Sjögren U, Figdor D, Persson S, Sundqvist G Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J. 1997; 30:297-306
Gulabivala KLondon, UK: University of London; 2004
Friedman S, Löst C, Zarrabian M, Trope M Evaluation of success and failure after endodontic therapy using glass ionomer cement sealer. J Endod. 1995; 21:384-390
Imura N, Pinheiro ET, Gomes BP, Zaia AA, Ferraz CC, Souza-Filho FJ The outcome of endodontic treatment: a retrospective study of 2000 cases performed by a specialist. J Endod. 2007; 33:1278-1282
Allen RK, Newton CW, Brown C A statistical analysis of surgical and nonsurgical endodontic retreatment cases. J Endod. 1989; 15:261-265
Cheung GS, Chan TK Long-term survival of primary root canal treatment carried out in a dental teaching hospital. Int Endod J. 2003; 36:117-128
Chu FC, Tsang CS, Chow TW, Samaranayake LP Identification of cultivable microorganisms from primary endodontic infections with exposed and unexposed pulp space. J Endod. 2005; 31:424-429
Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2006; 39:921-930
McDonald A, Setchell DJ Developing a tooth restorability index. Dent Update. 2005; 32:343-348
Recent Trends in Life Expectancy at Older Ages. 2015;
Cvek M, Granath L, Lundberg M Failures and healing in endodontically treated non-vital anterior teeth with post traumatically reduced pulpal lumen. Acta Odontol Scand. 1982; 40:223-228
Sjögren U, Hägglund B, Sundqvist G, Wing K Factors affecting the long-term results of endodontic treatment. J Endod. 1990; 16:498-504
Vertucci FJ Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984; 58:589-599
Krasner P, Rankow HJ Anatomy of the pulp-chamber floor. J Endod. 2004; 30:5-16
Successful root canal treatment requires management of the bacterial infection within the root canal space and protection of residual tooth structure with direct/indirect restorations. Long-term success depends upon prevention of re-infection of the root canal space as well as ensuring favourable distribution of the occlusal forces throughout the residual tooth structure. Appropriate planning and design of the final restoration prior to initiating root canal treatment is paramount in achieving this objective. This article describes simultaneous restorability assessment and access cavity preparation to optimize outcome of both endodontic and prosthodontic treatment of the endodontically involved tooth.
CPD/Clinical Relevance: This paper proposes a method to improve visibility and reduce iatrogenic errors whilst simultaneously facilitating effective design of the definitive restoration based on the quantity and distribution of residual tooth structure.
Article
The purpose of providing root canal treatment is to retain teeth as functional and/or aesthetic units of the dentition. To achieve this objective, the following criteria must be fulfilled:
The bacterial infection within the root canal system must be reduced to a level that allows a favourable environment for periapical healing;1
The tooth must be restored with a restoration that prevents coronal leakage and protects remaining tooth tissue from further damage.2
Successful decontamination of the root canal system alone is not sufficient to ensure long-term survival of the tooth as a functional unit. Effective pre-operative assessment of the strategic importance of the tooth in the context of the overall dentition, its periodontal support, the opposing dentition, static and dynamic occlusal forces on the tooth in question and the amount and distribution of residual tooth structure allow for careful case selection of teeth that are worth retaining with a favourable medium- to long-term prognosis.
The definitive restoration must seal the root canal space from the oral cavity as well as preserve and protect the residual tooth structure by ensuring even distribution of the occlusal forces. Endodontically treated teeth may be restored either directly, with plastic filling materials (amalgam, composite resin), or indirectly with cast partial, cast full or all-ceramic restorations. Aesthetics, functional requirements, financial considerations and the patient expectations are all to be considered when selecting the definitive restoration.
Definitive guidelines on the restoration of endodontically treated teeth do not currently exist due to a lack of satisfactory evidence. Establishing an evidence base based on randomized controlled clinical trials has not been possible to date, owing to the difficulty in structuring such a study in an ethical way, as well as the sample size required for statistically significant data. The literature is replete with retrospective studies which have not been standardized and therefore cannot be considered as a high level of evidence.
