Elderton RJ, Osman YI Preventive versus restorative management of dental caries. J Dent Assoc S Afr. 1991; 46:217-221
Elderton RJ Iatrogenesis in the treatment of dental caries. Proc Finn Dent Soc. 1992; 88:(1–2)25-32
Elderton RJ Overtreatment with restorative dentistry: when to intervene?. Int Dent J. 1993; 43:17-24
Hume WR Research, education, caries and care: taming and turning the restorative tiger. J Dent Res. 1992; 71
Kidd EA The diagnosis and management of the ‘early’ carious lesion in permanent teeth. Dent Update. 1984; 11:69-78
Elderton RJ The prevalence of failure of restorations: a literature review. J Dent. 1976; 4:207-210
Elderton RJLondon: London Hospital, Medical College; 1977
Elderton RJ Restorations without conventional cavity preparations. Int Dent J. 1998; 38:112-118
Elderton RJ Preventive (evidence based) approach to quality general dental care. Med Princ Pract. 2003; 12:12-21
Davies JA The relationship between change of dentist and treatment received in the general dental service. Br Dent J. 1984; 157:322-324
Mertz-Fairhurst EJ, Schuster GS, Failhurst CW Arresting caries by sealants: results of a clinical study. J Am Dent Assoc. 1986; 112:194-197
Ricketts DN, Kidd EA, Innes N, Clarkson JE Complete or ultraconservative removal of decayed tissue in unfilled teeth. Cochrane Database Syst Rev. 2006; 19
Browning WD, Chan DC, Swift EJ Critical appraisal: approaches to caries removal: What the clinical evidence says. J Esthet Rest Dent. 2013; 25:141-151
Kazemian A, Berg I, Finkel C How much dentists are ethically concerned about overtreatment; a vignette-based survey in Switzerland. BMC Medical Ethics. 2015; 16
Baghdadi ZD Preservation-based approaches to restore posterior teeth with amalgam, resin or a combination of materials. Am J Dent. 2002; 15:54-65
Ericson D, Kidd E, McComb D, Mjör I, Noack MJ Minimally invasive dentistry – concepts and techniques in cariology. Oral Health Prev Dent. 2003; 1:59-72
Kelleher M Ethical issues, dilemmas and controversies in ‘cosmetic’ or aesthetic dentistry. A personal opinion. Br Dent J. 2012; 212:365-367
Palcanis K How do I deal with what I perceive to be overtreatment by another dentist when his or her patients come to me to discuss their proposed treatment plans?. J Am Dent Assoc. 2011; 142:447-448
Friedman JW, Atchison KA The standard of care: an ethical responsibility of public health dentistry. J Public Health Dent. 1993; 53:165-169
Tomes JLondon: John Churchill; 1859
Black GVChicago: Medico-Dental Publishing Co; 1908
Handelman SL, Washburn F, Wopperer P Two-year report of sealant effect on bacteria in dental caries. J Am Dent Assoc. 1976; 93:967-970
Elderton RJ Assessment and clinical management of early caries in young adults: invasive versus non-invasive methods. Br Dent J. 1985; 158:440-444
Elderton RJ Management of early dental caries in fissures with fissure sealant. Br Dent J. 1985; 158:254-258
Schanschieff SG, Shovelton DS, Toulmin JKLondon: Department of Health and Social Security; 1986
Mount GJ Minimal treatment of the carious lesion. Int Dent J. 1991; 41:55-59
Horowitz AM Introduction to the symposium on minimal intervention techniques for caries. J Public Health Dent. 1996; 56:133-134
Bjørndal L, Larsen T Changes in the cultivable flora in deep carious lesions following a stepwise excavation procedure. Caries Res. 2000; 34:502-508
Diagnosis and management of dental caries throughout life. NIH Consensus Statement. 2001; 18:1-23
Ericson D, Bornstein R Development of a tissue preserving agent for caries removal. In: Albrektsson J Survey: Quintessence; 2001
Jenson L, Burdenz AW, Featherstone JD, Ramos-Gomez FJ, Spolsky VW, Young DA Clinical protocols for caries management by risk assessment. J Calif Dent Assoc. 2007; 35:714-723
Featherstone JD, Adair SM, Anderson MH Caries management by risk assessment: consensus statement, April 2002. J Calif Dent Assoc. 2003; 31:257-269
Featherstone JDB, Gansky SA, Hoover CI A randomized clinical trial of caries management by risk assessment. Caries Res. 2012; 46:118-129
The use of dental radiographs: update and recommendations. J Am Dent Assoc. 2006; 137:1304-1312
Banting D, Eggertsson H, Ekstrand KR Rationale and evidence for the international caries detection and assessment system (ICDAS II). Ann Arbor. 2005; 1001:48109-1078
