Hattab FN, Yassin OM. Etiology and diagnosis of tooth wear: a literature review and presentation of selected cases. Int J Prosthodont. 2000; 13:101-107
Bartlett D, Ganss C, Lussi A. Basic Erosive Wear Examination (BEWE): a new scoring system for scientific and clinical needs. Clin Oral Investig. 2008; 12:S65-S68
Bartlett D. A proposed system for screening tooth wear. Br Dent J. 2010; 208:207-209
Eccles JD. Dental erosion of nonindustrial origin. A clinical survey and classification. J Prosthet Dent. 1979; 42:649-653
Smith BG, Knight JK. An index for measuring the wear of teeth. Br Dent J. 1984; 156:435-438
Lussi A. Dental erosion clinical diagnosis and case history taking. Eur J Oral Sci. 1996; 104:191-198
Margaritis V, Nunn J. Challenges in assessing erosive tooth wear. Monogr Oral Sci. 2014; 25:46-54
Olley RC, Wilson R, Bartlett D, Moazzez R. Validation of the basic erosive wear examination. Caries Res. 2014; 48:51-56
DeBate RD, Tedesco LA, Kerschbaum WE. Knowledge of oral and physical manifestations of anorexia and bulimia nervosa among dentists and dental hygienists. J Dent Educ. 2005; 69:346-354
Kato T, Thie NMR, Montplaisir JY, Lavigne GJ. Bruxism and orofacial movements during sleep. Dent Clin North Am. 2001; 45:657-684
Seghi RR, Rosenstiel SF, Bauer P. Abrasion of human enamel by different dental ceramics in vitro. J Dent Res. 1991; 70:221-225
Lombardi RE. The principles of visual perception and their clinical application to denture esthetics. J Pros Dent. 1973; 29:358-382
Valena V, Young WG. Dental erosion patterns from intrinsic acid regurgitation and vomiting. Aust Dent J. 2002; 47:106-115
Hunter ML, Addy M, Pickles MJ, Joiner A. The role of toothpastes and toothbrushes in the aetiology of tooth wear. Int Dent J. 2002; 52:399-405
Bartlett DW. Retrospective long term monitoring of tooth wear using study models. Br Dent J. 2003; 194:211-213
Bartlett DW, Coward PY. Comparison of the erosive potential of gastric juice and a carbonated drink in vitro. J Oral Rehabil. 2001; 28:1045-1047
Chander S, Rees J. Strategies for the prevention of erosive tooth surface loss. Dent Update. 2010; 37:12-18
Young WG. The oral medicine of tooth wear. Aust Dent J. 2001; 46:236-250
Duchan E, Patel ND, Feucht C. Energy drinks: a review of use and safety for athletes. Phys Sportsmed. 2010; 38:171-179
Rees JS. The role of drinks in tooth surface loss. Dent Update. 2004; 31:318-326
Amaechi BT, Higham SM. Dental erosion: possible approaches to prevention and control. J Dent. 2005; 33:243-252
Graubart J, Gedalia I, Pisanti S. Effects of fluoride pretreatment in vitro on human teeth exposed to citrus juice. J Dent Res. 1972; 51:1677-1680
Rees J, Loyn T, Chadwick B. Pronamel and tooth mousse: an initial assessment of erosion prevention in vitro. J Dent. 2007; 35:355-357
West NX. Dentine hypersensitivity: preventive and therapeutic approaches to treatment. Periodontology 2000. 2008; 48:31-41
Attin T, Siegel S, Buchalla W, Lennon AM, Hannig C, Becker K. Brushing abrasion of softened and remineralised dentin: an in situ study. Caries Res. 2003; 38:62-66
Wiegand A, Burkhard JPM, Eggmann F, Attin T. Brushing force of manual and sonic toothbrushes affects dental hard tissue abrasion. Clin Oral Investig. 2013; 17:815-822
Tellefsen G, Liljeborg A, Johannsen A, Johannsen G. The role of the toothbrush in the abrasion process. Int J Dent Hyg. 2011; 9:284-290
Olivera AB, Marques MM. Esthetic restorative materials and opposing enamel wear. Oper Dent. 2008; 33:332-337
Sripetchdanond J, Leevailoj C. Wear of human enamel opposing monolithic zirconia, glass ceramic, and composite resin: an in vitro study. J Prosthet Dent. 2014; 112:1141-1150
Recent epidemiological data shows that the prevalence of tooth wear (TW) is increasing. Current available assessment tools are either too complicated to carry out on every patient or inadequate in identifying the nature of the condition. Moreover, early onset or localized lesions may be overlooked. This article describes a screening tool which may overcome these problems. This tool involves using the existing Basic Erosive Wear Examination scoring system and a proposed age-related grid. This will lead to an associated pathway, which indicates the recommended level of further investigations and management.
CPD/Clinical Relevance: Early identification and prevention of pathological tooth wear in the primary care setting is the key to slowing down the disease progression.
