Opdam NJ, Roeters JJ, Loomans RA, Bronkhorst E. Seven year clinical evaluation of painful, cracked teeth restored with a direct composite restoration. J Endod. 2008; 34:808-811
Seo DG, Yi YA, Shin SJ. Analysis of factors associated with cracked teeth. J Endod. 2012; 38:288-292
Signore A, Benedicenti S, Covani U, Ravera G. A 4- to 6-year retrospective clinical study of cracked teeth restored with bonded indirect resin composite onlays. Int J Prosthodont. 2007; 20:609-616
Banerji S, Mehta SB, Millar BJ. Cracked tooth syndrome. Part 2: restorative options for the management of cracked tooth syndrome. Br Dent J. 2010; 208:503-514
Van Dijken JWV. Direct resin composite inlays/onlays: an 11 year follow up. J Dent. 2000; 28:299-300
Ratcliff S, Becker I, Quinn L. Type and incidence of cracks in posterior teeth. J Prosthet Dent. 2001; 86:168-172
Saunders W, Saunders E. Prevalence of periradicular periodontitis associated with crowned teeth in an adult Scottish subpopulation. Br Dent J. 1998; 185:137-140
Schwartz RS, Robbins JW. Post placement and restoration of endodontically treated teeth: a literature review. J Endo. 2004; 30:289-301
Eliyas S, Jalili J, Martin N. Restoration of the root canal treated tooth. Br Dent J. 2015; 218:53-62
MacInnes A, Hall AF. Indications for cuspal coverage. Dent Update. 2016; 43:150-158
Tan I, Chen NN, Poon CY, Wong HB. Survival of root filled cracked teeth in a tertiary institution. Int Endod J. 2006; 39:886-889
Kang SH, Kim BS, Kim Y. Cracked teeth: distribution, characteristics, and survival after root canal treatment. J Endod. 2016; 42:557-562
This is the second-part of this three-part series. The first paper discussed the occlusal and cracked tooth aetiological factors which may be responsible for restoration failure. This paper will outline the restorative options for cracked and root canal-treated teeth. It will also briefly give an overview of some of the potential endodontic complications commonly associated with failed restorations. The third, and final, part of the series will provide an overview of the previous papers and conclude with a case report.
CPD/Clinical Relevance: Failure of amalgam restorations is a commonly encountered clinical problem in general practice and no one case presents in the same way. Therefore, a competent endodontic diagnosis and implementation of the most appropriate, minimally invasive restorative option requires an adequate knowledge of the current literature.
Article
Long-term treatment considerations for the management of cracked teeth
Direct intra-coronal restorations
Direct intra-coronal restorations of bonded amalgam and resin-composite should be considered in cavities <1/2 the tooth width and without signs of bruxism. A direct restoration is less invasive and will reduce pulpal trauma. It has been demonstrated that >90% of teeth restored with resin-composite remained vital after 7 years.1 There are some reservations with regards to bonded amalgam owing to a difference in thermal expansion coefficient which may be ineffective at limiting crack propagation.2
Indirect inlays
Indirect inlays are available as gold (Figure 1), ceramic or resin-composite. However, this form of treatment is not advised owing to their limited role in the management of cracked teeth. Additionally, considering their wedge retention design, there is a high risk that inlays will exert pressure on the cavity walls thereby exacerbating the crack line(s).
Figure 1. Gold inlay UR5.
Indirect onlays
Indirect onlays (Figure 2) may be used as a more conservative approach, with reduced trauma to the pulp. Indirect materials generally include gold (type III), cobalt chromium, lithium disilicate (pressed or milled) and composite (nanofill or nanohybrid). Indirect composite has demonstrated a six-year survival rate at 93%.3
Figure 2. (a, b) Indirect resin-composite onlay used to restore the LL6. (c, d) Lithium disilicate onlay restoring the UL6. (e, f) Gold onlays restoring the posterior teeth on the upper and lower arches.
Direct onlays
Direct resin-composite onlays (Figure 3) are cost-effective, aesthetic and minimally invasive; an important consideration if the pulp has already been traumatized over a period of time, presenting with symptoms of reversible pulpitis. These demonstrate high success rates for the treatment of cracked teeth, namely 100% over seven years4 and 72.7% over 11 years.5 Furthermore, considering that 20% of cracked teeth eventually require root canal therapy, a resin-composite onlay can easily be repaired if an endodontic access cavity is required in the future as it can be replaced with an indirect restoration. Bonded amalgam has poor aesthetics and reduced bond strengths to tooth structure compared with resin-composite. However, bonded amalgam demonstrates success rates comparable to an onlay.6
Figure 3. (a) Direct resin-composite onlays LL4 and LL6 which were placed over 2 years ago. The conformative approach was used at the time of placement, however, minor occlusal adjustments are now necessary. (b) LL6 amalgam onlay (without dentine pins) which has been in situ for approximately 15 years without issue and the tooth is still vital.
