Sigurdsson A, Trope M, Chivian N Traumatismos dentales y endodoncia, 10th edn. In: Hargreaves KM, Cohen S, Berman LH Barcelona: Elsevier; 2011
Pace R, Giuliani V, Pagavino G Mineral Trioxide aggregate in the treatment of external invasive resorption: a case report. Int Endod J. 2008; 41:258-266
Heithersay GS Clinical, radiologic and histopathologic features of invasive cervical resorption. Quintessence Int. 1999; 30:27-37
Smidt A, Nuni E, Keinan D Invasive cervical root resorption: treatment rationale with an interdisciplinary approach. J Endod. 2007; 33:1383-1387
Llena-Puy MC, Amengual-Lorenzo J, Forner-Navarro L Idiopathic external root resorption associated to hypercalciuria. Med Oral. 2002; 7:192-199
Belanger GK, Coke JM Idiopathic external root resorption of the entire permanent dentition: report of case. J Dent Child. 1985; 52:359-363
Heithersay GS Invasive cervical resorption: an analysis of potential predisposing factors. Quintessence Int. 1999; 30:83-95
Nakamura I, Takahashi N, Sasaki T, Jimi E, Kurokawa T, Suda T Chemical and physical properties of the extracellular matrix are required for the actin ring formation in osteoclasts. J Bone Miner Res. 1996; 11:1873-1879
García Ballesta C, Pérez Lajarín L, Cortés Lillo O Alteraciones radiculares en las lesiones traumáticas del ligamento periodontal: revisión sistemática. RCOE. 2003; 8:197-208
Levi L, Trope M Root resorption, 1st edn. In: Hargreaves K, Goodis H Chicago: Quintessence Publishing; 2002
Matsuda E Ultrastructural and cytochemical study of the odontoclasts in physiologic root resorption of human deciduous teeth. J Electron Microsc. 1992; 41:131-140
Okamura T, Shimokawa H, Takagi Y, Ono H, Sasaki S Detection of collagenase mRNA in odontoclasts of bovine root-resorbing tissue by in situ hybridization. Calcif Tissue Int. 1993; 52:325-330
Sahara N, Toyoki A, Ashizawa Y, Deguchi T, Suzuki K Cytodifferentiation of the odontoclast prior to the shedding of human deciduous teeth: an ultrastructural and cytochemical study. Anat Rec. 1996; 244:33-49
Ahmed N, Mony B, Parthasarthy H External cervical resorption case report and brief review of literature. J Nat Sci Biol Med. 2014; 5:210-214
Sasaki T, Motegi N, Suzuki H, Watanabe C, Tadokoro K, Yanagisawa T, Higashi S Dentin resorption mediated by odontoclasts in physiological root resorption of human deciduous teeth. Am J Anat. 1988; 183:303-315
Patel S, Ford TP Is the resorption external or internal?. Dent Update. 2007; 34:218-229
Patel S, Dawood A The use of cone beam computed tomography in the management of external cervical resorption lesions. Int Endod J. 2007; 40:730-737
Gulabivala K, Searson LJ Clinical diagnosis of internal resorption: an exception to the rule. Int Endod J. 1995; 28:255-260
Cohenca N, Simon JH, Roges R, Morag Y, Malfaz JM Clinical indications for digital imaging in dento-alveolar trauma. Part 1: traumatic injuries. Dent Traumatol. 2007; 23:95-104
Estevez R, Aranguren J, Escorial A, de Gregorio C, De La Torre F, Vera J, Cisneros R Invasive cervical resorption class III in a maxillary central incisor: diagnosis and follow-up by means of cone-beam computed tomography. J Endod. 2010; 36:2012-2014
Patel S, Kanagasingam S, Pitt Ford T External cervical resorption: a review. J Endod. 2009; 35:616-625
Gulabivala K, Searson LJ Clinical diagnosis of internal resorption: an exception to the rule. Int Endod J. 1995; 28:255-260
Heithersay GS Treatment of invasive cervical resorption: an analysis of results using topical application of trichloracetic acid, curettage, and restoration. Quintessence Int. 1999; 30:96-110
Gulsahi A, Gulsahi K, Ungor M Invasive cervical resorption: clinical and radiological diagnosis and treatment of 3 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103:e65-e72
Kitchens JA, Schwartz SA, Schindler WG, Hargreaves KM Iontophoresis significantly increases the transdentinal delivery of osteoprotegerin, alendroate and calcitonin. J Endod. 2007; 33:1208-1211
