Bowie P, McKay J, Dalgetty E, Lough M. A qualitative study of why general practitioners may participate in significant event analysis and educational peer assessment. Qual Saf Health Care. 2005; 14:185-189
Renton T, Master S. The complexity of patient safety reporting systems in UK dentistry. Br Dent J. 2016; 221:517-524 https://doi.org/10.1038/sj.bdj.2016.782
Renton T, Master S. Never say never: Never Events, NatSSIPs and the need for a new approach in dentistry. Faculty Dent J. 2016; https://doi.org/10.1308/rcsfdj.2016.141
Pemberton M. Developing patient safety in dentistry. Br Dent J. 2014; 217:335-337
Patient safety in dentistry Tara Renton Selina Master Mike Pemberton Dental Update 2024 44:10, 707-709.
Authors
TaraRenton
BDS, MDSc, PhD
Professor of Oral Surgery, King's College London; Honorary Consultant in Oral Surgery, King's College Hospital NHS Foundation Trust and Guy's and St Thomas' NHS Foundation Trust, London
Patient safety is the absence of preventable harm to a patient during the process of healthcare and is critical to the provision of a quality service. Many National Health Service (NHS) improvement initiatives have been developed in relation to patient safety, resulting in changes in culture, reporting and learning. These include the publication by the NHS England Surgical Never Events taskforce of ‘Standardize, educate, harmonize, commissioning the conditions for safer surgery’ in 2014 which was followed in 2015 by ‘National Safety Standards for Invasive Procedures (NatSSIPs)’. The principles identified in NatSSIPs are now being rolled out to local areas for their interpretation (Local Safety Standards for Invasive Procedures [LocSSIPs]).
CPD/Clinical Relevance: The aim of this article is to inform and update the reader on recent NHS England patient safety initiatives as applicable to dentistry, specifically the development of an example LocSSIP for wrong site extraction.
Article
Dentistry provides one of the NHS's highest volume of surgical interventions. Unlike other surgical procedures, the vast majority of these surgical interventions occur under local anaesthesia on conscious and often anxious patients. This high volume, often complex, work creates the opportunity for mistakes to happen, which can be devastating for both the patient and the clinical team. Wrong site surgery in dentistry may not always cause significant physical harm to the patient, such as the loss of a limb, but it is a source of injury and stress and may be symptomatic of problems in the clinical systems and processes of the environment within which it occurs. By a better understanding of why patient safety incidents, including wrong site surgery, occur it should be possible to improve patient safety systems and processes to reduce the risk of future harm.
By definition, patient safety is the absence of preventable harm to a patient during the process of healthcare, and the discipline of patient safety is the co-ordinated efforts to prevent harm from occurring to patients, caused by the process of healthcare itself.1
There have been several significant developments in the NHS since the Francis report (The Mid Staffordshire NHS Foundation Trust Public Enquiry) and these NHS patient safety key initiatives are summarized in Table 1.2 Many of these developments have been in response to a number of reviews and reports which have highlighted events which were potentially preventable and where there has been a clear lack of adherence to basic patient safety recommendations. A significant cultural change has taken place in secondary care with common use of the World Health Organization (WHO) checklist3 and the development of initiatives by the National Patient Safety Agency (an agency now succeeded and placed within NHS Improvement), ensuring reporting of serious and strategic events for NHS Trusts, maximizing learning from notifiable events and improving patient safety. However, many of these initiatives have not yet reached primary care medicine or dentistry.4
The Francis Report – Response to North Staffordshire
2013
Berwick Report
2013
Hard Truths government response – The Journey to PuttingPatients First
2013
King's Fund Response
2013
The NHS commissioning Board set up a task force to look at surgical safety, resulting in the publication Standardize, Educate, Harmonize: Commissioning the Conditions for Safer Surgery
2014
The revised Never events policy framework reassessed a subset of serious incidents and, therefore, this policy should always be read in conjunction with the Serious Incident Framework (https://www.england.nhs.uk/)2
2015
Key initiatives3The National Safety Standards for Invasive Procedures (NatSSIPs)Launching a new National Patient Safety Alerting System (NaPSAS)The monthly publishing of data on never eventsPublishing of key patient safety indicators by hospital on My NHS (NHS Choices)Launching the Patient Safety CollaborativeDeveloping an initiative with the Health Foundation to recruit a network of ‘5,000 Patient Safety Fellows'
2015
As of 1 April 2016, Patient Safety is now part of NHS Improvement.
