Garg D, Palaskar S, Shetty VP, Bhushan A. Adenomatoid odontogenic tumor – hamartoma or true neoplasm: a case report. J Oral Sci. 2012; 51:155-159
Handschel JG, Depprich RA, Zimmermann AC, Braunstein S, Kübler NR. Adenomatoid odontogenic tumor of the mandible: review of the literature and report of a rare case. Head Face Med. 2012; 1
Buchner A, Sciubba JJ. Peripheral odontogenic tumours: a review. Oral Surg Oral Med Oral Pathol. 2012; 63:688-697
Konouchi H, Asaumi J, Yanagi Y, Hisatomi M, Kishi K. Adenomatoid odontogenic tumor: correlation of MRI with histopathological findings. Eur J Radiol. 2012; 44:19-23
Barnes L, Eveson JW, Reichart P, Sidransky D. World Health Organization Classification of Tumours: Pathology and Genetics, Head and Neck Tumours.Lyon: IARC Press; 2005
Larson A, Swartz K, Heikinheimo K. A case of multiple AOT-like jawbone lesions in a young patient – a new odontogenic entity?. J Oral Pathol Med. 2012; 32:55-62
Vitrus R, Meltzer JA. Repair of a defect following the removal of a maxillary adenomatoid odontogenic tumor using guided tissue regeneration. A case report. J Periodontol. 2012; 67:46-50
Blumenthal NM, Mostofi R. Repair of an intrabony defect from an adenomatoid odontogenic tumor. J Periodontol. 2012; 71:1637-1640
Berglundh T, Persson L, Klinge B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J Clin Periodontol. 2012; 29:197-212
Iizuka T, Häfliger J, Seto I, Rahal A, Mericske-Stern R, Smolka K. Oral rehabilitation after mandibular reconstruction using an osteocutaneous fibula free flap with endosseous implants. Factors affecting the functional out-come in patients with oral cancer. Clin Oral Implants Res. 2012; 16:69-79
Chan MF, Hayter JP, Cawood JI, Howell RA. Oral rehabilitation with implant-retained prostheses following ablative surgery and reconstruction with free flaps. Int J Oral Maxillofac Implants. 2012; 12:820-827
Schepers RH, Slagter AP, Kaanders JH, van den Hoogen FJ, Merkx MA. Effect of postoperative radiotherapy on the functional result of implants placed during ablative surgery for oral cancer. Int J Oral Maxillofac Surg. 2012; 35:803-808
Barber AJ, Butterworth CJ, Rogers SN. Systematic review of primary osseointegrated dental implants in head and neck oncology. Br J Oral Maxillofac Surg. 2012; 49:29-36
Brad NW, Douglas DD, Carl AM, Jerry BE. Oral and Maxillofacial Pathology, 2nd edn. Michigan, USA: WB Saunders, Elsevier; 2005
Reichart PA, Philipsen HP. Adenomatoid odontogenic tumor. In: Reichart PA (ed). London: Quintessence Publishing Co Ltd; 2004
Kramer IRH, Pindborg JJ, Shear M. WHO International Histological Classification of Tumours: Histological Typing of Odontogenic Tumours, 2nd edn. Berlin: Springer Verlag; 1992
Philipsen HP, Srisuwan T, Reichart PA. Adenomatoid odontogenic tumor mimicking a periapical (radicular) cyst: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2012; 94:246-248
Chuan-Xiang Z, Yan G. Adenomatoid odontogenic tumor: a report of a rare case with recurrence. J Oral Pathol Med. 2012; 36:440-443
Philipsen HP, Samman N, Ormiston IW, Wu PC, Reichart PA. Variants of the adenomatoid odontogenic tumor with a note on tumor origin. J Oral Pathol Med. 2012; 21:348-352
Yilmaz N, Acikgoz A, Celebi N, Zengin AZ, Gunhan O. Extrafollicular adenomatoid odontogenic tumor of the mandible: report of a case. Eur J Dent. 2012; 3:71-74
Saluja R, Kaur G, Singh P. Aggressive adenomatoid odontogenic tumor of mandible showing root resorption: a histological case report. Dent Res J (Isfahan). 2012; 10:279-282
Shivali V, Pandey A, Khanna VD, Khanna P, Singh A, Ahuja T. A rare case of extrafollicular adenomatoid odontogenic tumour in the posterior region of the mandible: misdiagnosed as residual cyst. J Int Oral Health. 2012; 5:124-128
Bhandari N, Kothari M. Adenomatoid odontogenic tumour mimicking a periapical cyst in pregnant woman. Singapore Dent J. 2012; 31:26-29
Jivan V, Altini M, Meer S, Mahomed F. Adenomatoid odontogenic tumor (AOT) originating in a unicystic ameloblastoma: a case report. Head Neck Pathol. 2012; 1:146-149
Batra P, Prasad S, Parkash H. Adenomatoid odontogenic tumour: review and case report. J Can Dent Assoc. 2012; 71:250-253
Narayanan VS, Naidu G, Ragavendra R, Mhaske-Jedhe S, Haldar M. Adenomatoid odontogenic tumor of the mandible with unusual radiographic features: a case report. Imaging Sci Dent. 2012; 43:111-115
Bhatt R, Dave J, Nalawade TM, Mallikarjuna R. Adenomatoid odontogenic tumour in mandible in a 14-year-old boy. BMJ Case Rep. 2012; 8
Manjunatha BS, Harsh A, Purohit S, Naga MV. Adenomatoid odontogenic tumor associated with a dentigerous cyst. J Cancer Res Ther. 2012; 11
Carini F, Francesconi M, Saggese V, Monai D, Porcaro G. Implant-supported rehabilitation of a patient with mandibular ameloblastoma. Ann Stomatol (Roma). 2012; 3:21-25
