided in a post-graduate teaching hospital between 1978 and 1993. J Oral Rehabil. 1999; 26:302-320
King PA, Foster LV, Yates RJ, Newcombe RG, Garrett MJ. Survival characteristics of 771 resin-retained bridges provided at a UK dental teaching hospital. Br Dent J. 2015; 218:423-428 https://doi.org/10.1038/sj.bdj.2015.250
Thoma DS, Sailer I, Ioannidis A, Zwahlen M, Makarov N, Pjetursson BE. A systematic review of the survival and complication rates of resin-bonded fixed dental prostheses after a mean observation period of at least 5 years. Clin Oral Implants Res. 2017; 28:(11)1421-1432 https://doi.org/10.1111/clr.13007
Schweitzer RD, Schweitzer J. Free-end pontics used on fixed partial dentures. J Prosthet Dent. 1968; 20:120-138
Briggs P, Ray-Chaudhuri A, Shah K. Avoiding and managing the failure of conventional crowns and bridges. Dent Update. 2012; 39:78-84
Walton TR. An up-to-15-year comparison of the survival and complication burden of three-unit tooth-supported fixed dental prostheses and implant-supported single crowns. Int J Oral Maxillofac Implants. 2015; 30:851-861 https://doi.org/10.11607/jomi.4220
Walton TR. Changes in the outcome of metal-ceramic tooth-supported single crowns and FDPs following the introduction of osseointegrated implant dentistry into a prosthodontic practice. Int J Prosthodont. 2009; 22:260-267
Walton TR. Changes in patient and FDP profiles following the introduction of osseointegrated implant dentistry in a prosthodontic practice. Int J Prosthodont. 2009; 22:127-133
Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JY. Clinical complications in fixed prosthodontics. J Prosthet Dent. 2003; 90:31-41
Asbia S, Ibbetson R, Reuben RL. Occlusal convergence and strain distribution on the axial surface of cemented gold crowns. Stud Health Technol Inform. 2008; 133:21-32
A Contemporary Approach to the Provision of Tooth-Supported Fixed Prostheses Part 1: Indications for Tooth Replacement and the Use of Fixed Bridges Retained by Crowns
A Contemporary Approach to the Provision of Tooth-Supported Fixed Prostheses Part 1: Indications for Tooth Replacement and the Use of Fixed Bridges Retained by Crowns Richard Ibbetson Dental Update 2024 45:1, 707-709.
Fixed tooth replacement is a central part of prosthodontic care for patients. The approach and options for treatment have changed due to the decrease in dental disease in the population and the impact of the osseo-integrated implant. Despite the impact of the dental implant, there remain indications for the use of tooth-supported fixed prostheses. Improving oral health, the continued developments in resin-retained bridgework and the dental implant have reduced the indications for fixed prostheses retained by crowns. The last 30 years have seen a simplification in the design of fixed bridgework and this article describes the contemporary approach to this treatment modality. The first of this two part series discusses appropriate designs and the use of fixed bridges retained by crowns and the second part discusses fixed bridges where the abutment teeth require minimal or no preparation.
CPD/Clinical Relevance: To assist in the appreciation of the principles of design for fixed bridgework, whether supported by crowns or resin retainers.
Article
Changes in the pattern of dental disease with the reduction in tooth loss and an improved understanding of what constitutes a stable functioning dentition have altered the indications for tooth replacement.
When fixed tooth replacement is required, the need for tooth-supported fixed prostheses has decreased as a consequence of the impact of implants. Their increasing and generally beneficial use necessitates a re-evaluation of the advice that patients are given. In a recent informal survey, young dentists were asked how they would choose to have their own missing maxillary central incisor replaced, and well over 90% of respondents opted for an implant-supported prosthesis. This was not surprising, nor was their second choice, which was overwhelmingly a resin-retained bridge rather than a tooth-supported fixed bridge where the retainers were crowns.
Indications for tooth replacement
There are four indications:
Aesthetics;
Function;
Patient perception and self-image;
Occlusal stability.
Aesthetics
The aesthetic requirements of patients are a clear indication for some form of tooth replacement. It is likely that the majority of patients would prefer a fixed replacement for their missing teeth, however, it may not always offer the best aesthetic outcome. Deficiencies of hard and soft tissues are more easily managed with removable prostheses than fixed.
Function
This is more complex and many patients function well without detriment to their remaining dentition with less than the full complement of teeth. Patients can function adequately with shortened dental arches: the work of Kayser and colleagues has demonstrated this clearly.1 A minimum of ten pairs of opposing teeth is deemed to be necessary to provide reasonable function and maintain a degree of occlusal stability.
