Ruddle CJ Nonsurgical retreatment. J Endod. 2004; 30:(12)827-845
Peciuliene V, Rimkuviene J, Maneliene R, Pletkus R Factors influencing the removal of posts. Stomatologija. 2005; 7:(1)21-23
Abbott PV Incidence of root fractures and methods used for post removal. Int Endod J. 2002; 35:(1)63-67
Castrisos T, Abbott PV A survey of methods used for post removal in specialist endodontic practice. Int Endod J. 2002; 35:(2)172-180
Torabinejad M, Corr R, Handysides R, Shabahang S Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod. 2009; 35:(7)930-937
Naito T Surgical or nonsurgical treatment for teeth with existing root fillings?. Evid Based Dent. 2010; 11:(2)54-55
Tait CME, Ricketts DNJ, Higgins AJ Restoration of the root-filled tooth: pre-operative assessment. Br Dent J. 2005; 198:395-404
Ekuni D, Yamamoto T, Takeuchi N Retrospective study of teeth with a poor prognosis following non-surgical periodontal treatment. J Clin Periodontol. 2009; 36:(4)343-348
Pitt Ford TR, Rhodes JS Root canal retreatment: 1. Case assessment and treatment planning. Dent Update. 2004; 31:34-39
Ng YL, Mann V, Gulabivala K Outcome of secondary root canal treatment: a systematic review of the literature. Int Endod J. 2008; 41:(12)1026-1046
Roda RS, Gettleman BH Nonsurgical retreatment, 10th edn. St Louis, Mo: Elsevier Mosby; 2010
Gorni FG, Gagliani MM The outcome of endodontic retreatment: a 2-yr follow-up. J Endod. 2004; 30:(1)1-4
Ingle JI, Bakland LK, Baumgartner JC Retreatment of non-healing endodontic therapy and management of mishaps, 6th edn. USA2007
Garrido AD, Oliveira AG, Osório JE, Silva-Sousa YT, Sousa-Neto MD Evaluation of several protocols for the application of ultrasound during the removal of cast intraradicular posts cemented with zinc phosphate cement. Int Endod J. 2009; 42:(7)609-613
Chandler NP, Qualtrough AJ, Purton DG Comparison of two methods for the removal of root canal posts. Quintessence Int. 2003; 34:(7)534-536
Alfredo E, Garrido AD, Souza-Filho CB, Correr-Sobrinho L, Sousa-Neto MD In vitro evaluation of the effect of core diameter for removing radicular post with ultrasonic. J Oral Rehabil. 2004; 31:590-594
Soares JA, Brito-Júnior M, Fonseca DR Influence of luting agents on time required for cast post removal by ultrasound: an in vitro study. Appl Oral Sci. 2009; 17:(3)145-149
Smith BJ The removal of fractured post fragments in general dental practice using ultrasonic vibration. Dent Update. 2002; 29:(10)488-491
Rhodes JS Disassembly techniques to gain access to pulp chambers and root canals during non-surgical root canal re-treatment. Endod Topics. 2011; 19:22-32
Krell KV, Jordan RD, Madison S, Aquilino S Using ultrasonic scalers to remove fractured root posts. J Prosthet Dent. 1986; 55:46-49
Gomes APM, Kubo CH, Santos RAB, Santos DR, Padilha RQ The influence of ultrasound on the retention of cast posts cemented with different agents. Int Endod J. 2001; 34:93-99
Satterthwaite JD, Stokes AN Dentinal crack incidence following ultrasonic vibration to intra-radicular posts. N Z Dent J. 2004; 100:105-109
Dominici JT, Clark S, Scheez J, Eleazer PD Analysis of heat generation using ultrasonic vibration for post removal. J Endod. 2005; 31:301-303
Cherukara GP, Pollock GR, Wright PS Case report: removal of fractured endodontic posts with a sonic instrument. Eur J Prosthodont Rest Dent. 2002; 10:(1)23-26
Dixon EB, Kaczkowski PJ, Nicholls JI, Harrington GW Comparison of two ultrasonic instruments for post removal. J Endod. 2002; 28:111-115
Buoncristiani J, Seto BG, Caputo AA Evaluation of ultrasonic and sonic instruments for intraradicular post removal. J Endod. 1994; 20:(10)486-489
Carrotte P Endodontic problems. Br Dent J. 2005; 198:127-133
Dismantling restorations from teeth which require endodontic re-treatment can be difficult. Many dentists are reluctant to remove posts through fear of weakening, perforating or fracturing the remaining root structure. A variety of techniques have been described and developed for post removal. This is the first in a series of two papers which provide an overview of these techniques. The rationale for endodontic re-treatment, pre-operative assessment and factors affecting post removal are discussed. Techniques are illustrated with clinical case reports.
