Chambrone L, Tatakis DN. Long-term outcomes of untreated buccal gingival recessions: a systematic review and meta-analysis. J Periodontol. 2016; 87:796-808 https://doi.org/10.1902/jop.2016.150625
Khocht A, Simon G, Person P, Denepitiya JL. Gingival recession in relation to history of hard toothbrush use. J Periodontol. 1993; 64:900-905 https://doi.org/10.1902/jop.1993.64.9.900
Jati AS, Furquim LZ, Consolaro A. Gingival recession: its causes and types, and the importance of orthodontic treatment. Dental Press J Orthod. 2016; 21:18-29 https://doi.org/10.1590/2177-6709.21.3.018-029.oin
Chan HL, Chun YH, MacEachern M, Oates TW. Does gingival recession require surgical treatment?. Dent Clin North Am. 2015; 59:981-996 https://doi.org/10.1016/j.cden.2015.06.010
Baldi C, Pini-Prato G, Pagliaro U Coronally advanced flap procedure for root coverage. Is flap thickness a relevant predictor to achieve root coverage? A 19-case series. J Periodontol. 1999; 70:1077-1084 https://doi.org/10.1902/jop.1999.70.9.1077
Hwang D, Wang HL. Flap thickness as a predictor of root coverage: a systematic review. J Periodontol. 2006; 77:1625-1634 https://doi.org/10.1902/jop.2006.060107
Cairo F. Periodontal plastic surgery of gingival recessions at single and multiple teeth. Periodontol 2000. 2017; 75:296-316 https://doi.org/10.1111/prd.12186
Cairo F, Nieri M, Pagliaro U. Efficacy of periodontal plastic surgery procedures in the treatment of localized facial gingival recessions. A systematic review. J Clin Periodontol. 2014; 41:S44-62 https://doi.org/10.1111/jcpe.12182
Norberg O. Ar en utlakning utan vovnadsfortust otankbar vid kirurgisk behandling av. S. K. Alveolarpyorrhoe?. Svensk Tandlaekare Tidskrift. 1926; 19
Zucchelli G, De Sanctis M. Treatment of multiple recession-type defects in patients with esthetic demands. J Periodontol. 2000; 71:1506-1514 https://doi.org/10.1902/jop.2000.71.9.1506
Chambrone L, Ortega MAS, Sukekava F Root coverage procedures for treating single and multiple recession-type defects: an updated Cochrane systematic review. J Periodontol. 2019; 90:1399-1422 https://doi.org/10.1002/JPER.19-0079
Buti J, Baccini M, Nieri M Bayesian network meta-analysis of root coverage procedures: ranking efficacy and identification of best treatment. J Clin Periodontol. 2013; 40:372-386 https://doi.org/10.1111/jcpe.12028
Allen AL. Use of the supraperiosteal envelope in soft tissue grafting for root coverage. I. Rationale and technique. Int J Periodontics Restorative Dent. 1994; 14:216-227
Salem S, Salhi L, Seidel L Tunnel/pouch versus coronally advanced flap combined with a connective tissue graft for the treatment of maxillary gingival recessions: four-year follow-up of a randomized controlled trial. J Clin Med. 2020; 9 https://doi.org/10.3390/jcm9082641
Santamaria MP, Neves FLDS, Silveira CA Connective tissue graft and tunnel or trapezoidal flap for the treatment of single maxillary gingival recessions: a randomized clinical trial. J Clin Periodontol. 2017; 44:540-547 https://doi.org/10.1111/jcpe.12714
Wennström J, Lindhe J, Nyman S. Role of keratinized gingiva for gingival health. Clinical and histologic study of normal and regenerated gingival tissue in dogs. J Clin Periodontol. 1981; 8:311-328 https://doi.org/10.1111/j.1600-051x.1981.tb02041.x
Sullivan HC, Atkins JH. Free autogenous gingival grafts. I. Principles of successful grafting. Periodontics. 1968; 6:121-129
Agudio G, Nieri M, Rotundo R Free gingival grafts to increase keratinized tissue: a retrospective long-term evaluation (10 to 25 years) of outcomes. J Periodontol. 2008; 79:587-594 https://doi.org/10.1902/jop.2008.070414
Chambrone L, Chambrone D, Pustiglioni FE The influence of tobacco smoking on the outcomes achieved by root-coverage procedures: a systematic review. J Am Dent Assoc. 2009; 140:294-306 https://doi.org/10.14219/jada.archive.2009.0158
This is the second article in a two-part series on gingival recession. The first article covered the aetiology and prevalence of gingival recession, while this article focuses on the factors affecting decision making and the management, including treatment of gingival recession alongside the evidence base. With more than half of the population suffering from gingival recession, the clinician should be aware of the different options and treatment modalities available to manage gingival recession. This will enable them to engage with the patient, giving them the necessary and required information to make a patient-centred decision about the most suitable treatment option that will address their concerns.