Article
Tooth wear (TW) or Tooth Surface Loss (TSL) is used to describe the progressive loss of dental hard tissue by chemical and mechanical actions other than those caused by caries or trauma. It is a multifactorial process comprised of erosion, attrition, abrasion and abfraction.1
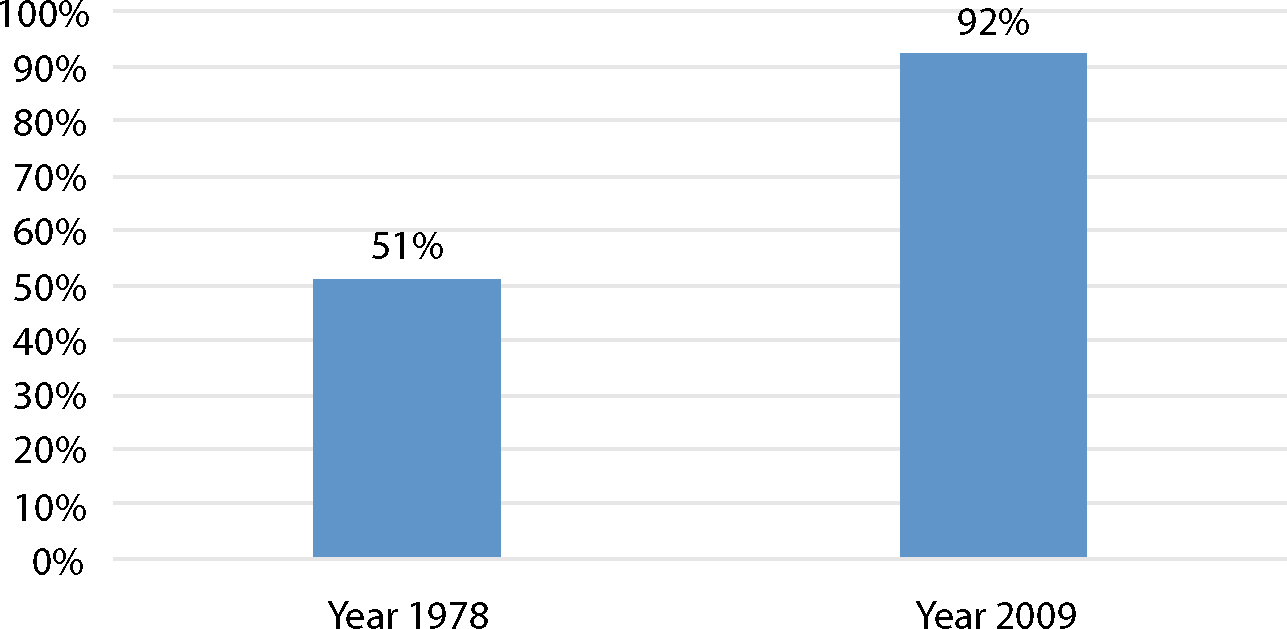
In England, Wales and Northern Ireland, improved dental health awareness and dental services in the last 30 years have reduced edentulous adults from 28% in 1978 to 6% in 2009. Compared with 30 years ago, the percentage of adults aged 45–50 who have over 20 natural teeth increased nearly two-fold (Figure 1).2 Because natural teeth now survive for longer, the impact of TW is critical to the ageing population. The overall prevalence of tooth wear has increased since 1998.3 The increase of anterior TW in the younger group, aged 16 to 24, was significantly higher than the older groups.3 Fortunately, the prevalence of TW-related dentine and pulp exposure for children aged 12 to 15 remains at a low level.4 This supports the fact that TW is not aggressive, but rather a slow process. Therefore it requires long-term preventive and monitoring strategies. The earlier the disease or potential risk is identified, the more likely a well-designed management regimen would be successful.
Figure 1. Adults aged 45–54 had 21 or more natural teeth in England.2
The aim of this article is therefore to describe a screening tool, which involves using the current Basic Erosive Wear Examination (BEWE)5,6 and a proposed age-related Red-Amber-Green (RAG) grid. This tool aims at effectively identifying the pathological or physiological nature of TW. According to the nature, one of the three management pathways can then be followed. The recommended additional investigations would inform a sound individualized dynamic diagnosis. A fit for purpose preventive, monitoring and restorative plan can then be formulated.
Initial assessment – screening
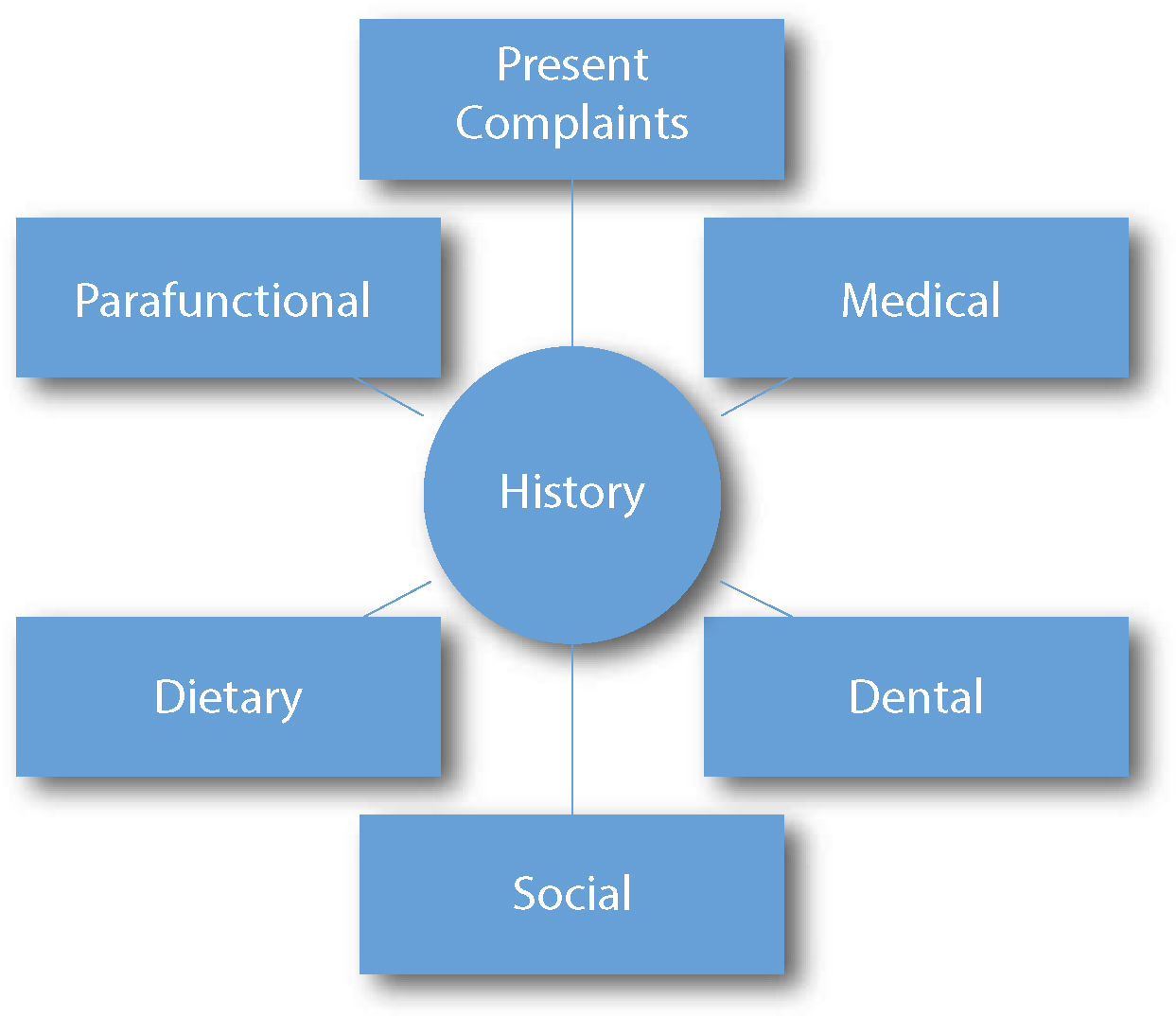
During routine dental examinations, patient's complaints (Table 1) and histories (Figure 2) may already highlight the condition of TW.