The second paper describes the use of specific post removal devices and the removal of fibre posts.
Clinical Relevance: Endodontic re-treatment has a more successful long-term outcome than surgical treatment for failed root canal treatment. This may involve the removal of existing post restorations or portions thereof.
Article
Jamie Dickie John McCrosson
Endodontic re-treatment can be complex and challenging. The goal is to access the pulp chamber, remove materials from the root canal space and, if present, address deficiencies or repair defects that are pathological or iatrogenic in origin.1 This may involve the removal of an existing post.
Many dentists are reluctant to attempt post removal through fear of weakening, perforating or fracturing the remaining root structure.2 As a result, a high number of patients are referred to specialist centres by general practitioners requesting removal or surgical treatment. However, the presence of a post should not be considered as an indication in itself for periapical surgery.3
Various techniques have been designed and developed for post removal. Dental practitioners should be reassured that, with good case selection, post removal is a predictable procedure. Root fractures rarely occur if appropriate techniques and devices are used.3,4
No single method always produces a successful result. In many cases, a combination of various techniques may be required. Therefore, familiarity with a variety of techniques may increase an individual clinician's chances of success.
Endodontic re-treatment vs apicectomy
A systematic review by Torabinejad et al found that endodontic surgery offers more favourable initial success, but non-surgical retreatment offers a more favourable long-term outcome.5 A study by Naito produced similar results.6
This appears to suggest that conservative endodontic re-treatment is the preferred choice compared with periapical surgery, as it is generally more successful and predictable.
Pre-operative assessment
Periodontal
Tait et al stressed that periodontal health is critical in determining the long-term success of teeth that have undergone root canal treatment and subsequent restoration.7 Since carrying out post removal and endodontic re-treatment is time consuming and costly, it could be counterproductive to embark on this approach when the overall oral condition gives a poor foundation for a successful restorative outcome. Teeth of poor prognosis include those with significant probing depths, mobility and furcation involvement.8
Additionally, some removal techniques require a degree of force to be applied and it would be ill-advisable to use these methods on teeth which are mobile as a result of periodontal disease.
Endodontic
When assessing teeth for endodontic re-treatment, there are several factors that need to be considered to determine the prognosis for successful endodontic re-treatment.9 These include:
Periapical radiolucency – Teeth with an apical lesion display have a lower success rate compared to those without;10
Size of radiolucency – Teeth with a lesion <5 mm in diameter have a greater success rate than those with a lesion >5 mm;10
Previous treatment factors – Poor access cavity design, untreated, poorly cleaned and obturated canals, instrumentation complications (eg ledges and separated instruments) and root fillings protruding through apices are known causes for previous failure.11 These issues would need to be overcome for a favourable outcome;
Perforations – The rate of success decreases if there is iatrogenic damage to the root canal anatomy;12
Pathological/microbiological factors – Radicular cysts and persistent intracanal and extracanal infection are potential causes of unsuccessful outcomes.11
Extract and replace?
Heroics should be avoided to retain teeth with a hopeless prognosis; however, there are clinical situations where extraction is not a preferred option either. In these situations, patients may wish to compromise by having treatment and retaining a tooth of a questionable long-term prognosis. They would need to be made aware of the prognosis and any contingency plan(s) prior to gaining consent for this approach.7
Batemen et al advocated that each case needs to be evaluated and selected appropriately, as extraction of the tooth followed by replacement with bridges or implants may provide a more predictable and favourable long term outcome. They suggested that such consideration be given to teeth with a history of previous anatomic breaches/problems, where the natural tooth has a poor prognosis and there are no issues with the costs of subsequent replacement teeth.13Figure 1 shows a post in an UL2 which has 50% horizontal bone loss and an UL1 with root surface calculus, indicating active periodontal disease. In order to avoid root fracture, a new post would need to be placed beyond the bone level, which in this case may be difficult. A reasonable alternative to post removal, endodontic re-treatment and the provision of a replacement post crown would be to extract and replace the UL2 with an adhesive cantilever bridge from the UL3 as this may give a more predictable outcome.
