Although professional Burnout is widely acknowledged, this paper proposes the concept that, in dentistry, there is a seldom identified phenomenon of Patient Burnout in some patients undergoing complex treatment, and that this may, on occasion, contribute to eventual Dentist Burnout. Warning signs and symptoms of potential Burnout patients are discussed and strategies proposed to prevent or minimize Patient Burnout
CPD/Clinical Relevance: As dentistry becomes increasingly complex and patient expectations often exceed the dentists' ability to deliver, the identification and management of Patient Burnout is likely to become an important factor in dental practice.
Article
In the past 20 years, there has been much focus on dental professionals' Burnout. Maslach and Jackson define Burnout as ‘a syndrome of emotional exhaustion (EE) and cynicism that occurs frequently among individuals who do “people-work” of some kind’.1 A recent systematic review into factors contributing to Burnout in dentistry identified 115 papers in its search, of which 33 were of a quality that met inclusion criteria.2 Although this, and many other publications, refer to Burnout in dentistry, they focus almost exclusively on the Dentist, the Dental Support Staff and Dental Students but, an equal and very necessary participant in dentistry, the PATIENT, is seldom, if ever, mentioned as a potential victim of dental Burnout.
Clinical dental care is the most invasive healthcare intervention which many patients experience outside of a hospital. Although GPs will carry out intimate personal examinations in a practice setting, these are generally brief and spaced, while complex dental care will often involve a long series of regular, potentially stressful, appointments over a protracted period of time. The increasing complexity of treatment options, high, and often unrealistic, patient expectations, and a focus on treatment rather than care, with less emphasis on diagnosis and planning than on performing procedures, all contribute to the potential development of an emotionally exhausted patient. A focus on ‘selling’ dental treatment and less on delivery of care, where the patient is often referred to as a client or customer, can result in a dissatisfied patient who may feel that he/she has been coerced into extensive and often expensive and irreversible treatment, rather than having been given time to consider all options and given informed consent freely. When this treatment extends over a long period, or leads to complications or disappointing results, there can be cumulative chronic stress which gradually erodes the patient/dentist relationship.
It is the purpose of this paper to put forward the hypothesis that Patient Burnout is an entity in its own right, and that, as a caring profession, we should be equally focused on the psychological as well as the dental wellbeing of our patients. We should be able to identify warning signs, prevent these, if possible, and manage this problem when necessary. It is also our purpose to propose a two-way relationship between Patient and Dentist Burnout, whereby a practitioner exposed to a number of patients undergoing protracted or complex treatment plans and manifesting signs of Burnout, cumulatively overwhelm the clinician, leading to the Emotional Exhaustion which typifies professional Burnout, hence developing a vicious circle. Dentist Burnout and the possible influences of Social Media were addressed in a previous article.3
Diagnosing Patient Burnout
Signs and symptoms of Patient Burnout
We can all have bad days, and one negative contact with a patient should not be over-interpreted. However, progressive negative changes in the patient/dentist relationship are likely warning signs. We should be watchful for some or all of the following:
The patient becomes less communicative and no longer maintains eye contact;
The patient presses for earlier completion of treatment even if well within the projected timeframe;
The patient becomes less tolerant of minor setbacks, such as provisional restorations needing repair or being kept waiting a few minutes before a treatment visit. Major setbacks, such as an implant failing to integrate, are met with a sullen silence followed by a negative attitude to retreatment ‘…I just know it's not going to work for me’;
The patient starts to arrive late for an appointment, or set deadlines (‘I have to be out of here by 4.30 to pick up my child’);
The phrase ‘…I didn't realize…’ becomes a feature of conversation. A Google search or advice from a friend leads the patient to ask ‘…why didn't you…?’;
The patient starts to question specific parts of his/her agreed treatment plan, (‘why do I need to see the hygienist every 3 months when I only came here to improve my smile?’);
The patient exhibits selective memory, focusing on what he/she wants but ‘forgetting’ having given consent to needed preparatory stages;
There can be many other individually small but cumulatively significant manifestations.
Likely candidates – can we spot them?
Nothing has been identified in the dental literature concerning Patient Burnout, however, with regard to medical Patient Burnout, likely candidates are identified as those going through life with chronic pain, chronic disease, rare auto-inflammatory diseases, and disability. A typical example is given by Lloyd.4 ‘…In August………I spent 12 out of 31 days at a hospital having either a doctor's appointment, a treatment or a test. I'm feeling quite burnt out right now. I still have two more major appointments in the next two weeks to get through and, at this point, while they are necessary, I am gritting my teeth just to get through them’.
Similarities in dentistry can be found in patients with complex and protracted treatment plans, often with a multidisciplinary component involving co-ordination of two or more clinicians. It has been our experience that four groups are particularly vulnerable to this problem.
Patients with a limited experience of complex and advanced dental care. Although inexperienced patients may consent to a complicated treatment plan extending over many months and multiple visits, if their only past dental experiences have involved emergency or basic operative care achieved in one or two visits, their lack of ‘Dental Sophistication’ can result in limited dental stamina, which may not be sufficient to cope with longer, more complex and, on occasion, uncomfortable appointments. This type of patient will often comment ‘….. didn't realize…’ as prolonged treatment progresses.
Patients whose primary focus is on a specific end result (often of a cosmetic nature). While they may well understand and agree to necessary preparatory procedures, such as periodontal management or orthodontic tooth movement, as time goes by they can become frustrated at the apparent ‘lack of progress’ and manifest evidence of the Emotional Exhaustion that typifies Burnout. ‘….why are you moving my back teeth when I only came to see you about the spacing of my top front teeth?….I wish I had never started this’.
Patients who undergo a significant change in circumstances during a long treatment plan. This may be a change in personal circumstances, such as a divorce or illness of a family member, or a change in occupational circumstances, such as a job loss, bankruptcy or even promotion, allowing less time to attend for treatment.
Patients who require extensive retreatment because of previous complex dental treatment which is failing. This is often of a poor standard and has been an ongoing frustration because of unanticipated problems, pain and often a falling-out with the original dentist. The patient is already close to Burnout and, despite our best efforts, what we may perceive as a minor setback can be sufficient to tip him/her over the edge. Patient frustration is often generalized to the profession as a whole and the new clinician in particular.