Griffin SO, Oong E, Kohn W The effectiveness of sealants in managing caries lesions. J Dent Res. 2008; 87:169-174
Kutsch VK, Milicich G, Domb W, Anderson M, Zinman E How to integrate CAMBRA into private practice. J Calif Dent Assoc. 2007; 35:778-785
Mickenautsch S, Yengopal V Validity of sealant retention as surrogate for caries prevention – a systematic review. PLoS One. 2013; 8
Pitts NB, Ekstrand KR International Caries Detection and Assessment System (ICDAS) and its International Caries Classification and Management System (ICCMS) – methods for staging of the caries process and enabling dentists to manage caries. Community Dent Oral Epidemiol. 2013; 41:e41-52
Elderton RJ, Merrett MCW Variation among dentists in identifying reasons for marginal deterioration of restorations. J Dent Res. 1987; 66
Maupomé G A comparison of senior dental students and normative standards with regard to caries assessment and treatment decisions to restore occlusal surfaces of permanent teeth. J Prosthet Dent. 1998; 79:596-603
Baelum V What is an appropriate caries diagnosis?. Acta Odontol Scand. 2010; 68:65-79
Bratthall D Dental caries: intervened-interrupted-interpreted. Concluding remarks and cariography. Eur J Oral Sci. 1996; 104:(2)486-491
Bratthall D, Petersson GH, Stjernswärd JR Cariogram Internet version 2.01. 2003;
Guideline on caries-risk assessment and management for infants, children, and adolescents. Pediatr Dent. 2013; 35:e157-64
Reich E, Lussi A, Newbrun E Caries-risk assessment. Int Dent J. 1999; 49:15-26
Paul A Brunton Caries risk assessment and criteria for intervention. When should you intervene?.London: Quintessence Publ Co; 2002
Featherstone JD The caries balance: the basis for caries management by risk assessment. Oral Health Prev Dent. 2004; 2:259-264
Mickenautsch S, Yengopal V, Bonecker M Evidence base of caries management by risk assessment (CAMBRA)[poster]: grey literature. J Minim Interven Dent. 2013; 6:(2)
Pitts N ‘ICDAS’ – an international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate clinical management. Community Dent Health. 2004; 21:193-198
The ICDAS website. (Accessed 28 August, 2015)
Braga MM, Oliveira LB, Bonini GAVC, Bönecker M, Mendes FM Feasibility of the International Caries Detection and Assessment System (ICDAS-II) in epidemiological surveys and comparability with standard World Health Organization criteria. Caries Res. 2009; 43:245-249
Ismail AI, Sohn W, Tellez M The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol. 2007; 35:170-178
Nelson S, Eggertsson H, Powell B Dental examiners consistency in applying the ICDAS criteria for a caries prevention community trial. Community Dent Health. 2011; 28:238-242
Ericson D What is minimally invasive dentistry?. Oral Health Prev Dent. 2004; 2:287-292
Peters MC, McLean ME Minimally invasive operative care. I. Minimal intervention and concepts for minimally invasive cavity preparations. J Adhes Dent. 2001; 3:7-16
Banerjee A Minimal intervention dentistry: part 7. Minimally invasive operative caries management: rationale and techniques. Br Dent J. 2013; 214:107-111
Overtreatment in caries management? a literature review perspective and recommendations for clinicians Indrajeet Ghosh Prakriti Dayal Samiran Das Dental Update 2024 43:5, 707-709.
Authors
IndrajeetGhosh
MMedSci, BDS
Associate Specialist, Department of Dentistry, (drighosh@tatasteel.com)
Professor, Department of Prosthodontics, Guru Nanak Institute of Dental Science and Research, Nilgunj Road, Panihati, Kolkata, West Bengal-700110, India
Dentistry, like various branches in the healthcare profession, is susceptible to overtreatment, especially in the management of dental caries, due to the adoption of an aggressive restorative approach. This philosophy provides no actual benefits to the patient in terms of arresting the disease process, which initially led to the carious lesions. Yet practitioners routinely continue to initiate restorative treatment procedures without attempting to understand and alter the biologic factors contributing to the caries process. This paper examines the available scientific literature in this regard and makes recommendations to the clinicians of today based on the available evidence.