All dental restorations have a finite life-span and the provision of any fixed prosthesis should clearly only take place if it is needed by the patient. Where a posterior tooth is lost, the decision to replace it in the absence of aesthetic need should not be made immediately. The tooth should be removed and a suitable period of healing and patient adaptation allowed before any replacement is discussed with the patient. If a patient is asked a week after loss of a molar, whether the tooth is missed, the answer will always be affirmative. It is clear that not all missing posterior teeth need replacement and patients may adapt easily to their absence. On the other hand, if, after a number of months, the patient indicates that he/she misses the tooth and would like it replaced, it is reasonable to consider doing so.
There are two additional factors which may cause the dentist to recommend tooth replacement at an early stage. The first is concern that the teeth adjacent to, and opposing, the edentulous space will move and the second that, should the patient wish to have an implant-supported fixed replacement, alveolar bone will be lost in the healing and re-modelling process. Both of these have an element of truth but cannot constitute valid reasons for routine early tooth replacement.
Changes in tooth position and occlusal stability
Changes in the position of posterior teeth following an extraction are unpredictable.2 A number of the older textbooks of crown and bridgework contain diagrams illustrating the possible sequelae of loss of a molar tooth. However, such changes are often mild and happen slowly. The provision of a fixed prosthesis to prevent posterior tooth movement is not valid. Changes in tooth position are not necessarily deleterious and do not constitute a loss of posterior occlusal stability. If occlusal stability were lost, any damaging effects will be found most commonly by increased loading of the anterior teeth. Figures 1 and 2 show a patient in whom the teeth were lost some 15 years earlier. There are changes in tooth position which are more marked on the right side than the left, but no loss of occlusal stability as there are no signs of increased loading of the anterior teeth, as would be evidenced by drifting, wear, fracture or increasing tooth mobility. If these are seen, a full occlusal analysis is required to determine whether replacement of the missing posterior teeth will be beneficial in reducing the loads on the dentition, and the anterior teeth in particular.
Figure 1. Right buccal view of a patient where the missing teeth were lost approximately 15 years earlier.Figure 2. Left buccal view of the same patient as in Figure 1, where the missing teeth were lost approximately 15 years earlier.
Deterioration in potential sites for dental implants