Complaints
Signs and Symptoms
Discomfort
Dentine hypersensitivityToothache (symptoms of pulpitis)Abscess or swellingSharp teethFood packingTemporomandibular disorder symptoms
Dental Aesthetics
Short and/or uneven front teethUpper teeth not showing when smilingDiscolorationIncreased translucency
Others
Chipped or fractured toothLost or fractured restorationsReduced masticatory efficiency
Figure 2. Histories related to TW.
Indices have been used in the past to assess the severity of tooth wear. Table 25,-9 summarizes the four most popular ones used in previous research.10 Clinically, it is impractical for busy general dental practitioners (GDPs) to carry out full TW charting for every patient as a part of their examination. Therefore, the simple and quick BEWE (Table 3) is ideal for screening purposes. In addition, the associated management guideline (Table 4) also provides clear guidance according to different cumulative scores.5,6 Although the BEWE was originally developed to examine and record the severity of erosive wearing lesions, it was validated to assess all types of TW.11 Nonetheless, the BEWE management grid has inherited some inadequacies:
Routine maintenance and observationRepeat at 3-year intervals
Low
1
Between 3 and 8
Oral hygiene and dietary assessment, and advice, routine maintenance and observationRepeat at 2-year intervals
Medium
2
Between 9 and 13
Oral hygiene and dietary assessment, and advice, identify the main aetiological factor(s) for tissue loss and develop strategies to eliminate respective impacts Consider fluoridation measures or other strategies to increase the resistance of tooth surfacesIdeally, avoid the placement of restorations and monitor erosive wear with study casts, photographs, or silicone impressionsRepeat at 6–12 month intervals
High
3
14 and over
Oral hygiene and dietary assessment, and advice, identify the main aetiological factor(s) for tissue loss and develop strategies to eliminate respective impactsConsider fluoridation measures or other strategies to increase the resistance of tooth surfacesIdeally, avoid restorations and monitor tooth wear with study casts, photographs, or silicone impressionsEspecially in cases of severe progression, consider special care that may involve restorationsRepeat at 6–12 months
Pathological or physiological TW cannot be identified.
The resulting risk level may be a false positive or a false negative. False positives tend to occur in older individuals with historical or physiological TW. False negatives tend to occur in younger ones who are under frequent intrinsic and extrinsic acid attacks with early hard tissue loss (ie cumulative BEWE ≤8).
Using the total score to decide management strategy may mask local moderate or severe TW.
Edentulous sextant(s) or extensively restored sextant(s) will decrease the overall cumulative BEWE score and result in underestimation.
According to the author, the sextant-based concept of BEWE was originally derived from the Basic Periodontal Examination (BPE).12 For BPE code 3 or 4, a follow-up probing depths charting is indicated to investigate the disease pattern and severity further. Similarly, a follow-up full charting should also be included in the management guideline for pathological TW.