Oteri G, Ponte FS, Pisano M, Cicciù M. Five years follow-up of implant-prosthetic rehabilitation on a patient after mandibular ameloblastoma removal and ridge reconstruction by fibula graft and bone distraction. Dent Res J (Isfahan). 2012; 9:226-232
Minichetti JC, D'Amore JC, Schwarz E. Complete oral rehabilitation of a postresection ameloblastoma patient: a clinical case report. J Oral Implantol. 2012; 37:735-744
Bodard AG, Bémer J, Gourmet R, Lucas R, Coroller J, Salino S, Breton P. Dental implants and free fibula flap: 23 patients. Rev Stomatol Chir Maxillofac. 2011; 112:e1-4
An adenomatoid odontogenic tumour (AOT) is an uncommon, benign, slow-growing tumour which is usually located in the anterior region of the maxilla without pain and represents 2.2–7.1% of all odontogenic tumours. An AOT often causes expansion of surrounding bone and displacement of adjacent teeth. The tumour is usually associated with an unerupted tooth, frequently canines or lateral incisors. Radiographically, they usually appear unilocular and may contain calcifications, and frequently resemble other odontogenic lesions such as dentigerous cysts or ameloblastoma. Treatment is conservative and the prognosis is excellent. The surgical management and implant-supported prosthodontic rehabilitation of an extrafollicular AOT case that occurred in the left premolar region of the mandible, causing painless swelling in a 25-year-old female patient, is presented. To the best of the authors' knowledge, this is the first extrafollicular type AOT case rehabilitated with dental implants following the total surgical enucleation.
CPD/Clinical Relevance: This article illustrates the healing capacity of jaw bones, which enables subsequent implant placement.
Article
An adenomatoid odontogenic tumour (AOT) is a relatively uncommon distinct odontogenic neoplasm that was first described by Steensland in 1905.1 This tumour is a hamartomatous, non-invasive lesion with a slow but progressive growth, accounting for only 2.2–7.1% of all odontogenic tumours.2 It is most often diagnosed in the second decade of life and about twice as many women are affected as men. The AOT is located in the maxilla twice as often as in the mandible and the anterior jaw is much more affected than the posterior area.3
According to Philipsen and Reichart, the AOT appears in three clinico-topographic variants: follicular (or pericoronal) (73%), extrafollicular (or extracoronal) (24%) and peripheral (3%). Both follicular and extrafollicular are intrabony.4 Clinical features generally focus on complaints regarding a missing tooth. The lesion usually presents as an asymptomatic swelling which is slowly growing and often associated with an unerupted tooth.5 Although larger lesions have been reported in the literature, the tumours are usually in the dimensions of 1.5–3 cm.4
The radiographical findings of AOT frequently resemble other odontogenic lesions, such as dentigerous cysts, calcifying odontogenic cysts and tumours, ameloblastomas and odontogenic keratocysts.6,7 Whereas the follicular variant shows a well-circumscribed unilocular radiolucency associated with the crown and often part of the root of an unerupted tooth, the radiolucency of the extrafollicular type is located between, above or superimposed upon the roots of erupted permanent teeth.4,7 However, the rare peripheral variant occurs primarily in the gingival tissue of tooth-bearing areas and may show some erosions of the adjacent cortical bone.5,7,8
The histological typing of the World Health Organization (WHO) defined the AOT as a tumour of odontogenic epithelium with duct-like structures and varing degrees of inductive change in the connective tissue.7 The tumour may be partly cystic and, in some cases, the solid lesion may be present only as a mass in the wall of a large cyst. Immunohistochemically, the classical AOT phenotype is characterized by a cytokeratin (CK) profile similar to a follicular cyst and/or oral or gingival epithelium, based on positive staining with CK5 CK17 and CK19.9
Conservative surgical enucleation is the treatment modality of choice. For periodontal intrabony defects caused by AOT, guided tissue regeneration with membrane technique is suggested after complete removal of the tumour. Recurrence of AOT is exceptionally rare.10,11
Dental implants are increasingly being used to replace missing teeth and the survival rates have approached 90–95% in recent years.12 The benefits of implant-retained prosthesis have been recognized for several years. Dental implants may improve denture retention and stability without unnecessary loading of vulnerable mucosa and they are an important component of multidisciplinary rehabilitation for patients after surgical resection. Function, comfort, aesthetics and quality of life can be improved.13,14,15,16 The surgical management, implant-supported prosthodontic rehabilitation and six years follow-up of an extrafollicular AOT case is presented.
