Glantz PO, Nilner K Root canal posts – some prosthodontic aspects. Endod Dent Traumatol. 1986; 2:(6)231-236
Guzy GE, Nicholls JI. In vitro comparison of intact endodontically treated teeth with and without endo-post reinforcement. J Prosthet Dent. 1979; 42:(1)39-44
Sorensen JA, Martinoff JT. Clinically significant factors in dowel design. J Prosthet Dent. 1984; 52:(1)28-35
Stokes AN. Post crowns: a review. Int Endod J. 1987; 20:(1)1-7
Trope M, Maltz DO, Tronstad L. Resistance to fracture of restored endodontically treated teeth. Endod Dent Traumatol. 1985; 1:(3)108-111
Nayyar A, Walton RE, Leonard LA. An amalgam coronal-radicular dowel and core technique for endodontically treated posterior teeth. J Prosthet Dent. 1980; 43:(5)511-515
Ross RS, Nicholls JI, Harrington GW. A comparison of strains generated during placement of five endodontic posts. J Endod. 1991; 17:(9)450-456
Luu KQ, Walker RT. Corrosion of a nonprecious metal post: a case report. Quintessence Int. 1992; 23:(6)389-392
Ferrari M, Vichi A, García-Godoy F. Clinical evaluation of fiber-reinforced epoxy resin posts and cast post and cores. Am J Dent. 2000; 13:(2 spec iss)15B-18B
Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JY. Clinical complications in fixed prosthodontics. J Prosthet Dent. 2003; 90:(1)31-41
Creugers NH, Mentink AG, Kayser AF. An analysis of durability data on post and core restorations. J Dent. 1993; 21:(5)281-284
Weine FS, Wax AH, Wenckus CS. Retrospective study of tapered, smooth post systems in place for 10 years or more. J Endod. 1991; 17:(6)293-297
Vire DE. Failure of endodontically treated teeth: classification and evaluation. J Endod. 1991; 17:(7)338-342
Cohen BI, Pagnillo M, Condos S, Musikant BL, Deutsch AS. Post removal using a thick-walled hollow tube post design. Oral Health. 1994; 84:(11)15-22
Deutsch AS, Cavallari J, Musikant BL, Silverstein L, Lepley J, Petroni G. Root fracture and the design of prefabricated posts. J Prosthet Dent. 1985; 53:(5)637-640
Deutsch AS, Musikant BL, Cavallari J, Silverstein L, Lepley J, Ohlen K Root fracture during insertion of prefabricated posts related to root size. J Prosthet Dent. 1985; 53:(6)786-789
Greenfeld RS, Roydhouse RH, Marshall FJ, Schoner B. A comparison of two post systems under applied compressive-shear loads. J Prosthet Dent. 1989; 61:(1)17-24
Musikant BL, Deutsch AS. A new prefabricated post and core system. J Prosthet Dent. 1984; 52:(5)631-634
Ricker JB, Lautenschlager EP, Greener EH. Mechanical properties of post and core systems. Dent Mater. 1986; 2:(2)63-66
Kishen A. Mechanisms and risk factors for fracture predilection in endodontically treated teeth. Endod Topics. 2006; 13:(1)57-83
Papa J, Cain C, Messer HH. Moisture content of vital vs endodontically treated teeth. Endod Dent Traumatol. 1994; 10:(2)91-93
Biven GM, Bapna MS, Heuer MA. Effect of eugenol and eugenol-containing root canal sealers on the microhardness of human dentin. J Dent Res. 1972; 51:(6)1602-1609
Bergeron BE, Murchison DF, Schindler WG, Walker WA Effect of ultrasonic vibration and various sealer and cement combinations on titanium post removal. J Endod. 2001; 27:(1)13-17
Abbott PV. Incidence of root fractures and methods used for post removal. Int Endod J. 2002; 35:(1)63-67
Ricketts DN, Tait CM, Higgins AJ. Tooth preparation for post-retained restorations. Br Dent J. 2005; 198:(8)463-471
Hepworth MJ, Friedman S. Treatment outcome of surgical and non-surgical management of endodontic failures. J Can Dent Assoc. 1997; 63:(5)364-371
Reit C. Decision strategies in endodontics: on the design of a recall program. Endod Dent Traumatol. 1987; 3:(5)233-239
Strindberg LZ. The dependence of the results of pulp therapy on certain factors. Acta Odontol Scand. 1956; 14:(21 suppl)1-175
Weiger R, Axmann-Krcmar D, Löst C. Prognosis of conventional root canal treatment reconsidered. Endod Dent Traumatol. 1998; 14:(1)1-9
Van Nieuwenhuysen JP, Aouar M, D'Hoore W. Retreatment or radiographic monitoring in endodontics. Int Endod J. 1994; 27:(2)75-81