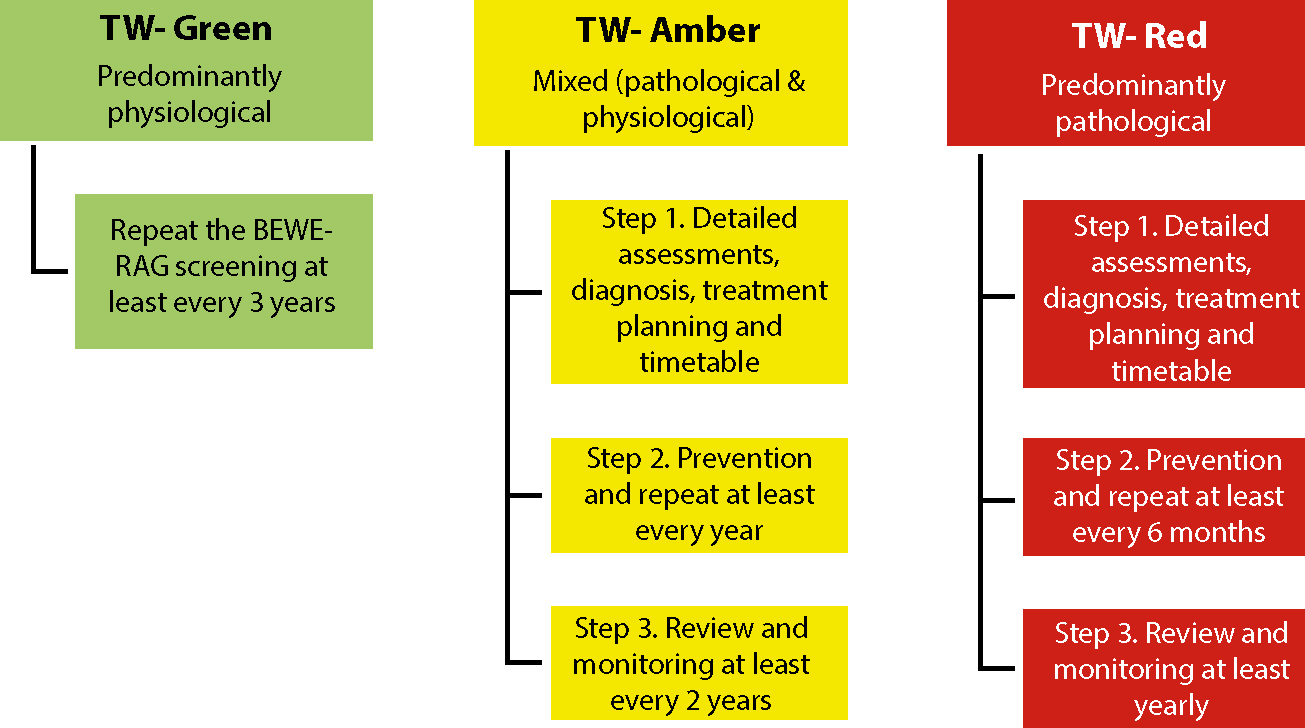
Using an additional age-related RAG grid (Table 5) and management pathways (Figure 3), the above inadequacies can be overcome. The age-groups in the Adult Dental Health Survey3 were used as a reference to decide the cut-off ages for each group in the RAG grid. The cumulative BEWE tiers were decided, based on hypothetical case scenarios with increasing severity (Table 6). The ‘Any BEWE’ and ‘≥50% BEWE 3’ were designed to address localized situations and missing sextants (ie partial BEWE). Once the GDP has become familiarized with the BEWE and RAG grid, the TW screening should only occupy approximately one minute of the examination appointment (Table 7).
Figure 3. RAG management pathways.
Cumulative BEWE tiers
Reasoning of the cut-off total score (using the BEWE and equivalent severity scenarios as references)
Predominantly pathological TW for age under (Based on author's experience)
Consider delaying screening for patients with acute symptoms, high caries risk or high periodontal riskComplete edentulous or all remaining teeth are hopelessAll remaining teeth were extensively restoredUnstable general health (ASA ≥4)
Steps
Choose the most worn permanent tooth surface from the first sextant
Exam, assess the BEWE score and record
Repeat for the other sextants
Substitute the results into the age-related RAG grid to identify the nature of the TW
Red and amber management pathways – Step 1
Detailed assessment
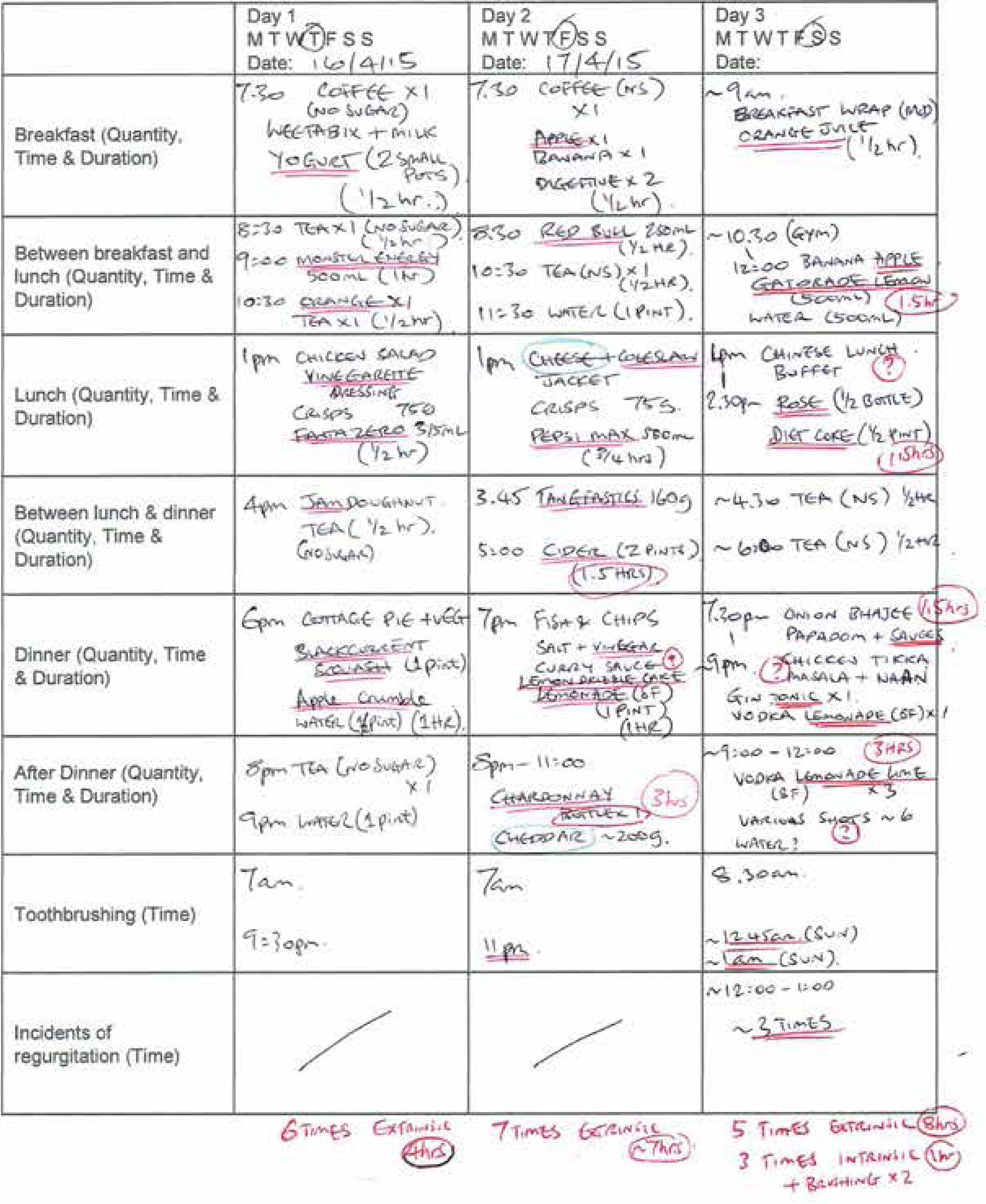
The first step of the TW-Red (predominantly pathological) and TW-Amber (mixed) management pathways is detailed assessments (Table 8). These assessments can be carried out in a separate appointment. This will allow the patient to complete a diet analysis sheet. Compared with the diet history sheet for high caries risk patients, the one in Figure 4 has also incorporated the components of intrinsic factors and brushing habit.