Warshawsky H, Goltzman D, Rouleau MF, Bergeron JJ Direct in vivo demonstration by radioautography of specific binding sites for calcitonin in skeletal and renal tissues of the rat. J Cell Biol. 1980; 85:682-694
Vinothkumar TS, Tamilselvi R, Kandaswamy D Reverse sandwich restoration for the management of invasive cervical resorption: a case report. J Endod. 2011; 37:706-710
Roig M, Morelló S, Mercadé M, Durán-Sindreu F Invasive cervical resorption: report on two cases. Oral Surg Med Oral Pathol Oral Radiol Endod. 2010; 110
Hiremath H, Yakub SS, Metgud S, Bhagwat SV, Kulkami S Invasive cervical resorption: a case report. J Endod. 2007; 33:999-1003
Yilmaz HG, Kalender A, Cengiz E Use of mineral trioxide aggregate in the treatment of invasive cervical resorption: a case report. J Endod. 2010; 36:160-163
Schwartz RS, Robbins JW, Rindler E Management of invasive cervical resorption: observations from three private practices and a report of three cases. J Endod. 2010; 36:1721-1730
Fernández R, Rincón JG Surgical endodontic management of an invasive cervical resorption class 4 with mineral trioxide aggregate: a 6-year follow-up. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011; 112:e18-e22
Quirynen M, Van Assche N, Botticelli D, Berglundh T How does the timing of implant placement to extraction affect outcome?. Int J Oral Maxillofac Implants. 2007; 22:203-223
Barone A, Rispoli L, Vozza I, Quaranta A, Covani U Immediate restoration of single implants placed immediately after tooth extraction. J Periodontol. 2006; 77:1914-1920
Aetiological, histopathological, clinical, diagnostic and therapeutical features of idiopathic cervical resorption Virginia Robles Gijón Cristina Lucena Martín Rosa Ma Pulgar Encinas José Manuel Navajas Dental Update 2024 43:10, 707-709.
Authors
Virginia RoblesGijón
MD, DDS, PhD
Assistant Professor, Department of Conservative Dentistry, School of Dentistry, University of Granada, Spain (vroble@ugr.es)
Root resorption is the loss of hard dental tissue as a result of odontoclastic action involving vital and pulpless teeth. Cervical root resorption (CRR) is a type of external resorption which usually occurs immediately below the epithelial attachment of the tooth in the cervical region. The idiopathic cervical resorption (ICR) refers to a clinical situation in which all other causes, whether local or systemic, have been ruled out as the origin of the disease. The early stage is asymptomatic and might be diagnosed by a routine radiograph or a clinical examination. In this study, the aetiological, histological, clinical and radiological analysis is undertaken; a review is made concerning the pathologies to which the differential diagnosis should be applied; and the different therapeutical options are discussed. This lesion sometimes demands the management of a broad field of multidisciplinary techniques such as restorative dentistry, endodontics, surgery, implants and prosthesis.
CPD/Clinical Relevance: Cone-beam computed tomography (CBCT) may be a useful tool to determine the true extent of external cervical resorption lesions.
Article
Root resorption is the loss of hard dental tissue as a result of odontoclastic action.1 There are two different types of root resorption, depending on location: internal and external. Cervical root resorption (CRR) is a type of external resorption which usually occurs immediately below the epithelial attachment of the tooth in the cervical region.2 It commonly affects mineralized tissues (cementum and dentine), and, except for some advanced stages, the predentine layer protects the pulp tissue because it is less mineralized. CRR defects can be difficult to diagnose and manage. This article provides a brief review of the aetiology, pathology, histology, clinical diagnosis and therapeutic options of CRR.