CPD/Clinical Relevance: The paper provides clinicians an approach to avoiding overtreatment by adhering to established clinical guidelines and accepted operative strategies.
Article
More than two decades have elapsed since academic stalwarts and caries researchers realized the need to apply a different treatment approach towards caries and cavitated lesions.1,2,3,4,5 Historically, tooth conservation by repeated restoration was favoured over extraction owing to the functional ability of the restored tooth.4 Dental schools favoured disciplines which mastered the art of improving upon existing restorative treatments, thus spawning what is termed as the ‘energetic restorative tiger’.4
Government-funded research in Western countries towards the latter part of the 20th century provided the insight into and the impetus for a better comprehension of the caries process. Recognizing that the cavitation of teeth via demineralization was only a symptom of the disease process and not the disease itself, researchers started focusing on the actual disease process and the steps that should be taken to arrest or reverse it.4,5 Beneficial to this new focus was the emergence of long-term clinical studies which suggested that the ‘repeat restoration cycle’ that dentists subjected their patients to actually shortened the life span of teeth.3,6,7,8,9,10 The research consensus was that the demineralization process in initial and incipient lesions can be arrested and possibly reversed without any restorative intervention by the patient's maintenance of excellent oral hygiene and change in lifestyle.9 Where it is necessary to restore frank cavitated lesions, a minimally invasive approach is suggested after a thorough caries risk assessment.7 Additionally, a stepwise excavation and sealing-in of caries is advocated.5,11,12,13
The term overtreatment can be used synonymously with ‘unnecessary treatment’ and involves making a patient go through a procedure when there is little or no evidence to support that the outcome of it will positively alter the health of the patient.14
Overtreatment in restorative dentistry occurs when a restoration-first policy or aggressive restoration attitude is adopted by the dentist.3 Such a philosophy does not usually allow the patient a full comprehension of the disease process and what can be achieved by his/her own attempts at arresting or reversing it. Instead, it propels the patient into a cycle of restoration and re-restoration. Overtreatment occurs also when defective restorations are replaced by invasive treatment modalities in lieu of minimally invasive restorative approaches including repair of restorations.15 Additionally, it is shown in the literature that clinicians tend to replace restorations particularly, and more often, if the work was not done by them.16 However, here it is important to note that dentists are ethically concerned about overtreating their patients.14,17,18,19
Reaffirmed Handelman’s observations - sealants applied even to occlusal caries extending into dentine can cause arrest of lesions by preventing exposure to nutrients in the oral cavity and even cause some remineralization
An example of minimal intervention techniques, Atraumatic Restorative Treatment (ART), endorsed by the World Health Organization, came into prominence in developing countries
Step-wise partial caries excavation process with calcium hydroxide placement revealed subsequently less cultivable microflora - demonstrating a change towards arrested lesions
14.
2001 NIH consensus development conference on the diagnosis and management of dental caries throughout life29
Detailed a systematic review of methods for the detection of dental caries and identified a shift toward improved diagnosis of non-cavitated, incipient lesions and treatment for the prevention and arrest of such lesions
Advocated a tissue-preserving approach for tooth restoration. Defined ‘Minimally invasive dentistry’ as maximal preservation of healthy dental structures.
Clinical protocols based on caries risk assessment, also included early detection and minimally invasive strategies that attempted to treat carious lesions differently depending on site (occlusal, approximal, or root); extent of the lesion (cavitated or not); and caries activity
Described pathologic risk and protective factors for caries development and progression. Realized that assigning risk assessment levels makes a difference in the effective management of patients with dental caries
18.