Recommended Assessments
Dietary and intrinsic acid analysisFull-mouth TW charting (eg Figure 5) and pattern analysis
Additional Special Investigations (if necessary)
Interview to gather information about possible eating disorder, alcohol and recreational drug habitExtra-oral and mucosal examinationsExisting ceramic restorations analysisPalpation, percussion and mobility testingVitality testing (to identify endodontic complication)RadiographsArticulatory and occlusal assessmentAesthetic assessmentSalivary analysis (flow rate and buffering capacity)
Liaise with Other Health Professionals (if necessary)
Medical GP (to identify intrinsic causes and cause of xerostomia)Psychologist (to assess eating disorder, anxiety and depression)
Figure 4. A completed diet sheet to study extrinsic, intrinsic factors and brushing habits.
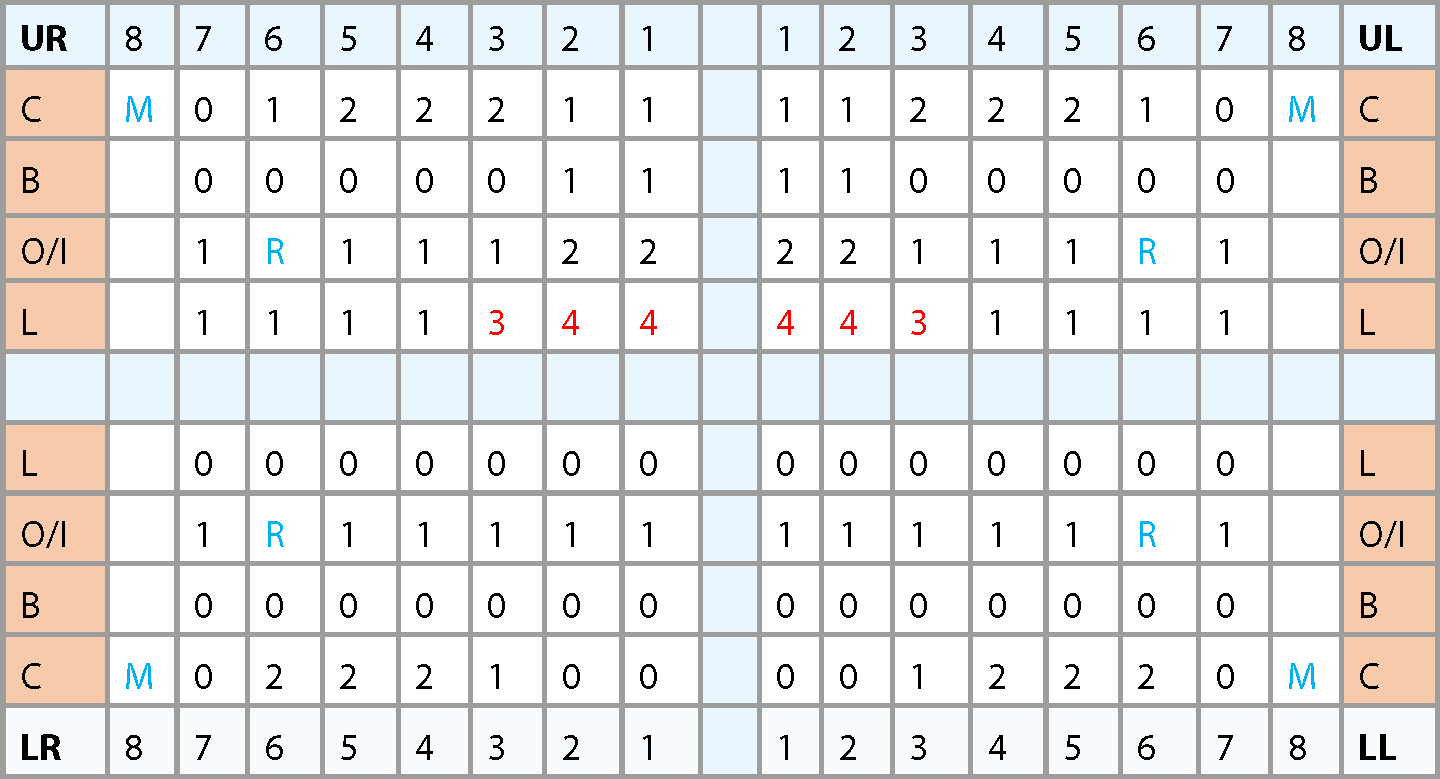
Similar to a full probing depth charting for periodontitis, a full TW charting is necessary to disclose the disease pattern of the pathological and mixed TW. It also facilitates diagnosis and treatment planning as well as enhancing patient communication. An example of a full charting using the Tooth Wear Index (TWI) (Table 9) is illustrated in Figure 5.