Aetiology
The aetiology of CRR is difficult to determine with certainty. In most cases a causal relation can be established, with different local predisposing factors such as dental trauma,3 orthodontic treatment,4 periodontal diseases and their treatments3 or intracoronal bleaching.5 Also, systematic pathologies can play a role in this type of resorption, although it is usually not possible to associate the two pathologies.6 Authors such as Gutmann et al6 and Llena-Puy et al7 have described a mild association of this type of resorption with a record of hypercalciuria and renal lithiasis. Finally, idiopathic root resorption (IRR) refers to a clinical situation in which all other causes, whether local or systemic, have been ruled out as the origin of the disease.8 According to Heithersay,9 15% of the patients have no predisposing factors.
Pathology
The pathogenic mechanism behind root resorption is unknown. Tooth cement and predentine are essential in root resistance to resorption, since the most external part of the cement (demineralized cementoid) is covered by a layer of cementoblasts, which constitute an unsuitable surface for the adhesion of clastic cells.10 Root resorption is started by damage to the precementum or predentine and odontoblast layer, resulting in exposure of the mineralized cementum or dentine, respectively. The clastic cells rapidly colonize the damaged root surface and will then start resorbing it. This beginning is due to the fact that the clastic cells bond to extracellular arginineglycine-aspartic acid (RGD) tripeptide proteins, which in turn bond to calcium crystals of the mineralized surfaces.11 After this bonding, the clastic cells secrete an acid solution that contains proteolytic enzymes (vacuolar H+ATPase and carbonic anhydrase); this begins the decalcification12 and subsequent degradation of the collagen and non-collagen organic matrix,13,14 resorbing both the dentine as well as the predentine.15
Histology
Cemento-enamel disjunction, ie where there is a fault at the junction of the enamel and dentine, has been recognized as risk factor. Physical or chemical injury can lead to damage to bone, cementum or dentine. This can trigger chemical changes within the affected tissues and can start the resorptive process.16
Histologically, the cells responsible for the resorption of the calcified dental tissues have morphological and biochemical characteristics of clastic cells. Generally, these are multinucleate, although they can sometimes be mononucleate. They come from mononucleate precursors that belong to the monocyte/macrophage lineage, as do osteoclasts, and ultrastructurally have similar characteristics.17
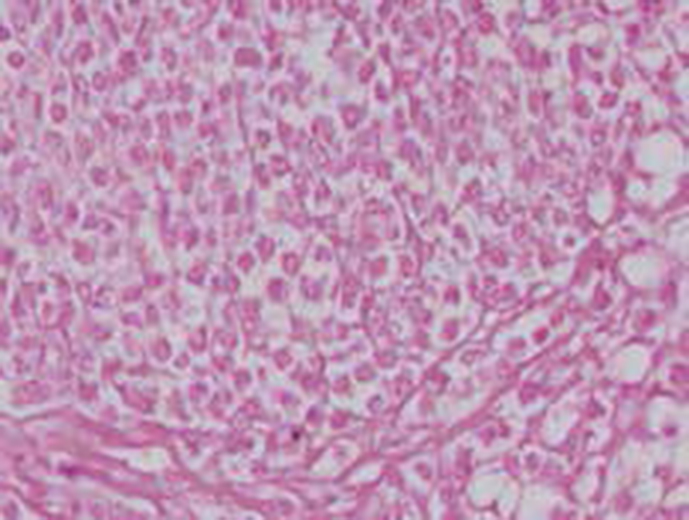
Figure 1 presents an incisor extracted with IRR. Histological evaluation revealed the presence of connective tissue replacing the hard dental structures, composed essentially of monomorphic cells of clear cytoplasm and scattered giant cells of osteoclastic appearance and accumulations of cells that appeared to be histiocytes. The presence of giant cells similar to the osteoclasts indicated resorption.
Figure 1. Maxillary central incisor with ICR: the histological examination shows monomorphic cells, giant cells, osteoclastic in appearance, and some cell accumulations, apparently histiocytes (Oral Medical Unit of the Odontology Faculty, University of Granada, Spain).