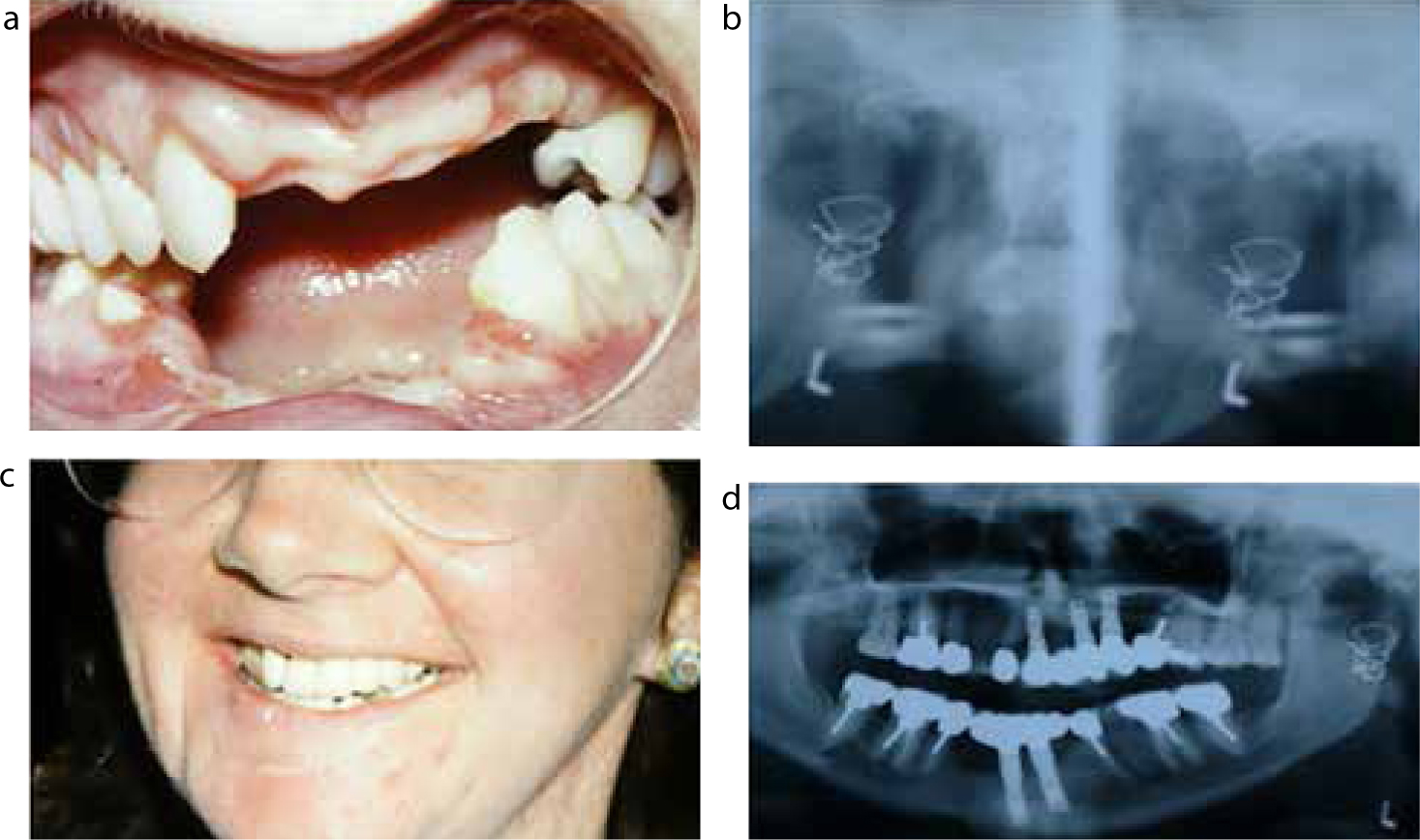
Figure 1.
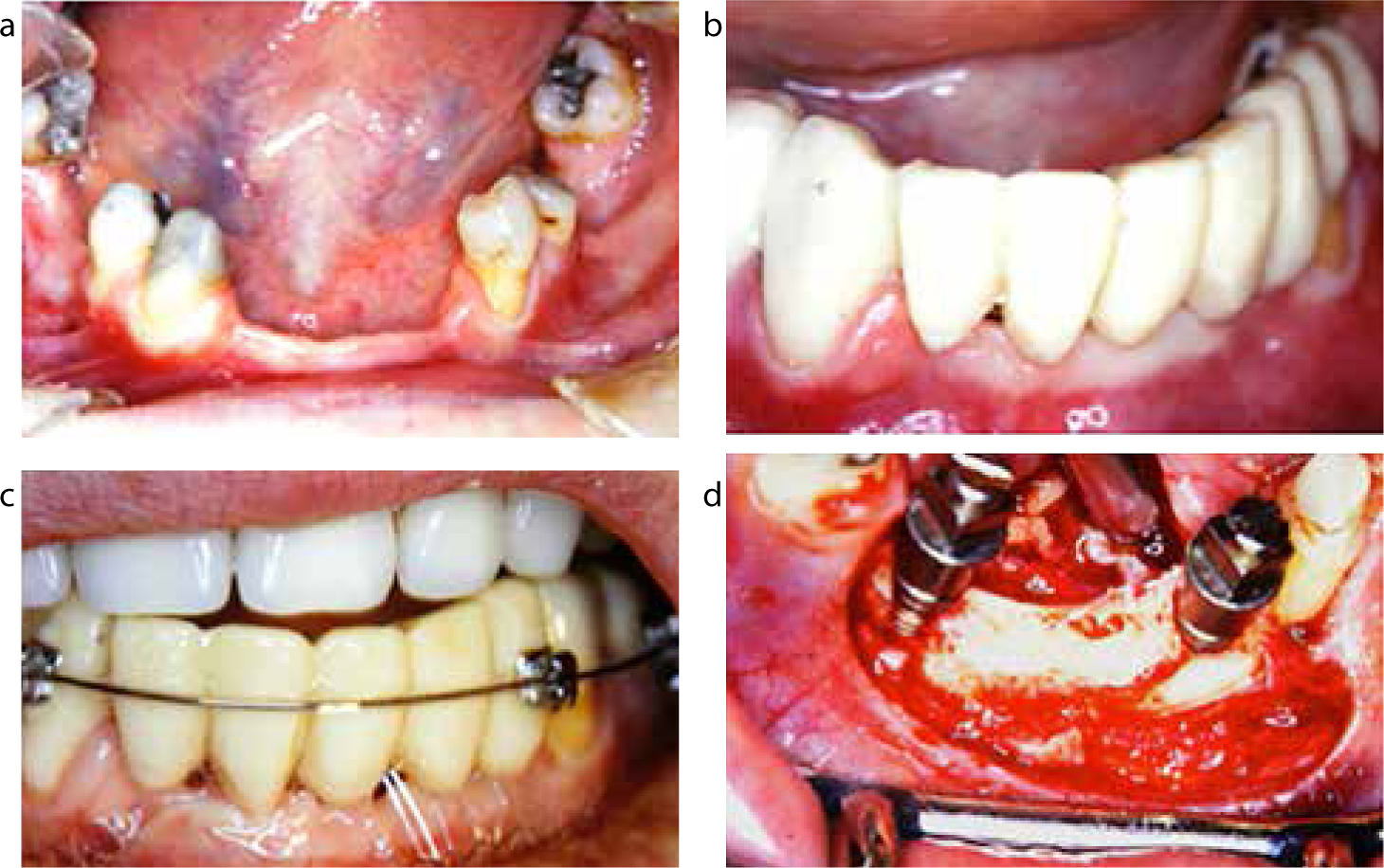
(a–d) Case A: Seven remaining lower teeth, including bilateral tipped molars. There was advanced ridge resorption in the posterior mandible which precluded the placement of posterior implants.Figure 2.