American Dental Association Council on Scientific Affairs (2006)35
Gave guidelines with 6 positive historical findings and 22 positive clinical signs or symptoms that may indicate the need for radiography
ICDAS II - provides a terminology to describe what is seen visually rather than dictate treatment protocol. Provides a caries detection criteria, caries activity criteria and a caries system
Evaluated evidence that suggested sealing both enamel caries and suspected occlusal dentinal caries was the most effective management approach if subsequent maintenance of the sealed surfaces could be assured
Show an emerging evidence base for CAMBRA in support for the viability of assessing the risk factors: saliva flow; salivary counts of S. mutans and lactobacilli; frequency of fermentable carbohydrate intake; past caries experience and advocated the use of preventive strategies like chewing gum; chlorhexidine; topical fluoride; glass ionomer restorations, to name a few
Partnership with ICDAS to determine objectively the management strategies based on lesion activity, surface integrity, etc, and taking into account caries risk factors. Applies principles of minimally invasive dentistry as solutions
Questionnaire based study showed that unnecessary treatments to patients seemed to be an ethically unacceptable conduct in the eyes of a sample of dentists in Switzerland
Discussion
Considerable variation exists between dentists on their treatment decisions regarding, among other things, the need for placing and replacing restorations.41,42 Lesion-activity and surface integrity of the concerned tooth should guide the treatment decision.43 Hence, the need arises for standardized models to ensure uniformity and objectivity in the approach to understanding the status of the caries process and managing it.