In relation to the immediate or relatively early provision of dental implants, there may be some justification for this in regions of the mouth where aesthetics are of importance. However, possible loss of alveolar bone height and width are rarely indications for taking an early decision to replace a missing posterior tooth. In the anterior region, the need to replace a tooth, which is about to be extracted, immediately is entirely understandable. However, caution should be exercised if the immediate placement is to be supported by a dental implant, as there are more complications than when implant placement is delayed.3
One essential aspect of fixed tooth replacement is to be aware that any prosthesis has a finite life-span. Those that are tooth-supported are likely to produce an element of damage to the abutment teeth when they fail. The greater the complexity of the intervention, the more complicated is the treatment provision which possibly increases the risks of failure.
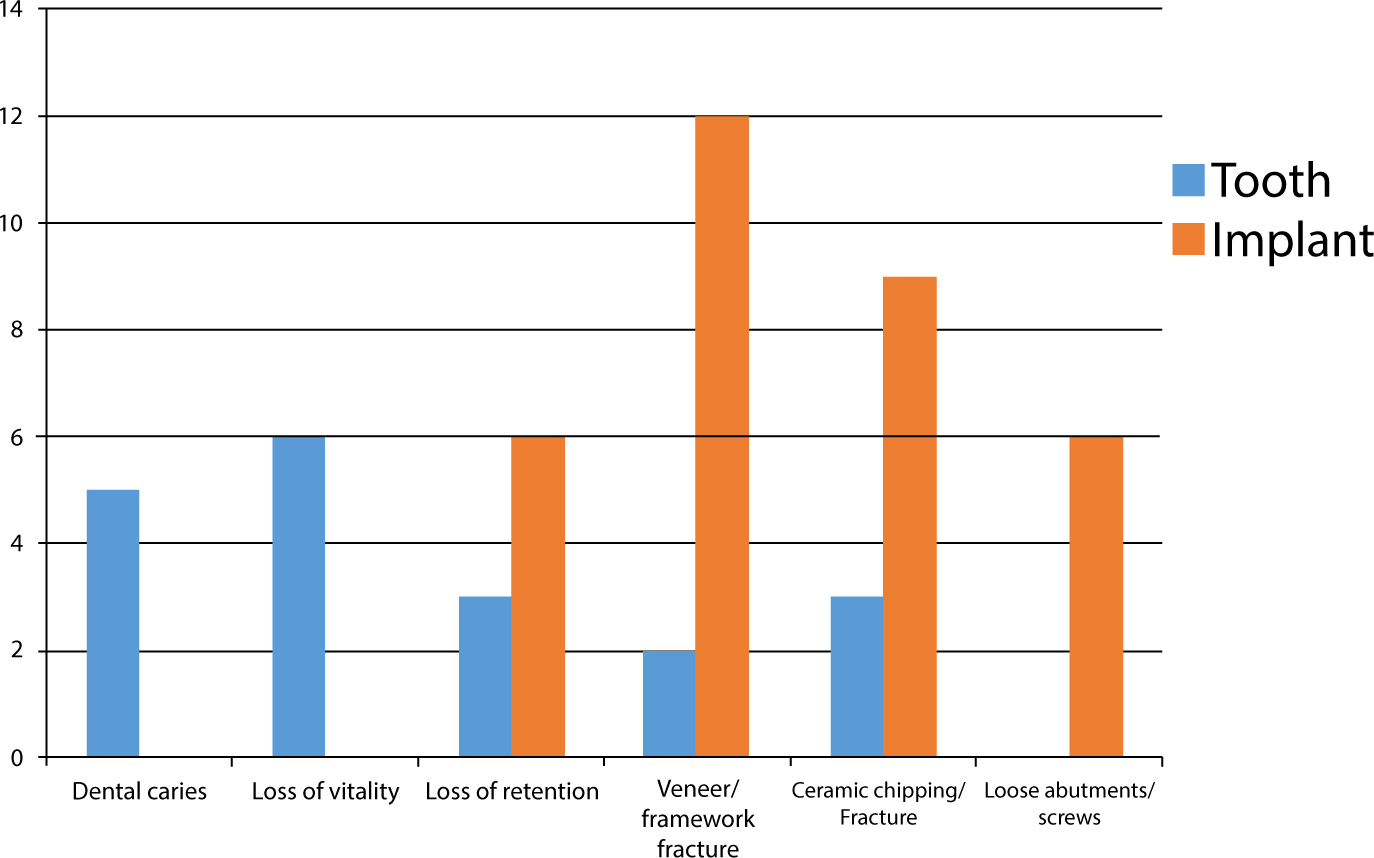
Dentists advising patients on their options for fixed tooth replacement must be able to provide information on success and complication rates to permit informed consent. One of the most useful papers is by Pjettursson et al4 and the data from this are shown in diagrammatic form in Figure 3. The complication rate for implant-supported prostheses is higher than for tooth-supported fixed bridges, where the retainers are crowns. However, the nature of the complications for the tooth-supported fixed prostheses is much worse than for implant-supported prostheses. It is unfortunate that this particular study does not contain data on the performance of tooth-supported bridges where the abutments are either minimally prepared or not prepared at all.
Figure 3. Complications of tooth-supported and implant-supported fixed prostheses. Redrawn from Pjettursson et al.4
In conclusion, the data indicate that the highest success rates for fixed tooth replacement can be achieved with implant-supported fixed prostheses.5 This applies whether the treatment is the replacement of a single tooth or multiples. However implant-based treatment is demanding and these demands are matched by patients' expectations. All forms of tooth replacement require appropriate discussions and planning with the patient and the range of options for treatment must be presented. There are clinical situations where the provision of an implant-supported prosthesis is less desirable than one that is tooth-supported. These are hard to define but, in general, as implant provision becomes increasingly complex, fixed alternatives that demand less of both the patient and operator should be considered. It remains appropriate that the simplest procedure that will satisfy the patient's requirements, whilst providing a reasonable prognosis, should be the treatment that is advised.
Changes in bridge design
The majority of concepts of bridge design were formed either just before or soon after the Second World War. These principles were based predominantly on mechanics and have stood both the test of time and some degree of scientific investigation. However, the improved understanding of the biological factors related to tooth-supported fixed prostheses has gradually modified thinking and clinical practice.