Score
Surface
Criteria
0
B/L/O/IC
No loss of enamel surface characteristicsNo loss of contour
1
B/L/O/IC
Loss of enamel surface characteristicsMinimal loss of contour
2
B/L/OIC
Loss of enamel exposing dentine for less than one-third of the surfaceLoss of enamel just exposing dentineDefect less than 1 mm deep
3
B/L/OIC
Loss of enamel exposing dentine for more than one-third of the surfaceLoss of enamel and substantial loss of dentineDefect less than 1–2 mm deep
4
B/L/OIC
Complete loss of enamel, or pulp exposure, or exposure of secondary dentinePulp exposure or exposure of secondary dentineDefect more than 2 mm deep, or pulp exposure, or exposure of secondary dentine
Figure 5. Example of a full TW charting using TWI.8(C – Cervical; B – Buccal; O – Occlusal; I – Incisal; L – Lingual; M – Missing; R – Existing restoration).
Patients with eating disorders, alcohol abuse problems or recreational drug habits are usually more secretive when a friend or family is present. Moreover, they may not want to disclose these habits to their own dentists. Cheilosis, parotid gland enlargement and fine fair facial hair may be present in patients with eating disorders.13 Tooth-grinding reported by the patient's bed-partner, tender masticatory muscles in the morning or cheek and tongue indentations usually indicate sleep bruxism.14 A long-term grinding habit can contribute to attrition. On the other hand, the porcelain occlusal surface of a ceramic restoration can cause significant abrasion to the opposing tooth.15
Full aesthetic assessment may be necessary, especially when the patient is concerned with his/her appearance. Anterior TW can destroy the harmony of dental aesthetics by making the crown height to width ratio disproportionate. It can also change the amount of teeth showing, which may result in an ageing smile.16
Diagnosis
Sound diagnosis is crucial to identifying the treatment needs and formulating an appropriate management plan. One must bear in mind that the BEWE-RAG system is just a screening tool. It can neither provide a diagnosis nor evaluate the current risk. Definitive diagnosis and aetiologies can usually be reached after the detailed assessments. Table 10 has summarized some key points that should be included in a TW diagnosis.
Nature
Localized or generalizedSeverity (mild, moderate or severe)Predominantly pathological or physiological or mixedCurrent risk level (high, medium or low)
Aetiologies
Primarily by erosion, attrition, abrasion or abfractionModified by one or more of above factors
Evident to Support the Aetiologies
Relevant historiesPatterns and morphologies of the TWFindings of the special investigations
Others
Dentine hypersensitivityEndodontic complicationOcclusal complicationAesthetic complicationChipping or fracturing of tooth substances
Sometimes, the lesion's pattern or clinical features may suggest the disease aetiologies.17 These are summarized in Table 11 and Figures 6–8. The role of erosion, attrition, abrasion and abfraction changes over time on a tooth surface. Practitioners can easily fall into a trap and conclude that the cause of a cervical lesion, such as Case 4 (Figure 9), is from toothbrushing. However, an in vitro study has shown that 80–100 years of toothbrushing with toothpaste may be required to produce 1 mm dentine loss.18 Therefore, it is unlikely that abrasion can be the sole cause of significant pathological TW. In fact, the Adult Dental Health Survey 20093 found that the prevalence of tooth wear was actually higher in subjects who brushed less than twice a day. So, an advanced non-carious cervical lesion (NCCL) which exposed the pulp is likely to be caused by abfraction, erosion and abrasion to varying degrees at different times.
Affect all surfaces but less on buccal surfaces of upper first molars and lingual surfaces of anterior teeth due to buffering effect of saliva
Enamel cupping of incisal or occlusal surfaces
Proud restorations
Worn incisal or occlusal surfaces unable to make occlusal contact at all
Extrinsic vs Intrinsic Patterns
Buccal erosive lesions at upper incisors and canines are closely related to extrinsic acid
Lingual erosive lesions at upper canines, lower incisors, upper and lower premolars are closely related to intrinsic acid17
Predominantly Attrition
Affects occlusal surfaces
Shiny facets
Corresponding to opposing teeth like jigsaw-type fitting on excursions (Figure 7 – Case 2)
Predominantly Abrasion
Toothbrushing
Affects cervical areas
Supragingival lesions
Porcelain
Affects occlusal surfaces of opposing teeth (Figures 8a and b – Case 3)
Predominantly Abfraction
Affects cervical areas at cemento-enamel junction with sharp edges
Figure 6. Case 1: Predominantly erosion.Figure 7. Case 2: Predominantly attrition on the upper right lateral incisor. Its bevelled incisal edge is corresponding to the opposing incisal edge on excursions.Figures 8.
(a, b) Case 3: Ceramic abrasion of the upper left canine exposing the palatal dentine. Also note the shiny palatal amalgam restoration and lack of stain when compared to the right-hand side.Figure 9. Case 4: Advanced localized NCCLs with endodontic complication.
Logical treatment planning and timetable
Tooth wear may be a slow process19 and will therefore rarely significantly deteriorate within a couple of years. Initial treatment should aim at stabilizing and preventing periodontal disease and caries. Although the TW on the upper first molars of Case 5 (Figure 10) may be the first thing which a dentist notices, this patient's attention should be drawn towards smoking, oral hygiene and periodontitis.