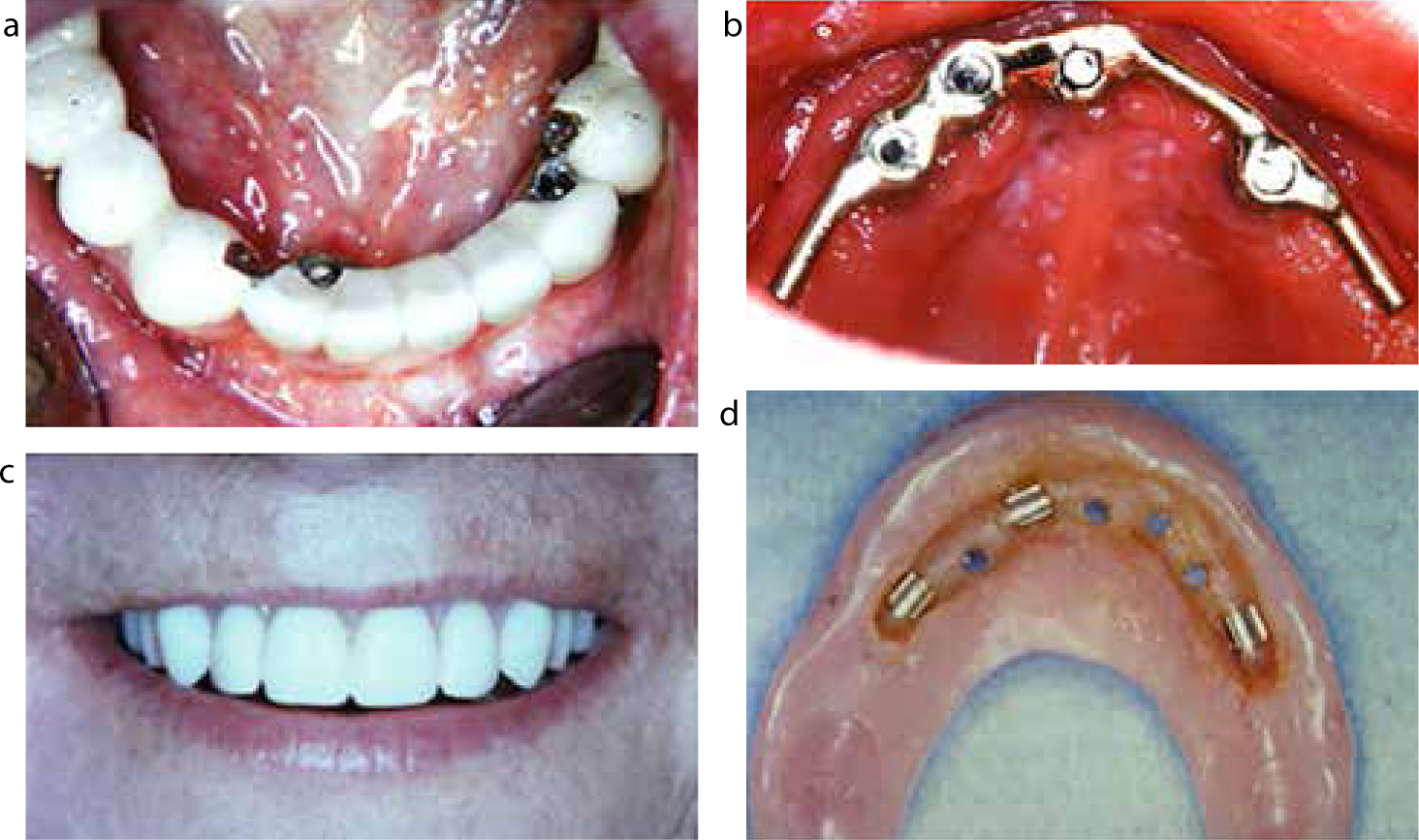
(a–d) Case A: Final restorations: mandible – anterior implant bridge and posterior tooth-supported bridges with distal telescopes; maxilla – bar-supported overdenture.
Case A illustrates two of these circumstances. The patient was a single, female lawyer, aged 39, who travelled over 200 miles for each visit. She had an edentulous maxilla and only 7 remaining lower teeth, including bilateral tipped molars. There was advanced ridge resorption in the posterior mandible which precluded the placement of posterior implants. She could not cope with a lower partial denture and her upper denture was getting more loose. At the time of treatment (1992–1994), the all-on-4 approach had not been proposed and the focus was on retaining as many teeth as possible. Hence the treatment plan proposed and accepted was to provisionalize LL5 to LR4 and use this for anchorage to upright the lower molars (by her local orthodontist); during orthodontics to place 2 anterior mandibular and 4 maxillary implants eventually to support a lower anterior fixed bridge and maxillary bar-supported overdenture, and to place 2 posterior mandibular bridges, with telescopic crowns on the molars, once these were uprighted. Anticipated treatment time was 12–16 months.
Treatment went largely as planned. One mandibular implant had a localized infection after placement but this responded well to treatment. It became clear, however, that the patient was manifesting many of the signs of Burnout outlined above. She became less communicative and no longer maintained regular eye contact; she pressed for earlier completion of treatment; she was unhappy about travelling in the winter. Eventually, we asked her ‘You're getting tired of this, aren't you?’ She agreed that she was and, as orthodontics was virtually completed, we suggested ‘How about if we gave you the winter off? Things should be stable for a few months.’ ‘That would be fantastic; just till April would be good’.