Saunders WP, Saunders EM. Coronal leakage as a cause of failure in root-canal therapy: a review. Endod Dent Traumatol. 1994; 10:(3)105-108
Fan B, Wu MK, Wesselink PR. Coronal leakage along apical root fillings after immediate and delayed post space preparation. Endod Dent Traumatol. 1999; 15:(3)124-126
Karapanou V, Vera J, Cabrera P, White RR, Goldman M. Effect of immediate and delayed post preparation on apical dye leakage using two different sealers. J Endod. 1996; 22:(11)583-585
Fox K, Gutteridge DL. An in vitro study of coronal microleakage in root-canal-treated teeth restored by the post and core technique. Int Endod J. 1997; 30:(6)361-368
Saunders WP. Royal College of Surgeons of England, Guidelines for Surgical Endodontics. 2001;
Hommez GM, Coppens CR, De Moor RJ. Periapical health related to the quality of coronal restorations and root fillings. Int Endod J. 2002; 35:(8)680-689
Kirkevang LL, Orstavik D, Horsted-Bindslev P, Wenzel A. Periapical status and quality of root fillings and coronal restorations in a Danish population. Int Endod J. 2000; 33:(6)509-515
Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J. 1995; 28:(1)12-18
Tronstad L, Asbjornsen K, Doving L, Pedersen I, Eriksen HM. Influence of coronal restorations on the periapical health of endodontically treated teeth. Endod Dent Traumatol. 2000; 16:(5)218-221
Saunders WP. A prospective clinical study of periradicular surgery using mineral trioxide aggregate as a root-end filling. J Endod. 2008; 34(:660-665
Ng YL, Mann V, Gulabivala K. Outcome of secondary root canal treatment: a systematic review of the literature. Int Endod J. 2008; 41:(12)1026-1046
Rud J, Andreasen JO. A study of failures after endodontic surgery by radiographic, histologic and stereomicroscopic methods. Int J Oral Surg. 1972; 1:(6)311-328
Rud J, Andreasen JO. Operative procedures in periapical surgery with contemporaneous root filling. Int J Oral Surg. 1972; 1:(6)297-310
Machtou P, Sarfati P, Cohen AG. Post removal prior to retreatment. J Endod. 1989; 15:(11)552-554
Hulsmann M. Methods for removing metal obstructions from the root canal. Endod Dent Traumatol. 1993; 9:(6)223-237
Suter B, Lussi A, Sequeira P. Probability of removing fractured instruments from root canals. Int Endod J. 2005; 38:(2)112-123
Stamos DE, Gutmann JL. Survey of endodontic retreatment methods used to remove intraradicular posts. J Endod. 1993; 19:(7)366-369
Castrisos T, Abbott PV. A survey of methods used for post removal in specialist endodontic practice. Int Endod J. 2002; 35:(2)172-180
Leuebke RG, Glick DH, Ingle JI. Indications and contraindications for endodontic surgery. Oral Surg Oral Med Oral Pathol. 1964; 18:97-113
Posts – when it all goes wrong! part 1: case assessment and management options Sam Rollings Brian Stevenson David Ricketts Dental Update 2024 40:2, 707-709.
Authors
SamRollings
BDS(Hons), MFDS RCS(Ed), MFGDP(UK)
SpR in Restorative Dentistry, Department of Restorative Dentistry, University of Aberdeen Dental School and Hospital, Cornhill Road, Aberdeen
Posts have been used for many years to retain restorations or cores for extra-coronal restorations in endodontically treated teeth. This article discusses the variety of post systems that are available and the incidence and reasons for failure of teeth that have been restored with posts. The treatment options available for the management of such failures are considered, in addition to the indications for both non-surgical and surgical management of endodontic failures. The attitudes of dentists and the perceived complications of attempting post removal are reviewed, along with the evidence to support the prevalence of complications.
Clinical Relevance: Failure of post-retained restorations is a relatively frequent finding due to failure of the restoration itself or the endodontic treatment. It is therefore important to understand and be aware of the various treatment options available, their indications and associated risks.