Case report
A 25-year-old female was referred to the Department of Oral and Maxillofacial Surgery by her general dental practitioner with a complaint of a painless swelling in the premolar region of the left mandible that had begun six months earlier. The swelling had gradually increased in size over the previous two months but there was no anaesthesia or paraesthesia of the lower lip or jaw and there was no history of trauma. Extra-oral examination of the patient revealed a vague swelling in the mandibular left premolar region which was non-tender on palpation. There was no local rise in temperature and the skin over the swelling and the surrounding area appeared normal.
Intra-oral examination revealed a painless swelling extending from mandibular left canine to second premolar, causing a mild buccolingual expansion. The consistency was variable, ranging from rubbery to hard in nature, there was no tenderness on palpation and the overlying mucosa was normal in appearance. The lingual tipping of the crown of the mandibular left first premolar was remarkable and the teeth LL3, LL4 and LL5 revealed a negative response to a vitality test (Figure 1).
Figure 1. A painless swelling extending from mandibular left canine to second premolar, causing a mild buccolingual expansion and lingual tipping of the crown of the mandibular left first premolar.
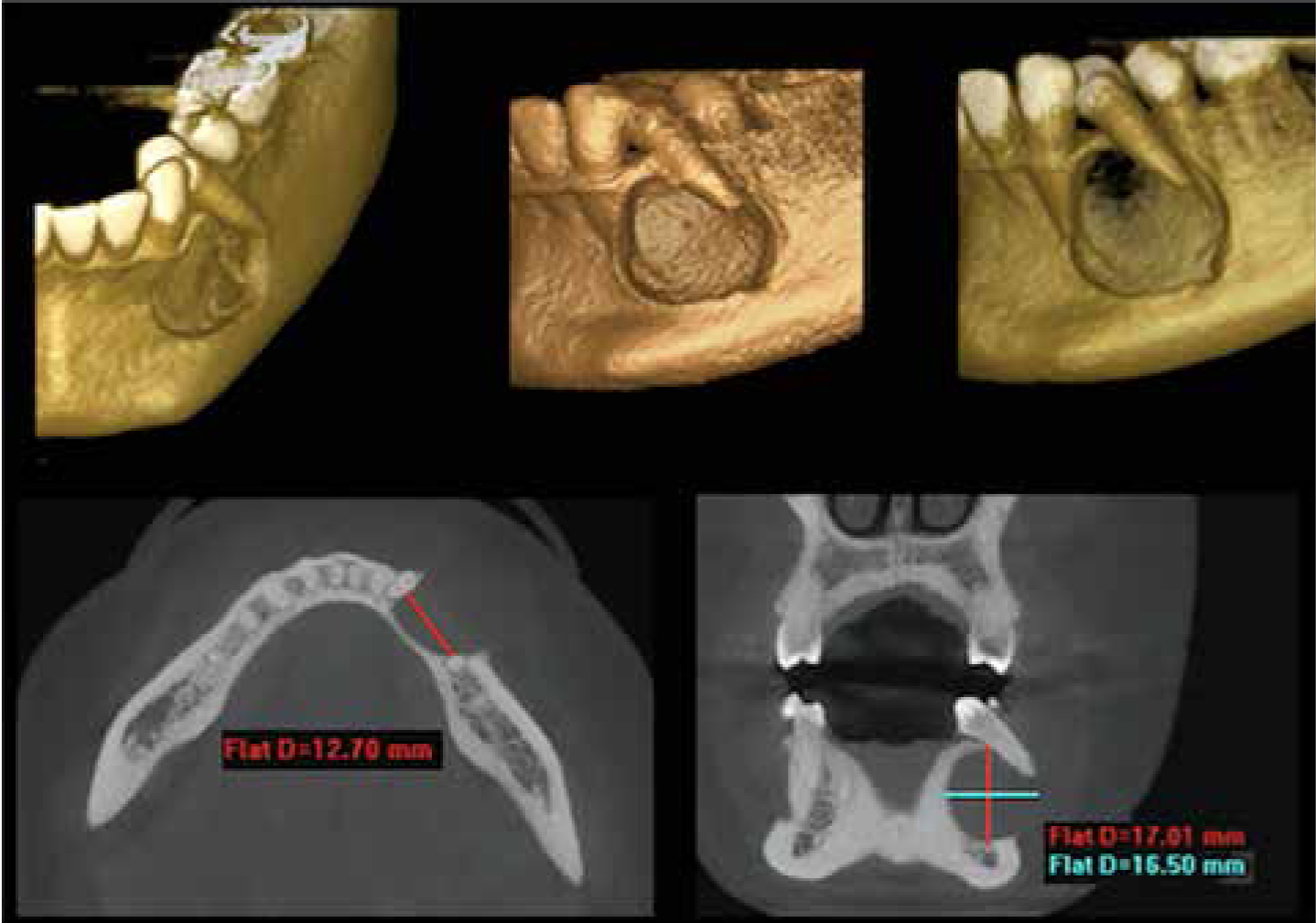
Radiographical evaluation revealed a well-circumscribed, round, unilocular radiolucency between the roots of the mandibular left canine and second premolar. No root resorption was seen but the lack of an intact periodontal ligament and lamina dura was noticed (Figure 2). Computed tomography (CT) scans demostrated remarkable buccolingual expansion with loss of buccal cortex. The dimensions of the lesion were 17.01 x16.50 x12.70 mm, radiographically (Figure 3). On the basis of first clinical and radiological examinations, the pre-diagnosis of radicular cyct was considered.