Figure 1. Radiograph of an intact post and core in UL2 with 50% horizontal bone loss.
The root and post
A well-angulated periapical radiograph should be used to investigate residual root morphology, length, width, curvature and thickness, as well as post location, length, width and angulation.14 It may also be possible to ascertain which type of post has been used, if previously unknown.
Clinical examination may reveal that the post is already loose due to marginal leakage, which can weaken the cement lute and facilitate removal. If this is the case, the presenting complaint can be that of a foul taste or halitosis.
The most common factors influencing post removal are summarized in Table 1.
Factor
Observations/Findings
Post Length
Posts of greater length can take longer to remove2,15
Decreasing the height and width of cast cores can facilitate removal16Materials:Composite cores around preformed posts can be more difficult to remove than amalgam cores3Cast gold cores - easier to reduce than cores made with non-precious metals3
Type of Lute
Posts cemented with zinc phosphate materials - easier to remove than those cemented with resin-based lutes15,17,18The type of lute cannot be determined without previous clinical notes15
Position of most coronal portion of post
Supracrestal – easier to remove19Subcrestal (i.e. fractured posts) – more difficult19
Wider, better adapted posts – difficult19Inappropriately adapted posts – less time to remove2
Accessing the post
A decision on the form of temporary restoration and its method of fabrication should be taken pre-operatively. The coronal restoration is then removed to expose the post.14,19 This paper does not focus on crown removal methods, but examples include the use of a high speed bur, an excavator, an ultrasonic device, the Safe Relax device (see below) or a sliding hammer, all of which may coincidentally remove the post.
Any encasing restorative material and cement around the post head is then removed.14,21 For preformed posts, any restorative material forming the core should be trimmed. With custom post and cores, the core should be separated from the root face by removing the core/cement interface with an ultrasonic scaler or long neck round bur, eg ISO size 006 (D205 LN bur, Dentsply Maillefer, Ballaigues, Switzerland), ISO size 100 or ISO size 120 (0197 LN bur, Komet, Rock Hill South Carolina) burs (Figure 2). If cutting with a bur is necessary, it should only be done on the core material in order to preserve tooth structure. Any encircling metal collars should also be removed to diminish the ‘ferrule effect’.22
Figure 2.
(a) LN round ISO size 120 bur; (b) LN round ISO size 100 bur.
Methods for removing posts
A summary of post types, their difficulty of removal and suggested removal method(s) is provided in Table 2.
*Removal devices include the Eggler, Universal Post Remover (UPR), Ruddle kit and Masserann collectively (see Part 2).
Ultrasonic scaler
Ultrasonic devices have been suggested to facilitate post removal for over 25 years.23 They are the most common method used to remove posts from all tooth types.4 The transfer of ultrasonic energy down the length of the post/cement/dentine interface promotes cement failure and loosens the post. It is particularly effective in cases where zinc phosphate and glass ionomer cements have been used,24,25 but has little influence on resin cements.23 Removal with an ultrasonic scaler requires less force than the majority of post removal devices17 and causes minimal loss of dentine.24 However, dentine cracks,4,25 significant heat generation26 and root perforation27 are all possible complications.
Piezo-electric ultrasonic scalers21,22,27 with large, flat, parallel-sided tips are the most effective.22 The tip should be applied, with water spray to the side of the post and the unit activated at full power.19 The tip should be guided circumferentially around the post and along any exposed length.28 For fractured posts, a 2 mm deep trough may be cut around the post fragment with a LN bur to allow the scaler tip to contact the side of the post.19,22 This trough needs to be kept as narrow as possible to retain tooth tissue.