Article
Posts have been used to restore non-vital, endodontically treated teeth for over two centuries and they still play an important role in contemporary practice. Their use should not, however, be regarded as routine for all endodontically treated teeth and should only be used when there is insufficient coronal tooth tissue to gain retention for a restoration or core for a crown or bridge abutment. It is important to note that posts do not reinforce the roots of weakened, endodontically treated teeth. On the contrary, tooth preparation for post placement can result in further weakening of the root, predisposing it to a vertical root fracture (Figure 1) and can lead to iatrogenic perforation (Figure 2).1–4
Figure 1. Vertical root fracture associated with a post-retained restoration. The tooth is now unrestorable.Figure 2. Iatrogenic perforation associated with UR3 during post space preparation and placement.
If an anterior root-treated tooth has sufficient coronal tooth tissue remaining then there is minimal risk of a fracture compared to a similarly restored vital tooth. These teeth may simply be restored conservatively with a direct, bonded restoration which can, in certain situations, strengthen the tooth.5 Posts are also usually unnecessary in molar teeth as a 4 mm height of pulp chamber wall alone, or in some instances the coronal 1–2 mm of root canal (Nayyar Core), will be sufficient to retain the core.6 Post space preparation in posterior teeth carries with it the risk of lateral perforation because the roots are often curved and/or narrow, in particular the mesial roots of lower molar teeth and buccal roots of upper molar teeth. ‘It has however been recommended that most root-treated posterior teeth should have cuspal protection with a full occlusal coverage indirect restoration.’
Post systems
Active or passive?
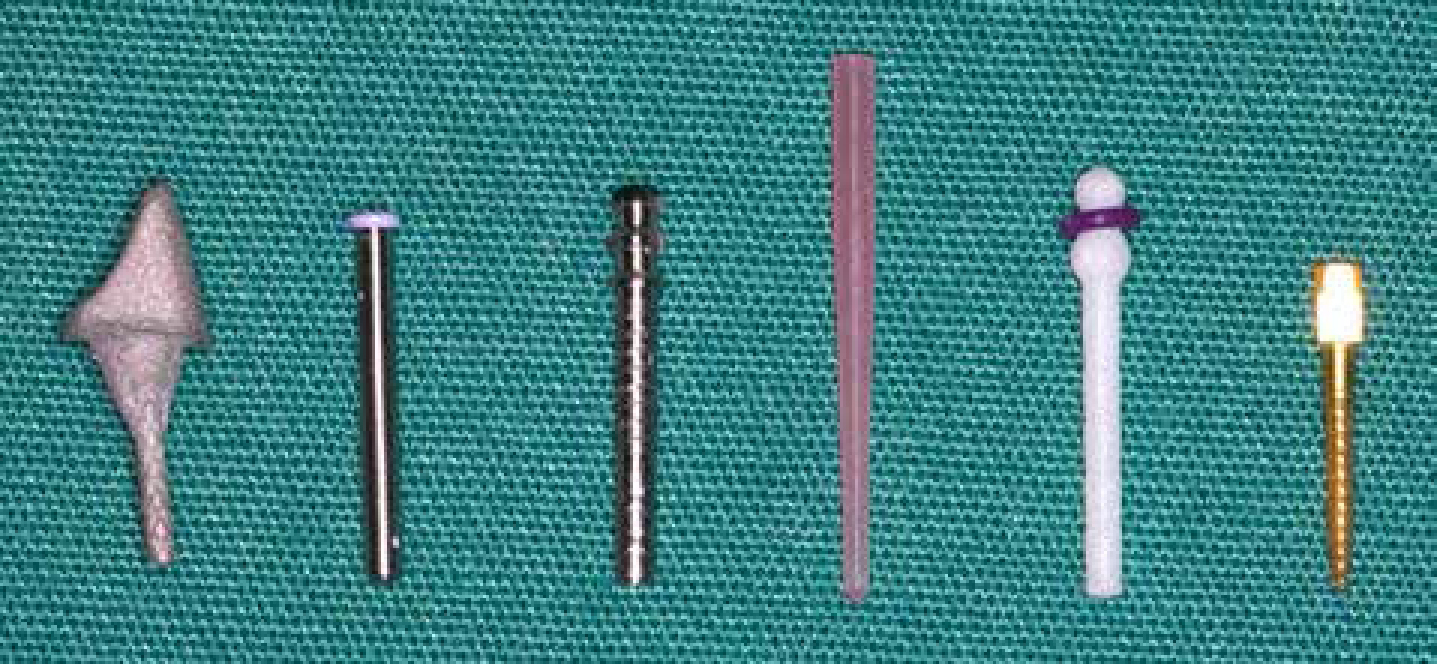
There is a multitude of post systems available on the dental market and Figure 3 illustrates just a small range of post types. Posts can generally be divided into two separate subgroups, depending on whether they are active or passive and hence on how retention is achieved. Active posts are usually prefabricated and threaded in design, and can be either self-threading or pre-tapped. When placing a self-threading post, the thread of the post itself cuts the counter thread into the walls of the dentine. Strains of a greater magnitude are generated if a self-threading post is threaded rapidly compared to slowly as there is less time for strain relaxation to occur between turns.7 Manufacturers of self-threading posts recommend threading the post space until the post is firmly and completely seated prior to cementation, as this reduces the strain generated at the time of cementation.7 Pre-tapped post systems use a pre-tapping device to cut the counter thread into the walls of the dentine prior to post cementation.