After discussion it became apparent that, not only was the level of treatment far beyond any past experience, but she had also acquired a much heavier workload as her partner in law practice had been elected to high political office. She returned in the spring, back to her original self, and treatment was completed uneventfully. While the first warning sign could be anticipated, the change of circumstances would be impossible to predict.
Minimizing Patient Burnout
While it is clear that we cannot anticipate all potential factors leading to Burnout, these are certain basic rules to minimize its occurrence.
Avoid inaccurate communications
Timeframe
Do not promise completion within a tight timeframe and, where practical, outline in writing a likely range of time for the duration of treatment. Better to say that treatment is likely to take 6 to 8 months and finish in 7 months, than to say it will take 6 months and take 7 months.
Outline the possibility of delays
Hence, in written communication,… ‘If all goes well, treatment is likely to take 6 to 8 months’.
Explain risks as well as benefits
Generally, there is a risk of around 20% that a crowned tooth will need root canal treatment, or a risk of around 5% that any implant may not be successful. These can be preceded in a letter by an introduction such as, ‘You should be aware that…’
Ensure that estimates include possible additional costs
For example, in root canal treatment it is better to estimate high and come in under estimate than the reverse.
Ensure that you discuss all reasonable options
To address the patient's needs as well as wishes, always include the do nothing option, and advise the patient of the likely costs, prognosis and duration of each option.
Tell the truth
Don't be drawn into discussions, or making excuses, as this can be prompted by questions such as…’Why didn't Dr Soandso tell me I had gum disease?’ The only true answer is ….’I really don't know. You would have to ask him that directly’. While your success rates for implant integration may be 98%, patients having one implant will have a rate of 100% or 0%. Tell them this since, if their implant fails, all the statistics in the world will not help their individual circumstance.
Writing to the patient
Outline all proposed treatment choices in writing using straightforward terminology. This should explain risks, benefits, all common or significant potential complications and a clear explanation of likely costs, timeframe and need for patient compliance. There is no better response to the patient who says ‘…I didn't realize…’ than to show them your copy of the letter they received prior to agreeing to treatment. It is fundamental to proper consent that the patient has not only had all options explained, but has had time to consider them before commencing treatment. A more detailed review of all aspects of communicating with the patient are to be found in Bain 2003.5
Keep talking throughout treatment
David Ausubel, a prominent educationist, advocated the use of an Advanced Organizer prior to a lecture or seminar.6 Basically, tell the students what you are going to discuss; discuss it then, on completion, review key points and tell them what you will discuss next time.
In the same way, at each appointment remind the patient of what is planned and get consent; carry it out; tell them what has been done and advise them of any variances, then, briefly review what will be done next time. Questions should be encouraged at every stage.
Too often dentists will do all of the talking up front to sell a complex treatment plan, then barely communicate on the so-called ‘treatment’ visits. ‘Open wide’ is not a suitable opening line.
Do not go too fast
There is a risk in taking an inexperienced patient too rapidly from only emergency or basic care to ‘advanced’ care. Just as you would not expect someone who has only experienced a pushbike to cope with a Ferrari, we are best to take the inexperienced patient gradually towards more complex care. In addition to minimizing potential Burnout, this will allow better assessment of oral hygiene and dietary improvements, as well as compliance with recommended recall and maintenance appointments. Sadly, financial motivation will, on occasion, put rapid treatment ahead of slower more controlled care.
Undersell and over-deliver (with help if necessary)
It is a basic tenet of any business to be able to deliver what they sell, and yet dentistry has many ‘Selling Coaches’ but few ‘Delivery Coaches’. Hoover UK went under, with years of legal cases because they ‘sold’ free holidays with a certain spend on their appliances, but were unable to deliver what they had promised. Much Dental Burnout can be traced back to dentists getting in beyond their skill level with complex treatment plans, with resulting stress from legal or GDC investigations. In no way should dentists only ‘swim at the shallow end’, but should also learn there before venturing to the ‘deep end’. Working with colleagues with more experience and training is not only better for the patient in many situations, but can provide a one-on-one mentoring experience for the less experienced clinician. The patient who has been oversold a promised result which does not materialize, or does not last (see Case B) is a likely candidate for Burnout, as disappointment is compounded by often painful complications and a growing resentment at being misled by a supposed expert.
KISS (Keep It Simple Stupid)
Dennis Tarnow, former Professor and Chairman of Periodontics and Implant Dentistry at NYU, repeatedly advocates this approach to complex implant dentistry. Often dentists over-complicate a treatment plan by using all of the tricks that can be delivered when a simpler approach would be just as satisfactory. Case A, if it was to be treated today, would likely do as well, or better, with an All-on-4 or 5 approach, sacrificing the remaining lower teeth and avoiding orthodontics. At many meetings one author (C Bain) sees multiple surgical procedures used in an attempt to augment an edentulous ridge vertically, when pink porcelain or acrylic can achieve an often faster and generally better aesthetic result with no surgery and certainly no risk of sloughing or black triangles.
Simple, however, should never be misinterpreted, and a simplistic approach used, which omits essential phases of treatment, such as achieving periodontal health, good oral hygiene and allowing adequate healing time before proceeding to the final restorations. Most dentists have seen patients who have had progressive anterior spacing and flaring of teeth treated by wider veneers or crowns, without periodontal management of the establishment of a stable posterior occlusion.