CARIOGRAM conceptualized in 1997 by Swedish and British caries researchers was initially used as an educational tool to depict the interplay of causal factors in determining caries risk.44 Well-documented validation of the concept is available in the scientific literature and, over time, it evolved into an Internet Version which can be used by clinicians to determine an overall-risk picture of caries for their patients.45 Risk-assessment being a key determinant of the strategy applied in caries management, the CARIOGRAM illustrates, in the form of a pie-circle diagram, whether the overall risk of an individual patient is high, intermediate or low. It also underlines those causes which make the individual at risk for caries and therefore allows the clinician to address them for caries managment. Additionally, the CARIOGRAM allows for factoring-in the clinician's judgement in the overall picture.
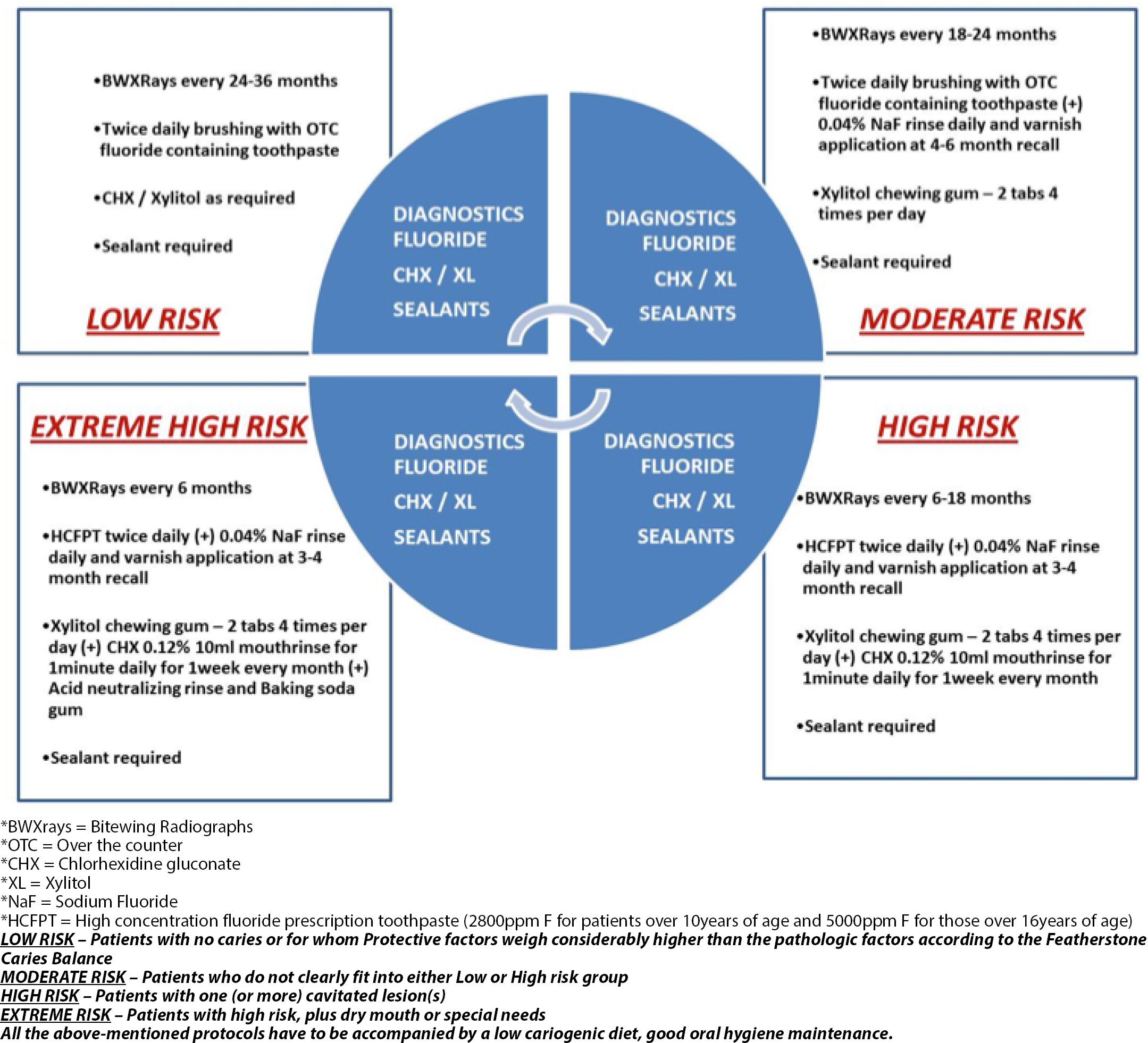
CAries Management By Risk Assessment (CAMBRA) first published in 2003 in the Journal of the Californian Dental Association, applies various factors (both biological as well as lifestyle factors) into a statistical model to reach a decision on the individual person's risk of caries in the future (Figure 1). Caries risk assessment is a method of determining the probability of caries incidence (that is, the number of new cavities or incipient lesions in a certain period) as well as the probability of a change in the size or activity of existing carious lesions, given that all other aetiological factors (diet, time, susceptible surface and plaque levels) remain the same.46,47,48 Determining risk status is an essential component for caries management because it enables the clinician to determine whether to restore or monitor lesions, while determining the recall period for monitoring the progression/reversal of the lesions.
Figure 1. The Caries management by risk assessment model (CAMBRA): illustrating the management protocols of patients falling in Low, Moderate, High or Extreme Risk groups. (Adapted from Jenson et al, 2007).31
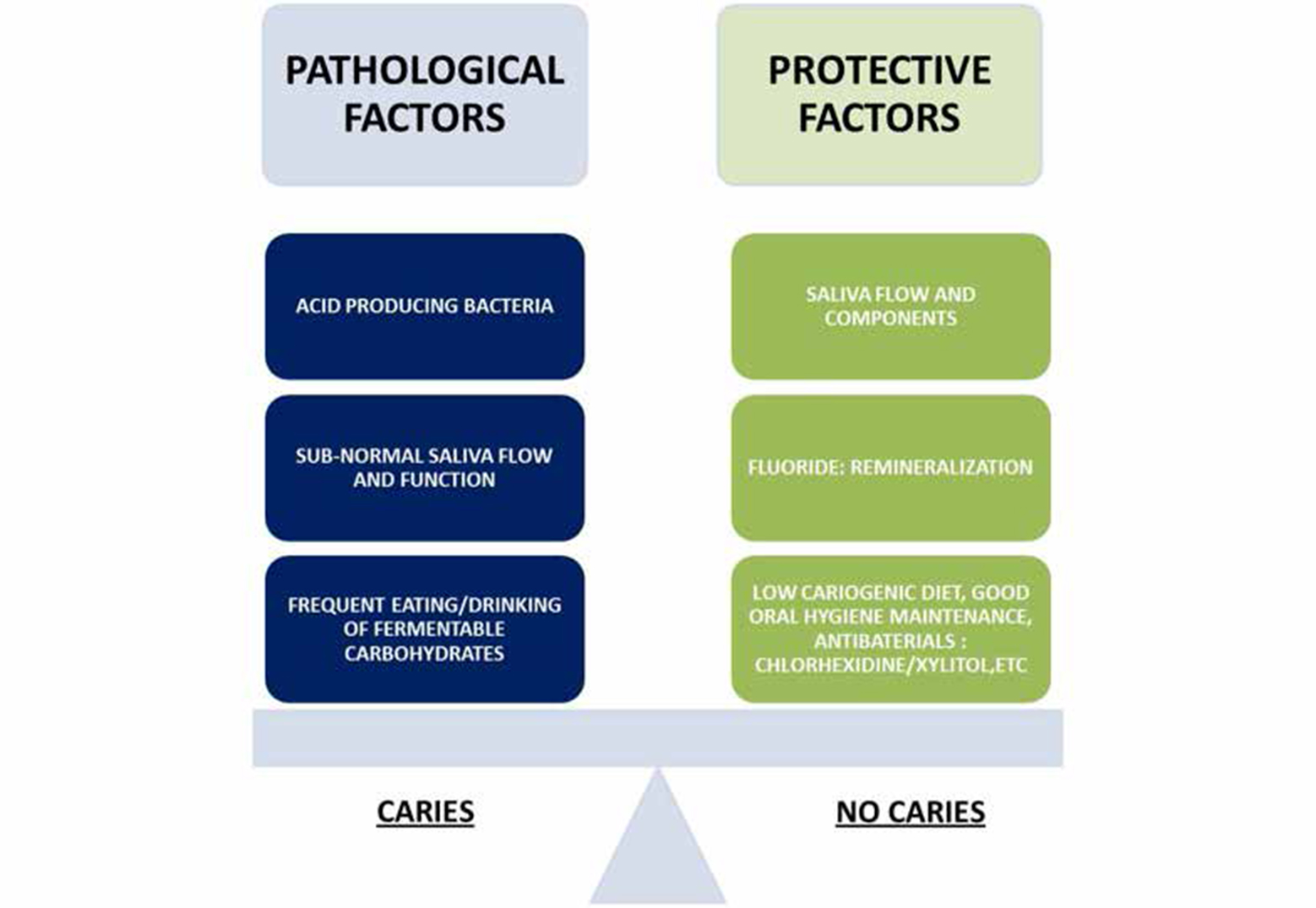