2016
Launch of generic LocSSIPs for Wrong Site Extraction
2017
In 2009, the National Patient Safety Agency in England introduced a list of ‘Never Events’ directly related to patient safety to encourage the implementation of measures to avoid them.5 Since 2012, ‘wrong tooth extraction’ has been included as a ‘Never Event’ under the theme of ‘wrong site surgery’.6 In response to the ongoing occurrence of ‘Never Events’, the NHS Commissioning Board set up a task force to look at improving surgical safety, which resulted in the publication ’Standardize, educate, harmonize: commissioning the conditions for safer surgery’ in February 2014.7 This is the final report of NHS England's surgical Never Events task force and includes a literature review and survey of 600 practitioners, which was requested in order to examine the three most common Never Events including:
Wrong site surgery (which includes operating on the wrong site, carrying out the wrong procedure, and operating on the wrong patient);
Wrong prosthesis (for example, the wrong size components in a replacement hip);
Retained foreign object (the most frequently retained foreign object is surgical swabs, but this also includes surgical instruments).
The task force was also asked to:
Analyse the reasons for the persistence of these three never events in surgery;
Consider whether the World Health Organization checklist was helping to reduce them;
Make recommendations about what NHS England, with its responsibilities for commissioning, could do to reduce them further.
The main recommendations of the report cover three themes:
Standardize – The development of high-level national standards of operating environment processes that will support all providers of NHS-funded care to develop and maintain their own more detailed, standardized, local procedures. The report also recommends the establishment of an Independent Surgical Investigation Panel to review selected serious incidents externally;
Educate – Consistency in training and education of all staff in the operating theatres, development of a range of multimedia tools to support implementation of standards and support for surgical safety training including human factors; and
Harmonize – Consistency in reporting and publishing of data on serious incidents, dissemination of learning from serious incidents and concordance with local and national standards taken into account through regulation.
In 2015, following this report, a further group was tasked with creating the standards of high-level operating environment processes. The resultant report published by NHS Improvement in 2015 was entitled The National Safety Standards for Invasive Procedures (NatSSIPs).2 The aim of this was to collate national and local learning from the analysis of Never Events, Serious Incidents and Near Misses and to draw out a set of recommendations that would enable the provision of safer care for patients undergoing invasive procedures.
Before describing the development of NatSIPPs into Local Safety Standards for Invasive Procedures (LocSIPPs), it would be beneficial to review some of the definitions and terminology of each individual type of event in order to clarify how events are classified, which in turn should guide those involved in how to manage the event (including involvement of the patient and relatives/carers), how to report it, and how the whole team can learn from it to ensure a reduction of risk of recurrence.
Patient safety incidents (PSIs)
By definition, a PSI is any unintended or unexpected incident which could have or did lead to harm for one or more patients receiving NHS care. PSIs include:
Near Misses
Never Events
Notifiable Safety Incidents
Near Misses
Near Misses (no harm) provide the richest opportunity to learn and improve patient safety. The concept of a ‘near miss’ is taken from a corporate model Heinrich's Safety Triangle, which places Near Miss events at the base of the triangle, accidents in the middle and, finally, fatalities at the top. Near Misses offer learning opportunities in the absence of actual harm occurring. The assumption is that, by analysing, learning lessons and eliminating Near Miss events alone, accidents and fatalities will eventually disappear. Medical studies have reported that ‘near miss’ experiences are an important reminder to use checklists in surgery and, systematically and relentlessly, to seek to find ways to reduce risk.