Short, intense periods of vibration should be applied at different positions for no longer than 15 seconds1,26,28 to prevent excessive heat production. Check for any looseness at regular intervals. Posts generally loosen within 10–15 minutes of vibration.1 Smith suggested that it takes a maximum of one minute per millimetre of post.19 If the post remains firm, an alternative technique can be considered or used in conjunction with the ultrasonic scaler to produce a favourable result. Any alternative methods used for posts cemented with zinc phosphate and glass ionomer cements will likely require less force for removal owing to the previous ultrasonic instrumentation.24
Ultrasonic scalers can also unwind threaded active (screw) posts if they are guided around the post in an anticlockwise direction.20,22
Figures 3 and 4 show the removal of an intact custom post and a fractured post using an ultrasonic, respectively.
Figure 3.
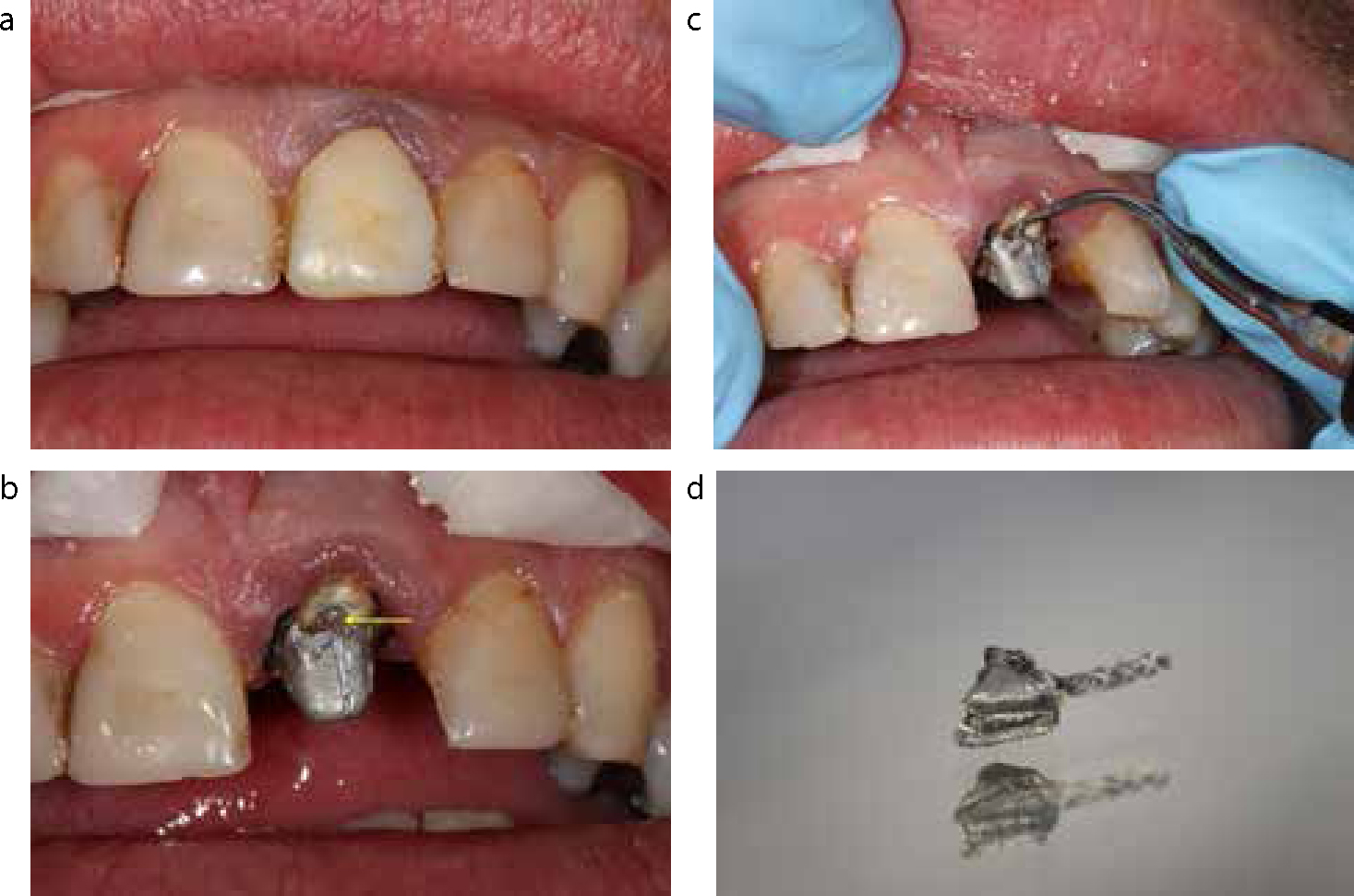
(a) A post-retained metal ceramic crown with poor marginal adaption on UL1. (b) The exposed core after removal of the coronal restoration. Note the existing separation between the core and at the labial root face. (c) A piezo-electric ultrasonic scaler being applied. (d) The removed post and core.Figure 4.