Full coverage crowns
Full coverage crowns are a highly destructive treatment modality and a significantly higher proportion of teeth treated in this manner lead to root canal treatment compared with the other methods of restoration.7 Post-crowns, particularly for molar teeth, should be avoided where possible in favour of adhesively bonded restorations due to the increased risk of procedural errors and the effects that the procedure will have on the apical seal of the root canal filling. Root fractures may also occur following the removal of sound tooth structure and weakening of the root (Figure 4).8
Figure 4. (a, b) Catastrophic failure of post-crown restoration.
Root canal therapy
This article will not consider the different factors influencing the prognosis or recommended protocols related to performing the endodontic procedure, as this has already been extensively covered in a recent series in Dental Update (Modern Endodontic Principles Parts 1–8 – Dent Update 2015; 42(7) 599–611 – 2016; 43(5) – 430–441). Instead, it will summarize the differential diagnoses and the restorative implications after the tooth has been root-filled.
Diagnosis
It is beyond the scope of this article to discuss all the relevant clinical and radiographic diagnostic procedures necessary to determine pulp health. However, a brief insight into pulpal complications commonly associated with failing restorations may help the reader draw comparisons and find similarities between the signs and symptoms of endodontic conditions with those of cracked teeth and occlusal trauma (Table 1).
Diagnoses
Signs and Symptoms
Reversible pulpitis
Increased response to cold, hot and sweet, which is non-lingering in natureMay give exaggerated response to pulp testingNormal radiographic appearance
Symptomatic irreversible pulpitis
Lingering pain following hot and cold fluidsInitially episodic in nature and progresses into a constant severe painDifficult to localize the pain initially, but once the periodontal ligament is involved the patient can locate the toothA widened periodontal ligament may be seen in later stagesIrreversible pulpitis can alternatively be asymptomatic or hyperplastic
Pulpal necrosis
No responses to pulp testing and is normally pain free
Symptomatic acute apical periodontitis
Painful to biting and/or percussion or palpationVariable clinical symptoms – mild discomfort to extreme painIt may or may not have an apical radiolucent area
Non-symptomatic acute apical periodontitis
Longstanding inflammatory condition with no clinical symptomsApical radiolucent area on radiograph.
Acute apical abscess
Swelling and/or exudate presentRapid onset, spontaneous pain and extremely tender to pressureWidening of the periodontal ligament
Chronic apical abscess
Gradual onset with minimal discomfortSinus tract may be present with discharge of pusAppears as apical radiolucent area radiographically
Following discussion of the previous topics, it should be clear how a clinical misdiagnosis could easily be made under certain circumstances, particularly when the patient is likely to attend at short notice as an emergency appointment! Furthermore, a combination of factors could be overlooked, for example, a cracked molar with signs of reversible pulpitis which is also a working side interference. This reiterates the importance of a thorough evaluation of the patient history, clinical examination and a holistic approach with consideration of alternative potential aetiologies.
Treatment considerations
It is important to preserve pulp vitality where possible, as the best root-filling is the living pulp tissue. Therefore, when there is any uncertainty regarding the diagnosis, it is recommended to place a sedative or biomimetic (eg Biodentine™, Septodont) dressing following removal of caries and the old restoration. The tooth should subsequently be kept under regular review at following appointments. However, when it is clear that the pulp has been irreversibly damaged, then prevention of infection and peri-apical disease becomes the new priority.9
The heavily restored tooth, in which the restoration has been present for a length of time, may result in irreversible pulpitis. This is normally due to leakage which includes:
Caries: previously known as secondary and recurrent caries, but it is now termed Caries Associated with Restorations/Sealants (CARS);
Marginal breakdown of the restoration.