Never Events
The revised Never Events Framework of March 20158 reassessed a subset of serious incidents and, therefore, this policy should always be read in conjunction with the Serious Incident Framework (2016).9
The updated criteria for Never Events describe a particular type of serious incident which meets all the following criteria:
They are wholly preventable where guidance or safety recommendations that provide strong systematic barriers are available at a National Level and should have been implemented by all healthcare providers.
Each Never Event has the potential to cause serious patient harm or death (although serious harm or death is not required to have happened to meet the category of Never Event).
There is evidence that it has occurred in the past (ie it is a known source of risk).
It can be easily defined, identified and continually measured. (This requirement helps minimize disputes around classification and ensures focus on learning and improved patient safety).
It is anticipated that the Never Event list will be reviewed on a regular basis.
What is a Never Event in dentistry?
The Revised Never Events policy and framework 2015 from NHS England8 modified the list of Never Events related to dentistry to the following three incidents:
Wrong site surgery, ie a surgical intervention performed on the wrong patient or the wrong site, including wrong tooth extraction of a permanent (adult) tooth even if re-implanted. It includes interventions that are considered surgical but are done outside of a surgical environment, eg a biopsy.
Wrong implant/incorrect placement of dental implant.
Retained foreign object.
Notifiable Safety Incidents
Notifiable Safety Incidents (NSIs) include events where the patient experiences moderate to severe harm.10 Definitions of patient harm are outlined in Table 2.11 The terminology for these varies but includes; NSIs, Serious Events (SEs), Serious Untoward Events (SUEs), Serious Adverse Events (SAEs) and Serious Adverse Incidents (SAIs). Notifiable Safety Incidents (NSIs) for health service bodies are defined as intended or unexpected incidents that, in the reasonable opinion of a healthcare professional, could result in, or appears to have resulted in, one of the following:
Death;
Severe harm;
Moderate harm or prolonged psychological harm.
Harm to the patient may be low/moderate/severe
Moderate harm is defined as:
▪ Requires a moderate increase in treatment;
▪ Significant but not permanent harm;
▪ Moderate increase in treatment means unplanned return to surgery or a re-admission, prolonged episode of care, extra time in hospital or as an outpatient, cancelling of treatment or transfer to another treatment area.
Severe physical harm is defined as:
▪ Permanent lessening of a bodily sensory motor psychologic or intellectual function;
▪ Not related to the natural course of the service user's underlying illness or condition.
Severe psychological harm is defined as:
▪ Psychological harm which a person has experienced, or is likely to experience, for a continuous period of at least 28 days
What happens after a patient safety incident, including Notifiable and Never Events?
The main objective of the post incident process is to minimize any repetition of the event and to maximize patient safety. This process involves:
Recognition and Duty of Candour;
Reporting;
Learning from the event using Key Lines of enquiry and Root Cause Analysis;
Implementing necessary changes to faults in systems and processes;
Providing support for all the staff involved.
Recognition
The Duty of Candour regulations ensure that providers are open and transparent with people who use services and other ‘relevant persons’ (people acting lawfully on their behalf) in relation to care and treatment.12 The statutory duty requires reporting of all serious events (including Never Events) and notification of the patient, with a prompt apology.12 If a member of staff is aware of an incident having taken place, then efforts should be made to encourage the staff involved to report the incident, but if they are reluctant to do this, then the witness is obliged to report based upon Duty of Candour.12,13,14 It also sets out some specific requirements that providers must follow when things go wrong with care and treatment, including informing people about the incident, providing reasonable support, providing truthful information and an apology.
Reporting
Patient safety incident event notification must be made by all services registered under the Health and Social Care Act (HSCA),13 including NHS Trusts, independent healthcare, adult social care, primary dental care and independent ambulance providers.12,13 From 1 April 2010, it became mandatory for NHS Trusts in England to report all serious patient safety incidents to the Care Quality Commission.14,15 All incidents resulting in death or severe harm should be reported to the National Reporting and Learning System (NRLS),16,17,18 and to the Strategic Executive Information System (StEIS),17 which captures all Serious Incidents and forwards reports onto the Care Quality Commission (CQC).19,20 All NHS primary care staff have a Duty of Candour statutory duty since April 2015 to recognize and report serious events including Never Events.21 However, being open is not enough. When things go very wrong, patients are entitled to candour, but they also need caring and compassionate support, a credible and independent investigation into what happened, a thoughtful approach to restitution, and proper accountability.