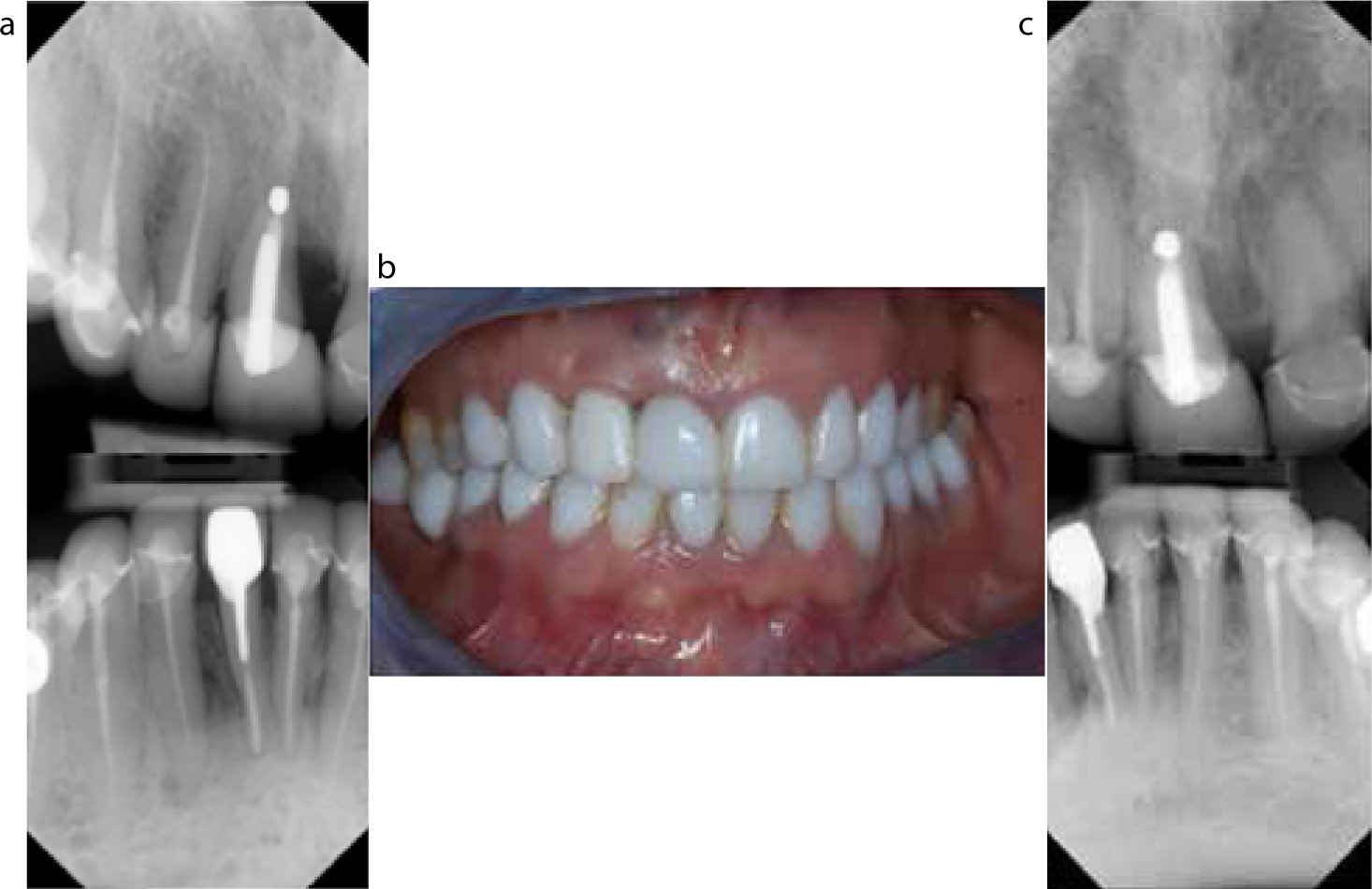
Figure 3.
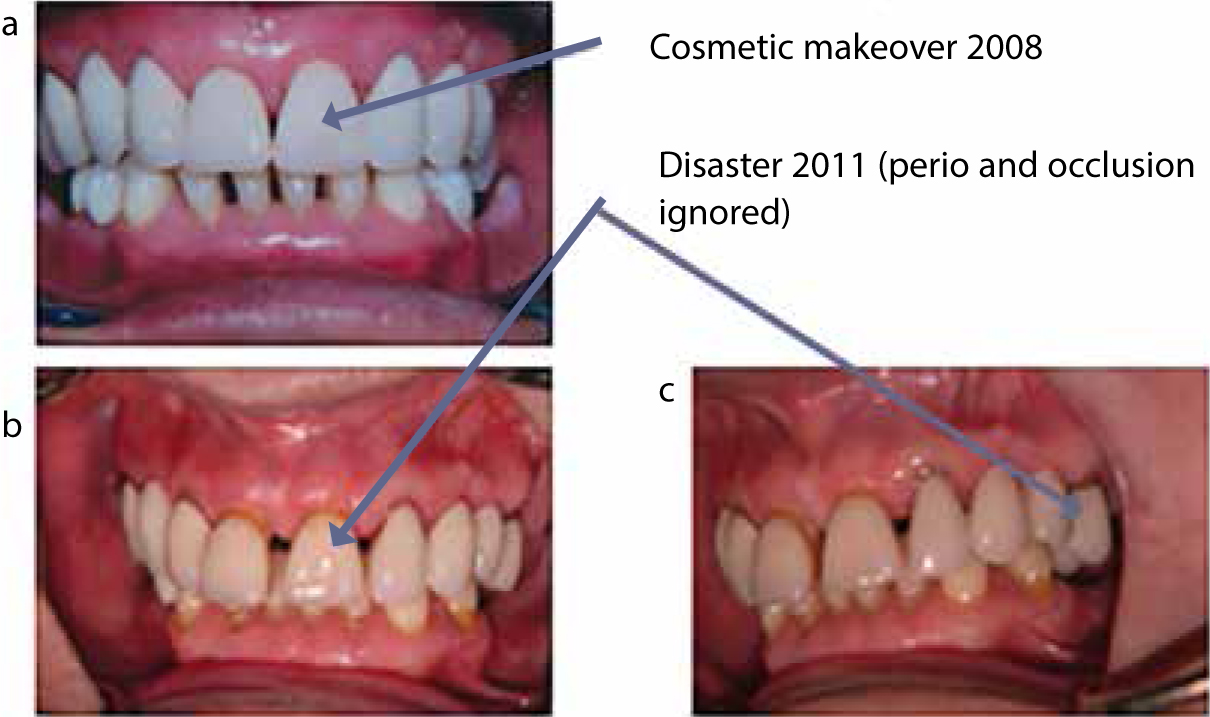
(a–c) Case B: Increasing anterior spaces due to advancing periodontitis and lack of a stable posterior occlusion. Treated by wide metal/ceramic restorations with no consideration of periodontal or occlusal problems.
This case sadly resulted in a legal case when increasing anterior spaces due to advancing periodontitis and lack of a stable posterior occlusion were treated by an ‘expert cosmetic’ dentist, with wide veneers and a bizarre occlusion on a bridge supported by an over-erupted tooth. When seen for a medico-legal report, the patient was totally exasperated (‘I wish I had never started’), having been told that she would have ‘a perfect smile’ and, within 3 years, being told by a dental hospital consultant that she would lose all her upper teeth.