Clinical
Clinically, cervical root resorption can begin and progress asymptomatically. When the lesion is visible, the aspect varies from a small defect at the gingival margin (Figure 2) to a pink discoloration of the tooth crown (Figure 3). This discoloration is a result of the highly vascular granulation (resorptive) tissue within the tooth becoming visible through the thinned out (resorbed) dentine and translucent overlying enamel.18 The pink colour at the level of the cervical region detected by the patient and/or the dentist is sometimes the first clinical sign of the problem, although the pathological condition may often go unnoticed until a pulp and/or periodontal problem arises.1
Figure 2. The presence of a small defect at the gingival margin, associated with the change in the underlying coloration, guides the clinician towards a diagnosis of idiopathic cervical resorption.Figure 3. Pink tooth.
Diagnosis
The resorptive condition is often detected by routine radiographic examination. Heithersay9 defined four levels of resorption according to the radiographic appearance of the process:
Class 1, a small, invasive resorptive lesion near the cervical area with shallow penetration into the dentine;
Class 2, a well-defined, invasive resorptive lesion that has penetrated close to the coronal pulp chamber but shows little or no extension into root dentine;
Class 3, a deeper invasion of dentine by resorbing tissue, involving not only the coronal dentine but also extending at least to the coronal third of the root;
Class 4, a large invasive resorptive process that has extended beyond the coronal third of the root canal.
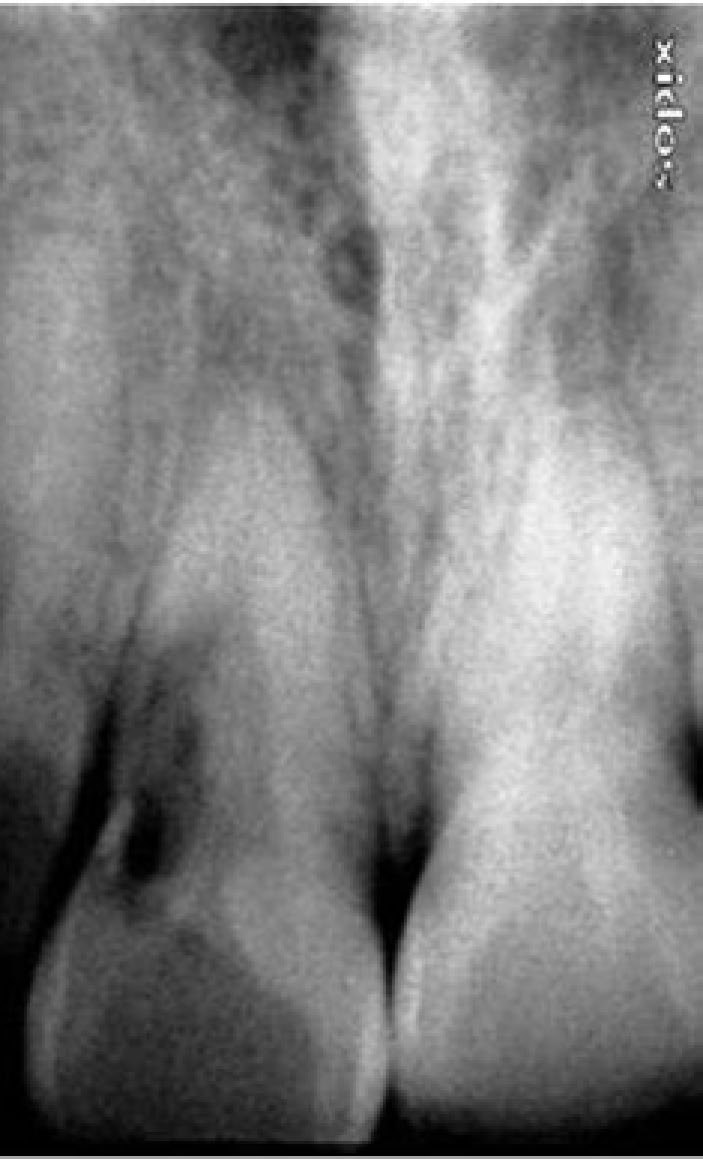
Classically, CRR appears as an image with well-defined or irregular radiolucent edges in the cervical region of the tooth (Figure 4). However, when the lesion progresses, it can have a mottled appearance that can be confused with dental caries (Figure 5).18 As is well known, this type of examination provides rather limited information on the extent of resorptive lesions.19 The use of CBCT to assess CRR lesions may help to determine their position and depth in relation to the root canal. CBCT is an extra-oral imaging technique that shows the area of interest in meso-distal and vestibule-lingual planes, enabling three-dimensional reconstructions. This vision in three dimensions provides a more exact idea, both of the position of the lesion as well as its depth. In addition, it offers advantages over conventional CT scans by lowering costs, submitting the patient to less radiation20 and, finally, avoiding unnecessary surgical exploration so that the restorability of the tooth can be assessed before treatment.19,21,22
Figure 4. Radiolucency restricted to the amelocemental junction area.Figure 5. Radiolucent lesion that extends to the middle third of the root.