Importantly, Never Events are not over when a patient leaves the operating environment. The task force10 looked carefully at the support that patients and their loved ones need when Never Events and other serious incidents happen. Indeed, the staff involved most are often severely affected by events and may require additional support.22
The way in which notifications are made will depend on their nature and the type of service. The process differs slightly for NHS Trusts compared with other providers. For NHS Trusts, the requirement to report incidents is typically met by reporting incidents to the CQC20,21 and the NRLS.16,17
The CQC has statutory powers to take regulatory action over non-compliance with the Duty of Candour. These include refusal or removal of registration, warnings, special measures, fines and, in certain circumstances, criminal proceedings.20,21 Currently, for the Serious Incident Framework, it is stated that there is nothing to stop independent healthcare providers reporting to the NRLS,16 but it is not mandatory and they still need to report to CQC.20,21 NHS Improvement undertakes open reporting of national Never Event occurrence, highlighting that dental wrong site extractions are the most common wrong site surgery Never Event reported in England.6,23 Despite wrong site extraction (WSE) being the most common reported Never Event (20–40% monthly reported figures),6,23 underreporting is significant in dentistry, likely in part due to lack of awareness of the benefits of reporting in enhancing patient safety, complex reporting systems and a poor culture of openness and regulatory support.24,25,26
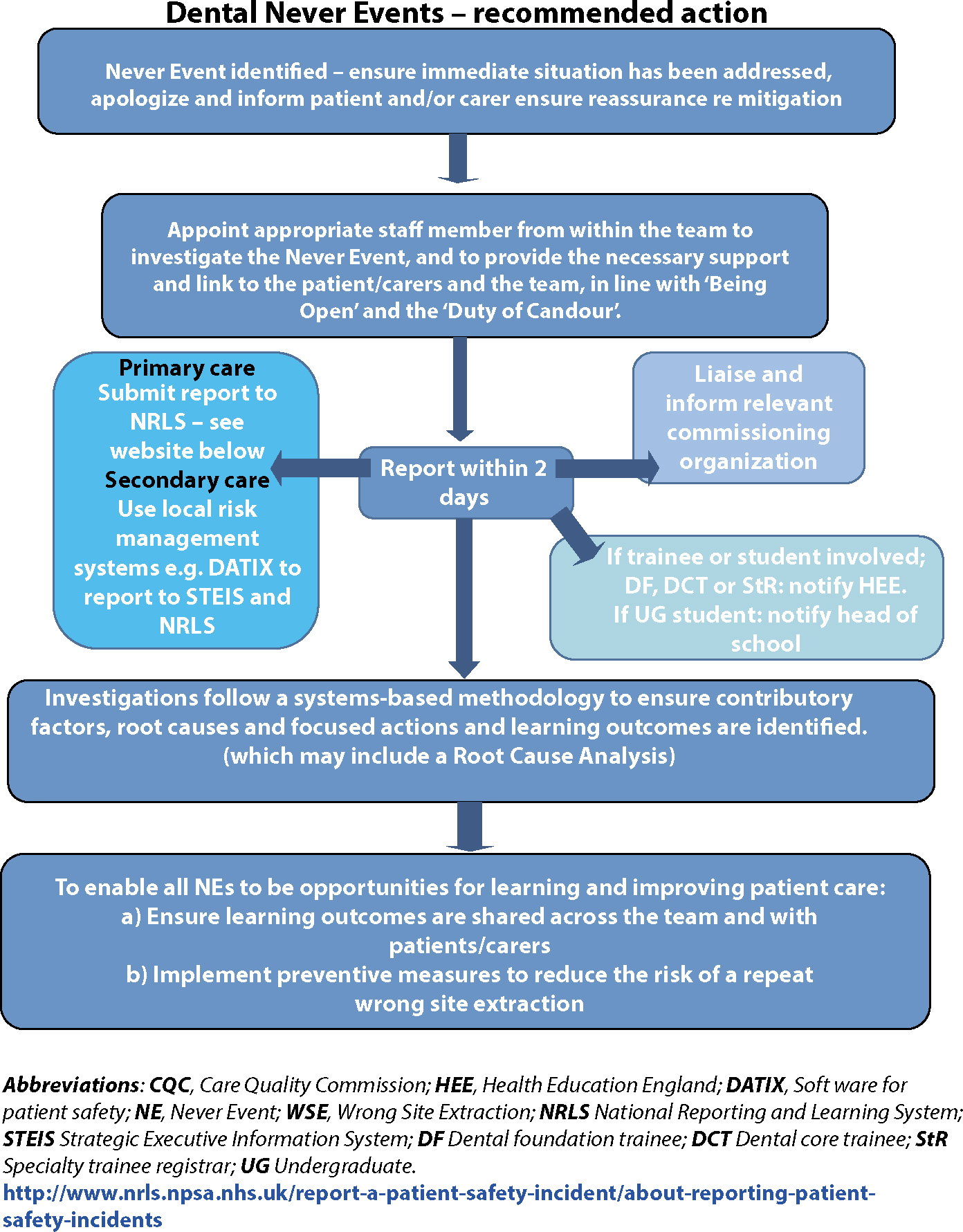
How to report a Never Event is summarized in Figure 1. There is intention to rationalize and simplify reporting systems from primary care, by NHS England and the CQC and Figure 1 summarizes the current reporting systems accessible to primary dental care.
Figure 1. Flow chart for reporting a Never Event (wrong site surgery) in dentistry.
Effective practice governance mechanisms should be established to ensure:
Timely reporting and liaison with their commissioning bodies (NHS patients);
That the incident is reported to the CQC;
Compliance with reporting and liaison requirements with agencies such as: NHS Improvement (applies to Hospital Trusts); the Care Quality Commission (CQC) and other bodies dependent upon the type of notification (Public Health England, the Health and Safety Executive, and coroners)