CPD/Clinical Relevance: The clinician should be aware of the different options and treatment modalities available to manage gingival recession.
Article
The first article of this two-part series discussed the prevalence, aetiology and classification of gingival recession. In this article, the different treatment options for managing gingival recession are discussed with an option appraisal of the different treatment modalities and when intervention should be considered.
Gingival recession usually affects the buccal surfaces of teeth, with recession of 1 mm or more involving at least one or more sites in more than half the population.1 Gingival recession per se tends to remain asymptomatic; however, some patients may complain of compromised aesthetics and hypersensitivity, usually exacerbated by an associated habit, such as traumatic tooth brushing. The recession may also contribute to compromised plaque control especially when there are high muscle attachments (Figure 1). However, it has been reported that irrespective of good patient motivation and plaque control, untreated gingival recession does have the tendency for further apical displacement over time.2
Figure 1. High muscle attachment inhibiting effective plaque control and subsequent gingival recession.
This article provides an overview of the decision-making process for the management of patients with gingival recession not caused by periodontal disease, and covers the different types of surgical procedures available.
Decision to treat
The decision to treat gingival recession is driven by patient expectations and site/tooth-related factors that will determine the risk and rate of deterioration of the recession (Table 1). Patients with gingival recession fall into two categories, those who are asymptomatic and those who are symptomatic. Asymptomatic patients will either be aware or unaware of the recession and are often unconcerned by its presence. Symptomatic patients on the other hand will have specific needs dictated by their symptoms, i.e. sensitivity or aesthetics.
Table 1. Indications for the treatment of gingival recession.
Dentine sensitivity
Aesthetic concerns
Non-carious tooth surface loss
Inability to maintain adequate oral hygiene around the defect
Progression of recession defect over time
The presence of predisposing factors and precipitating factors should be considered for all patients with gingival recession. In addition to the normal clinical parameters, such as plaque control and probing depths that are recorded as part of their clinical assessment, for all patients, irrespective of their category, the following should also be considered:
Generalized or localized recession: if localized how many sites?
Is there keratinized gingival tissue present? i.e. none or <2 mm;
Gingival tissue biotype: thin vs thick;
Are there any site-related factors? e.g. root position, muscle attachments
Are there any habits? e.g. picking at the gingivae;
Are there any other factors? e.g. tongue studs;
Is there any periodontal disease?
Once this information has been gathered as part of the history, the patients' expectations should be established and a preventive care plan, outlined in Table 2, agreed with the patient. This plan should be established for both asymptomatic and symptomatic patients, with the preventive strategy aiming to improve patient awareness about their gingival recession and their role in managing it. There should also be a focus on managing and correcting any modifiable aetiological factors, including traumatic brushing techniques or habits that are exacerbating the recession, with adjunctive scaling and polishing and application of desensitizing agents where necessary.
Table 2. List of gingival recession prevention strategies.
Identification of key aetiological agents
Patient education on the condition
Oral hygiene instruction and correction of tooth brushing technique
Smoking cessation
Application of desensitizing agents
Removal of sources of trauma (e.g. piercings and poor toothbrush technique)
Management of periodontal disease
The role of traumatic tooth brushing in recession has been reported, and correcting the brushing technique is a vital first step in the management of the gingival recession even when there are no obvious signs of toothbrush trauma.3 The preventive phase will also provide the opportunity of evaluating the patient's expectations and their compliance. Once this phase has been completed an appraisal of the options, whether to monitor the recession or surgically intervene, should be undertaken. A patient-centred decision should be made so that the patient's expectations and aspirations can be met. Figure 2 suggests the decision-making algorithm to be followed.
Figure 2. Treatment decision-making algorithm for patients with gingival recession.
Monitoring the gingival recession
This option is usually undertaken when there are no symptoms from the recession, the patient decides not to have anything done, or there is a low risk of progressive deterioration over time. The risk of deterioration will be dependent on the patient's habits and the local factors, such as the tooth position, gingival tissue biotype and presence of keratinized tissue and muscle attachments.
Monitoring is usually undertaken following patient education, and includes recording recession charts, photographs and study casts. The recording of recession can be an unreliable measure, especially due to the variation in the probe angulation and position, and thus photographs and study casts offer a more reliable means of monitoring the recession over time.