Figure 3. A selection of post types available today: from left to right, a precious metal cast post and core, titanium ParaPost® XP™ Temporary Post (Coltène-Whaledent, France), titanium alloy ParaPost® XT™ (Coltène-Whaledent, France), quartz fibre DT Light-Post™ Illusion™ (Recherches Techniques Dentaires, France), quartz fibre ParaPost® Fiber White (Coltène-Whaledent, France) and gold-plated brass Dentatus® Anchorage Post (Dentatus AB, Sweden).
Whilst active posts are more retentive than passive posts of comparable dimensions, the latter are the preferred choice, as less strain is introduced into the root and the risk of irretrievable vertical root fracture is reduced. Passive posts can either be custom-made (usually as a cast post and core) or prefabricated. Their surface is usually either smooth or serrated (negative recesses cut into the post surface) and their shape can be either tapered or parallel. In general, parallel-sided, serrated posts are the most retentive design of passive post.
Metal or non-metal?
Posts can be fabricated from a range of materials which can be divided into metallic or non-metallic compositions. Custom-made cast posts and cores (indirect, laboratory made) are most commonly formed from gold alloys, which have a lower gold content and are harder compared to pure gold, whilst prefabricated metallic posts are mostly made out of stainless steel, titanium, titanium alloy, nickel-chrome or other non-precious metal alloys. Nickel-chrome has the advantage of being strong but, more recently, there has been a trend towards the use of titanium alloy and titanium posts owing to their strength and biocompatibility. Titanium alloys are much stronger than pure titanium due to the addition of small amounts of aluminium and vanadium and, whilst both are easy to use, they do have the disadvantage that they are slightly more radiolucent than nickel-chrome and tend to spark when cut with a high-speed bur. A potential disadvantage of using non-precious metal alloy posts is that they tend to undergo corrosion in situ.8
The newer, non-metallic posts are made out of either carbon or quartz fibres embedded longitudinally in an epoxy resin, or zirconia, and are all substantially more radiolucent than the metallic alternatives. Fibre posts have the advantage that their modulus of elasticity is closer to that of dentine, which results in microscopic flexure. This means that occlusal forces are not directly transmitted to the root dentine, as with a rigid metallic post, which may result in a reduced risk of vertical root fracture. A retrospective study which evaluated the treatment outcome of fibre-reinforced epoxy resin posts and cast post and cores, over a four-year period, found that 9% of the teeth in the group restored with cast post and cores demonstrated root fracture compared to none in the group restored with fibre-reinforced epoxy resin posts.9 Quartz fibre and zirconia posts have the advantage of being translucent, white or tooth-coloured, which has an added aesthetic benefit when used in conjunction with composite cores and all-ceramic crowns or bridges.
Failure of post-retained restorations
In the dental literature, the reported failure rate of post-retained restorations is very variable. Whilst a review of the literature in 2003 by Goodacre et al found that the incidence of complications was about 10%, over a mean observation period of 6 years, an earlier review by Creugers et al reported a higher failure rate in the order of 22% over an average of 5 years follow-up.10,11 The most common reasons reported for failure of post-retained restorations were post loosening, root fracture, caries and periodontal disease. There are obviously many variables which will dictate the success of post-retained restorations and these include:
Patient factors (such as the amount of sound tooth remaining, the occlusion and their caries and periodontal disease risk status);
The type of post used; and
The clinical experience and abilities of the dentist.
Bearing these factors in mind, Weine et al reported one of the highest success rates for teeth which had been restored with cast, tapered posts and cores and found that, over a 10-year period, only nine out of 138 teeth (6.5%) failed.12 It is worth noting that more restorations fail due to decementation, root fracture or iatrogenic perforation than from endodontic failure.13
In summary, the reasons for failure of teeth restored with post-retained restorations can either be based on biological failure, iatrogenic damage or material/design failure. The causes of these and their management are detailed in Table 1.
