Pal US, Sharma NK, Singh RK, Mahammad S, Mehrotra D, Singh N, Mandhyan D. Direct vs. indirect sinus lift procedure: a comparison. Natl J Maxillofac Surg. 2012; 3:31-37
Riben C, Thor A. The maxillary sinus membrane elevation procedure: augmentation of bone around dental implants without grafts – a review of surgical technique. Int J Dent. 2012; https://doi.org/10.1155/2012/105483
Wallace SS, Froum SJ. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann Periodontol. 2003; 8:328-343
Hallman M, Sennerby L, Lundgren S. A clinical and histological evaluation of implant integration in the posterior maxilla after sinus floor augmentation with autogenous bone, bovine hydroxyapatite or 20:80 mixture. Int J Oral Maxillofac Implants. 2002; 17:635-643
Felisati G, Salibene AM, Di Pasquale D, Borloni R. How the simplest dental implant procedure can trigger an extremely serious complication. BMJ Case Rep. 2012; 2012
Wallace SS. Lateral window sinus augmentation using bone replacement grafts: a biologically sound surgical technique. Alpha Omegan. 2005; 98:36-46
Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. Part 1: lateral approach. J Clin Periodontol. 2008; 35:216-240
Alkan A, Celebi N, Bas B. Acute maxillary sinusitis associated with internal sinus lifting: report of a case. Eur J Dent. 2008; 2:69-72
Kim JJ, Freire M, Yoon JH, Kim HK. Postoperative maxillary cyst after maxillary sinus augmentation. J Craniofac Surg. 2013; 24:e521-523
Meleo D, Mangione F, Corbi S, Pacifici L. Management of the Schneiderian membrane perforation during the maxillary sinus elevation procedure: a case report. Ann Stomatol. 2012; 3:24-30
Schwartz-Arad D, Herzberg R, Doley E. The prevalence of surgical complications of the sinus graft procedure and their impact on implant survival. J Periodontol. 2004; 75:511-516
Al-Dajani M. Incidence, risk factors and complications of schneiderian membrane perforation in sinus lift surgery: a meta-analysis. Implant Dent. 2016; 25:409-415
Aimetti M, Romagnoli R, Ricci G, Massei G. Maxillary sinus elevation: the effect of macrolacerations and microlacerations of the sinus membrane as determined by endoscopy. Int J Periodont Rest Dent. 2001; 21:581-589
Viňa-Almunia J, Peňarrocha-Diago M, Peňarrocha-Diago M. Influence of perforation of the sinus membrane on the survival rate of implants placed after direct sinus lift. Literature update. Med Oral Patol Oral Cir Bucal. 2009; 14:E133-136
Wallace SS, Mazor Z, Froum SJ, Cho SC, Tarnow DP. Schneiderian membrane perforation rate during sinus elevation using piezo-surgery: clinical results of 100 consecutive cases. Int J Periodont Rest Dent. 2007; 27:413-419
Migration of bone graft material into the maxillary sinus: a case report Christina Evangelou Georgina Peck Nishma Somaia Wayne Halfpenny Dental Update 2024 44:10, 707-709.
Authors
ChristinaEvangelou
BDS(Hons), MFDS RCSEdin
Royal Free Trust, Oral and Maxillofacial Department, Barnet Hospital, Wellhouse Lane, Barnet, Hertfordshire, EN5 3DJ, UK
A 48-year-old patient presented at the Oral and Maxillofacial Surgery department complaining of symptoms of chronic sinusitis and gave a history of a recent sinus lift procedure in primary care. The patient was examined and investigated via a CBCT which showed extruded bone graft material in the left maxillary antrum. The patient then had to undergo surgery under general anaesthetic to remove the foreign material from the antrum, which eventually relieved his symptoms. This paper discusses potential complications of sinus lift procedures, including perforation of the Schneiderian membrane, perioperative recognition, potential management and how to avoid this complication.
CPD/Clinical Relevance: Membrane perforation is the most common complication of sinus lift procedures. Clinicians need to be aware of the risk, presenting symptoms, investigation and necessary treatment of this complication.
Article
Dental implants are becoming increasingly popular for restoring the aesthetic and functional needs of the adult population. The latest Adult Dental Health Survey found that 1% of the adult population has at least one dental implant1 and this figure is expected to rise.
Sufficient volume and density of bone is required for successful implant placement. In the posterior maxilla, this is often problematic due to alveolar bone resorption and sinus pneumatization.2
The maxillary sinus lift procedure is used to increase vertical bone volume in the posterio-lateral maxilla in order to place the implants.
