Gunraj M. Dental root resorption. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 88:647-653
Tronstad L. Root resorption – etiology, terminology and clinical manifestations. Endod Dent Traumatol. 1985; 1:221-227
Heithersay G. Clinical endodontic and surgical management of tooth associated bone resorption. Int Endod J. 1985; 18:72-92
Gulabivala K, Searson L. Clinical diagnosis of internal resorption: an exception to the rule. Int Endod J. 1995; 28:255-260
White S, Pharoah M., 5th edn. St Louis, Mo: Mosby; 2004
Andreason JO. External root resorption: its implication in dental traumatology, paedodontics, periodontics, orthodontics and endodontics. Int Endod J. 1985; 18:109-118
Bakland L. Root resorption. Dent Clin N Am. 1992; 36:491-525
Frank A, Torabinejad M. Diagnosis and treatment of external invasive resorption. J Endod. 1998; 94:500-504
Fuzz Z, Tsesis I, Lin S. Root resorption – diagnosis, classification and treatment choices based on stimulation factors. Dent Traumatol. 2003; 19:175-182
Heithersay G. Management of tooth resorption. Aust Dent J. 2007; 52:S105-S121
Root resorption is a pathological process that may occur after surgical, mechanical, chemical or thermal insult. Generally, it can be classified as internal and external root resorption. Depending on the diagnosis, an orthograde, surgical or a combined approach is used in management of these cases.
Clinical Relevance: General dental practitioners can face difficulties in diagnosis and treatment planning for cases with root resorption. An understanding of the aetiology and pathogenesis of root resorption is critical for diagnosis, effective management and improves outcome.
Article
Root resorption is a pathological process that is not uncommon after injuries or irritation of periodontal ligament or pulp.1 Such injuries may result from surgical, physical, chemical or thermal insult. Resorption may also occur due to mechanical stimulation, infection or neoplastic disease.
Pathogenesis
The result of this process is loss of hard dental tissues (ie cementum and dentine) by dentinoclastic cell action. The function of dentinoclasts is controlled by various activating and preventing resorption factors. Activating factors include:
Osteoclast activating factor;
Macrophage chemotactic factor;
Prostaglandins, heparin and bacterial products.
Preventive factors acting on dentinoclasts include: anti-invasion factor and the intermediate cementum layer.2 Injuries and irritations may stimulate activating factors or reduce preventive factors, hence dentinoclasts may become activated and subsequent root resorption may occur.
Root resorption continues as long as the simulating factor is present. The stimulating factor could be mechanical stimulation, pressure, infection, neoplastic process or a combination of any of these factors.3,4 Once the stimulating factors are removed, root resorption may be arrested. Cementum and dentine may form again, depending on the severity of the damaged surface area.
Classification
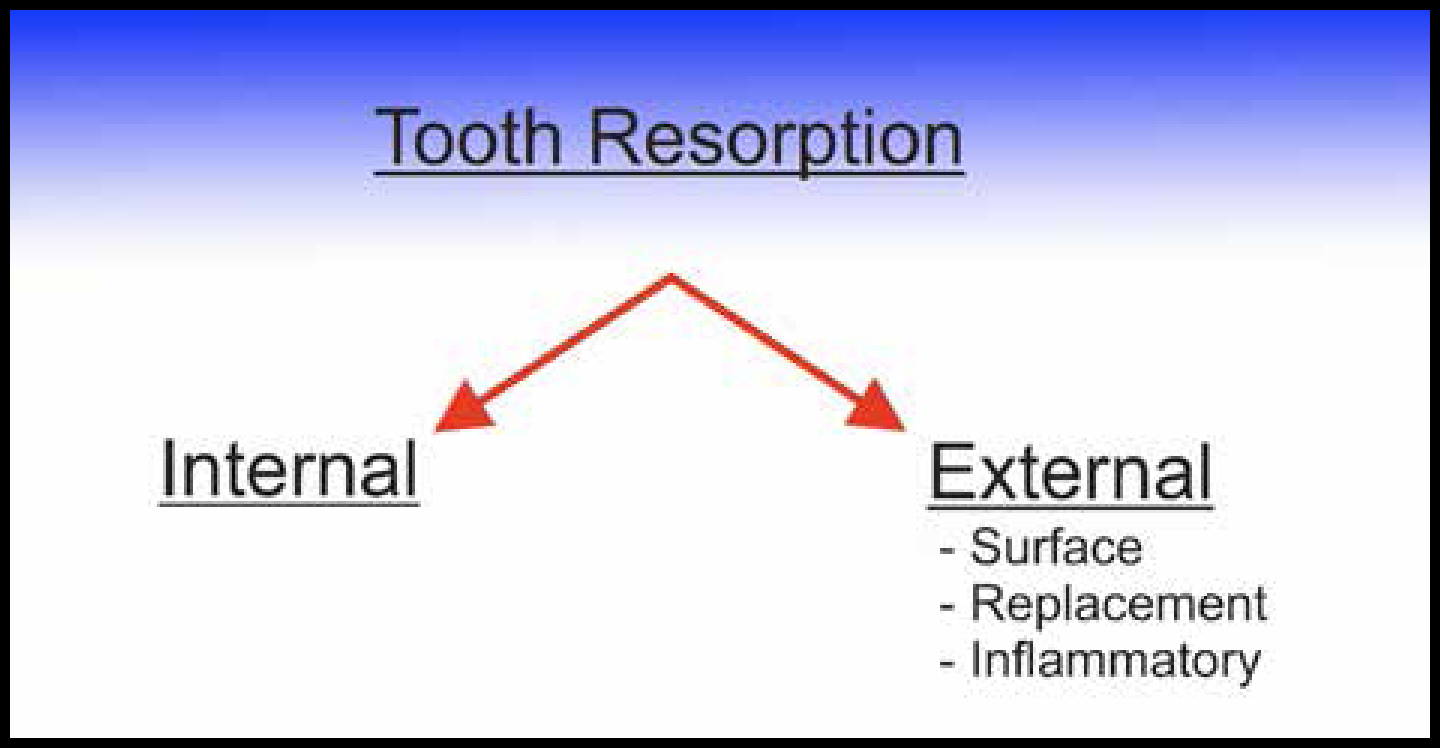
Classification of root resorption has an important role in the process of diagnosis and treatment planning (Figure 1).
Figure 1. Classification of root resorption.
In addition to classifying the type of resorption, the following issues need to be addressed to reach a treatment plan:
Will the resorptive process be self limiting or does it require further intervention?;
If the resorptive process is progressive (as observed from assessment over time), what treatment options can we provide?;
If treated, what are the short- and long-term prognoses?;
When is extraction and prosthetic therapy indicated?
The following section will discuss the signs and symptoms, clinical and radiographic presentations of each type of root resorption. This will be followed by clinical examples on the management of root resorption.
Internal resorption
The process of internal resorption occurs in chronic pulpal inflammation and less commonly after dental trauma or due to dystrophic idiopathic changes.5 In this process the pulp tissues coronal to the lesion become necrotic. In order for the internal resorption to progress, both dentinoclast-activating factors and the cells viable to keep the resorptive process going must be present. Hence, teeth that are actively continuing to resorb internally must be connected to the blood supply of the apical vital tissues.