The protective factors need to be addressed in every patient, making them collectively weigh more heavily than the pathological factors (which in turn need to be mitigated) to tip the scale towards a ‘No Caries’ scenario (Figure 2). Achievement of this favourable balance forms the basis of the CAMBRA model.32,33,49 The evidence-base supports the CAMBRA model.38,50 Practitioners are however recommended to review their national guidelines on the usage of antibacterials like CHX/Xylitol before prescribing to patients. A sample treatment plan for a high caries risk patient has been proposed (Table 2).
Figure 2. Caries balance model (adapted from Featherstone49) defining the pathological and protective factors which can tip the scales towards a ‘caries’ or ‘no caries’ scenario.
Phase 0
Phase I
Phase II
Phase III
Phase IV
Comprehensive oral exam
Caries bacterial test Diet analysis
Bitewing radiographs
Adult prophylaxis
Oral hygiene instruction
Dietary advice
Prescribe chlorhexidine gluconate (0.12%) rinse to be used once daily at night for one week each month. Repeat monthly. Use separated by one hour from high concentration fluoride toothpaste
Prescribe HCFPT used twice daily in place of low concentration fluoride toothpaste
Fluoride varnish of all teeth
Complete endodontic therapy of LL6
Sealants for all posterior teeth
Hold on orthodontics and prosthetics till caries and periodontal processes are stabilized
Re-evaluate caries and periodontal status at 4-6 weeks from initial therapy/phase I
Periodic oral exam every six months
Caries bacterial test every six months to check for compliance and efficacy of the chlorhexidine rinse
Review compliance with chlorhexidine gluconate rinse and HCFPT and oral hygiene
Adult prophylaxis
Fluoride varnish of all teeth
From the guidelines provided by the CAMBRA model it is important to note that the assessment part and the non-surgical management of caries form the primary management strategy and the restorative intervention by the dentist in the form of sealants or composite restoration is the supplementary strategy and should be as per the ICDAS sealant protocol.