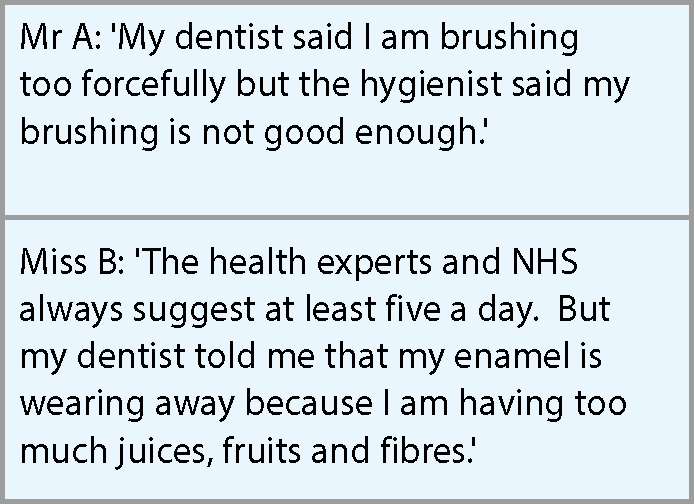
Figure 10. Case 5: 62/M smoker, the cumulative BEWE was 14. Using the age-related RAG grid, the nature of the TW is Amber (mixed pathological and physiological). The history showed frequent consumption of dried sticky sour fruits as a snack in childhood. The diet analysis shows current low risk in extrinsic and intrinsic acid. The TWI charting had highlighted the unique pattern. The articulatory assessment shows no sign of parafunctional habit. The current risk of TW is low. This is confirmed by the fact that all other teeth are relatively unaffected.Figure 11. Examples of confusing and contradicting health advices.
In addition to prioritizing managements into different stages, it is imperative to check the outcome of the previous management before proceeding further. Some patients may take longer to achieve a satisfactory outcome than others. If so, the treatment sequence must be driven by a patient's oral health rather than by a patient's desire. Operative treatment for TW is seldom indicated in the first stage and sometimes no such treatment may be the best option. Table 12 has summarized the logical treatment cascade.
OHI, scaling and remove other plaque retentive factorsDietary analysis and adviceOther advices including TW-relatedProfessional and self-applied fluoride regimenSmoking cessation adviceCaries stabilizationExtraction of non-restorable teethReferral to manage gastric reflux, alcohol abuse, eating disorder, anxiety and depression
Confirm satisfactory outcome of above and no active diseaseRegular assessment of periodontal, caries and other disease risksTW monitoringPreventive advice reinforcement
6. Rehabilitation and elective treatments (if indicated)
OrthodonticsOcclusal planning – conformative or reorganizedAesthetic treatments (include whitening)Direct adhesive restorations for TW purpose including the direct DahlPre-restorative and pre-prosthetic surgeryProvisional indirect restorations and prosthesisIndirect restorations and prosthesisImplant placement and superstructure construction
7. Maintenance and recall
Regular assessment of periodontal, caries and other disease risksTW monitoringPreventive advice reinforcementMonitor restorations and repair or replace when necessary
Red and amber management pathways – Step 2: Prevention
For TW-Amber and TW-Red, the next step of the management pathways is prevention (Table 13). However, many patients may find that preventive advice can be confusing and sometimes contradicting (Figure 11). Therefore, advice should be carefully chosen according to the diagnosis, aetiologies and risk level. A diet analysis sheet (Figure 4) is a good tool to provide clear individualized preventive advice. Emphasis should be made on frequent intrinsic acid attacks because of its extremely low pH and high titratable acidity.20 For extrinsic acids, reducing the frequency, duration and avoiding consumption between meals are far more important than reducing the amount of intake.21
Prevention
Advise or prescribe
Advise or prescribe with cautions
Erosion
Reduce frequency and duration of dietary acid intake
Consume with main meal when saliva is abundant
Avoid consumption of sport drinks, energy drinks and acidic alcoholic drinks
Use straw to bypass teeth
Fluoride: professional applied, mouthwash and high concentration toothpaste
Post acid attack regimen: hard cheese, baking soda, tooth mousse or non-fruity chewing gum
Dentine bonding agent
Referral to GP for alcohol and drug support
Referral to psychologist for eating disorder
Avoid drinks and foods with extremely low pH and/or high titratable acidity
Attrition and Abfraction
Reduce smoking, alcohol and caffeine consumption.14
Do not brush within 30 minutes after intrinsic or extrinsic acid attack.29
Avoid high abrasive toothpaste
Use low abrasive restorative materials.
Avoid excessive force of toothbrushing
The erosive power of carbonated and citric sports drinks can be enhanced by them being consumed during prolonged vigorous exercises, as dehydration results in reduced salivary secretion and hence less protection.22 Increased erosion can result from regular consumption of energy drinks as they usually are acidic and contain large amounts of caffeine which can reduce salivary flow.23 Alcoholic drinks such as wines, ciders, cocktails and alcopops can cause the worst damage as they are acidic, strong diuretics and they can induce intrinsic acid reflux.22,24 Nevertheless, preventive advice relating to these drinks may not be very popular to the patients. It may sound more appealing to advise consuming such drinks with main meals, reducing frequency and duration, using a straw and employing the protective regimen mentioned below.
Saliva has calcium and outstanding buffering ability, which promotes remineralization and reduces demineralization. We should recommend that patients consume dietary acid with a main meal when the saliva is abundant. Inbetween meals, salivary flow can be stimulated by non-fruity, sugar-free chewing gum. Mouthrinsing with antacid tablets, sodium bicarbonate or baking soda solution immediately after intrinsic or extrinsic acid attacks can neutralize the residual acid. This will minimize the erosive damage.25 When hydroxyapatite is combined with fluoride to form fluoroapatite, the critical pH decreases.26 This favours remineralization and disfavours demineralization. Therefore, regular topical fluoride application is indicated for patients with higher risk of TW. Topical fluoride can also be used to improve dentine hypersensitivity in NCCLs. Sensitive toothpaste and Tooth Mousse (GC) should be recommended to this group of patients.27 A coating with a dentine bonding agent may protect the tooth substance from acid attack and may reduce hypersensitivity.28
Smoking and drinking habits, stressful lifestyle, medications, medical or psychological conditions can contribute to sleep bruxism.14 Hard acrylic occlusal splints can reduce further attrition for confirmed cases. On the other hand, soft nightguards may increase the activity of the masseter muscle after long term wearing.14 They are not suitable for patients with developing dentition. In addition, the full coverage design hinders the post-erosion remineralization. It is also plaque retentive, which increases the periodontal and caries risk.