Reason for Failure
Aetiology of Failure
Treatment
Biological
Caries
Failed primary and secondary prevention
High caries risk
Poor marginal fit/contour
Assess restorability
Patient centred preventive approach
Repair margin
Consider replacement of restoration
Periodontal disease
Failure to stabilize disease
Poor oral hygiene
Susceptible patient
Presence of plaque retentive factors
Assess prognosis
Patient centred preventive approach
Eliminate any plaque retentive factors
Periodontal treatment
Endodontic failure
Inadequate initial endodontic treatment
Resistant bacteria
Coronal leakage
Remove post and carry out repeat orthograde root canal treatment
Damage to root surface caused by trauma or over heating with post space drill in the presence (inflammatory) or absence (replacement) of infection
External inflammatory resorption – remove post and carry out repeat orthograde root canal treatment and surgical treatment if appropriate and accessible
External replacement resorption – monitor and maintain, or extract if severe
Root fracture: vertical/horizontal/angular
Unnecessary weakening of the root by overzealous tooth tissue removal during endodontic treatment or post space preparation
Extensive tooth tissue loss due to caries or fracture
No ferrule
Traumatic occlusion
Extraction in almost all instances with deep subgingival fractures
Iatrogenic
Perforation of root
Inappropriate or difficult endodontic treatment
Inappropriate post space preparation
Root resorption – see above
Depending on accessibility repair can be carried out either internally or externally via a surgical approach:
Repair with MTA (Mineral Trioxide Aggregate, Tulsa Dental, OK) or similar material if below alveolar crest (sub-crestal)
Repair with glass ionomer or resin composite-based materials if above alveolar crest (supra-crestal)
Material/design
Fracture or bending of post
Poor design – eg post too narrow
Increased occlusal forces
Casting/manufacturing errors
Remove post, assess and eliminate reason for failure and replace restoration using new design as required
Core failure
Inappropriate material use and/or techniques
Replace core
Decementation
Inadequate length of post
Lack of retentive features eg no serrations
Traumatic occlusion
Poor cementation technique
Assess and eliminate reason for failure and either recement or replace restoration using new design as required
Many of the causes of failure outlined in Table 1 are not specific to post-retained restorations, but those that are, such as decementation, root fracture, perforation and endodontic failure will be discussed in more detail.
Decementation
Physiological micro-movement of natural teeth occurs throughout the day due to normal masticatory forces, which can lead to partial breakdown of the cement lute around post-retained restorations.14 Disruption of the cement lute around the most coronal aspect of the post results in the fulcrum of movement transferring apically, which amplifies the lever action. This magnifies the stress, which is transmitted to the remaining cement lute, resulting in failure of the restoration due to complete decementation of the post or, at worst, root fracture.15–17 This pattern of failure is often accelerated with passive, prefabricated parallel-sided posts as there is often poor adaptation of the post to the coronal third of the post space.17–19 Active, threaded posts pose a specific problem because significant coronal leakage and caries can occur around the post prior to the threads disengaging, at which stage the tooth may be unrestorable.
Root fracture
Root canal treatment has been implicated as a major aetiological cause of tooth fracture, the reasons for which are due to a variety of factors including:
Dentinal weakness;
The restorative materials and endodontic medicaments used; and
It was at one stage thought that endodontic treatment resulted in a decrease in the moisture content of the dentine, which resulted in the tooth becoming more brittle and therefore more prone to fracture. A study by Papa et al, however, contradicts this theory as they demonstrated, using matched pairs of freshly extracted human teeth, that there was no statistical difference in the moisture content between root canal treated teeth and vital teeth.21 This having been said, it is generally accepted that root canal treated teeth have decreased strength, but this is more likely to be due to loss of coronal tooth structure rather than any changes in the biochemical properties of the dentine which may have occurred following removal of the pulp.
It is possible that some types of endodontic sealer may affect the physical properties of root canal treated teeth. For example, eugenol has been shown to increase the microhardness of dentine and is often a constituent in root canal sealers.22 Some types of endodontic sealer may also influence the retention of posts, as a study by Bergeron et al demonstrated that the use of a resin-based sealer, AH26 (Dentsply/Maillefer, Tulsa Dental, OK), significantly increased the retention of posts, compared to groups obturated with a zinc oxide and eugenol sealer, Roth's 801 Elite Grade cement (Roth International, Chicago, IL).23
Preparation of a root for a post further weakens the root dentine, however, careful removal of gutta-percha root filling material and post space preparation with gradually increasing sized instruments (Gates Gliddens and post space drills/reemers) to no greater than a third of the diameter of the root, can potentially reduce the risk of root fracture. This having been said, the risk can never be completely eliminated as occlusal forces are transmitted to the weakened root.