Dentists also see implant patients receiving ‘Teeth in a Day’, often followed by final ceramic restorations ‘Within a week’. When, a few months later, gaps open up under pontics and shrinkage reveals the metal of implants, it is often the next, retreating dentist, who finds the new patient already Burntout, already financially compromised and certainly disillusioned. They present a significant management challenge.
Lack of empathy
For the first time around 25 years ago, one author (C Bain) experienced dental students, learning to give local anaesthetic, who had never had a dental injection themselves. While this is a testament to effective prevention, it makes it difficult for younger dentists to relate to the treatment they plan to provide to patients with complex problems. Equally, having treated many dentists as patients, one author (C Bain) knows that most, about to receive a palatal injection, will tense up since they know that there is likely to be discomfort. Dentists must never lose sight of the fact that they are often asking patients to undergo many long and potentially uncomfortable appointments. The dental chairside assistant's hand gently placed on the patient's arm at difficult points in treatment, together with communication by the dentist of concern for their comfort, will minimize the likelihood of Burnout.
Figure 4.
(a–d) Case C: After major trauma, treatment included a costochondral (rib) graft to replace the condyle, several implant and multiple root canal treatments and crowns. She had over 50 appointments in 3 years and happily a satisfactory result was achieved.
This patient was involved in a life-changing car accident in which she lost multiple teeth and fractured many others. She also had a complex jaw fracture and lost one condyle and significant alveolar bone. Treatment included a costochondral (rib) graft to replace the condyle, several implants and multiple root canal treatments and crowns. She had over 50 appointments in 3 years and happily a satisfactory result was achieved. On completion, she looked at her teeth in the hand mirror, smiled and said ‘If I ever have two more children I am going to call them…’. The author's (C Bain) immediate thought was that the endodontist and he would be honoured and perpetuated in her family. ‘I'm going to call them Pelton and Crane!’. When asked why, she said that it was the name on one author's dental light, which she had stared at for three years. She did not visibly Burnout during her treatment, but taught one author (C Bain) a valuable lesson in humility and an appreciation of what patients can often be asked to go through.
Listen to the patient
Some patients will communicate their growing Emotional Exhaustion using a few of the expressions outlined above. If Burnout appears to be developing and the situation is relatively stable it may be wiser to give patients some time off, rather than try to persuade them towards rapid completion.
Figure 5.
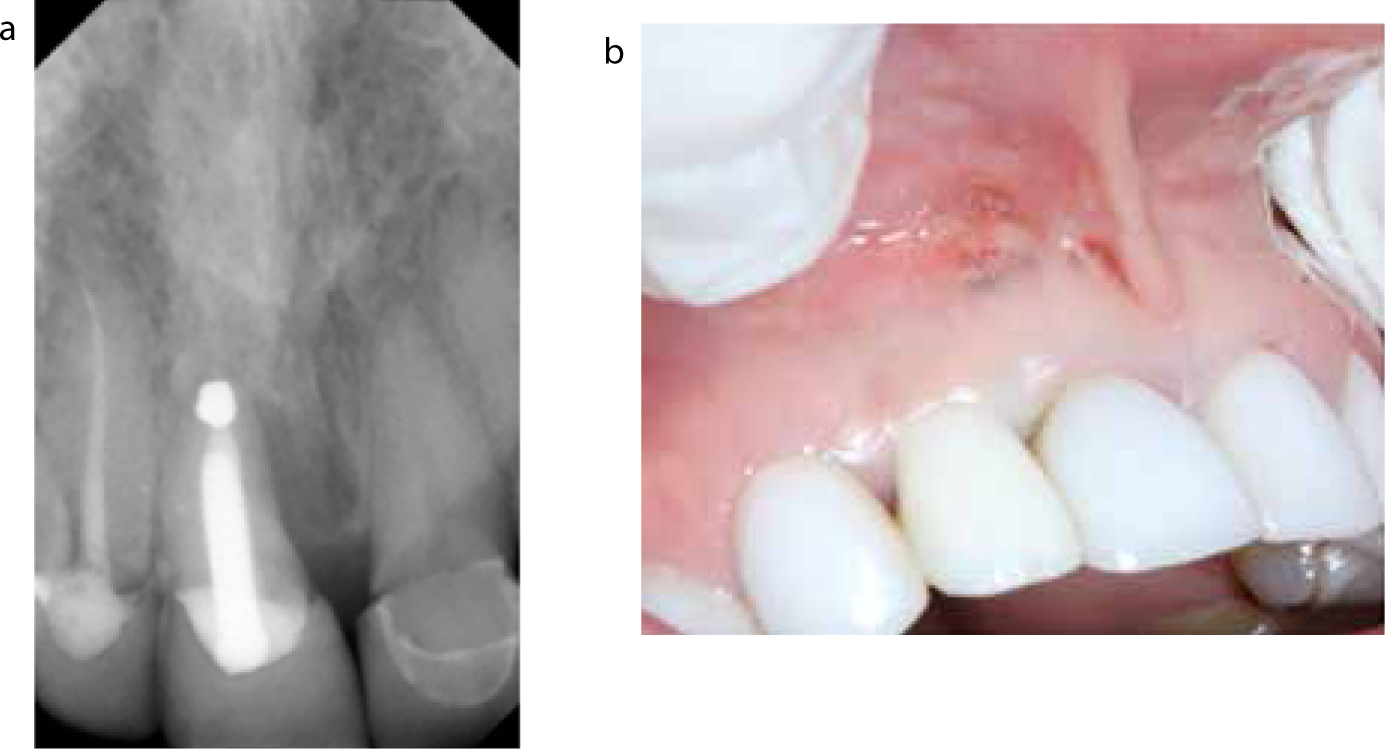
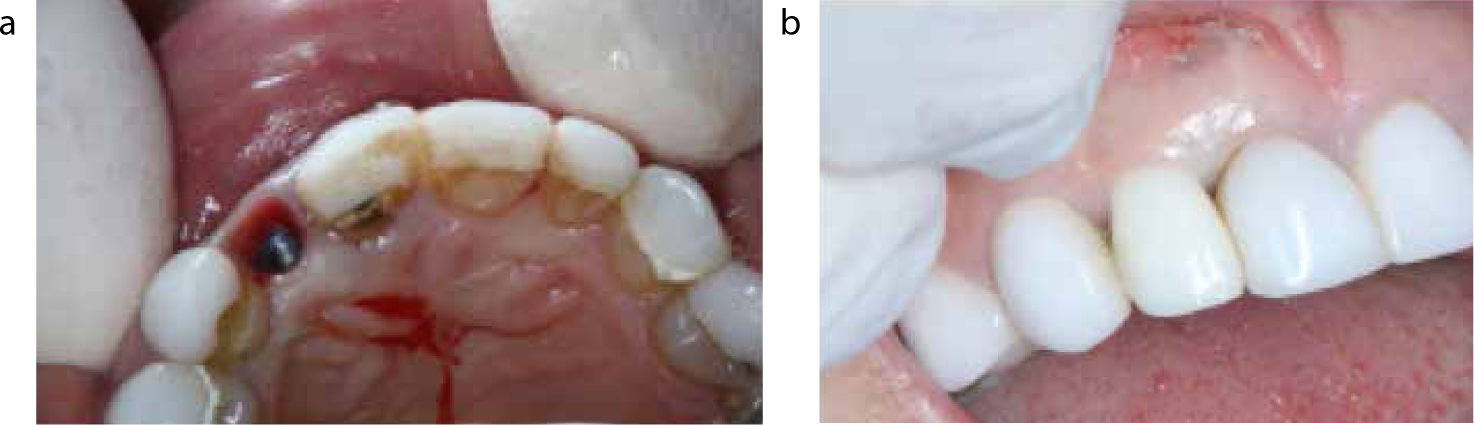
(a–c) Case D: Patient presented with multiple failing veneer and root fillings. Tooth UR1 was deemed hopeless and implant replacement advised.Figure 6.