Figure 2. A well-circumscribed, round, unilocular radiolucency extending throughout the mandibular left canine to the mandibular second premolar with the lack of an intact periodontal ligament and lamina dura.Figure 3. CT scans demonstrated remarkable buccolingual expansion with loss of buccal cortical plate, thinning of lingual cortical plate and the tipping of mandibular left first premolar.
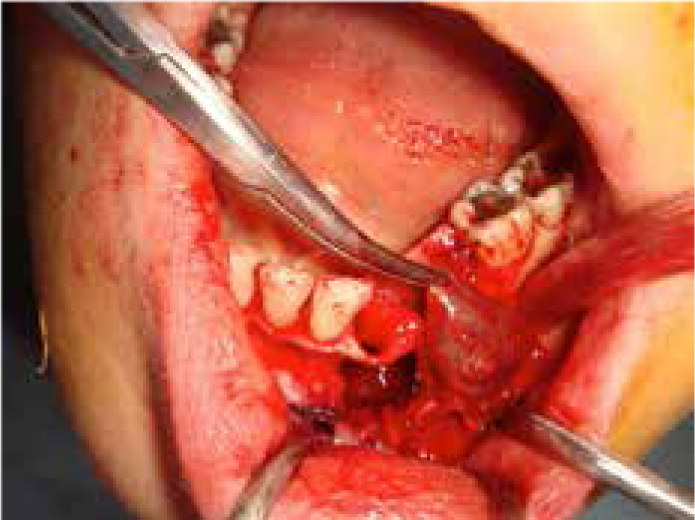
Surgical enucleation of the lesion was planned and the patient was informed about the surgical procedures and possible risks of the operation. Informed consent was taken and the patient underwent surgery with local anaesthesia. A mucoperiosteal flap from the mandibular right central incisor to the left first molar was reflected to expose the lesion. The buccal cortical plate had several areas of complete resorption and the lingual cortical plate was very thin. The lesion was totally enucleated, preserving mental nerve and the teeth LL3, LL4 and LL5 were extracted (Figure 4). The surrounding bone margins were corrected with tungsten burr, irrigated with saline solution and the flap was sutured with 3/0 silk stiches. The patient was prescribed an antibiotic (amoxicillin 1 g, 2x1, 5 days, orally), an analgesic (naproxen sodium 550 mg, 2x1, 5 days, orally), and an antiseptic mouthwash (4% chlorhexidine gluconate 10 ml, 3x1, 5 days).
Figure 4. The lesion was totally enucleated, preserving the mental nerve.
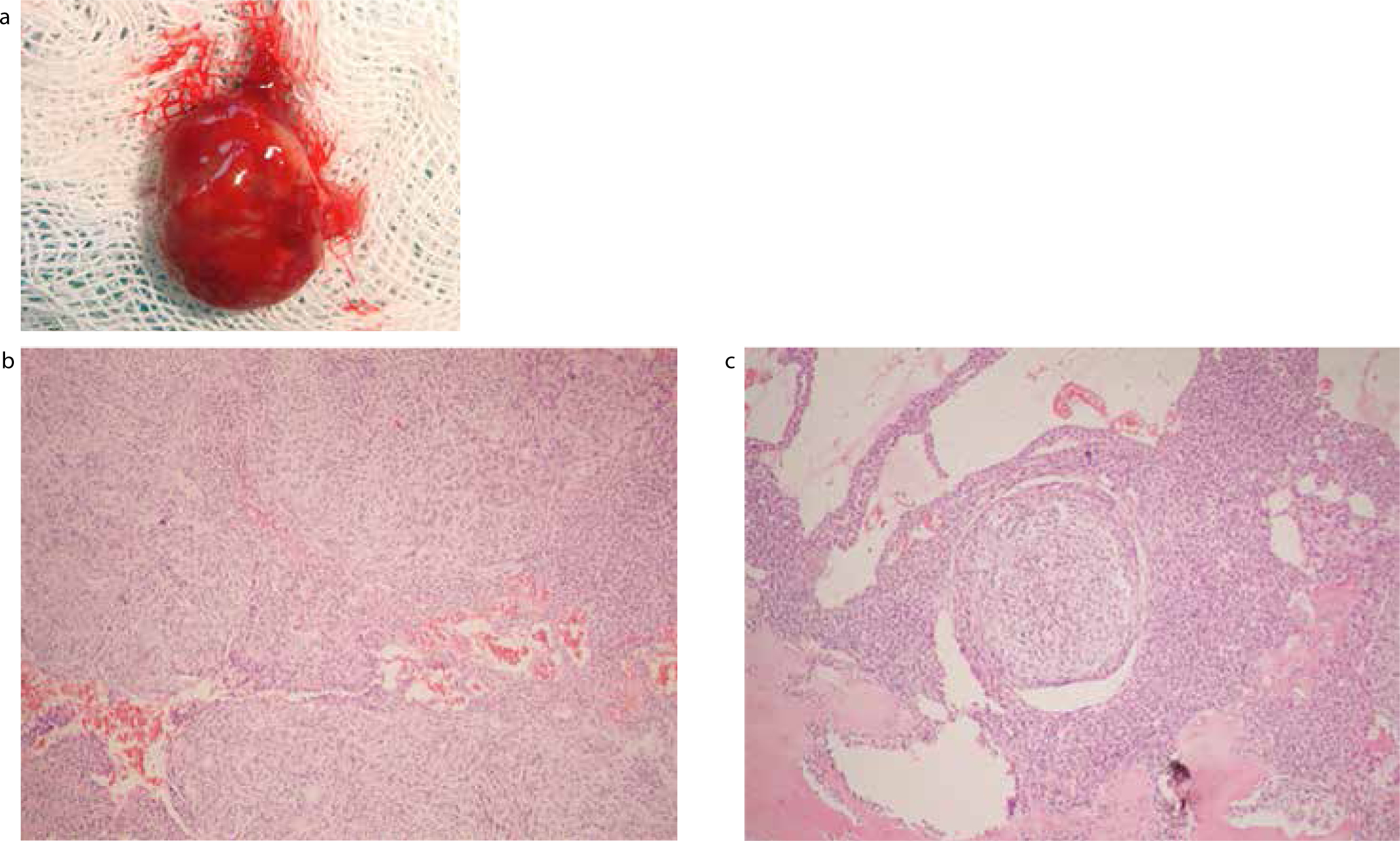
Gross examination of the specimen showed a single soft tissue measuring 2x1.5 cm (Figure 5a). At low magnification, the most striking pattern was solid nodules composed of cuboidal and columnar cells of odontogenic epithelium. In some areas, cells were arranged in the form of whorls, tubular rosette-like structures and nests. The duct-like areas were lined by a single row of columnar epithelial cells. Some