Early thoughts on the support necessary for fixed bridgework can be traced back to the classic paper by Ante,6 which proposed a conservative approach to the assessment of the periodontal support offered by potential abutment teeth. These classical principles were slow to change. It was perhaps the work of Nyman and Lindhe7 in the 1970s which demonstrated the capacity of teeth with healthy but severely reduced levels of periodontal support to act as abutments for fixed bridgework. Their work cannot be applied directly to all patients as the occlusal loads in these patients were found to be significantly lower than for dentitions with more normal levels of periodontal support.8,9,10 However, they showed that, although periodontal support is clearly important, it is the combination of periodontal health with a reasonable level of periodontal support that is important. In the presence of periodontal health, there is no evidence to link increased loading with loss of periodontal attachment.
The description of the mechanics of fixed bridge design can be attributed to the work of Tylman11 and other researchers of that time. The principles in relation to the behaviour of beams still hold good today and are well summarized by Shillingburg et al.12 The role of torsion and bending of fixed prostheses remains an important element of fixed tooth replacement, whether this be by means of teeth or dental implants.
Improved knowledge and understanding of the biological and mechanical aspects of fixed prostheses have led to changes in design principles. However, the literature appears to treat the design principles of bridges using crowns as retainers as being fundamentally different from those for resin-retained bridgework. This does not seem entirely appropriate as many of the mechanical principles of adhesive bridge design are identical to those described for fixed bridges retained by gold partial veneer crowns, frequently used before the development of metal-ceramic restorations.
There are general over-arching principles of design that are applicable to all tooth-supported fixed bridges.13,14 These are:
Designs should be simple;
Retainers should cover as much of the functional surfaces of the teeth as possible;
Prostheses should be as rigid as is feasible;
The occlusal contacts must be controlled.
These apply to tooth-supported fixed bridgework, whether supported by crowns or resin-bonded retainers.
Simple designs
The dental implant has removed the indications and need for bridge spans of greater length and, consequently, has reduced the requirements for complex designs.
If support on each side of the edentulous space is required, bridges should generally not use more than one abutment at each end of the span: there are few indications for the use of double abutments.
Occlusal coverage
The retainers for tooth-supported fixed bridges should cover as much of the functional surfaces of the abutment teeth as possible. This is clearly not a factor where full crowns are the retainers, but it is where partial coverage retainers are used. Partial veneer crowns are so rarely employed in fixed bridges that the principles underpinning their successful use have been largely forgotten, but the parallel between these retainers and those used for resin-retained bridges is clear.13,14 Coverage of the functional surfaces provides control of the occlusal contacts and this control should be exercised, both on mandibular closure and excursive mandibular movements. This becomes of significant importance when the decision is made to provide a resin-retained bridge of fixed-fixed design.
Rigidity
Rigidity in a fixed prosthesis is a function of the materials from which it is made and the occluso-gingival thickness of the elements of the bridge. Nearly all the research on torsion and bending of fixed prostheses was carried out on bridges that were considered to be made of cast gold. The commonest material used currently for a fixed bridge is cast metal veneered with porcelain: it is not clear how the behaviour of this combination differs from cast gold but it is reasonable to assume that the same principles apply. Bridges usually have sufficient thickness in their pontics, but it is the connectors and the retainers that are at greater risk. A minimum connector height of 2 mm is described12 and this should be increased in longer span bridgework or where higher loads are anticipated. At a clinical level, the major limiting factor on the dimensions of connectors is clinical crown height, whilst the need to have sufficient embrasure space to allow access for effective cleaning by the patient reduces the height that can be occupied by the connectors. Retainer thickness is important to minimize flexure of the retainer and the stresses on the cement lute. Thickness may be compromised where crown height is in short supply or when providing a resin-retained bridge where inter-occlusal space is limited.
Types of design for bridges
Classically four designs are described:
Fixed-fixed;
Fixed-movable;
Cantilevers;
Complex or Hybrid.
Fixed-fixed bridges
In a fixed-fixed design, there are one or more abutments at each end of the span and all the connectors in the bridge are rigid. As a consequence, loads are distributed more equally between the abutment teeth. This design is indicated particularly where spans are long. Exactly what constitutes a long span can only be determined by knowing the number of teeth to be replaced and the loads that may be exerted on the prosthesis. It might generally be conceded that the replacement of more than two teeth in the posterior part of the mouth and more than three anteriorly would constitute long spans, however, absolute descriptors are frequently impossible.
Anterior bridges where more than one tooth is being replaced are generally made fixed-fixed (Figure 4), as the pontics lie outside the axis between the abutments and are therefore relatively cantilevered with respect to them: this places increased stress upon them.
Figure 4. A fixed-fixed bridge retained by crowns replacing four maxillary incisors circa 1990.