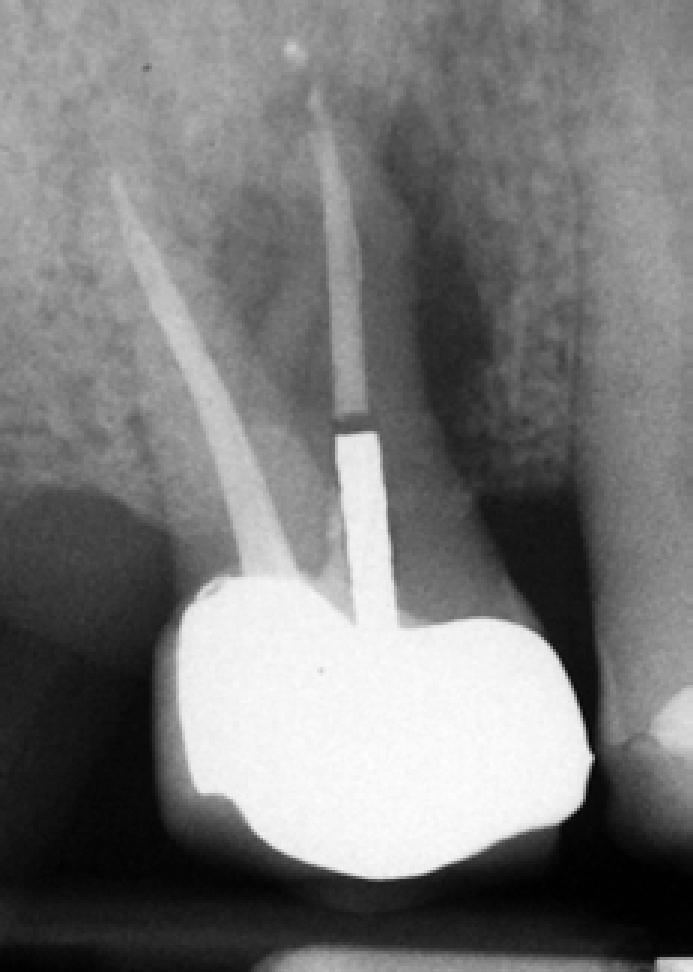
There are a number of signs that may indicate the presence of a vertical root fracture. The classic signs include mobility of the post and restoration, repeated decementation of the restoration and the presence of an isolated, deep and narrow periodontal pocket. Other signs and symptoms may include sinus formation, tenderness to biting, tenderness to percussion and increased mobility of the tooth, however, these signs could also be associated with peri-radicular periodontitis.24 Radiographs may aid in the identification of a vertical root fracture by demonstrating the presence of a complete or incomplete fracture line, or by a general widening of the periodontal ligament space.24 The classic radiographic sign of a long-standing vertical root fracture is a halo radiolucency (Figure 4). However, the use of a radiograph for the diagnosis of a vertical root fracture in the absence of any clinical signs or symptoms should be interpreted with care as, for a fracture line to be visible radiographically, the x-ray beam has to pass along the line of an undisplaced fracture, which would be a rare event. Horizontal and oblique root fractures that occur in relation to posts are usually as a result of excessive occlusal forces, poor post design or a lack of ferrule. The importance of the ferrule effect in increasing the fracture resistance of a post restored tooth has been well documented in the literature.25 The ferrule is the collar of tooth tissue that is encompassed and braced by the crown that is cemented onto the core and tooth preparation. In Figure 5a, the teeth have approximately 4 mm of coronal tooth tissue to brace and create a ferrule effect with the cemented crown, whilst in Figure 5b the teeth have no coronal tooth tissue for a ferrule and, as such, are more susceptible to root fracture.
Figure 4. Radiographic appearance of a tooth with a long-standing vertical root fracture.Figure 5. Teeth prepared for post-retained restorations with (a) and without (b) the ferrule effect.