Signs and symptoms
In most cases of internal root resorption the tooth is asymptomatic, however, a history of pulpal symptoms may be a feature as the pulp is involved first. If the pulp succumbs completely and periradicular tissues become inflamed, symptoms of periapical periodontitis may be evident.5
Clinical presentation
Clinically, if the internal resorption is in the cervical/coronal part of the tooth, it may present as a pinkish hue because of the prolific capillaries in the pulpal inflammatory tissue resorbing the coronal dentine and enamel.6 If internal resorption is in the mid/apical third of the root, it is for the most part clinically silent and would normally be diagnosed radiographically.7
Radiographic features
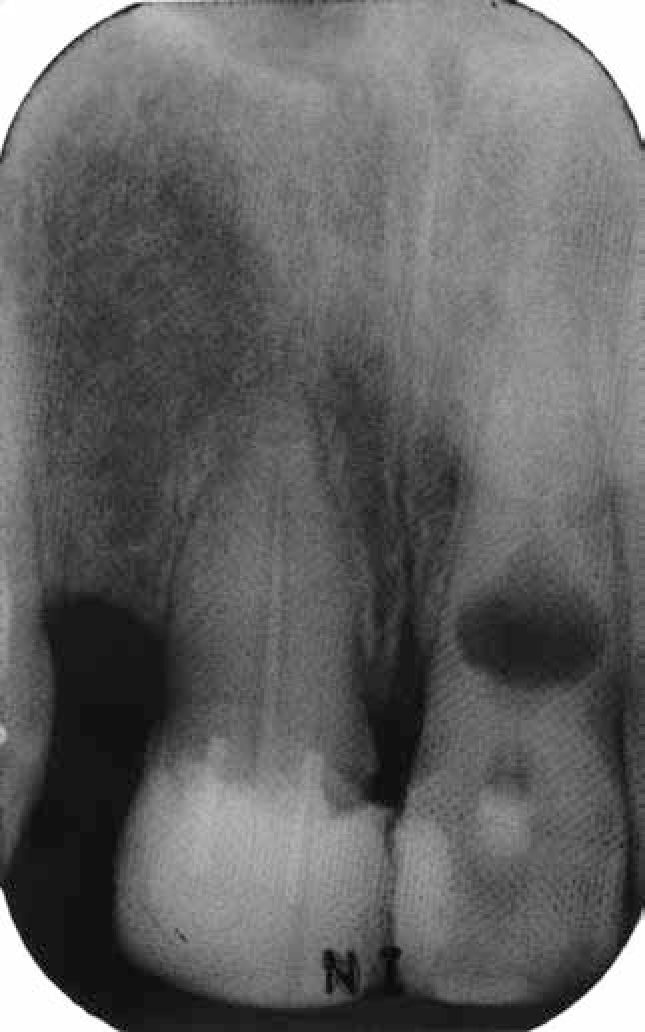
Radiographs reveal the lesions as radiolucent, round, oval or elongated within the root or crown and continuous with the image of the pulp chamber or canal. The outline is usually sharply defined and smooth or slightly scalloped as a result of an irregular widening of the canal of the pulp8 (Figure 2).
Figure 2. Internal resorption on UL1.
External resorption
External inflammatory resorption
External inflammatory resorption usually occurs when infection is superimposed on a traumatic injury, however, it can also be induced in some cases of endodontic pathosis. Damage of the cementum layer will initiate this resorption, exposing the underlying dentine to the passage of bacteria or their metabolites to the external root surface. This activates the dentinoclast cells which results in resorption of both tooth and bone.