An implication of a fixed-fixed design is that, because the loads are distributed equally between the abutments, the teeth at either end of the span should have broadly comparable retention and resistance form. This is both a function of the way the teeth are prepared if crowns are being used as retainers and also of the morphology of the teeth themselves. For example, the differential in dimensions between a mandibular molar and premolar is easy to see and will impact the development of generally equal retention and resistance form.
Mild degrees of non-alignment between the abutment teeth are not a source of particular difficulty for the provision of a fixed-fixed bridge. However, significant mal-alignment risks excessive tooth removal and increased pulpal damage as the abutments must present a common path of withdrawal. It is good practice for the clinician prior to any bridge preparation involving crowns to rehearse the preparations on a study cast prior to executing them in the mouth. It is sensible when making the clinical preparations to gauge the overall path of insertion of both abutments before beginning. The smaller of the two teeth should be prepared first: if the larger abutment is prepared first, any error in the path of insertion when applied to the smaller abutment tooth may result in an excessive removal of tooth structure.
Fixed-movable bridges
These are designed with one connector being movable thus allowing a degree of differential movement between the abutments. The degree of movement will be controlled by the length of the span and the design of the movable connector. Movable connectors can be constructed with differing degrees of tolerance, allowing greater or lesser movement. The correct location for the movable connector is in the distal aspect of the minor retainer and this is always the more anterior of the abutments, irrespective of its size. For example, in Figure 5, the fixed-movable bridge made using crowns as the retainers replacing the maxillary right second premolar with the first molar and first premolar as abutments, the molar is the major abutment and the premolar the minor, with the movable connector located in the distal of the premolar. The movable connector should be designed so that the female is within the distal of the minor abutment and the male part in the mesial of the pontic. This results in the bridge behaving as a fixed-fixed prosthesis under direct axial loading, whilst under all other loads there will be a degree of separation of the components of the movable connector such that the major retainer and abutment receive a greater proportion of the load. This type of stress breaking is useful when there is a differential in retention and resistance form between the retainers, or when the minor abutment has been compromised by previous restorative procedures.
Figure 5. A fixed-movable bridge replacing a maxillary premolar. Note the position and orientation of the movable connector.
The second indication for a fixed-movable design is in bridges retained by crowns where the abutment teeth have distinctly different axial inclinations. Preparation for a fixed-fixed design under these circumstances results in excessive removal of tooth structure in order that the preparations align. The use of a movable connector allows the two abutments to have retainers with different paths of insertion, thus preserving tooth tissue with less risk of compromising the dental pulp.
The literature15 also indicates that, at least on theoretical grounds, it may be beneficial to the periodontal ligaments of the abutment teeth if they are not rigidly linked together, with a fixed-movable bridge allowing a degree of independent mobility between the abutment teeth. This postulation, whilst interesting, has never been proved to have any influence on long-term outcomes.
A strategically placed movable connector allows longer span bridgework to be constructed in smaller sections, thereby increasing serviceability and improving the prospects of full seating. It can also improve the mechanics of bridges where two teeth are missing but there is an abutment not only at the ends of the span but also in the middle. This is the so-called ‘pier abutment’, which is well described in the literature.16 The movable connector is placed in the distal of the pier abutment, with the female component within the distal of the retainer of the pier abutment and the male in the mesial of the pontic. However, this situation presents perhaps less commonly due to the impact of the dental implant as an alternative way of replacing the missing teeth and an emphasis on shorter spans and simpler designs (Figure 6).
Figure 6. Management of the pier abutment at UL1 by using multiple resin-retained prostheses.
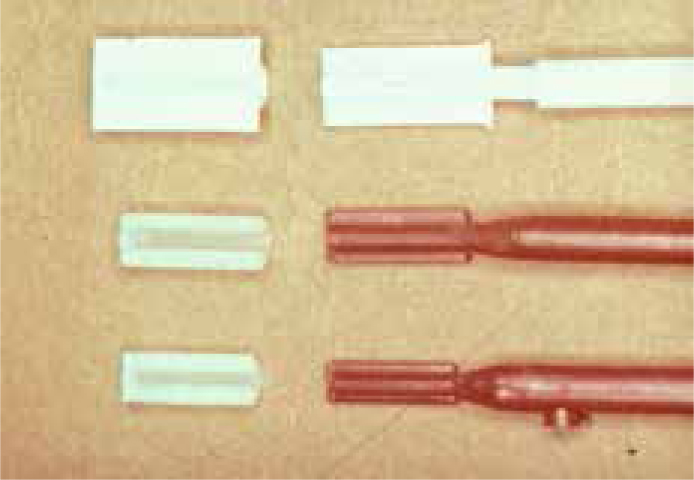
The movable connector occupies both vertical and horizontal space and it should be housed within the normal contours of the restored minor abutment. This necessitates preparing a box in the distal surface of the tooth which should align with the path of withdrawal of the preparation of the major abutment (Figure 7). Pre-formed plastic patterns, often called erroneously semi-precision attachments, provide a convenient way of constructing fixed-movable connectors (Figure 8). The clinician may find it helpful to have one of these cast in non-precious alloy so that it can first be sterilized and then used clinically to ensure that the box is of the appropriate size.