The recession should be monitored annually and, along with the above parameters, should include a comprehensive periodontal examination and any changes in the patient's history and symptoms. Digitally scanned images, which allow the superimposition of the previous and up-to-date images, can also be used with the key advantage of these providing a direct comparison of the change in the recession defects (Figure 3).
Figure 3. Digital scans, such as this scan of the mandible, can allow review of the recession around these lower incisors over time.
Treatment of gingival recession
In cases where there is a risk of progressive deterioration due to various factors listed above, or there are symptoms or concerns raised by the patient, intervention using a non-surgical or surgical approach may need to be considered.
Non-surgical approach
Different non-surgical options can be considered to treat gingival recession and their use will be dictated by the extent and location of the recession and its severity. Different restorative options, including veneers, crowns or gingival masks, can be used to treat gingival recession however, such options are usually not suitable for localized recession defects. The gingival mask is beneficial in cases where there is generalized recession as a result of periodontal disease with residual recession and ‘black triangles’ (Figure 4). Orthodontic intervention can also be used to treat gingival recession, however, in such cases, further surgical intervention is often required.4
Figure 4. (a–c) Use of a gingival mask to treat generalized recession defects.
Surgical approach
The surgical approach to treating gingival recession aims to address concerns the patient may have about the appearance, or alternatively to manage any local anatomical factors that may influence the future progression of the recession. These include thin gingival tissue biotype, absence or presence of a narrow band (<2 mm) of keratinized tissue, and recession extending beyond the depths of the mucogingival junction.5 A full list of indications and contraindications is presented in Table 3.
Table 3. Indications and contraindications for surgical intervention.
Documented evidence of progressing gingival recession despite appropriate advice and therapeutic intervention
Smoking
Anatomical variation, such as shallow vestibular depth, aberrant frenum position, absence or a narrow band of keratinized tissue (<2 mm) where poor oral hygiene has induced gingival inflammation despite therapeutic intervention being undertaken
Poor oral hygiene and active periodontal disease
The patient has aesthetic concerns that cannot be managed satisfactorily non-surgically
Large defects where surgery outcomes are unpredictable (e.g. Millers Class IV)
Orthodontic or restorative treatment is to be undertaken on a tooth with predisposing factors or the presence of any of the above
In patients who have aesthetic concerns, the rationale for the surgical intervention is to obtain root coverage. Flap thickness >0.8 mm is reported to be a stronger indicator of complete root coverage, and where this is not achievable, biotype modification has been proposed.6,7 Thus, when any surgical intervention is being considered, it is critical that the clinician is clear about the objective of the surgical intervention and the anticipated endpoint. This clarity will help ensure that effective communication with the patient takes place, thus ensuring that the patient expectations are managed, especially in situations where complete root coverage is not achievable. When surgical treatment is being planned the clinician must ask the following questions:
Is there enough keratinized tissue?
Are there any muscle attachments?
What is the gingival tissue biotype, thin or thick?
How prominent is the root in the alveolar housing?
Are there any cervical restorations?
What do I want to do – achieve root coverage or increase the band of keratinized tissue to prevent progression?
Depending on the answers to the above questions, the clinician will be able to plan the appropriate surgical treatment and communicate this with the patient. This ensures that the patient fully understands the proposed surgery and the anticipated endpoint, especially if this is at variance to what the patient is expecting. Root coverage procedures are planned to cover root surfaces when hypersensitivity and/or aesthetics are of concern. In contrast, when there is lack of keratinized tissue, the objective of the surgical intervention will be to increase the band of keratinized tissue in the first instance, and not necessarily cover the root surface.
Root coverage techniques are undertaken with either a coronally advanced flap alone, or more commonly with a connective tissue graft (CTG) taken from the palate (Figure 5). In contrast, free gingival grafts (FGG) are taken when increased keratinized tissue is needed and usually have unpredictable results when considered for root coverage (Figure 6).
Figure 5. (a–c) Patient with recession defect treated with CTG and coronal advancement flap with the aim of achieving root coverage. Courtesy of Hong Jin TanFigure 6. Patient with a narrow band of keratinized tissue (a) before and (b) after FGG procedure.
Alternative materials are also available instead of the autogenous grafts for root coverage and enhancing tissue thickness. These off-the-shelf materials help overcome the disadvantages associated with second-site morbidity and quantity. These materials act as scaffolds for fibroblasts and endothelial cells to build up new connective tissue and promote epithelial cell migration from the borders of the adjacent tissue over the matrix.