Choosing the appropriate restoration type is often a personal decision for the clinician based on clinical findings in individual cases. Operator and patient preference, as well as economic factors, also play a significant role. The literature does, however, lend itself to certain recommendations. Teeth without permanent restoration, with temporary restorations and with gutta-percha filling material exposed to the oral environment were found to be associated with significantly lower success rates than those containing a definitive restoration.3,4,5 Root-treated teeth with extra-coronal restorations were associated with significantly better survival than their contrary counterparts.6,7
The European Society of Endodontology (ESE) guidelines state that an adequate restoration should be placed after root canal treatment to prevent subsequent bacterial recontamination and tooth fracturing.8 The difficulty arises in selecting the most appropriate restoration that will result in the long-term survival of the tooth. McDonald and Setchell attempted to standardize the process of restorability assessment with the introduction of ‘The Restorability Index’.9 This is a welcome step in the right direction towards standardizing restorability assessment. This publication also suggests removing all of the restorative material. The restorability and definitive restoration may be decided upon on removal of the restorative material, or having prepared the tooth for an extra-coronal restoration prior to initiating endodontic treatment by categorizing the distribution and thickness of residual tooth structure.
The debate continues as to whether a dental implant-retained prosthesis or root canal treatment and an appropriate restoration is superior. Where adequate sealing of the root canal system and protection of residual tooth structure cannot be predictably achieved, extraction with or without prosthodontic replacement is prudent. However, where an adequate endodontic treatment and definitive restoration can be provided, this should always constitute the first choice treatment. This allows patients to retain their natural tooth in function, delaying or removing the need for the provision of a dental implant.
Dental implants do not command a 100% success rate. If a dental implant fails or is unsatisfactory, the patient options are then limited, particularly if the natural tooth is lost in the third or fourth decade of life. With life expectancy in the UK on the increase,10 the patient is best served by delaying the placement of a dental implant and maintaining the natural dentition for as long as is practical.
Access cavity preparation
The first operative stage of root canal treatment is access cavity preparation. The phrase ‘access is success’ is well founded. Primary root canal treatments in which iatrogenic perforations occurred were found to have significantly lower success rates.4,11,12 Whilst there is a relatively common anatomy to each tooth type in the human dentition,13 inter-individual variations make the process of access cavity preparation a bespoke process for each tooth.
Publications such as ‘Anatomy of the pulp-chamber floor’14 provide guidance notes and laws that aid in access cavity design and finding canal orifices: ‘Because the fundamental foundation on which all surgical procedures are performed is an intimate knowledge of anatomy, any attempt to perform endodontic therapy must be preceded with a thorough understanding of the anatomy of both the pulp chamber and the root-canal system'.14 Therefore, knowledge of the common anatomy of the pulp chamber and root canal systems of various teeth is the first key factor in success. A significant amount of information may also be obtained from the pre-operative radiograph which can guide access cavity design, as well as act as an intra-operative guide for depth and location of anatomical structures.
Conventional access cavity preparation can be made easier with the use of magnification and lighting. Magnification loupes and LED lights or an operative microscope improve visualization within the access cavity when prepared through existing restorations. The shadow cast from the surrounding tooth structure/restorative material can limit visualization of pulp chamber anatomy.
Restorability assessment
Root canal treatment may be completed without due consideration to the requirements of the definitive restoration. Whilst a technically excellent root canal treatment may have been completed, if there is insufficient tooth structure to retain either a direct or indirect restoration that will prevent coronal leakage and protect remaining tooth tissue from further damage, this may lead to a situation where the tooth requires extraction.
In a time where implant-retained prostheses are being increasingly prescribed over retention of a natural tooth via root canal treatment, which is perceived by many as having a lower success rate, it is important that endodontic treatment is performed on teeth with a reasonable medium- to long-term endodontic and prosthodontic prognosis. Providing root canal treatment on teeth that were unrestorable in the first instance only serves to skew the data in favour of implant-retained prostheses and fuel a perception amongst patients that root canal treatment results in the tooth being extracted anyway.
The decision to remove existing restorations or access the root canal system with the restoration in situ is complex. Aesthetics, financial considerations and time constraints all play a role. Whilst there are no guidelines, it is best practice to remove all restorative materials, direct or indirect restorations, except where the clinician providing the root canal treatment personally placed the direct/indirect restoration and documented that there was sufficient residual tooth structure should root canal treatment be required. The tooth must also show no signs of clinical marginal deterioration or radiographic signs of recurrent caries.