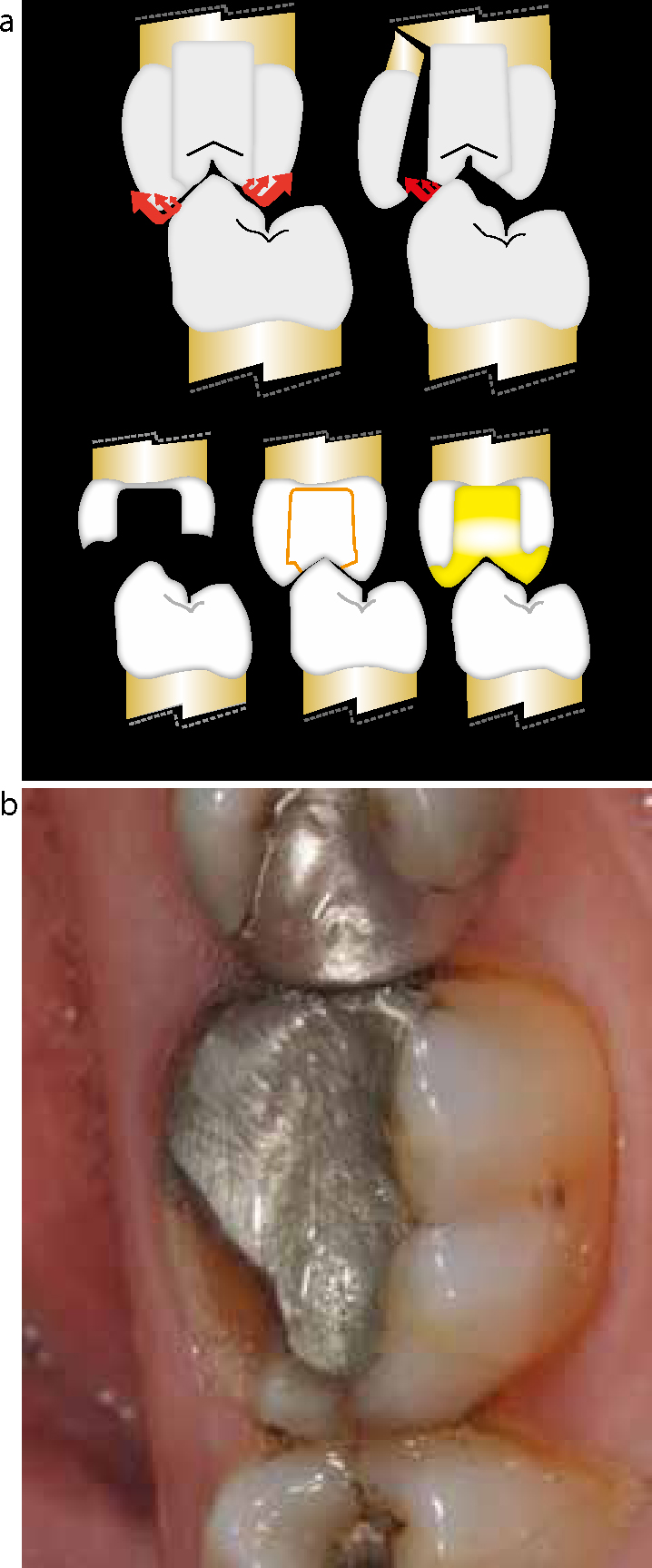
Therefore, it is advisable to remove the old coronal restoration prior to commencement of endodontic treatment so that the cause for the leakage does not go undetected. This also aids accurate assessment, prognosis and facilitates visualization during treatment. Importantly, endodontic procedures reduce tooth stiffness by 5%,8,9 the presence of an occlusal restoration reduces stiffness by 20%,9,10 and a mesial-occlusal-distal (MOD) restoration reduces stiffness by 63%. Furthermore, proprioception is reduced by 30% following root canal treatment,9,10 predisposing the tooth to higher occlusal forces due to a lack of preventive biofeedback from the pulp.8 With this information in mind, heavily restored, endodontically treated molars and premolars, weakened by the loss of one or more marginal ridges and a cavity >1/2 of the tooth width, should be provided with cuspal protection in the form of an onlay or crown (Figure 5).9 Otherwise, the tooth will be at high risk of cuspal fracture, cracked tooth and/or split tooth (as previously discussed) which may lead to extraction.
Figure 5. (a) The importance of occlusal coverage to avoid tooth fracture.8 (b) Clinical situation of a LR6 with a fractured lingual cusp. This was root canal treated without cuspal coverage and restoration is >1/2 the tooth width; an onlay or crown should be considered in this situation.
Crack formation within the tooth structure is another source of leakage with regards to restored and non-restored teeth. A cracked tooth has a high risk of pulpal complications due to bacterial penetration combined with chronic thermal sensitivity. Moreover, it has been reported that the proportion of cracked teeth requiring RCT increases with increasing probing depths, therefore those >4 mm will have a poor prognosis.10 Interestingly, despite the initially high failure rates of root-treated cracked teeth demonstrated by Tan et al11 (14.5% over two years), a more recent study by Kang et al12 demonstrated a 95% success rate after 5 years. Clearly, further research is required in this area to formulate a predictable long-term prognosis of a root-treated cracked tooth and the influence of underlying factors, such as crack extension.
Therefore, in the author‧s opinion, any cracked tooth that has been root-filled should be provided with a direct resin-composite onlay. This will provide a suitable restorative solution, whilst avoiding additional patient costs and time for treatment. The tooth should then be kept under regular review and, if non-symptomatic, then the restoration can either be left in situ, or it can be replaced with an indirect onlay if the clinician feels that this is appropriate.
Conclusions
Full occlusal coverage restorations are the most appropriate form of treatment with regard to cracked teeth. Direct composite or indirect onlay restorations can be considered as the ideal treatment options as they are minimally invasive, thereby minimizing the risk of additional trauma to an already weakened tooth.
When failure of a large restoration occurs, the clinician must always assess for pathology, radiographically and clinically, prior to the provision of definitive treatment. Importantly, the reason(s) for restoration failure should be clearly understood and all attempts must be made to retain the pulp vitality where possible. However, when this is not practical, or where previous attempts failed, root canal therapy should be initiated as soon as possible. Under most circumstances, the majority of posterior teeth with a root filling will require a cuspal protection restoration for long-term, post-operative stability. Consideration should be given to a direct resin-composite onlay where cracks are present within the tooth structure.