Toothbrushing within 30 minutes of extrinsic or intrinsic acid attack is generally not recommended.29 Brushing with excessive force may be avoided by using electric toothbrushes.30 Using a softer toothbrush instead of a harder one does not necessarily reduce abrasion.31 As mentioned above, toothbrushing with toothpaste cannot solely cause significant NCCLs. Any modification of a good brushing habit may reduce its effectiveness. To avoid further damage, we should choose a less abrasive restorative material when restoring an occlusal surface opposite to a worn tooth. Direct composite resin is the first choice as it is tooth-coloured, conservative, strong and low abrasive. Indirect restorations with porcelain surface can achieve the best aesthetic outcome but they are more abrasive than metal alloys and monolithic zirconia.32,33
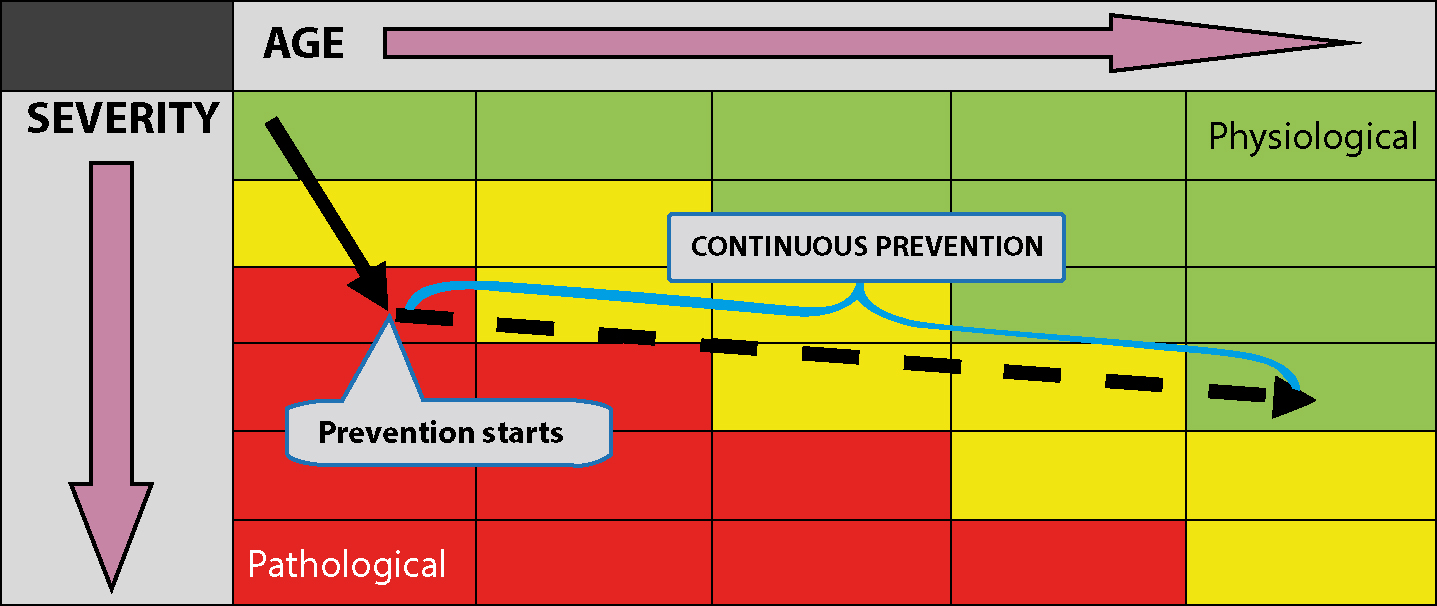
The preventive regimens will slow down the TW process. Hopefully, when the patient gets older, the cumulative BEWE score moves relatively horizontally across the age-related RAG grid. That is when the condition moves away from the red pathological TW zone (Figure 12).
Figure 12. The goal of TW prevention.
Red and amber management pathways – Step 3. Review and monitoring
As mentioned in Table 12, the periodontal, caries and other disease risks, including TW, should be regularly revised. This is also a good time to reinforce the preventive advice and carry out a new diet analysis. The minimum review intervals are two years for TW-Amber and one year for TW-Red. Barlett states that inadequate sensitivity of the BEWE makes it unsuitable for monitoring purposes.6 Barlett advises the use of TWI and study models to monitor TW. However, the study models can cause storage and damage problems.19 Digital models taken by the CAD/CAM technology offer a good alternative to this option. Digital photographs (Figures 13a and b) can also be used to monitor TW. They are relatively inexpensive and easy to share. Moreover, they enable instant preview, visual and colour comparison.
Figures 13. Case 6: (a) LL6 in Aug 2006, (b) LL6 in March 2015. Note the difference in area of exposed dentine on the occlusal surface after almost nine years.
Restorative and prosthetic considerations
During restorative and prosthetic treatment planning, a GDP should weigh up the possible harmful effects of these interventions against the damage from alternative treatments or no treatment. Specialist referral should be considered when the complexity is outside one's ability.
The BEWE-RAG TW screening system was not designed to make a diagnosis, therefore restorative and prosthetic treatments were not included in the management pathways. Operative interventions should only be prescribed on an individual basis according to the full TW charting and diagnosis. Take TWI as an example, lesions of scores 0, 1 and 2 do not need to be restored. Isolated TWI scores 3 and 4 usually do not need any treatment except for their complications. On the other hand, more extensive TWI scores 3 and 4 may require operative interventions.
Conclusion
Tooth wear has become an important dental condition, affecting many of the young generation. The BEWE-RAG tool simplifies the screening process and enables early identification of pathological TW. This can be easily done in a primary care setting. The associated management pathways assist a GDP to reach a sound diagnosis and evaluate the current risk. Early prevention and progress monitoring will avoid further deterioration. Nonetheless, the proposed screening tool may require further improvements and research to prove its validity.