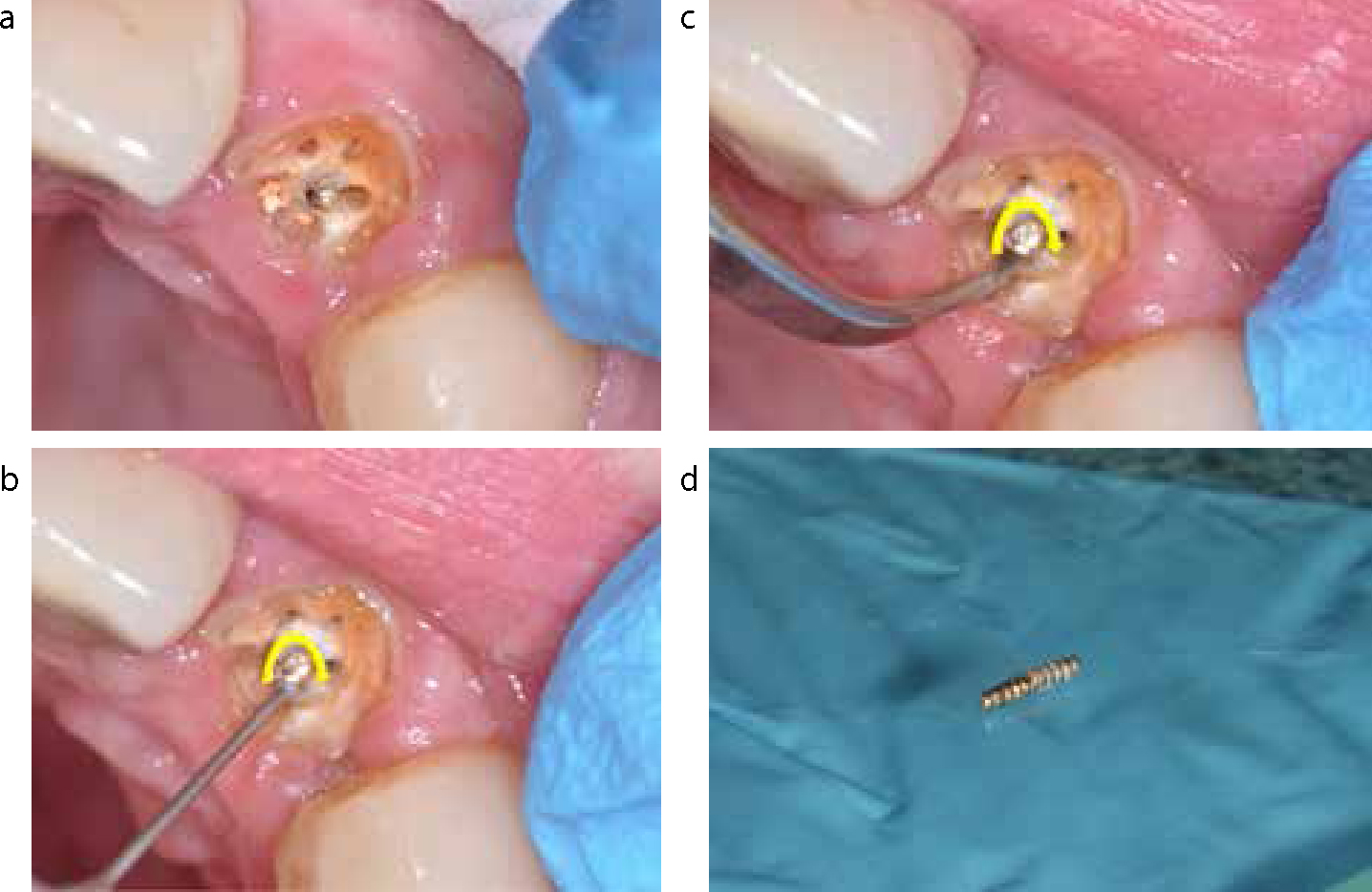
(a) A fractured post in UL2. Note the pin holes of a previous restoration and residual gut-ta-percha. (b) Use of a LN bur to create a 2 mm space around the post fragment. (c) A piezo-electric ultrasonic being circumferentially applied to the side of the post, as well as up and down the exposed length. (d) The removed post fragment.