Signs and symptoms
Teeth could be asymptomatic or have signs of irreversible pulpitis or necrotic pulp.9
Clinical features
Clinical findings may include tooth discoloration, tenderness to percussion, tooth mobility or periodontal defects. Careful evaluation of the periodontal condition is recommended because inflammatory resorption can be sustained by bacterial infection involving gingival tissues.10
Radiographic features
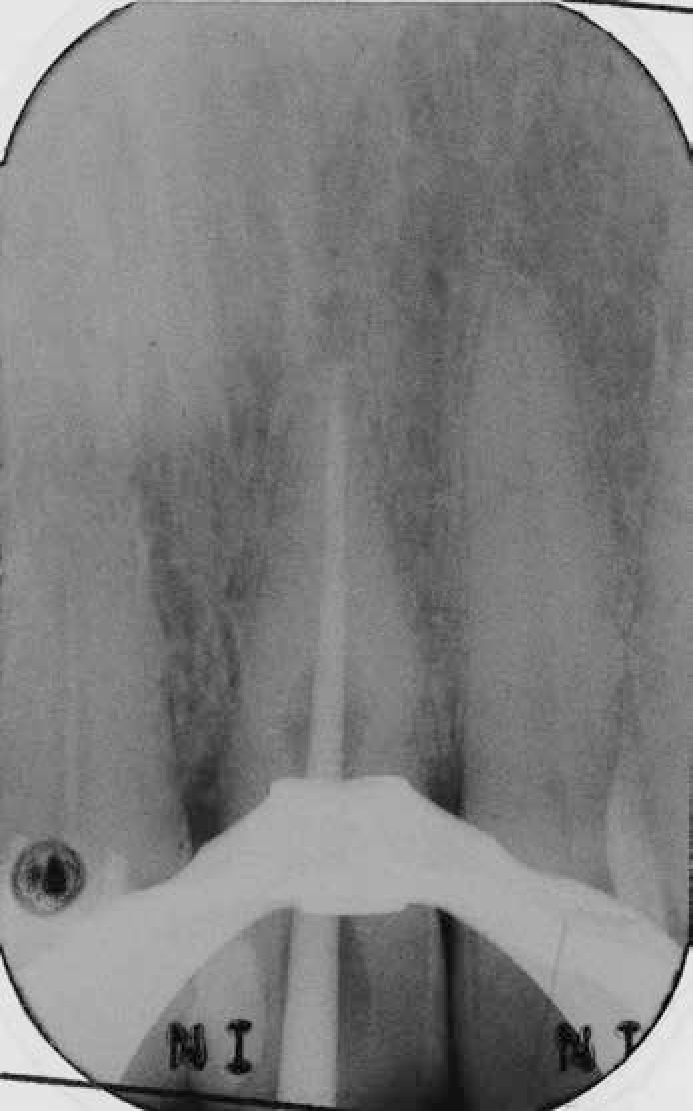
Radiographically, this type of resorption appears as an irregular area of resorption involving loss of both tooth structure and adjacent alveolar bone (Figure 3). The irregular area may appear superimposed over the root canal and could be misdiagnosed as internal resorption. The main radiographic feature to differentiate between these two entities is that the outline and the integrity of the canal space remain uninterrupted in external resorption.11
Figure 3. External cervical root resorption: irregular area of resorption involving loss of tooth structure on UL2.
External surface resorption
External surface resorption is a shallow resorption of cementum, often with involvement of a small amount of underlying dentine. This type of resorption is self limiting and transient and can follow some traumatic injuries or orthodontic treatment. In the absence of superimposed infection surface, resorption heals by forming reparative cementum.
Signs and symptoms
Teeth are asymptomatic and the pulp is usually vital. The tooth in question is frequently firm and immobile but not ankylosed in the dental arch.12
Radiographic features
The apical and cervical regions are common sites for this type of resorption. When the lesion begins at the apex, it generally causes smooth resorption of the tooth structure, resulting in blunting of the root apex. The bone and the lamina dura follow the resorbing root and present with a normal appearance around the shortened root.8
External replacement resorption
External replacement resorption follows the death of viable periodontal ligament cells due to factors such as compression or drying of the ligament cells in the case of delayed re-implantation of an avulsed tooth.13 This process involves the progressive replacement of tooth structure by alveolar bone and may (in severe cases) lead ultimately to tooth loss. External replacement resorption is commonly seen during and after orthodontic treatment. An incidence of 1.5% of external replacement resorption has been reported for the maxillary central incisors and 2.2% for lateral incisors.14
What has an effect on the progression of external root resorption to either external surface resorption or external replacement resorption is the severity of injury and the amount of damaged surface. If the injury is minimal and the damaged surface does not cover a large surface area, the tissues will heal by forming reparative cementum and external surface resorption will occur. On the other hand, if the injury is severe and the damaged area is large, bone cells will be able to attach to the root surface before the cementum-producing cells; external replacement resorption and ankylosis are the result of this process.12
Signs and symptoms
Initially, teeth may appear healthy but, as the tooth loses its vitality, signs and symptoms of necrotic pulp will be noted.