Despite having been advised that the direct/indirect restoration should be removed for restorability assessment, on occasion patients may express a wish to proceed through the existing restoration or forego a cuspal coverage restoration, mainly for financial reasons. In this instance, patients should be warned that the success of the root canal treatment may be compromised and the long-term survival of the tooth as a functional unit may be guarded. If the clinician feels that this treatment is inappropriate and that the root canal treatment should not be initiated without a restorability assessment, the importance of these preceding steps must be conveyed to the patient and an alternative treatment plan should be devised should the patient not wish to proceed in this manner.
Removal of all restorative material confers the following advantages:
Ensures that the tooth is restorable prior to initiating endodontic treatment. Radiographs and the clinical appearance of restorations can be deceptive and the certainty of restorability is obtained by inspecting the residual tooth structure on its own merits;
Allows better visualization and lighting of the roof of the pulp chamber;
Facilitates identification and visualization of any cracks present and their depth;
Reduces the amount of tooth structure removed to access the root canal orifices;
Ensures the root canal system is sealed circumferentially following placement of a temporary restoration, which cannot be guaranteed with existing restorations which may have marginal leakage;
Facilitates decision-making in regards to core type (direct, indirect) and the need for a post which can be factored in at the time of obturation;
Removes interferences with electronic apex locators which occurs with metallic restorations;
Allows design and planning of the most effective definitive restoration once root canal treatment is complete.
Combined restorability assessment and access cavity preparation
The following case illustrates, step-by-step, the use of the restorability assessment to plan the definitive restoration simultaneously and make access cavity preparation easier.
Rubber dam should be placed exposing one tooth either side of the tooth to be treated (Figure 1). This ensures adequate isolation when the roof of the pulp chamber is breached but also allows for better evaluation of the margins of the cavity. If it is difficult to expose the margins of the cavity under rubber dam, this is a good indicator that placing a definitive resin composite restoration or preparing crown margins may not be feasible. (NB The occlusion should again be assessed prior to rubber dam placement as this is not possible once it is in situ).
Figure 1. Pre-operative view with rubber dam isolation.
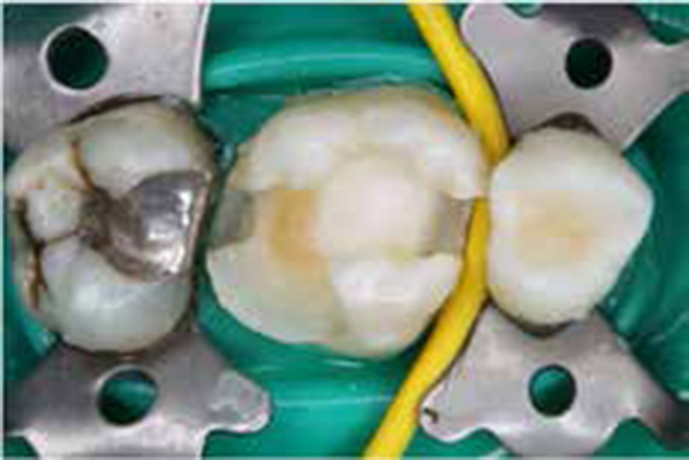
In the first instance, the existing restorative material(s) should be removed to evaluate the quantity and distribution of residual tooth structure, the accessibility of the restoration margins and the extent of any potential cracks adequately (Figure 2).
Figure 2. Intra-operative view with restorative material removed.
Owing to a lack of evidence or guidelines, the restorability assessment is subjective. However, clinicians should decide if the tooth is restorable by visualizing the final restoration and asking questions such as:
Can I achieve an adequate seal at the margins of the tooth with a direct restoration?
Does the residual tooth structure require cuspal coverage to prevent further fracture?
Would the margins be amenable to preparation of a crown margin?
Would there be a sufficient ferrule to retain an extra-coronal restoration?
What type of core material would be required? Would a post be needed to retain the core?
Is there sufficient enamel present to facilitate bonding of a composite resin restoration?