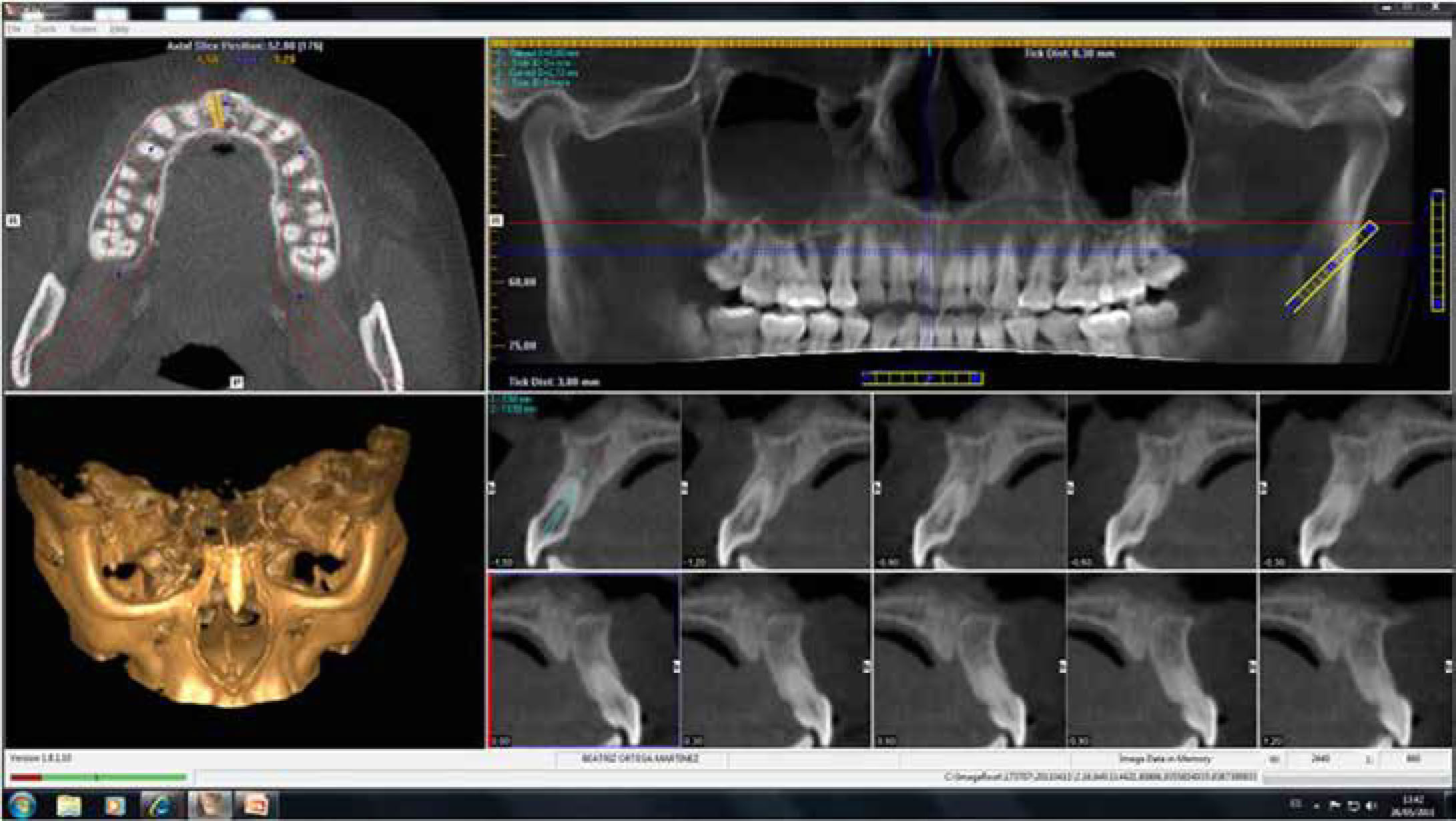
The diagnostic accuracy of CBCT has been demonstrated to be superior to conventional radiographs23 (Figures 6 and 7).