Figure 7. Distal box in the minor abutment at UL4 prepared to house the movable connector for a fixed-movable bridge UL4 to UL7.Figure 8. Examples of pre-formed plastic patterns used to create movable connectors.
Cantilevers
The cantilever is the most mechanically unsound of designs as all the loads are transmitted to the sole abutment. However, they offer simplicity of design without the requirement to link abutment teeth at each end of the span. Traditional textbooks, particularly those written in North America, where the influence of the great innovators, researchers and clinicians of the pre- and post-World War II periods is still understandably strong, are cautious in their use of cantilevers anteriorly and recommend avoidance, if possible, posteriorly unless specific requirements are met. The reasons for this need to be understood as, in many parts of the world including the United Kingdom, the cantilever has become the design of choice when a single missing tooth is to be replaced by a tooth-supported fixed prosthesis. This is particularly true for the replacement of single missing anterior teeth using a resin-retained bridge as the data indicate that this design gives the highest success rate for these adhesive fixed prostheses.17,18,19
The traditional fixed prosthodontic literature indicates two concerns with the cantilever design. The first is the risk of bodily movement of the abutment, retainer and pontic and the second is fracture of the abutment tooth. There is literature evidence for the latter but little for the former.20
Occlusal forces are higher in the posterior part of the mouth than anteriorly and, traditionally, it has been recommended that the use of posterior cantilevers as bridges retained by crowns is better avoided. If this design is selected, most classical texts would recommend the use of double abutments, which must have excellent crown height to provide sufficient retention and resistance form, and only light contacts on the pontic. Figures 9, 10 and 11 show a posterior double abutted cantilever bridge replacing a first maxillary premolar. The illustrations are nearly 30 years old and this type of design would be rarely recommended today due to the complex mechanics produced by the double abutments. There is a lack of useful research evidence in this area, however, it has become apparent that expert opinion has produced some movement away from this traditional teaching. Current opinion will, in the case of cantilever bridges in the posterior part of the mouth, permit the use of a large tooth as the single abutment for the replacement of a smaller tooth, ie a molar abutment with a premolar pontic.21 It is also the case that, in the posterior part of the mouth, mesial-facing cantilevers carry a lower risk than distal-facing cantilevers
Figure 9. Double abutments for a posterior cantilever bridge retained by crowns.Figure 10. Occlusal view of the double abutted cantilever bridge replacing a maxillary first premolar.Figure 11. Buccal view of the double abutted cantilever bridge replacing a maxillary first premolar.
The quality of the abutment may also be a factor relevant to the incidence of abutment fracture. Posterior teeth which have lost large amounts of coronal tissue will have cores replacing the missing dentine. It is likely that such teeth used as the abutment for a cantilever bridge retained by a crown may be more prone to coronal fracture when stresses are increased, as they are for cantilever designs. The same will not necessarily be the case for a relatively intact tooth used to support a resin-retained bridge.
Complex or hybrid bridges
The term complex bridge has been used traditionally to describe a fixed prosthesis, where different types of bridge are used within the overall prosthesis: for example, a bridge where one part is made fixed-fixed and another segment is either fixed-movable or a cantilever. The use of the term ‘hybrid’ is possibly more useful as it also permits inclusion of fixed prostheses where a variety of both designs and retainers is used.