amount of eosinophilic material in the centre of the rosettes and tubular structures was also observed. The final histopathological examination was reported as an extrafollicular type AOT (Figures 5b, c). The post-operative healing was uneventful and the patient was followed-up for two years post-operatively every six months and there was no sign of recurrence.
Figure 5.
(a) Macroscopic view of the excised specimen. (b) Whorled arrangement of cells, duct-like spaces are lined by a single row of columnar epithelial cells (x100, HE). (c) Solid nodule composed of odontogenic epithelium; amorphous material in the background (x200, HE).
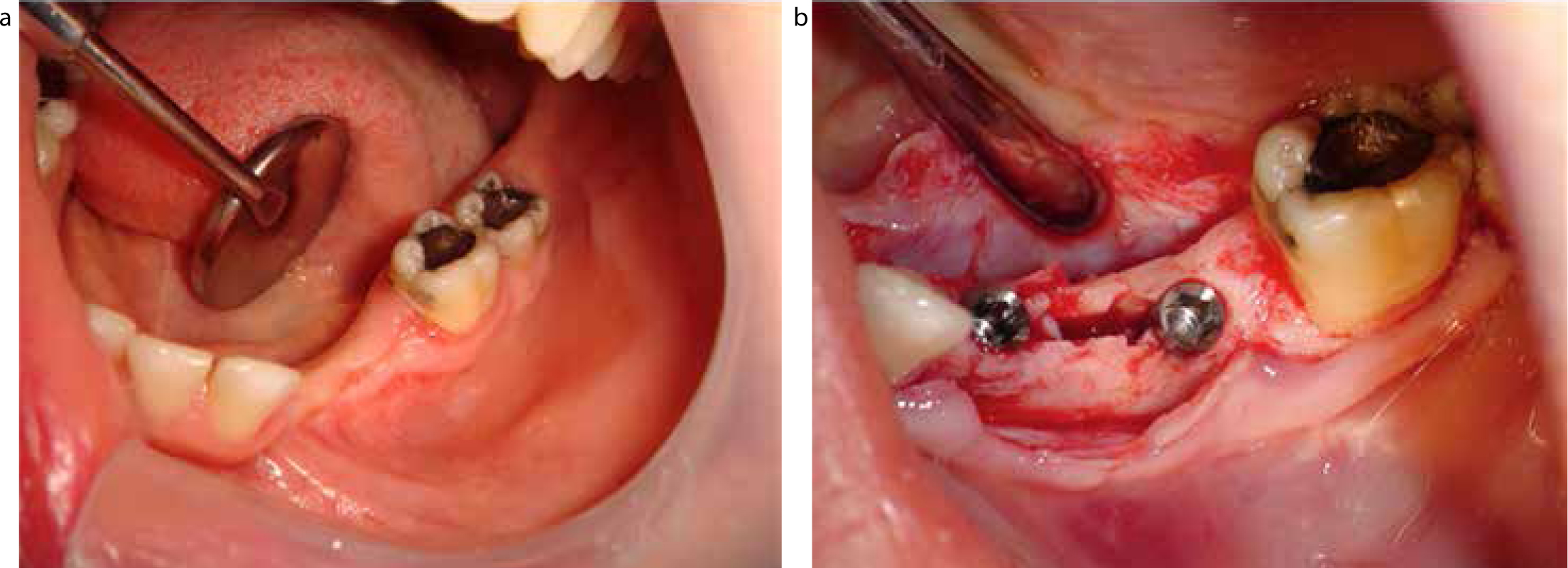
After a two years follow-up period, prosthodontic treatment options were discussed and a mandibular, fixed, implant-supported prosthesis was planned. The patient was informed about the procedures and informed consent was taken. Under local anesthesia following the full thickness crestal incision, the mucoperiosteal flap was reflected in both the buccal and lingual direction. The bucco-lingual width of the crestal bone was insufficient so the crestal split osteotomy was made to facilitate the implant insertion without any cortical dehiscence. Additionally, dead spaces of the bone was augmented with bovine bone graft (Geistlich Bio-Oss®) and a collagen membrane (Geistlich Bio-Gide® 25x25 mm). Two implants (3.7 mm in diameter, 10 mm in length and 3.7 mm in diameter, 11.5 mm in length) (Tapered Screw-Vent ® Zest Anchors LLC, CA) were placed and primary wound closure was obtained (Figures 6a, b). The patient was prescribed an antibiotic (amoxicillin 1 g, 2x1, 5 days, orally), an analgesic (naproxen sodium 550 mg, 2x1, 5 days, orally), and an antiseptic mouthwash (4% chlorhexidine gluconate 10 ml, 3x1, 5 days). The sutures were removed one week post-operatively and the wound healing was satisfactory.