Figure 6. The cone-beam computerized tomography scan (CBCT) reveals the true extent of the resorption as well as the integrity of the root walls.Figure 7. CBCT detail showing the ICR entry at the level of the amelocemental junction area.
It is important to perform a differential diagnosis of CRRs with two fundamental pathologies: subgingival caries and internal root resorption. The differential diagnosis with subgingival caries is made by a clinical exploration in such a way that the caries will feel sticky on probing them and does not present with a pink spot,23 while the resorptive cavitation usually has sharp and tapered margins with a hard bottom and an underlying pink spot (Figure 8). The differential diagnosis must also be performed with internal resorption; the parallax technique is useful to follow the continuity of the pulp canal to distinguish between internal and external resorption.18 A second radiograph taken from a different mesiodistal angle would alter the relationship of the defect to the root canal in the case of external root resorption, but not in that of internal resorption.24
Figure 8. Typical morphology of the resorptive cavitation with sharp and tapered margins.
The clinical prognosis rests mainly on the extent of the resorptive process. The amount of the resorption serves as a guide for the clinician to select the best treatment. Therefore, the radiographic assessment of the resorptive process is crucial for the differential diagnosis, treatment and prognosis of the tooth.
Treatment options
The treatment of CRR depends on its severity, its location, or whether the lesion compromises or not the root canal system. Therefore the treatment options according to the amount of hard tooth tissue lost would be:
Surgical exposure of the lesion, debridement, and restoration.
Surgical exposure, debridement, and restoration preceded by endodontic treatment.
Tooth extraction and immediate implant with a temporary crown.
Tooth extraction and replacement with a prosthesis (removable prosthesis or fixed prosthesis).
No treatment, with eventual extraction of the tooth once it becomes symptomatic.
Heithersay9 stated that, in CRR Classes 1 and 2, practically 100% of the conservative treatments (A and B) were successful. In Class 3 the percentage of success dropped to 78% and, in Class 4, the percentage fell to 12.5%. Consequently, the recommendation is to treat only defects belonging to Classes 1 to 3, while extraction is proposed for Class 4 lesions.
With respect to the conservative approach, the overall aim of treating external resorption is the complete removal of resorptive tissue, the restoration of the defective area and the prevention of further resorptions.23 Endodontic treatment will be necessary in those cases in which the CRR lesion had perforated the root canal.
The restoration phase often requires vestibular-flap surgery23 to gain complete access to the resorption lacuna (Figure 9). Heithersay25 recommended topical application of 90% aqueous solution of trichloroacetic acid (TCA) and curettage of the lesion. The trichloroacetic acid produces the coagulation and necrosis of the resorptive tissue,25 thus avoiding the persistence of remains of the affected tissue18,26 since, if this occurred, it would have a high probability of relapse in the future.23
Figure 9. Vestibular-flap surgery.