Clinical features
Clinically, teeth suffering from replacement resorption have metallic sound upon percussion and lack of mobility; these are signs of ankylosis. In addition, they may have other clinical problems, such as infra occlusion, incomplete alveolar process development (if the patient was young when the trauma occurred), and prevention of normal mesial drift.10
Radiographic features
Radiographically, replacement resorption appears as total loss of periodontal ligament space followed by evidence of the progressive replacement of tooth structure by bone and, in time, radiographically the outline of the tooth root is lost (Figure 4).13
Figure 4. External replacement resorption: loss of tooth structure followed by the progressive replacement of tooth structure by bone.
Tables 1 and 2 summarize the aetiological factors and key features of root resorption, respectively.
External resorption
Replantation of teeth
Orthodontic forces
Eruption of adjacent teeth
Root fracture
Trauma
Necrotic pulp
Root planing
Pathology
Cysts
Ameloblastoma
Giant cell tumours
Fibro-osseous lesions
Heredity
Bleaching
Surgery
Dento-alveolar
Orthognathic
Mandibulectomy/Maxillectomy
Internal resorption
Chronic pulp inflammation
Trauma
Pulpotomy
Restorative procedures
Cracked tooth
Invaginated cingulum
Orthodontic tooth movement
Resorption Type
Clinical Features
Clinical Findings
Location on Root
Pulp Sensitivity (Thermal or Electric)
Radiographic Features
Root Canal
Internal resorption
Pink spot on crown in cervical 1/3.Mostly has no clinical symptoms in mid/apical 1/3
May have tenderness over apex
Anywhere
May be positive
Symmetrical oval-shaped enlargement of root canal
Canals expand into lesions
External inflammatory resorption
Tooth discoloration, tenderness to percussion, tooth mobility and periodontal defects
No symptoms, or signs of irreversible pulpitis or necrotic pulp
Anywhere
Negative
Irregular radiolucent lesion of root and adjacent bone
Intact
External surface resorption
Healthy
None
Usually apical as a result of trauma or orthodontic treatment
Positive
Smooth resorption resulting in blunting of root apex and shortened root
Intact
External replacement resorption
Metallic sound on percussion, lack of mobility
No symptoms, initially signs of necrotic pulp as tooth loses vitality
Anywhere
May be positive
Asymmetrical replacement of root structure with bone. Loss of periodontal ligament space
Intact
Treatment
Once a diagnosis has been reached there is a need to assess:
If endodontic intervention (orthograde/surgical) will stabilize the root resorption or not; and
If the remaining tooth structure is restorable.
The exact treatment plan required is specific to each case, depending on patient factors, clinical and radiographic findings.
If the tooth is deemed to be unrestorable, the tooth has to be extracted and the treatment plan should be focused on replacing the tooth with an appropriate fixed/removable prosthesis. However, if the tooth is restorable, endodontic intervention with either orthograde or surgical endodontics, or both, may be feasible to preserve the tooth.
The aim of orthograde root canal treatment is to stabilize the root resorption process and to achieve hermetic seal. Alteration in the anatomy of root canal systems due to root resorption may make this more challenging to achieve.
If root resorption has resulted in an open apex, then it may be necessary to create an apical barrier prior to the obturation stage. Mineral Trioxide Aggregate (MTA) can be placed from an orthograde approach (Case 1) to create this apical barrier.
MTA is considered to be an ideal material for use against bone, because it is the only material that is reported to allow apposition of cementum and the formation of bone consistently, and it may facilitate the regeneration of the periodontal ligament. In addition, MTA has an antimicrobial effect, is highly biocompatible and possesses good sealing properties.15 These properties also mean that MTA is ideal for surgical repair of external resorption which is not supragingival. MTA cannot be used supragingivally as its slow set (4–24 hours) means that it may be washed away by saliva. For repairs that are partly supragingival, a material such as composite or glass-ionomer is required.