Tooth-supported fixed bridges using crowns as retainers
The ability to use dental implants together with the slow but steady decrease in dental caries have reduced the indications for fixed prostheses retained by crowns. The dental implant has also improved the prognosis for a tooth-supported fixed bridge when it is indicated. The data published by Walton22,23,24 showed that, following the introduction of the dental implant, the length of tooth-supported bridge spans has reduced whilst, correspondingly, his outcomes for bridgework in general have improved, the implication being that it is now not necessary, or even advisable, to consider tooth-supported fixed bridges where the risks are relatively high: examples are longer span bridgework or compromised abutment teeth. Walton's data indicate that spans have become shorter, which reduces the demands on both the abutment teeth and the prosthesis. In his studies, which are consistent with many others, the root-treated tooth used as an abutment produced lower survival rates than when vital teeth were available. However, it is of note that he reported that the increased use of dental implants has improved the survival rate of tooth-supported fixed bridges where endodontically-treated abutments were used as abutments. This seeming paradox is explained by the author having avoided the use of those root-treated teeth which have lost large amounts of coronal tissue or others have conditions that were likely to result in poorer outcomes. Walton's study has relevance as it has a clear message that not all endodontically treated teeth have poor prognoses. The inevitable influence of patients' expectations and the keenness of some dentists to provide dental implants has led many to a conclusion that root-filled teeth should not be used as abutments for fixed bridges. Walton's data indicate that such a conclusion is erroneous.
There can be little or no reason for using tooth-supported fixed bridgework retained by crowns where the abutment teeth are generally sound or with minor previous restorative intervention. Overall, there has been a major reduction in the need for such bridges. However, there are occasional exceptions to this which are:
Replacement of an existing bridge retained by crowns;
A tooth lost adjacent to crowned teeth;
Patient preference.
Replacement of an existing bridge retained by crowns
The major indications are the replacement of an existing tooth-supported bridge where the abutments are in reasonable condition or the loss of a tooth adjacent to one that is already crowned. Figures 12 and 13 show a patient who had lost the maxillary right lateral incisor and the maxillary right canine had a rather elderly and unaesthetic crown. The tooth was considered a good risk as an abutment so, following healing and re-modelling of the site of the lateral incisor, a cantilever was made using the canine as the abutment. Short anterior spans are suitable for a simple cantilever design and there is little benefit in making such a bridge fixed-fixed as the mechanics become more complicated. Where an existing bridge is to be replaced, it should be remembered that abutment teeth that have served satisfactorily for many years are unlikely to perform as well when a replacement bridge is made. Not only are there the pulpal sequelae to consider, but dentine is a relatively brittle material increasing the risk of fatigue fracture with time.
Figure 12. Labial view of a cantilever bridge retained by a crown replacing the right maxillary lateral incisor.Figure 13. Palatal view of the cantilever bridge replacing the right maxillary lateral incisor.
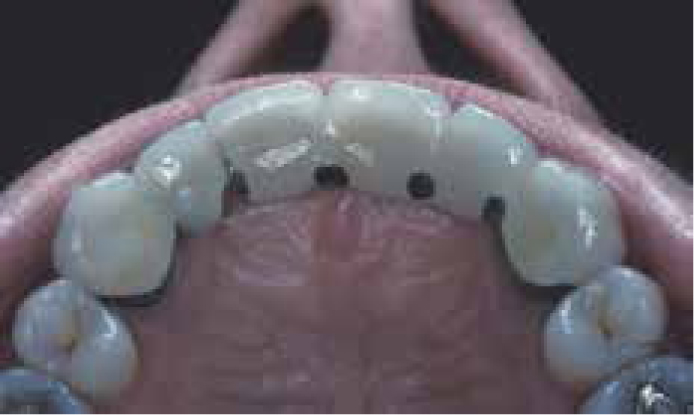
Figures 14 and 15 show a patient who had an unaesthetic fixed-fixed bridge where the canine was already adjacent to the central incisor. The condition of the maxillary left canine and second premolar were considered to be good and the replacement of the bridge with a further tooth-supported fixed prosthesis seemed reasonable. However, the patient was concerned about the further use of metal-ceramic units and, despite discussions where the potential disadvantages of all-ceramic fixed prostheses were outlined, wished to have an all-porcelain bridge. A veneered fixed-fixed zirconia bridge was made (Figures 16 and 17). Figure 18 shows the preparations necessary to provide sufficient space for the technician to work and it is evident that these lead to further loss of tooth structure: the implications of this are both pulpal and structural. This type of preparation is only possible where there is good crown height, not only to allow sufficient inter-occlusal space to be created but also to house the connectors.
Figure 14. Facial view of an unaesthetic fixed-fixed bridge where the canine was adjacent to the central incisor.Figure 15. Palatal view of the fixed-fixed bridge where the canine was adjacent to the central incisor.Figure 16. Facial view of veneered zirconia bridge UL3, 4 and 5.Figure 17. Occlusal view veneered zirconia bridge UL3, 4 and 5.Figure 18. View of the working cast showing the preparations for a veneered fixed-fixed zirconia bridge UL3 and UL5.