Perforation
Root perforation during post space preparation is usually the result of poor pre-operative assessment (narrow, curved or tilted root) and/or poor operator technique (use of post drills that are too wide and end-cutting). Most perforations, whilst usually avoidable, significantly reduce the prognosis of the tooth. The success of perforation repair is largely dependent on the material used, timing of the repair and location of the perforation. MTA (Mineral Trioxide Aggregate, Tulsa Dental, OK) is the material of choice for perforations created below bone level, whilst glass ionomers or resin composite-based materials can be used if the perforation is supra-crestal. Perforation repairs should ideally be placed as soon as possible after the perforation has occurred. Generally, cervical third perforations have a poorer prognosis, especially if they are involved with the epithelial or connective tissue attachment of the tooth compared to those occurring in the mid or apical third. Perforations are often easier to repair internally with the aid of an operating microscope and surgical repair (external repair) of a perforation is easier if the perforation is accessible from the labial/buccal aspect of the root. A newer material, Biodentine™ (Septodont, France), a bioactive, calcium silicate cement, was launched in 2010 and shows great promise for applications such as perforation repair and other indications advocated for MTA.
Endodontic failure
Distinguishing between healing of an endodontic lesion and failure can be difficult. It is recommended that endodontically treated teeth are followed up for at least four years to assess the treatment result and therefore serial radiographs are required to determine radiographic failure.26–29 One study reported little deterioration in teeth with small periapical areas, sometimes over an extended period of time.30 Therefore, careful case selection may allow monitoring of small, clinically asymptomatic periapical areas, however, large, expanding periapical radiolucencies require either repeat orthograde root canal treatment, peri-radicular surgery or extraction and replacement if indicated.
Once it has been established that endodontic failure has occurred, it needs to be addressed. Inadequate root canal treatment is usually the cause and may be due to:
Insufficient shaping and cleaning of the root canal system;
Under or over filling when obturating;
The presence of uninstrumented canals or recalcitrant infection.
Microleakage may also contribute to endodontic failure, and the importance of the coronal seal has been well documented.31 The chances of endodontic failure can be reduced by preparing the post space immediately after obturation and placing the definitive post crown as soon as possible, providing the tooth remains asymptomatic.32,33 Temporary post crowns leak considerably more along their entire length compared to permanently cemented posts and their prolonged use should be avoided.34
General treatment planning considerations
An alternative to salvaging a failed post and providing repeat endodontic treatment (non-surgical or surgical), if required, would be to extract the tooth and replace it, if clinically indicated, using either a fixed (implant- or tooth-retained) or removable prosthesis. The decision whether to invest significant clinical time from the patient's perspective, as well as the dentist's, and the cost of treatment will depend on a number of patient and clinical factors. Whether the tooth is in the aesthetic zone, is a strategic tooth for retention of a fixed or removable prosthesis, or there are medical reasons to avoid extraction will influence the decision-making process. Other clinical factors, such as the tooth's restorability, periodontal bone support, presence of an existing removable prosthesis which could be simply added to, and long-term prognosis of treatment, should also be considered.
Treatment of endodontic failure
Endodontic failure can be treated either non-surgically or surgically, however, there are clear indications for adopting each approach.35 Unfortunately, many dentists prefer to adopt a surgical approach as post removal is considered time consuming and also requires the provision of a new restoration. Dentists are also wary of the risk of complications occurring, in particular root fracture. However, there is evidence that a good quality root filling and adequate coronal restoration is required to provide a seal throughout the entire length of the tooth-restoration interface to produce a satisfactory outcome.36–39 Surgical treatment alone is unlikely to treat the deficiency that has led to endodontic failure, therefore removal of the post-retained restoration is often required to enable repeat orthograde root canal treatment and placement of an adequate coronal restoration.