Learning from the event using Key Lines of enquiry to investigate and root cause analysis
In line with the Never Events policy framework, providers of NHS-funded care should conduct investigations which follow a systems-based methodology to ensure contributory factors, root causes and focused actions and learning are all identified.27 Investigation and analysis of a Never Event should collect information regarding not only the technical aspects of what went wrong, but also the human factors that may have contributed to the Never Event. Managing the response to Never Events is a critical component of corporate and clinical governance.
Implementing the necessary changes to faults in the systems and processes
Demonstration of learning from Near Misses and Never Events will improve patient safety. This should include the following:
A particular focus on the system changes that have been made to reduce the probability of recurrence;
How learning has been shared at all levels within the organization, and also at an external level, demonstrating a strong and supportive culture, which supports the team involved in a Never Event, enabling the required learning from the incident and facilitating improvements in the quality of practice. At an individual level, the practitioner should be logging the incident and providing a reflection and learning outcomes for their Appraisal/Portfolio documents, where relevant.
Providing support for all the staff involved
An open and just culture is essential to facilitate and enable reporting and learning from Never Events with resultant improvement in patient safety. The dental profession is facing high levels of complaints and litigation rates, leaving teams feeling intimidated. The regulation of dentistry is changing and the regulators are becoming aware of the adverse impact of the existing culture.
Importantly, all those involved in an incident need appropriate support, both patients10 and staff.22 How professionals deal with the Never Event will affect patients, colleagues, and the systems we design to keep patients safe. Therefore, professionals need help to manage the situation well, not only for their own benefit, but also to build a safer culture of care.22
What developments are taking place in primary care dentistry?