Autogenous material demonstrates better outcomes in relation to mean root coverage and the percentage of sites exhibiting complete coverage than alternative materials.8 While guided tissue regeneration using barriers has been proposed for root coverage procedures, owing to the risks with membrane exposure and adverse outcomes, the technique has not gained widespread use.9 Other materials, such as enamel matrix-derived proteins, have also been advocated; however, the evidence base behind the use of these and their outcomes remains limited.9
Techniques
Coronally advanced flap (CAF)
This is the most widely used flap design for root coverage, first described by Norberg in 1926,10 and has since undergone several modifications. The flap uses a split-full-split approach to overcome issues with scar tissue formation and blood supply. The procedure was modified with no vertical releasing incisions for use with multiple recession defects by Zuchelli and De Sanctis.11 In cases where there is at least 2 mm of keratinized tissue beyond the recession defect, and at least 1 mm of gingival tissue thickness with no other anatomical factors, then the CAF on its own will give good results. However, for most cases, predictability, gingival tissue stability and long-term outcome is improved when a CTG is used with the CAF.12 This is especially relevant if there are muscle attachments or thin to no keratinized tissue. In these cases, harvesting a CTG with an epithelial collar should be considered to enable a concurrent increase in both keratinized tissue width and overall tissue thickness, while also improving the graft handling properties (Figures 7–9).
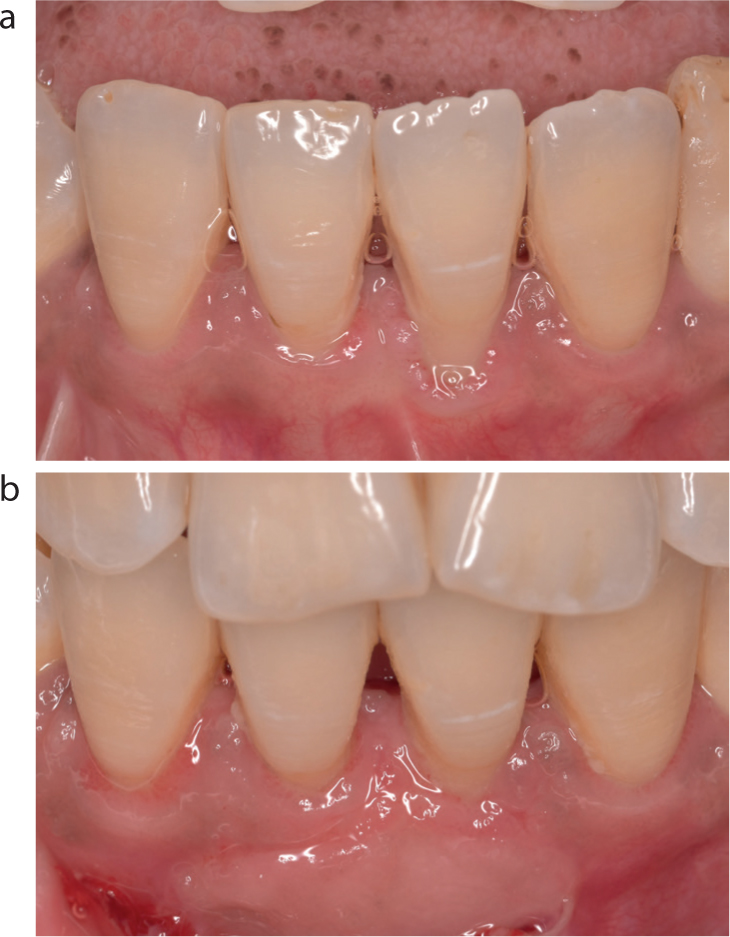
Figure 7. Harvesting a CTG with an epithelial collar can not only increase the band of keratinized tissue present at the recipient site, but also improve graft handling.Figure 8. (a,b) This patient has undergone FGG to increase the band of keratinized tissue, but creep of the gingival margin over time has also led to increased root coverage.Figure 9. (a–c) Use of a CTG with epithelial collar to concurrently increase keratinized tissue, tissue thickness, as well as achieve metal coverage around a dental implant.
The CAF with a CTG has been reported to be the gold standard for root coverage for both single and multiple recession defects.12,13 The European Federation of Periodontology (EFP) suggest that CTG with enamel matrix derivatives (EMD) have better outcomes than CTG alone; however, CTG with CAF demonstrates significantly better outcomes than both in terms of keratinized tissue gain as well as recession reduction.9
Tunnelling techniques
Tunnelling techniques have also been used, either full thickness or partial thickness, depending on the gingival tissue biotype, for root coverage with a CTG. Studies have shown no significant differences between the tunnelling technique and CAF and connective tissue in terms of root coverage; however, others have indicated a superior clinical outcome with a CAF.14,15,16 Tunnelling techniques are challenging, and both operator- and technique-sensitive.