The probability of success of a non-surgical approach must be weighed against the predictability of micro-surgical management.40 Repeat orthograde root canal treatment of previously failed endodontic therapy provides good results, even if a post is present and has to be removed. A relatively recent systematic review reported a pooled success rate of approximately 77%.41 Surgical success is more predictable when the cleanliness of the root canal and the quality of endodontic obturation have been improved prior to surgery via an orthograde approach.42,43 There may also be various medical considerations (eg patients on bisphosphonates) or anatomical considerations (proximity to the maxillary antrum or inferior dento-alveolar neurovascular bundle) that contra-indicate surgery.44 If the root canal preparation and obturation is inadequate, repeat orthograde root canal treatment is advised as a surgical approach will not completely cleanse and seal the root canal system.45 A surgical approach alone may be indicated if there is a satisfactory coronal seal and if no improvement can be made to the technical quality of the root canal filling. The main indications for a purely surgical approach are listed in Table 2.24,45,46
Recently revised root canal treatment that cannot be improved upon
Very wide post in a thin root
If post removal is likely to weaken the root excessively
If there is an extremely long, well-fitting post which has a low chance of successful removal
If following post removal the tooth is likely to be rendered unrestorable
Occasionally for financial reasons
Unusual root canal anatomy
Excessive overfill of root canal filling
The presence of a separated instrument where it is inadvisable to attempt removal by an orthograde approach or bypass
Assessment prior to post removal
Assessment of a tooth which is to undergo post removal will involve both a clinical and radiographic examination in addition to obtaining as much information as possible from the patient's clinical notes regarding the placement of the post due for removal, in particular the type of post placed and the luting cement used. A pre-operative long cone paralleling periapical radiograph of the tooth is essential to confirm the presence of the post and aid with assessment. However, it is important to remember that a radiograph only gives a two-dimensional image of a three-dimensional object. The assessment allows the dentist to determine which method of post removal has the highest likelihood of success in the given clinical situation. Some clinical situations may contra-indicate certain post removal techniques as they jeopardize the remaining tooth/root structure.
Factors that need to be taken into consideration in relation to the post are:
The number of posts and their location/orientation in the tooth;
The post design (active or passive; tapered or parallel-sided; smooth or serrated);
Is the post part of the crown substructure (integral post crown);
The post material;
The accessibility of the post;
The cemented depth;
The type of cement;
The post adaptation to the post space; and
The length and diameter of the post in relation to the root.
Factors that need to be taken into consideration in relation to the tooth, root and restoration are:
The circumferential dimension of the root;
The length of the root;
The root curvature (including any external concavities);
Remaining coronal dentine after post removal; and
Type of core restoration.
Other factors that need to be considered are:
The availability of inter-arch space;
Adequate access for removal;
Patient co-operation;
Does the dentist have the equipment and expertise to complete the procedure and deal with any complications; and
How the tooth will be temporized during the procedure (especially if it is in the aesthetic zone).
A dentist's judgement, training, experience and opportunity to access various post removal devices and instruments will influence the success of post removal. In addition, each of the factors mentioned above will influence how successful post removal is likely to be. These factors will be discussed in more detail with the individual techniques for post removal in the next article in this series of two.
Attitudes towards and complications of post removal
Complications can occur with both the attempted removal of a post-retained restoration and the subsequent treatment that will be required to restore the tooth definitely. Complications include root perforation, root fracture, endodontic flare up, excessive removal of tooth substance rendering the tooth unrestorable, extraction (due to the use of post pullers), post fracture and damage to the periodontal ligament cells (due to inadequate cooling while using ultrasonic energy or during post space preparation). A survey of American Endodontists confirmed these concerns.47 First, there was a generalized perceived danger that post removal could cause a root fracture or perforation, especially if the post in question was long, large and threaded. It is interesting to note, however, that there is currently no evidence in the literature to support this widespread belief.24,47,48 Secondly, it was thought that posts cemented with resin composite cements could not be removed regardless of the techniques available. Thirdly, there was a reluctance to attempt post removal if the tooth in question was incorporated in the design of a multi-unit fixed restoration or removable prosthesis. Finally, remuneration issues may have also played a role.
A further survey by Castrisos and Abbott investigated the attitudes of members of the Australian and New Zealand Academy of Endodontists towards carrying out post removal for a tooth which required endodontic retreatment.48 Sixty-six percent preferred to remove the post, whilst 27% were indifferent as to either post removal or surgical management. Of those who preferred a surgical approach, 75% were concerned about root fracture. However, out of the 66% who preferred to remove the post, only 46% were concerned about root fracture. The occasions when post removal may be avoided were:
In the presence of a wide post in a tooth with a thin root;
If the restoration was clinically satisfactory;
If the removal of the restoration would potentially render the tooth unrestorable; or
If the patient chose to have surgery.
It can be gleaned from these studies that many dentists avoid post removal owing to potential adverse events and prefer to carry out surgical treatment.49 Although, in the survey by Castrisos and Abbott, 45% of the endodontists had observed a root fracture during the attempted removal of a post, this is relatively rare and the evidence from this study and another by Abbott has shown that the prevalence of root fracture is 0.002% and 0.06%.24,48 It is also difficult to prove whether attempted removal of the post alone led to the fracture or whether there was a pre-existing fracture in the tooth. It can therefore be concluded that, with good case selection, post removal can be a predictable procedure. The next article in this short series will describe the methods available for removing posts.