The development of Local Safety Standards for Invasive Procedures (LocSSIP)
The NatSIPPs publication required that organizations review their current local processes for invasive procedures and ensure that they are compliant with the new national standards.2 It was suggested that this will be done by organizations working in collaboration with staff to develop their own set of Local Safety Standards for Invasive Procedures (LocSSIPs). The aim was not in any way to replace the existing WHO Surgical Checklist,3 but rather to enhance it by looking at additional factors, such as the need for education and training. The development of LocSSIPs has been encouraged for all high volume surgical procedures.2
Definition of invasive procedure
What is an invasive procedure?2 In the National Safety Standards for Invasive Procedures it defines an ‘interventional procedure’ as a procedure used for diagnosis or for treatment that involves:
Making a cut or a hole to gain access to the inside of a patient's body;
Gaining access to a body cavity (such as the digestive system, lungs, womb or bladder) without cutting into the body;
Using electromagnetic radiation (which includes X-rays, lasers, gamma rays and ultraviolet light), eg using a laser to treat eye problems.
The Revised Never Events Policy and Framework and the NatSSIPs document both have detailed FAQ sections which are designed to provide guidance on interpretation. The guidance in the NatSIPPs document is that, if the procedure has the potential to lead to a Never Event, then it falls under the remit of the NatSIPPs.2
Development of a LocSSIP toolkit for dental extraction
A subgroup of the NatSSIPs committee was formed representing all appropriate stakeholders in dentistry, to develop a generic LocSSIPs and toolkit that can be modified according to local needs. The main aim of the LocSSIP working group was to assist the development of locally adapted safety standards by providing templates and guidance and to encourage the uptake of generic recommendations around NatSSIPs. The development of LocSSIPs and toolkit aims to provide guidance on recognizing, reporting and learning from wrong site surgery.
How are LocSSIPs connected to Never Events in dentistry?
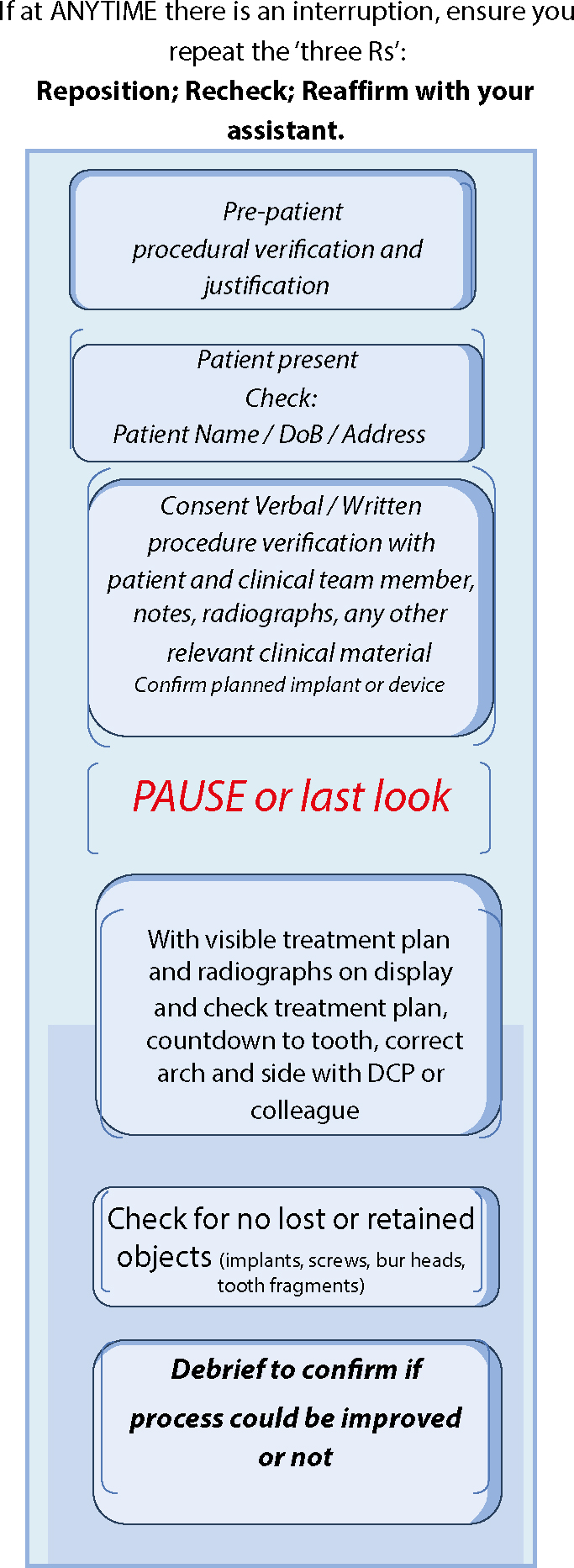
For all invasive procedures, a Local Safety Standard for Invasive Procedures (LocSSIP) should be developed and implemented, based on the principles outlined in the NatSSIPs document. For example; Wrong Site Extraction is a Never Event and hence there is a need for developing a template LocSSIP that can be used, or adapted for use, in clinical dental practice in all settings where NHS patients are treated. The template ‘Dental extraction LocSSIPs individual patient pathway’ (Figure 2) provides a simple example. Providers are encouraged to develop LocSSIPs.28
Figure 2. Example dental extraction LocSIPPs individual patient pathway.