(a, b) Case D: There was intermittent recurring drainage from UR1 but the patient had no pain. Because of the lack of a labial plate, a delayed implant was planned.Figure 7.
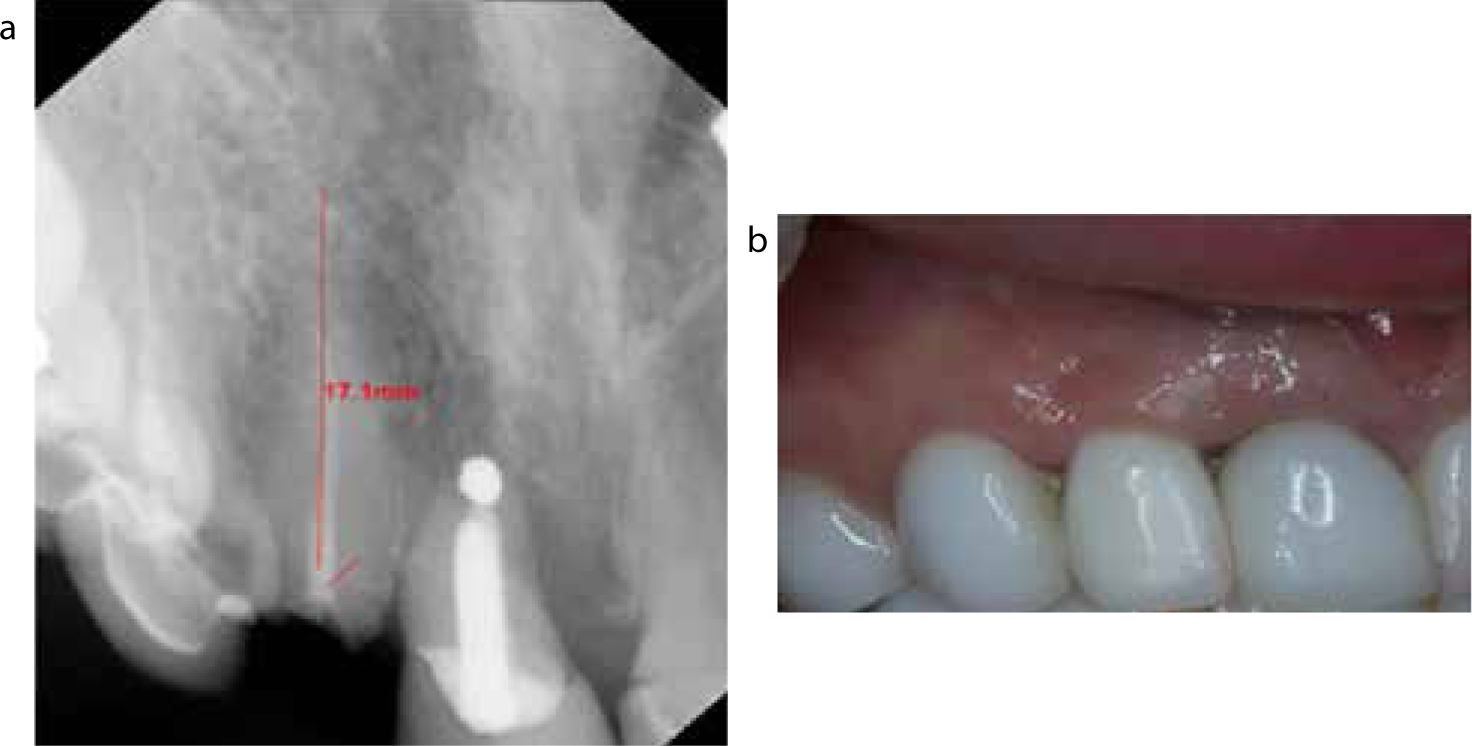
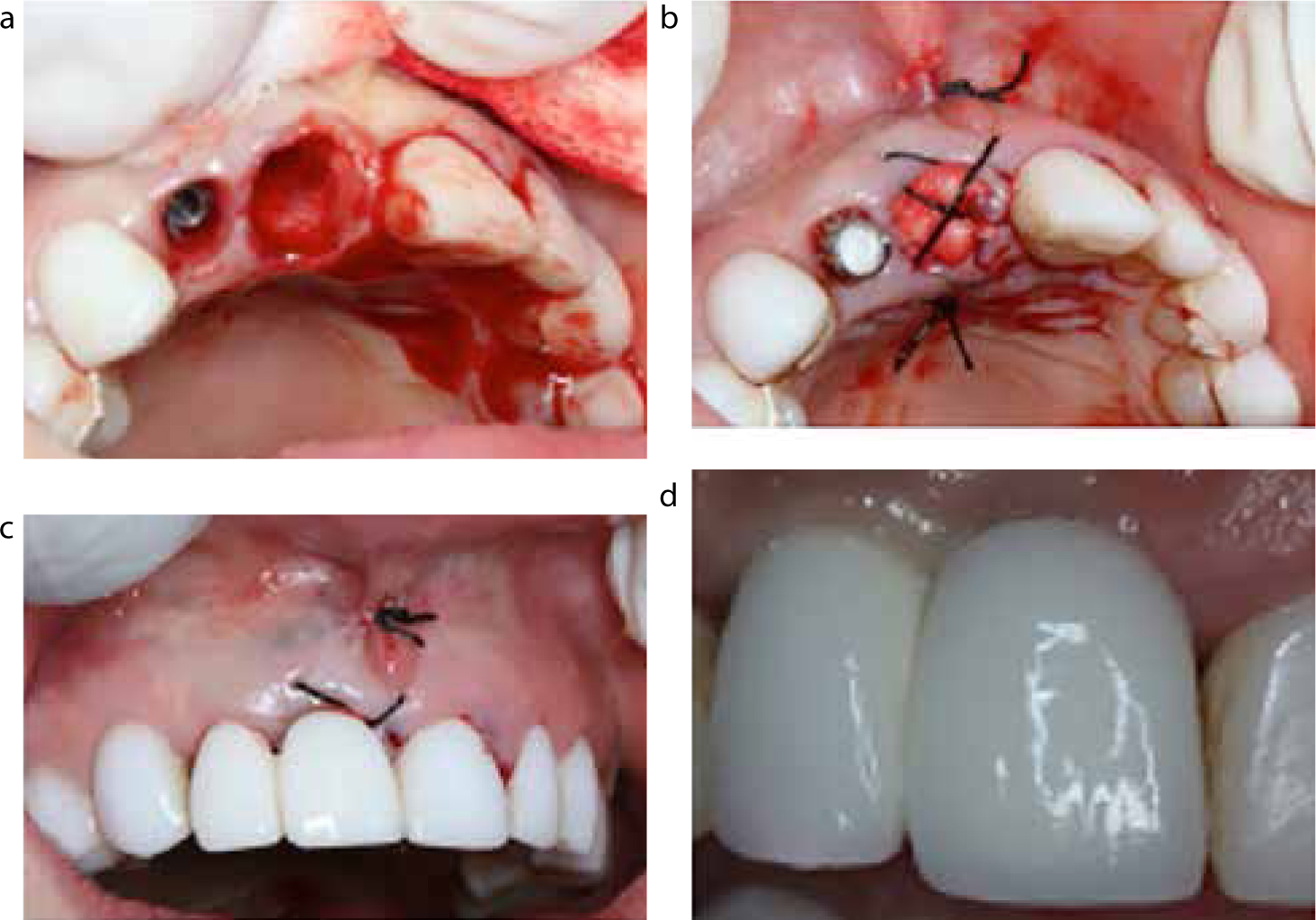