A recent study by Kitchens et al27 has suggested a new method of treatment of CRR that involves chemo-mechanical debridement of the root canal, obturation of the apical part of the canal, removal of the smear layer, and subsequent iontophoretic delivery of calcitonin via the dentinal tubules directly to the CRR lesion. Calcitonin is a polypeptide responsible for inhibitory action on osteoclasts via specific cell receptors. It might also act to inhibit odontoclast activity directly and to suppress inflammation.28 Further research is required before this option can be routinely recommended in the treatment of CRR.
Ideally, the restorative material chosen for these types of lesions should reinforce the remaining tissues, should have a coefficient of thermal expansion close to that of the dental structure, and should be biocompatible.29 The most commonly used materials are: composite resin,30 glass-ionomer cement,31 and mineral trioxide aggregate.16,18,32 Before any adhesive process, Schwartz et al33 consider it necessary to ‘refresh’ the dentine because the TCA severely demineralizes it. Vinothkumar et al29 proposed a new technique called a ‘reverse sandwich restoration’ (RSR), consisting of placing a 1-mm layer of micro-filled resin composite and restoring the remnants of the defect with resin-modified glass-ionomer cement (RMGIC). The micro-filled resin was used together with RMGIC because they tend to flex with the tooth rather than debond, as occurs with the more rigid macro-filled resin. Compared to conventional sandwich restoration, RMGIC forms a significantly stronger bond to cured resin composite in RSR than that of resin composite to cured RMGIC in the absence of etching; the development of subgingival plaque over RMGIC is prevented by achieving a smooth finish using the cervical matrix.29
In any case, it is highly advisable that the restorative procedures mentioned above are performed under isolation with rubber dam (Figure 10). The absolute isolation improves visibility providing the indispensable conditions of isolation required for endodontic treatments and improving the quality of adhesion procedures (Figures 11 and 12). Also, it protects adjacent tissues from the caustic effects of TCA, thereby avoiding burns.23,33
Figure 10. Isolation with rubber dam.Figure 11. The isolation with rubber dam improves the quality of adhesion procedures.Figure 12. Resin composite restoration completed.
Some authors, such as Schwartz et al33 and Fernández and Rincón34 have described conservative treatment of Class 4 CRR that was successful in follow-ups of 10 and 16 years, respectively. However, these cases involved patients of 80 and 67 years old, respectively, which have refused tooth extraction; therefore, their circumstances and their desires determined the design of the treatment plan. In fact, the authors themselves33 called this type of treatment ‘heroics’, an example of this being a woman 80 years old (mother of one of the authors) presenting a Class 4 lesion in the right maxillary central incisor. In this case the treatment included an endodontic, zirconium post, and ‘open sandwich’ restoration.
In Class 4 CRR, the tooth extraction is the chosen treatment followed by prosthetic repositioning. The treatment options should be discussed with the patients and the most suitable chosen according to the needs of the patient and the recommendations of the professional. These include:
Immediate removal of the prosthesis;
Immediate denture placement followed by resin-retained bridges (RRB);
Long-term prosthesis removal;
A fixed prosthesis; and
Standard or immediate implant placement (6 weeks) with a temporary crown.
Heithersay9 recommends, in most cases of Class 4 CRR, tooth extraction and immediate implant placement as the chosen treatment, because this option guarantees long-term results, offers a reliable prognosis, and provides an immediate aesthetic result. The advantages of immediate implant placement include fewer surgical operations and less treatment time.35 Authors, such as Barone et al,36 suggest that this type of treatment is a good option, especially in the case of only one tooth being compromised, as it eliminates the need for a temporary bridge and appears to maintain the pre-existing architecture of soft and hard tissues, in most cases.
Conclusion
It can be concluded that CRR is a difficult pathology to diagnose before clinical symptoms of pulp or periodontal problems arise. Given that early detection is essential for the best management of CCR, the dentition of patients with a CCR lesion and no apparent identifiable aetiological factors should be thoroughly assessed to ensure that no other teeth are affected by CCR.
CBCT provides the better information on the true extent of lesions, helping the clinician to recommend the most appropriate treatment without the need for prior surgical exploration.
It can also be concluded that the treatment of this type of lesion demands the management of a broad field of multidisciplinary techniques such as restorative dentistry, endodontics, surgery, implants and prosthesis.