If the tooth is deemed restorable, the definitive restoration should be decided upon at this point. The need for any post/core material should also be finalized as this may influence the obturation technique selected during root canal treatment.
The outline of the access cavity should be prepared over the pulp chamber until the roof of the pulp chamber is perforated (Figure 3). Note the amount of light entering to the level of the pulpal roof and the increased visibility with the restorative material removed.
Figure 3. Intra-operative view showing initial outline of the access cavity over the roof of the pulp chamber which is breached over the MB canal (blue arrow).
The roof of the pulp chamber should be removed with a bur that has a non-cutting tip, such as the Endo-Z Bur (Dentsply Maillefer, Ballaigues, Switzerland). Care should be taken to ensure that the entire roof of the pulp chamber is removed and that straight-line access has been achieved for all canals (Figure 4). This method results in removal of less healthy tooth structure as the visibility is improved and the lack of a restorative material core allows for more precise and conservative removal of dentine.
Figure 4. Intra-operative view with the roof of the pulp chamber completely removed. (b) Crack penetrating into pulp chamber.
This also allows identification and better visualization of any cracks that may penetrate to the pulp chamber. A decision can then be made whether the tooth is restorable or not, depending on the cracks' depth of penetration and/or communication with the periodontal tissues (Figure 4b).
Once a satisfactory access cavity has been achieved and all canals have been located, the tooth needs to be temporized to ensure a four-walled access cavity to retain the irrigant. To achieve this, a cotton-wool pledget should be placed in the access cavity (Figure 5). A matrix band is then applied and the cavity filled with glass-ionomer cement (GIC). A small layer of CavitTM or VaselineTM may be placed over the cotton-wool pledget to prevent the cotton-wool pledget sticking to the GIC. GIC is the ideal choice for the temporary core material as it bonds to tooth structure, gives a good marginal seal and has acceptable wear characteristics.
Figure 5. Cotton pledget in access cavity.
Once the GIC has fully set, remove the matrix band, remove the excess GIC and polish the margins (Figure 6). At this point the tooth is ready to re-establish access to the root canal system and begin root canal treatment. (If there is concern regarding possible fracture of the residual tooth structure between appointments, an orthodontic/copper band can be placed to reinforce the tooth).
Figure 6. Temporary core material polished.
The access cavity is now established in the conventional manner by simply preparing an outline smaller than the actual size of the pulp chamber, the cotton wool is located easily and removed with an endodontic probe (Figure 7). Placing the Endo-Z bur into the access cavity, it quickly removes the excess glass-ionomer that overlays the cotton wool and quickly re-establishes the ideal access cavity without removing excessive amounts of dentine (Figure 8). The tooth is now ready for root canal instrumentation.
Figure 7. Initial outline of access cavity with cotton-wool pledget visible within the pulp chamber.Figure 8. Outline of the final access cavity.
If a multi-visit approach is adopted, a cotton-wool pledget can be placed in the pulp chamber, as previously described, and GIC or IRM™ may be used to temporize the access cavity (Figure 9). IRM™ has the advantage of being different in colour from glass-ionomer and makes re-establishing access at subsequent visits easier. It also possesses anti-bacterial qualities should any marginal leakage occur.
Figure 9. IRMTM temporary restoration in access cavity.
Discussion
Following the above steps can reduce, if not eliminate, the risks of iatrogenic damage associated with access cavity preparation, as well as the risk of performing root canal treatment on teeth that have a poor restorative prognosis. Cases where root canal treatment was provided without undertaking a restorability assessment to assess the feasibility of crown margin placement can leave, as in this case, the patient irate that he has spent many hours and hard earned money on this tooth which is already failing after 6 months due to the depth of the margin distally (Figure 10).
Figure 10. Root canal treatment was provided without undertaking a restorability assessment to assess the feasibility of crown margin placement.
Conclusion
This paper proposes a method to improve visibility and reduce iatrogenic errors during endodontic access cavity preparation whilst simultaneously facilitating effective design and planning of the definitive restoration based on the quantity and distribution of residual tooth structure. This procedure can be undertaken quickly and help to avoid unrestorable teeth undergoing root canal treatment.
This paper proposes a method of improving case selection for root canal treatment, by reducing iatrogenic errors in access cavity preparation and with better planning of definitive restorations.