Other techniques
The double papilla flap and laterally sliding flaps with a CTG have also been used for root coverage procedures; however, these flaps tend to be technique-sensitive and in the authors' experience, often some unzipping of the flap occurs during the healing phase with suboptimal outcomes.8,17,18 A full range of techniques, their indications advantages and disadvantages are presented in Table 4.
Table 4. Indications, advantages and disadvantages for each surgery type.
Single or multiple recession defects where root coverage is the desired outcome and there is an adequate width of keratinized gingivae and a deep vestibule
High predictability
Single-site surgery so less morbidity
High percentage of root coverage
Can treat multiple defects
Can be combined with: CTG; GTR; ADMG; EMD; XMG; or other biomaterials
Good aesthetics
Retains its own blood supply
Not possible if there is inadequate keratinized tissue width or a thin gingival biotype unless completed alongside another procedure
This can be combined with coronal advancement surgery to increase the thickness of the gingival tissue covering the recession defects in thin gingival biotypes
High predictability
High percentage of root coverage
Allows coronal advancement surgery to be used even with thin gingival biotype
Good aesthetics
Second surgical site with increased morbidity when compared to alloplastic biomaterials
Techniques using FGG are aimed at increasing the band of keratinized/attached gingivae, and removing aberrant frenal/muscle attachments or shallow vestibules. Although it has been shown that keratinized tissue is not needed for health, the lack of keratinized tissue compromises the patient's ability to maintain plaque control, thereby leading to inflammation.19
The FGG, in small recession defects can be placed directly over the denuded root surface to obtain increased keratinized tissue and coverage.20 For deep recession defects where there is <2 mm or lack of keratinized tissue, the FGG is placed to obtain an increase in the keratinized tissue. If root coverage is subsequently desired, a CAF with a CTG, as described above, can then be undertaken. The success rate of FGG varies widely, between 11% and 100%, when success is defined by root coverage, with an average increase in keratinized tissue width in the year post surgery of 4.2 mm.21,22
Creeping attachment is often seen after FGG are placed and is a result of the coronal migration of the grafted gingivae. This can take place over several years following the surgery.23 The amount of creep that takes place is determined by the width of the recession, the positions of the graft and the tooth, and the oral hygiene of the patient.23 Narrow recession defects, where the graft has been placed over the denuded zone, show the most creep leading to complete root coverage. Figure 8 shows a case where a FGG was used in a narrow recession defect to increase the keratinized tissue with coronal creep taking place over a period of time.
Dehiscences/recession defects around dental implants
Peri-implant soft tissue dehiscences or recession defects have been reported, and while the techniques outlined above can be considered to treat these, it is important to appreciate that the outcome will be dependent on several factors. These include the bucco-lingual position of the implant, the shape of the implant-retained crown, and the height of the anatomical papillae. These factors will need to be taken into consideration when establishing the objective for intervention to ensure that the correct choice has been adopted for treatment. The benefit of keratinized tissue around dental implants has been reported, and has been shown to reduce the risk of peri-implant mucositis and inflammation.24Figure 9 shows the use of CTG with an epithelial collar to concurrently increase keratinized tissue, tissue thickness and achieve exposed metal coverage around a dental implant.
Long-term maintenance
Once the treatment for the gingival recession has been completed, the patient should be followed up and documented on a regular basis to monitor the stability of the grafted sites. This should include a summary of the treatment completed, the objective of treatment and a record of the outcome achieved against this desired objective. Aetiological factors, including the patient's brushing technique and correction of these factors, should also be noted and these parameters should be evaluated when monitoring the site during the recall period. Over time other patient-related factors, as well as the ongoing tooth brushing technique, should continue to be monitored, and the patient reminded of the influence of these on the treatment outcome. Predictable and successful treatment outcomes can be achieved when recession is managed effectively; however, patient engagement and understanding is of key importance for long-term outcomes to be sustained.
Conclusion
This article highlights the importance of the clinician being aware of the factors that influence the presence of gingival recession and the role the clinician plays in raising the patient's awareness of these factors if the treatment of the gingival recession is to be successful. The role of the first phase of treatment, with prevention and correction of the modifiable and susceptibility factors, has been highlighted with the different options for treatment underpinned by the evidence base. Successful outcome of the surgical treatment is dependent on careful and structured planning, with the objective of the treatment being considered to ensure that the patient is given the correct information to aid their decision making.