The use of gutta-percha (GP) cones and thermoplastic GP is generally the method of choice to achieve complete obturation of the canals. Thermoplastic GP is particularly useful to treat irregular canal anatomy such as that seen in internal root resorption.
If the tooth suffers from external root resorption, a surgical approach may be considered in the management of these cases. In these cases, a muco-periosteal flap could be raised to identify the resorbed area. This may be followed by curettage and repair of the root surface area with appropriate sealing material. Prior to attempting any surgical repair, it is essential to locate the position of the resorption (buccal/lingual) and assess whether its size is likely to be amenable to repair. The location of root resorption could be located with the use of parallax technique, when obtaining radiographs, or with the use of Cone Beam Computerized Tomography (CBCT).
In cases of complex external and internal root resorption, both of the previously mentioned techniques could be used in an attempt to arrest root resorption process. However, these cases should be appropriately selected and should be carried out by experienced clinicians.
The following section will explain cases in which orthograde, surgical and combined (orthograde and surgical) techniques were used in the management of root resorption.
Cases 1 and 2: orthograde technique
Case 1
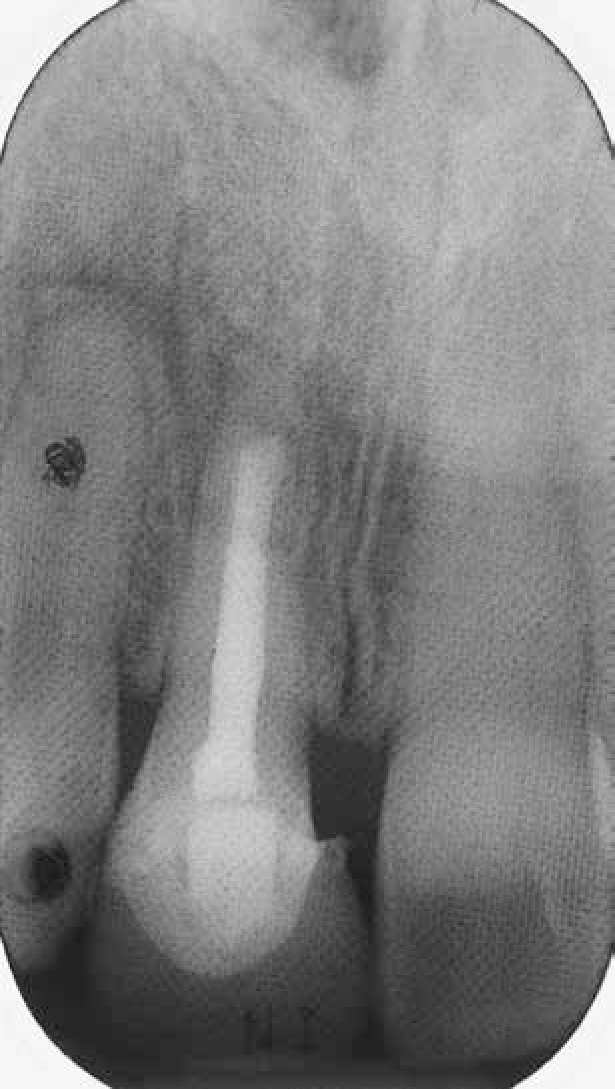
A 24-year-old lady had her LR5 transplanted to replace the UR1 when she was 11 years of age. She was referred to the restorative department regarding the unsatisfactory appearance of the crown on the UR1 due to gingival recession. This was improved by adding a small amount of composite filling cervically. Figure 5 shows the initially transplanted LR5 in the position of the UR1. The LR5 was extirpated and a radiograph was obtained with a file in situ showing that the root resorption originates from the mesial aspect of the apical third of the root (Figure 6). After root canal preparation, an MTA plug was placed at the level where the external root resorption is communicating with the root canal to achieve appropriate apical seal (Figure 7). The remainder of root canal space was filled with thermoplastized gutta-percha (Obtura II, Spartan, US). After 18 months of carrying out the treatment, the patient was still symptom-free. Clinically, the tissues were healthy and no tenderness was noted. Radiographic examination revealed full bony infill and apical healing with the root-treated tooth (Figure 8).