Sonic scaler
Endodontic sonic instruments can also be used in a similar fashion to their ultrasonic counterparts since their elliptical pattern of oscillation can cause disruption of the cement lute.26 However, Buoncristiana et al concluded that sonic instruments were poor in terms of post removal when compared to ultrasonics,29 whereas Cherukara reported a case where two posts were removed successfully by this means.27
Unscrew
Threaded active posts, examples of which include Dentatus (Dentatus AB, Hagersten, Sweden) or Radix Anker (Dentsply, Weybridge, UK), can simply be ‘unscrewed’ anticlockwise using the corresponding tool supplied by the manufacturer for their placement. If the tool no longer fits due to post damage, cotton wool can be placed over the post to provide a better fit.20,22
Alternatively, fine forceps can be used for unscrewing (see below). If a groove (pre-existing or cut by a bur) is present coronally,30 a flat instrument (such as an enamel chisel or flat plastic) or small screwdriver can be inserted and turned anticlockwise to unthread the post (Figure 5).
Figure 5.
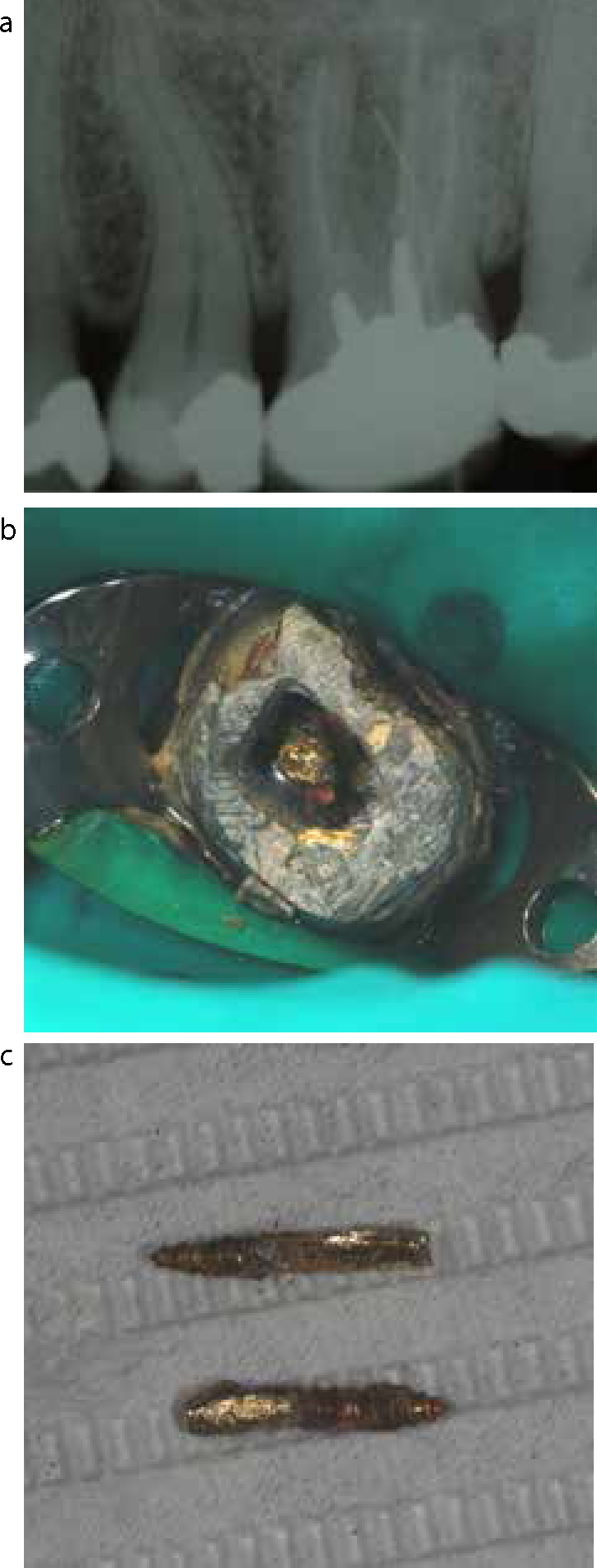
(a) Radiograph showing two active threaded (screw) posts in an UL6 with a peri-api-cal radiolucency tracked by a gutta-percha point. (b) The exposed posts. (c) The removed posts after unscrewing with an enamel chisel.