International Caries Detection and Assessment System (ICDAS) is an international standardized visual assessment tool developed in 2002 to grade an examined tooth's caries status numerically. Based on the coding that the tooth receives on visual examination, a management system International Caries Classification and Management System (ICCMS) to treat it is outlined. ICDAS II is currently being used widely by both clinicians and epidemiologists in standardizing their assessments in different settings and thereby formulating their management strategies accordingly51 (Table 3). The ICDAS employs two important elements which should be noted by clinicians, the first being that oral prophylaxis is necessary prior to visual examination of the tooth in question and second, the use of compressed air is essential to detecting early signs of caries.52
Code
Description
0
Sound
1
First Visual Change in Enamel (seen only after prolonged air drying or restricted to within the confines of a pit or fissure)
2
Distinct Visual Change in Enamel seen on a wet tooth surface
3
Localized Enamel Breakdown (without clinical visual signs of dentinal involvement)
4
Underlying Dark Shadow from Dentine
5
Distinct Cavity with Visible Dentine
6
Extensive Distinct Cavity with Visible Dentine
However, reservations exist about feasibility of applying the ICDAS codes in a dental practice setting for treatment decisions, and this is due to the exhaustive nature of the coding system (separate criteria for root caries, coronal caries, caries adjacent to restorations, radiographic scoring and clinical correlation, etc), although it's an effective tool for researchers and epidemiologists.53,54,55
For clinicians, a guide has been made with the categories/codes merged into 4 simple stage-based categories so that management decisions can be made easier. The management strategy takes into account also whether the lesion is Active/Inactive. The 4 merged categories have been listed in Table 4.
1. Sound
Code 0
2. Initial stage caries
Codes 1 and 2
3. Moderate stage caries
Codes 3 and 4
4. Extensive stage caries
Codes 5 and 6
The ICCMS advocates a spectrum of management strategies for coronal caries, ranging from ‘Risk-based Prevention’ for ‘sound teeth’ through to ‘NOC (No Operative Care)’ in the form of ‘Resin-based sealants for Initial Active lesions’ ending in ‘TPOC (Tooth-Preserving Operative Care)’ for ‘Extensive Active and Inactive lesions’.40
Minimally Invasive Dentistry (MID) involves the practice of minimally invasive operative caries management strategies and techniques based on a better understanding of the caries disease process. It addresses the causal factors responsible for caries rather than the symptomatic ones (cavitated lesions). It entails therefore only the minimum removal of healthy tooth structure operatively that would enable restoration of lost tissue, as well as promoting the arrest or reversal of the disease process that is caries.56 The availability of better adhesive restorative materials and newer preparation and caries removal techniques has helped in the emergence of the MID concept.