The replacement of a fixed bridge implies that a previous one has failed or requires replacement on aesthetic grounds. The dentist must have a full understanding of the cause of failure before a replacement is provided. Dental caries25 is recorded as being the commonest cause of failure of fixed prostheses using crowns as retainers. However, the data are simplistic. In order for recurrent caries to occur, the intra-oral conditions must be present, namely inadequate dietary and plaque control. However, the same paper shows a higher failure rate for fixed bridgework than for single crowns. There are two possibilities why this is the case. The first is that people with missing teeth have most frequently lost them because of poor disease control and, if this continues, restorations will be at higher risk of failure.
The second relates to the integrity of the cement lute. There is no scientific evidence linking marginal discrepancies around crowns with recurrent caries, but fixed bridgework places increased stress on the cement26 beneath the retainers. It is possible that this increases the disintegration and loss of the cement: protection of which is in part linked to the geometry of the tooth preparation. Features that increase retention, but particularly resistance form, will reduce the stress on luting cements, which are weaker in shear than under compression. Resistance form is a function of the preparation height to diameter ratio, whilst control of taper limits the paths of withdrawal of the retainers. Preparations for bridge abutments require sufficient crown height and control of taper and many benefit from the use of additional features to increase their resistance form, such as axial grooves and boxes. However, these are rarely as effective as crown height and control of taper.
Figure 19 shows a fixed bridge which had become uncemented on the more distal abutment, the maxillary second molar. It is to be noted that the retainer is broad and flat and therefore lacking resistance form. Figure 20 shows the tooth after the bridge had been removed and an access cavity prepared through the retainer as the tooth was both carious and pulpally non-vital. The picture of the preparation shows the tooth to be short and with a high base diameter to height ratio. This might have provided reasonable retention but its resistance form would have been poor. Treatment options were discussed with the patient who was keen to have a further fixed replacement of the maxillary first molar. The site is not necessarily the most suitable for an implant-supported crown but the situation was not appropriate for a further tooth-supported bridge without both retention and resistance form being improved. Following root canal treatment, surgical crown lengthening of both abutments was carried out (Figure 21). This made significantly more coronal tooth structure available. An amalgam dowel core was placed in the maxillary second molar and both it and the maxillary second premolar re-prepared. Figure 22 shows the final preparations which have good parallelism and appropriately prepared occlusal surfaces. However, the crown height was not sufficient for the use of porcelain occlusal surfaces, which require additional occlusal reduction compared with cast metal. Axial grooves, prepared with a 170 friction-grip tungsten carbide bur, were used to reduce the rotational radius of the preparation and increase resistance form. These grooves were made in the long axis of the preparation rather than parallel to an axial surface. The increase in the available crown height also created space for suitable connectors to be provided. Figure 23 shows the completed bridge; the design was fixed-movable with the movable connector located in the distal of the minor retainer and with the male being part of the pontic. This is the only position appropriate for the movable connector so that the two parts are fully mated under occlusal loading. Reversing the movable connector, as is sometimes seen, is likely to result in the male and female elements separating or pulling apart as a consequence of occlusal loading and mesial drift. The fixed-movable design was selected to minimize the loads on the minor abutment tooth, with a distal box having been prepared in the second premolar.
Figure 19. Occlusal view of a maxillary fixed-fixed bridge which was uncemented on UL7.Figure 20. Occlusal view with bridge removed showing loss of tissue due to dental caries and a lack of crown height at UL7.Figure 21. UL7 following root canal treatment and surgical crown lengthening.Figure 22. The completed re-preparation of the maxillary left second molar showing minimal taper, appropriate occlusal form and additional axial grooves to increased resistance form.Figure 23. The final fixed-movable bridge with metal-occlusal surfaces and the movable connector in the distal surface of the maxillary left second premolar.
There is no clinical study which demonstrates the superiority of fixed-movable bridges constructed to provide short-span fixed prostheses. However, where the minor abutment is relatively small or somewhat compromised, the use of the movable connector reduces the loading on the minor retainer and abutment under all circumstances apart from direct axial loading.
Conclusion
This first of a two-part article has reviewed the indications for the use of tooth-supported fixed bridgework retained by crowns. It has emphasized that the indications for this type of fixed prosthesis have diminished significantly and that there have been changes in the principles underpinning their design. The second part of the article will consider the influence of patient preference on the choice of fixed prosthesis and will describe the use of bridges where little or no preparation of the abutment teeth is required. The resin-retained bridge should be the first choice where a fixed prosthesis retained by natural teeth is required.