The procedure involves intra-oral access to the maxillary sinus. The sinus membrane (Schneiderian membrane) is lifted and a bone graft material (allogenic, autogenic or synthetic) is placed under the lining.3 It is possible to place an implant at the same time as the sinus lift procedure.4 However, some literature recommends a healing period of 6–9 months for mature bone formation prior to implant placement.5
Although a sinus lift procedure is considered to be a routine and low risk procedure, numerous complications can arise both intra- and post-operatively.6
Case presentation
A 48-year-old, fit and healthy, non-smoking male presented to the Oral and Maxillofacial Surgery department with symptoms of chronic sinusitis, including congestion, pain and tenderness of the left cheek and a feeling of a blocked nose. He was afebrile and systemically well. The patient gave a history of a recent sinus lift procedure and was planning on having implant placement in the near future. The surgery was performed by an experienced general dental practitioner (GDP) in primary care who reported using Bio-Oss®, Bio-Gide® and the patient's own bone fragments. The Schneiderian membrane was secured by placing a piece of Bio-Gide® prior to placing the graft material. The GDP reported that the surgical procedure was completed as planned with no immediate complications recognized. However, the patient began to complain of sinusitis symptoms and was prescribed several courses of broad-spectrum antibiotics, anti-inflammatory analgesics and a nasal spray, which provided initial relief. However, the symptoms returned and the patient was referred to secondary care.
Investigations
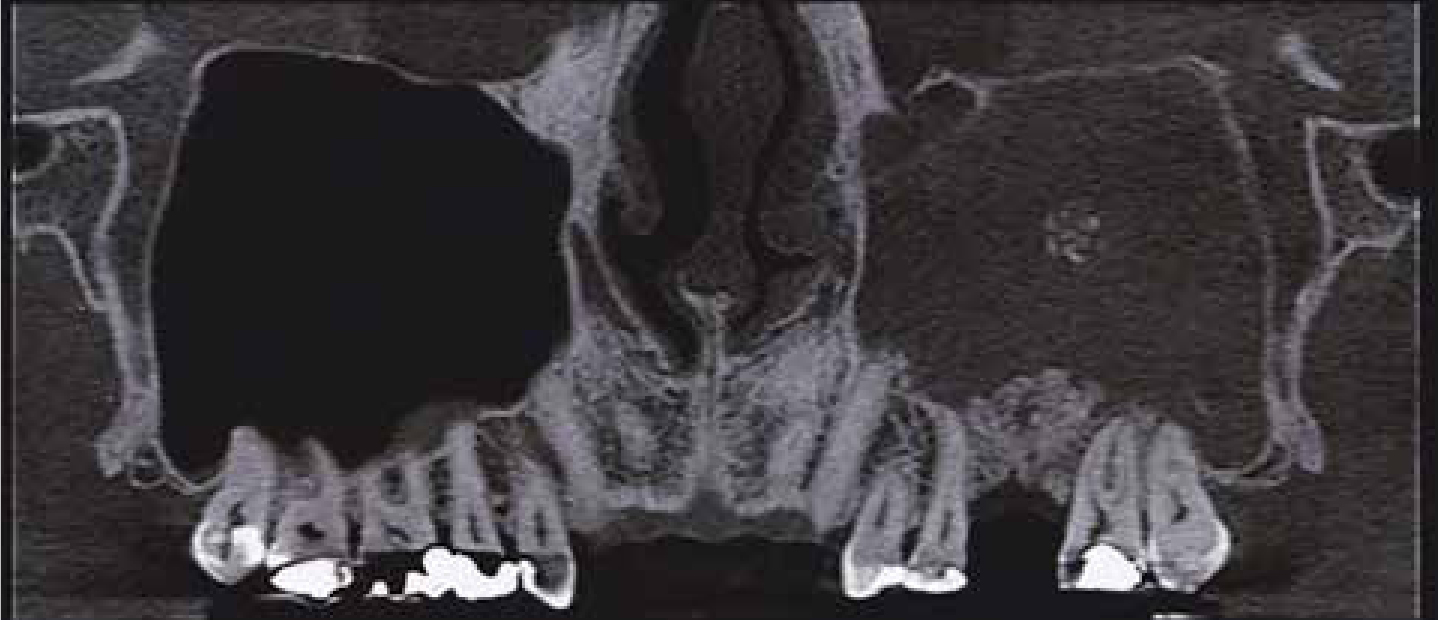
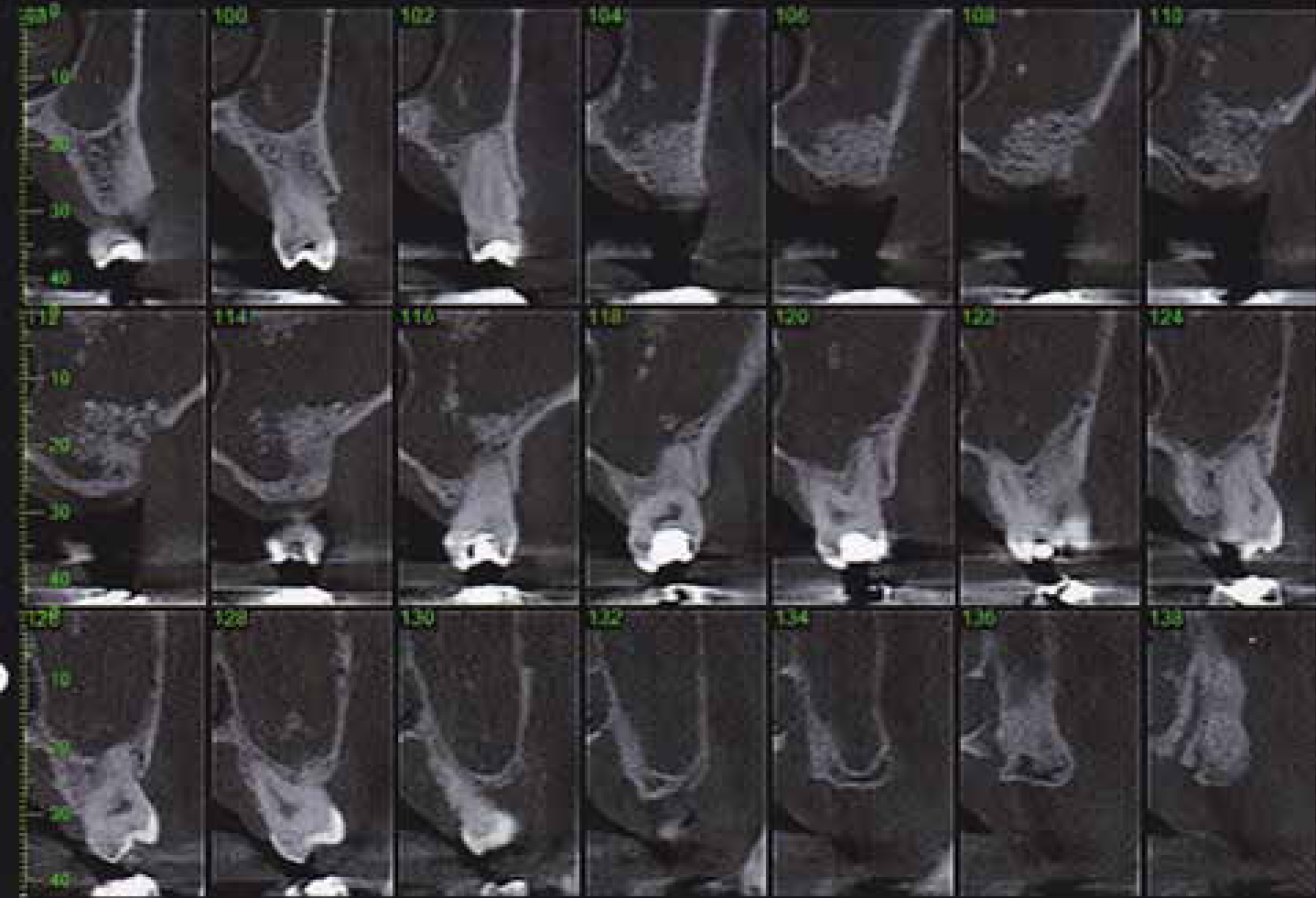
At consultation, a systematic extra-oral and intra-oral examination was performed. It was found that the left cheek was swollen with erythema. The zygomatic buttress was tender on palpation but no oro-antral communication was noted. Following the consultation, the patient was sent for a CBCT (Figures 1 and 2).
Figure 1. Coronal CBCT image showing bone graft material extending into the left maxillary antrum.Figure 2. Sagittal CBCT image showing bone graft material at the base of the maxillary sinus and floating up into the sinus.
The CBCT showed that there was extruded bone graft material into the maxillary sinus which had evidently resulted in left chronic maxillary sinusitis.