Figure 6.
(a) Intra-oral view after two years tumour-free period from total enucleation. (b) Two dental implants were placed with crestal split osteotomy and then the dead spaces were reconstructed with bone graft and collagen membranes.
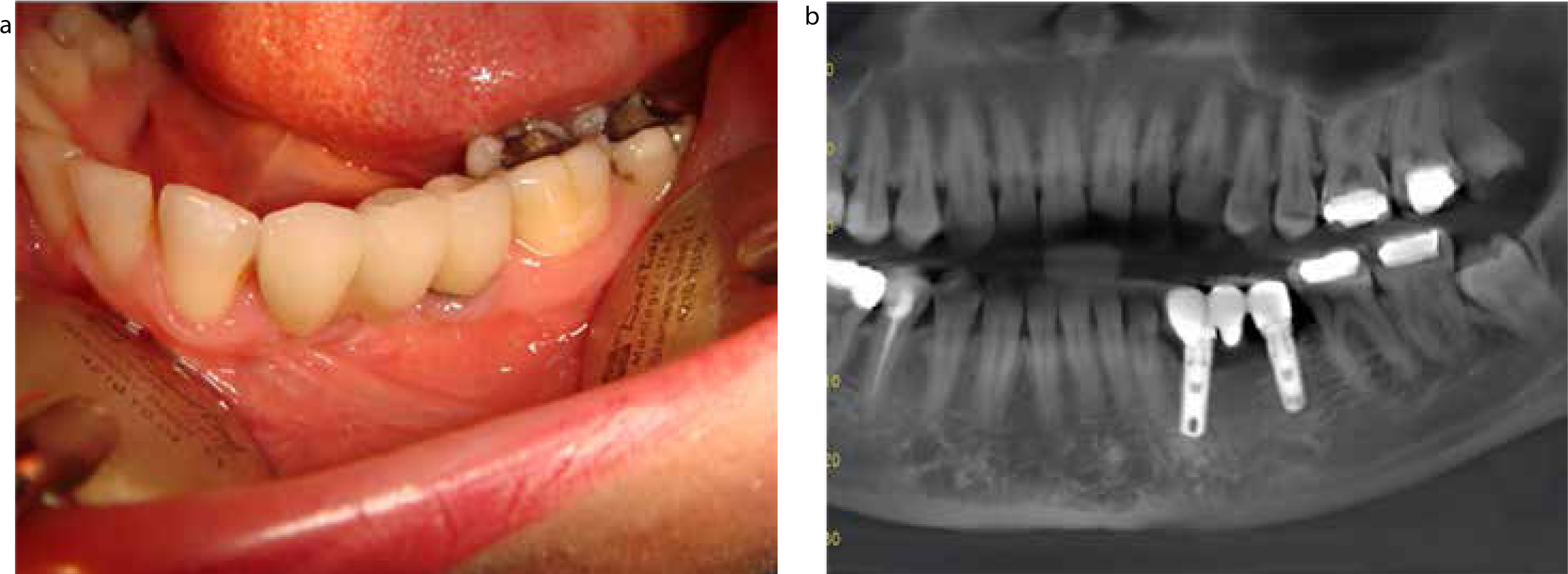
A period of six months allowed for optimum osseointegration before starting the prosthetic process. After clinical examinations of surrounding soft tissues and radiological examinations of bone and dental implants, the healing caps were screwed onto the implant which helps the surrounding gum tissue to heal and reform. After two weeks, healing caps were removed, the impression copings were screwed into the implant and then impressions were taken. A three-unit bridge, which is made of porcelain fused to a metal alloy, was fabricated for the patient as a final restoration. Clinical and functional assessments, as well as prosthesis satisfaction, were evaluated. Since the prosthetic rehabilitation was completed, the patient has been followed-up periodically every year. Peri-implant soft tissues are healthy with optimal integration of implants, steady levels of bone around the limited presence of keratinized mucosa and there has been 1.2 mm mean peri-implant bone resorption. At the time of this report, the patient had undergone six years of clinical and radiographic follow-up and had not exhibited any sign of implant mobility or tumour recurrence (Figures 7a, b).