How are LocSSIPs applied?
The example ‘Dental extraction LocSSIPs individual patient pathway’ provides an outline of good practice for the dental team when undertaking dental extractions and related procedures (Figure 2). By ‘PAUSING’ (for confirmation) with a minimum of 2 people and routinely rechecking mid procedure, errors can be minimized. Errors are more likely to happen with interruptions, which can be commonplace in the dental surgery, so if distractions do occur, recheck the treatment plan (using displayed surgical plan and X-ray) and reaffirm with your assisting member of staff before continuing. The ultimate responsibility for wrong tooth extraction remains with the dentist. Identification of teeth is outside the GDC core Scope of Practice for dental nurses. However, by utilizing an empowered and experienced dental nurse as an assisting member of staff in all stages of the pathway when appropriate, this will engender the correct team mind-set and approach to improving patient safety.
What resources are available in the LocSSIPs Toolkit?
The LocSSIP Toolkit for Wrong Site Extraction, includes a number of useful documents:29
Introduction to LocSSIP for Wrong Tooth Extraction;
Frequently Asked Questions;
Example patient pathway (to reduce risk of Wrong Tooth Extraction);
Flow chart outlining recommended action if a Wrong Tooth Extraction occurs (including key information about reporting);
An Exemplar depicting a typical scenario of a Wrong Tooth Extraction which outlines risk factors and, also, recommended actions;
A section on ‘Learning from Never Events’ plus a template for a Learning log where the learning from the incident can be logged, eg for Appraisal/Portfolio;
A list of all the groups who contributed to the LocSIPP documentation.
Conclusion
In summary, unless patient safety6 awareness is improved in dentistry and the recognition and reporting of incidents is encouraged, improvement in dental patient safety will be limited.23 It is recognized that the reporting systems for incident reporting for dentistry are obscure and complicated.24 Pemberton highlighted that patient safety in dental practice requires several elements including:26
Building a safety culture;
Identifying threats to patient safety by incident reporting;
Learning and reporting;
Communication and education in patient safety.
The LocSSIP for the dental extraction toolkit aims to start the process of improving awareness of Patient Safety Incidents in dentistry, reporting and learning from these events and, hopefully, to provide simplified guidance for those who are unfortunate enough to have been involved in a Wrong Site Extraction. LocSSIPs for dental extraction is supported by the NHS in England, the General Dental Council and the Care Quality Commission. In dental practice, the dental team will need to develop and promote a patient safety culture led by the senior clinician and/or practice manager who needs to provide a supportive environment where learning is encouraged after safety incidents. The CQC will expect to see evidence of incident and near miss recognition and reporting, using a log book with evidence of learning from these events. In addition, evidence of team training and human factor training is essential. It is hoped that, with the uptake of this LocSSIP toolkit, there will be improved knowledge and good practice in relation to exodontia, together with an improved culture of patient safety in dentistry overall.
The authors gratefully acknowledge all colleagues in the subgroup of the NatSIPPs who helped develop the LocSIPPs ‘Wrong Site Extraction’ documentation.