Figure 5. Initial transplanted LR5.Figure 6. External root resorption is on the mesial aspect of apical third of the root.Figure 7. The MTA plug on the level of external root resorption.Figure 8. Radiograph 18 months post-operatively.
Case 2
A 66-year-old patient was referred from his GDP regarding persistent infection related to his UL1. Upon clinical examination, the UL1 was not tender to percussion. No mobility or pocketing was noted. Radiographic examination revealed a well-defined, round-oval radiolucency on the cervical and mid apical third (Figure 2). The diagnosis was internal resorption. The treatment of choice in this case was an orthograde approach by chemo-mechanical debridement of the canal using conventional hand instruments and filling the apical two-thirds with GP (Figure 9), as opposed to MTA in the previous case, and to backfill the remainder of the canal with thermoplastized gutta-percha (Obtura II, Spartan, US). The patient was reviewed 6 months later, and there were no signs of infection, clinically or radiographically (Figure 10).
Figure 9. Radiograph with master cone to fill apical two-thirds with GP.Figure 10. Radiograph 6 months post-operatively.
Case 3: surgical technique
An 18-year-old patient was seen in the restorative department regarding the pink appearance of the UL2. The patient reported a history of extensive orthodontic treatment. On clinical examination, the UL2 had external cervical resorption, along with gingival overgrowth covering part of the lesion (Figure 11). The sensibility tests for the UL2 were positive. The treatment of choice in this case was to use the surgical approach to gain access to the cervical root resorption and to repair with composite. A mucoperiosteal flap with a distal vertical releasing incision was raised to expose the lesion (Figure 12). The cervical root resorption was restored with composite (Figure 13), the flap was repositioned and the gingival margin was contoured with inverse bevel gingivectomy (Figure 14). The patient was reviewed and the site of surgery healed well. Composite was used in this case as the restoration was partly supragingival.
Figure 11. Ginigival margin overgrowth covering the cervical root resorption on UL2.Figure 12. A mucoperiosteal flap raised from UL1–3.Figure 13. Cervical root resorption was restored with composite.Figure 14. Flap repositioned and the gingival margin contoured.
Case 4: surgical and orthograde approach
A 44-year-old patient was referred regarding persistent infection related to UL2. Clinical examination revealed a cavity which was probed on the labial aspect of the tooth (Figure 15). Radiographic examination revealed an appearance of external cervical root resorption and a short single point root filling (Figure 3). In this case, the plan was to replace the root canal treatment, this to be followed up by a surgical procedure to restore the resorption area.
Figure 15. Pre-operative clinical view of external cervical root resorption on UL2.
After the root canal retreatment, a mucoperiosteal flap was raised to identify the extent of the resorbed area (Figure 16). The enamel and dentine were minimally prepared (Figure 17). The cavity was restored with composite (Figure 18) and the flap repositioned. On a 1-year review, the patient was still asymptomatic and the gingivae had healed well (Figure 19). Radiographically, the repaired area was sound and the periapical area had healed well (Figure 20). As the periodontal ligament does not re-attach to composite, there is a periodontal pocket in the region of the repair. That is in contrast to MTA, to which soft tissues may attach.
Figure 16. A mucoperiosteal flap raised to identify the extent of resorbed area on UL2.Figure 17. The enamel and dentine on UL2 was minimally prepared.Figure 18. The resorbed area on UL2 was restored with composite.Figure 19. One year post-operative clinical view of UL2.Figure 20. One year post-operative radiographic view for UL2.
Discussion
The basis of this paper is to provide clinicians with an overview on root resorption with a view to increasing their understanding of this topic and to assist them in reaching a diagnosis. In addition, it explains methods of root resorption management. Decisions on management are made on a case by case basis. Orthograde endodontics, surgical endodontics and, on occasion, a combination of the two may be able to stop further resorption successfully and preserve the affected tooth.