Figure 7.
(a) Intra-oral view at the sixth year of follow-up. (b) OPG was taken after 4 years from the implant operation: 1.2 mm mean peri-implant bone loss without any signs of peri-implant gingivitis and/or peri-implantitis.
Discussion
An AOT is an uncommon, benign, asymptomatic, slow growing tumour that occurs more commonly in the anterior maxilla and is rarely reported in the mandible.17,18 It is defined as a tumour of the odontogenic epithelium with duct-like structures and varing degrees of inductive change in the connective tissue.7,19 There is a female over male incidence of almost 2:1 and these appear most often in the second decade of life. AOT is most frequently associated with a missing permanent tooth (the permanent maxillary canine being the most frequent).4,20
The lesions are typically asymptomatic, but may cause cortical expansion and displacement of the neighbouring teeth and root resorption is very rare. Because of its predilection for tooth-bearing bone, it is thought to arise from odontogenic epithelium.20 Although larger lesions have been reported in the literature, the tumours are usually 1.5–3cm in dimension.4 The sex and age of the patient was consistent with the literature and a slow growing, asymptomatic swelling causing buccolingual expansion with loss of buccal cortex, with 17.01 mm in the greatest diameter, was seen in the presented case. The most remarkable features were the rare localization (posterior mandible) of the lesion and the absence of an unerupted tooth.
The radiographical findings of an AOT frequently resemble other odontogenic lesions, such as dentigerous cysts, calcifying odontogenic cysts and tumours, ameloblastomas and odontogenic keratocysts.6 An AOT occurs in intra-osseous as well as in peripheral forms. Radiographically, the intrabony variants comprise a follicular and extrafollicular type. The follicular type shows a well-defined, unilocular radiolucency associated with the crown and often part of the root of an unerupted tooth, mimicking a dentigerous or follicular cyst. The extrafollicular type is not associated with an unerupted tooth and the radiolucency of the extrafollicular type is subdivided into:
E1: without relation to tooth structures; neither erupted nor unerupted;
E2: inter-radicular, adjacent roots diverge apically due to tumour expansion;
E3: superimposed at root apex level;
E4: superimposed at mid-root level.
The peripheral type appears as a gingival fibroma or epulis attached to the labial gingiva.4
Growth of the intrabony variants commonly results in cortical expansion. Displacement of adjacent teeth due to expansion is much more common than root resorption. The follicular type is three times as frequent as the extrafollicular type for both genders, also follicular and extrafollicular types are over two times more often located in the maxilla than in the mandible and most of the tumours involve the anterior aspect of the jaws.4 In the present case, a panoramic radiograph revealed a well-circumscribed, round, unilocular radioluceny between the roots of the mandibular left canine and second premolar. The patient had no root resorption but there was a tipping of the mandibular left first premolar and also the tumour was not associated with an unerupted tooth. CT scans demonstrated remarkable discontinuity and loss of the buccal cortical plate and thinning of the lingual cortical plate. Although all features of the lesion were in accordance with the radiographical view of an AOT mentioned in the literature, on the basis of the clinical and radiographic findings, the lack of an intact periodontal ligament and lamina dura in the involved teeth, along with negative vitality, the pre-diagnosis of radicular cyst was made.
The histopathological features of the tumour were described as a tumour of odontogenic epithelium with duct-like structures and with a varying degree of inductive changes in the connective tissue. The tumour may be partly cystic and, in some cases, the solid lesion may be present as masses in the wall of a large cyst. Moreover, eosinophilic, uncalcified and amorphous material can be seen and is called ‘tumour droplets’. Some tumour droplets show a homogeneous matrix, whereas most tumour droplets are not seen.7,19 In the presented case, solid areas were predominant and solid nests were composed of tubular and rosette-like structures. Connective tissue was minimal, the tumour was surrounded by a thin fibrous capsule and tumour droplets were also observed. According to the histopathological analysis, together with the radiographical and clinical features of the case, the final diagnosis was made as extrafollicular type AOT.