Care should be taken when removing active posts as they can become locked in the canal due to the flow of luting cement into the grooves present along the post shaft. Removal of such posts should never be forced.20,22
Safe Relax – Anthogyr
The Safe Relax system by Anthogyr (Sallanches, France) is an automated device primarily used to remove crown and bridgework. However, it can also be used for tapered and parallel non-active posts with their respective cores intact. It comprises a series of hooks and cables that can be used for various restorations. These attach to the system's handpiece device which is connected to the dental unit's air motor (Figure 6).
Figure 6. Safe Relax handpiece and hook inserts.
If a point of application does not exist prior to use, one can be established by separating the core from residual root face with an ultrasonic scaler or LN bur. One of the systems hooks is attached to the handpiece and its tip positioned at the point of application. Traction is applied by pulling the device in a coronal direction before pressing the motor pedal to initiate a series of ultra-fast micro-strokes in an axial direction to withdraw the post. These micro-strokes will not start unless the initial traction is applied. The device operates at a recommended speed range between 5,000 and 25,000 rpm and the intensity and frequency of the micro-strokes can be altered.31
This method can result in sudden removal of the post. Therefore, care should be taken to ensure that there is adequate patient airway protection to prevent aspiration. The sudden movement may increase the risk of root fracture, although no evidence of this has been published at present. Manual sliding hammers are also available; however, the authors' opinion is that this is a dangerous option and would not be recommended. Figures 7 (a–h) show a custom post being removed using the Safe Relax system.
Forceps
Stieglitz forceps19 (Claudius Ash, Potters Bar, Hertfordshire, UK) and other fine forceps (eg upper roots) (Figure 8) can be used to grip and unthread screw posts in an anticlockwise direction. Sufficiently loose parallel and tapered posts can also be removed if they are round/circular in shape. Small, gentle, alternating rotations should be used along with adequate finger support buccally/labially and palatally to help detect any tooth movement. If any resistance is met, the forceps should not be forced further and an alterative method of removal must be adopted. Excessive force could lead to root fracture, rupture of the periodontal ligament fibres or extraction of the tooth. Therefore, forceps should only be used if the post is already loose within the canal.
Figure 7.