Chemo-mechanical excavation of carious dentine, air abrasion, enzymatic digestion, ozone treatment, antibacterial therapy (fluorides, chlorhexidine, etc) are all part of the MID conceptualized techniques. Numerous clinical studies have reported good patient acceptance and the evidence base supports these treatment techniques.57,58
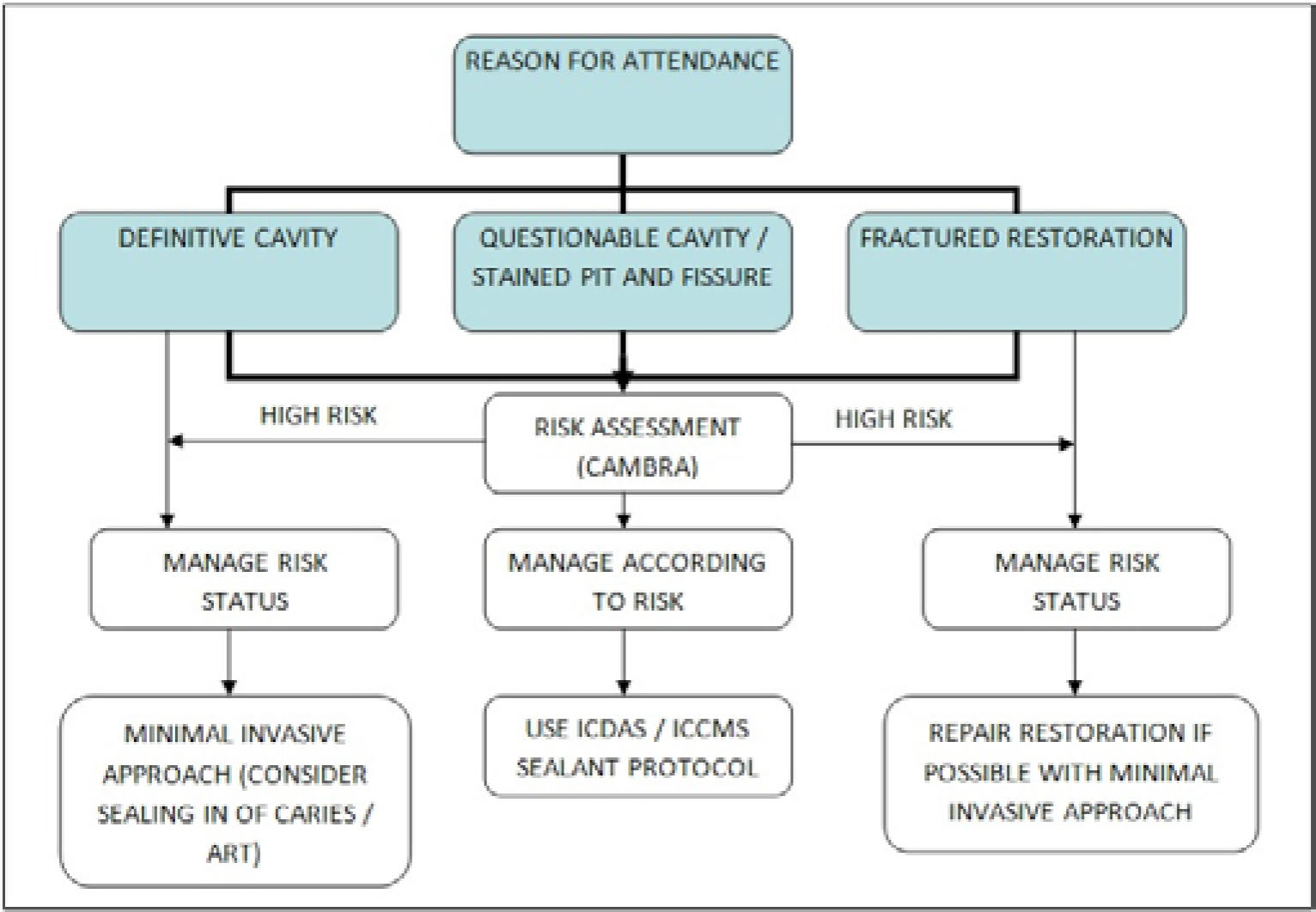
Minimally invasive restorative dentistry also advocates the sealing in of caries with a fissure sealant or composite restoration, and there is considerable evidence base to suggest that caries sealed in does not progress because the microbial flora is denied fermentable carbohydrates as a substrate (an essential requirement for caries progression). This procedure will be effective only if the tooth-restoration interface is truly sealed by the restorative material that is used. Although this school of thought is a paradigm shift from the traditional school of thought (as in GV Black's teachings), the evidence base supports such a caries management philosophy. In light of the available literature, a mechanistic approach to the management of dental caries is not suggested anymore.48 A decision algorithm has been made to assist the practitioner in making operative/non-operative decisions in managing initial carious lesions (Figure 3).
Figure 3. A decision algorithm for management of a patient with caries according to the clinical picture and risk status of the patient.
Conclusions
The following recommendations are based on the evidence from the scientific literature reviewed, including the authors' opinions towards taking caries disease management in the right direction.
Clinicians should assess caries risk status (CAMBRA, Cariogram risk models etc) in an individual patient before picking up the handpiece to place a restoration.
Initial lesions, particularly occlusal pit and fissure caries, are difficult to gauge with regards to depth of caries; and when in doubt, ICDAS guidelines could be used to decide the line of treatment and recall visit check-up criteria.
Initial lesions treated operatively, without adherence to an appropriate caries management protocol, may constitute overtreatment on the part of the clinician.
Wherever patients are encountered where restorative intervention is an absolute necessity, principles of minimally invasive dentistry should be applied to ensure overtreatment does not take place.
Repair rather than replacement of restorations should be a priority among clinicians and this conforms to the principles of MID.
Clinicians, at all costs, should avoid driving their patients through the re-restoration cycle as it has proved to be counter-productive to their overall goal of managing the caries disease process. Every effort has to be made to prolong the life-cycle of the concerned tooth.
Radiography in diagnosis of caries should be as per the approved guidelines and not routine. Bitewing radiographs are advised as per the caries risk assessed at intervals consistent with the guidelines given by the CAMBRA model.