Treatment
An ENT colleague was consulted regarding the possibility of functional endoscopic sinus surgery to remove the bone graft. However, this was assessed to be an unsuitable option to remove all of the displaced material successfully. Therefore, a Caldwell-Luc approach under GA was deemed most appropriate to irrigate the sinus and remove the extruded graft material. A modified gingival crevicular incision was prepared from the upper left central incisor to the upper left second molar tooth. An anterior maxillary wall osteotomy window (approximately 1 cm in width) was used to access the maxillary sinus. Minimal debris was noted but the maxillary sinus lining was seen to be atrophied. On examination, there were no signs of acute infection. Following irrigation with saline and a 30° sinus endoscope, no further abnormal findings were noted. The incision was closed with resorbable sutures and clarithromycin was prescribed, 500 mg, BD for 14 days.
Outcome and follow-up
The patient was reviewed 1 and 7 months post-op. At the 1 month review, the patient complained of ‘occasional congestion’ but this was an improvement compared to the chronic sinusitis symptoms previously experienced. The patient also complained of ‘slight numbness’ of the upper left quadrant, although this had been improving also. On examination, no abnormalities were detected. At the 7 month review, the patient was asymptomatic and, on examination, the surgical site had completely healed. At this point, the patient was discharged. It is worth noting that, on contacting the patient a year later, the authors were informed that, due to the complications he had experienced with the sinus lift procedure, he had decided against implant placement.
Discussion
Sinus lift procedures are a relatively common and predictable method of increasing bone volume in the posterior maxilla.7 However, there are numerous complications associated with this technique. These predominantly consist of disturbed wound healing, haematoma, sequestration of bone, transient maxillary sinusitis and post-operative infection.8,9 Development of a sinus cyst is also a possible, but rare, complication of the sinus lift procedure.10
One of the most common serious complications is haemorrhage from branches of the maxillary artery, including anastomoses between the infra-orbital artery and the posterior superior alveolar artery, which is frequently located at the site in which the surgeon makes the bone window to access the antral cavity.11
Membrane perforation is another common complication of sinus lift procedures. Schwartz-Arad et al found that it occurred in 44% of patients who underwent a sinus lift procedure.12 A more recent systematic review by Al-Dajani reported a weighted incidence rate of 23.5%, ranging from 3.65 to 41.8%.13 However, infection of the bone graft secondary to membrane perforation is a rare occurrence. A systematic review of 24 studies showed a mean incidence of 2.9%.8
In this case, the graft material was displaced through the sinus membrane although, unfortunately, this was not realized by the surgeon at the time of surgery. Hence the graft material was free to move aroun the antrum. Aimetti et al observed that the presence of these foreign bodies created the conditions for initial inflammation and oedema of the mucosa, leading to reduced ventilation and mucociliary clearance.14
There are a number of predisposing factors to membrane perforation including:
Previous sinus pathology;
Irregularities of the sinus floor, eg due to root protrusions;
There are a number of systems available to minimize membrane perforation, including ultrasonics and piezoelectric techniques which may reduce incidence of perforation to 7%.16
Methods for checking for membrane perforation include direct visualization, and some clinicians advocate pinching the patient's nose and asking them to blow whilst checking the antrum for bubbles.
Management of the perforation is generally dependant on its size. Viňa-Almunia et al outlined various methods for repair of a perforation. For a small perforation, the possible management includes, sealing the perforation with a collagen membrane, securing it with a resorbable suture or fibrin glue, or allowing the membrane to fold over itself when lifting it. In the case of large perforations, many authors abandon the sinus lift completely, whilst others continue the procedure using a resorbable membrane in the perforation or placing a lamellar bone sheet.15
Given the potential complications to the sinus lift procedure, some surgeons prefer alternative techniques. These include; sinus tenting, ‘tilted’ or ‘angulated’ implants, zygomatic implants or using a short implant (4–8 mm long).17
It is worth noting that membrane perforation does not necessarily mean implant failure. Nooh reported a 98.4% implant survival rate when placing the implant in the posterior maxilla by intentionally perforating the Schneiderian membrane and protruding the implant up to 3 mm beyond the sinus floor in cases of reduced crestal bone height.18
In conclusion, a systematic clinical and radiographic examination must be completed before conducting a sinus lift procedure. In some cases, CBCT may be advisable, for example if there is suspicion of the presence of antral septa or pathology. The surgery itself must be conducted with care and using techniques or systems to minimize membrane perforation risk.
However, despite thorough treatment planning and careful surgery, complications can arise and it is imperative to advise patients on the relevant risks before undertaking treatment. In addition, checking for sinus membrane perforation should be part of peri-operative procedure and knowledge of how to manage it, should it occur, is essential.