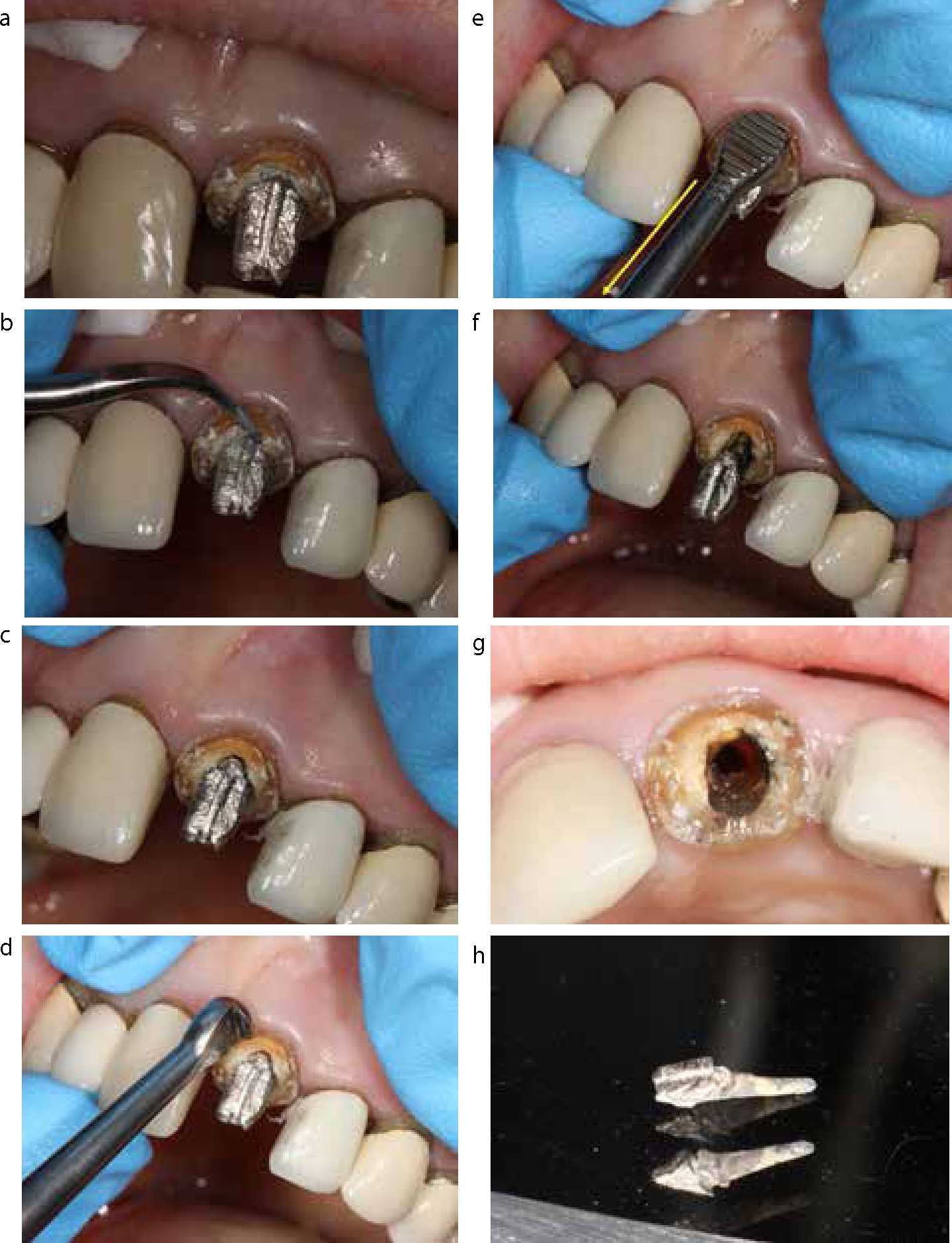
(a) A custom post and core in UL1 (after crown removal). (b) Ultrasonic separation of the core from root face. (c) The core now separated from root face. (d) Selection of the Safe Relax hook insert. (e) Application of the hook between core and root face, along with traction in a coronal direction (arrow). (f). The dislodged post after a series of automated micro-strokes. (g) The post space after removal. (h) The removed post and core.Figure 8.
(a) Upper fine root forceps; (b) Stieglitz forceps.
Burs
LN burs can be used to aid with the removal of short posts (5 mm or less) of thin diameter. High speed burs should never be used.22 The bur should be worked around the post circumference (keeping it as close to the post as possible) to destroy the cement lute interface or the post itself completely. This can lead to widening of the root canal/post space and the authors would advocate that this approach should not be considered unless all other options have been exhausted.
If a tungsten carbide bur is applied to fragments of 2 mm (or less), it can occasionally bind to the post. As a result, withdrawal of the bur from the root canal also removes the post fragment. This outcome obviously damages and sacrifices the bur.
Summary
This paper has highlighted different techniques that may be appropriate in different situations and that all techniques may be difficult to execute. It gives the reader some insight into which technique may work effectively, depending on the clinical circumstances.
The use of conservative methods before more destructive methods is recommended (ie those which cause greater dentine loss or increase the risk of root fracture).
Ultrasonic devices are very beneficial when it comes to post removal procedures as they are the least destructive method of removal and can also facilitate the use of other techniques/devices.
The next paper in this series covers the use of devices specifically designed for retrieving posts as well as the removal of fibre posts.