Conservative surgical excision or curettage has been proven as a treatment of choice because all variants of AOT show an identical and benign biological behaviour. However, in only three of 750 cases, the recurrences have been reported after conservative treatment in the literature.4,21
Several AOT cases have been reported in the literature to date. Philipsen et al presented an extrafollicular type AOT in a 17-year-old female patient which revealed a swelling of the maxillary left lip and infra-orbital region with a soft, fluctuant buccal swelling and a firm palatal swelling extending from the UL2 to the UL5 region in intra-oral examination. A well circumscribed radiolucency superimposed onto the apical half of the root of UL3 in radiographic examination was detected. They have totally enucleated the lesion under local anaesthesia and reported an uneventful healing.22 Philipsen et al also reported a 15-year-old girl with a periapical radiolucent lesion affecting two teeth initially suspected of periapical disease, although clinical findings seemed to indicate a non-endodontic lesion. They chose an exploratory surgical approach and the final diagnosis of the removed non-cystic tissue mass was microscopically confirmed to be an AOT.20
Yilmaz et al presented an extrafollicular AOT case in the anterior mandible of a 15-year-old female who was treated successfully with total enucleation.23 Saluja et al reported a patient with a large extrafollicular type AOT in the mandible with a significant root resorption of the involved displaced teeth which is not generally reported in AOTs. They removed the lesion along with the mobile teeth (mandibular lateral incisor, canine, premolars and the first molar) and the patient was followed-up for a while without recurrence but there were no data about the reconstruction and/or rehabilitation of the defect site.24
In another case report, an extrafollicular AOT occurring in the body of the mandible in an 18-year-old male patient, which was distinct and secondly clinically and radiologically diagnosed as a residual cyst, was successfully treated with total excision.25 Bhandari and Kothari presented an extrafollicular variant of AOT mimicking a periapical lesion in a 25-year-old pregnant lady. They enucleated the lesion extending from the right central incisor up to the right first premolar, along with the canine tooth, and reported that the recovery was uneventful and the healing was satisfactory.26 A case of an extrafollicular AOT, which is believed to have originated from the epithelial lining of a unicystic ameloblastoma, was presented but the surgical treatment procedure, post-operative recovery and rehabilitation details were not mentioned in the report.27
Although, in some of the case reports, uneventful healing of the defective areas after surgical excision without any reconstruction process were reported,20,22,23,24,25,26,28,29,30,31 some authors presented successful reconstruction of bony defects with different bone substitutes and membranes because of the extensive surgical resection of AOT lesions, in the literature.3,10,11 Because the final diagnosis of the lesion was not made definitely before the surgical excision, reconstruction was not performed to avoid additional complications, such as infection or graft rejection in the presented case.
Dental implants are an important component of multidisciplinary rehabilitation for patients after surgical resections of tumours or oral cancer patients. Regarding the aesthetic appearance and the masticatory rehabilitation of these patients, the application of a removable prosthesis not supported by dental implants may be difficult, or sometimes impossible, owing to the post surgical alteration of the anatomy, the low salivary flow and the acceptability by the patient. Therefore, rehabilitation with dental implants is more acceptable and reliable for the restoration of masticatory and aesthetic functions.13,32 Implants may improve denture retention and stability without unnecessary loading of the vulnerable mucosa; also function, comfort, aesthetic and the quality of life can be improved.14
Traditionally, implants have been selectively placed secondarily after resection and reconstruction. The benefits of secondary placement include adequate recognition of recurrence, a more accurate assessment of oral health and post-operative function and, in cases of mandibular segmental resection, a better appreciation of the positioning of the implants compared to the primary placement.16 Several case reports have been published, including the implant-supported prosthetic rehabilitations after extensive surgical resections and reconstructions.13,33,34,35 Oteri et al presented a combination of surgical and prosthetic solutions applied to a case of oral implant rehabilitation in a post-oncologic reconstructed mandible after ameloblastoma removal.33 In a retrospective study, 74% of patients, who were rehabilitated with implant-supported prostheses after mandibular reconstruction with a microvascular free fibula flap, have found oral rehabilitation ‘satisfactory’.35
Although many case series and reviews present successful results of oral rehabilitations with dental implants after surgical resections of odontogenic tumours or oral cancers in both jaws, no case report was found in the literature presenting the implant-supported prosthetic rehabilitation after surgical excision of an extrafollicular AOT lesion. In the presented case following the surgical excision and final histopathologic diagnosis, at the end of two years of tumour-free follow-up period, implant-supported prosthetic rehabilitation of the defective site was planned. The insufficient bucco-lingual width of the crestal bone was reconstructed with the crestal split osteotomy to facilitate the implant insertion without any cortical dehiscence and the dead spaces of the bone was augmented with bovine bone graft and collagen membrane. Osseointegration of the dental implants and the newly formed bone in the operation area was satisfactory.
Recurrence of AOT is exceptionally rare.10,11 Although the tumour was encapsulated and shows an identical benign behaviour, follow-up is of tremendous importance considering the rare localization and conservative surgical excision of the tumour. The patient was followed-up two years after surgical excision of the lesion, before dental implant placement and prosthetic rehabilitation. Since the tumour had been operated on, clinical and functional assessments as well as prosthesis satisfaction, were evaluated annually. The patient has been asymptomatic and has had no signs of recurrence for six years.
Conclusion
Because of being the extrafollicular type of AOT, and with respect to the localization of the lesion in the mandible, the presented case is a rare case of AOT and corresponds with the general descriptions in the literature. It can be concluded that the rarity of AOT may be associated with its slowly growing pattern and symptomless behaviour. Therefore it should be distinguished from more common lesions of odontogenic origin in routine dental examinations. After proper surgical excision and careful periodical follow-ups, without any sign of recurrence, the operation sites can be safely rehabilitated with dental implants instead of removable prostheses. Osseointegration of the dental implants and the newly formed bone in the operation area was satisfactory, as in the healthy bone, and this treatment option can also increase the patient satisfaction level and quality of life.