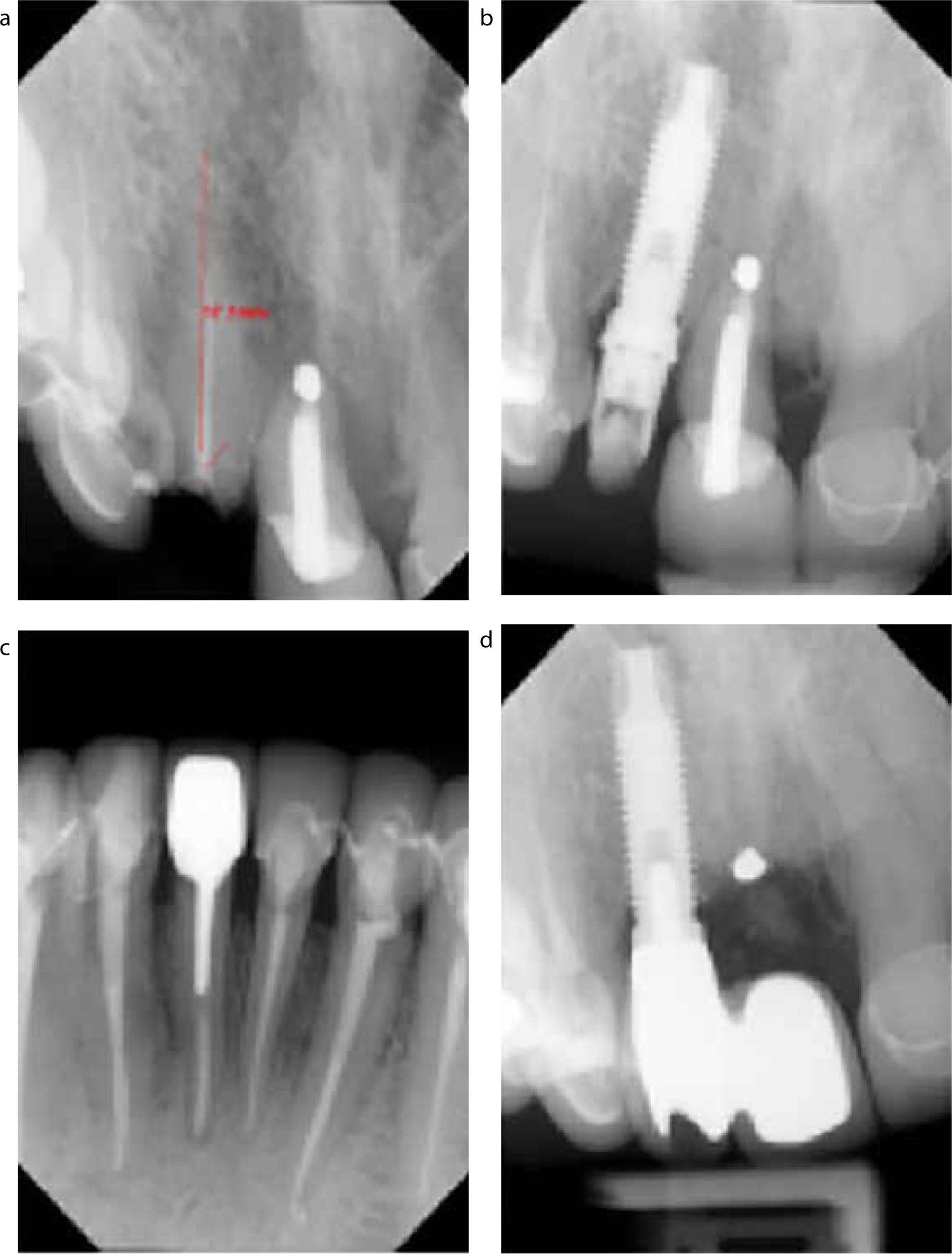
(a, b) Case D: Because UR2 fractured within the Biologic Width the plan was changed so that an immediate implant was placed in the UR2 site and, after integration, the UR1 was to be removed and a cantilever temporary fitted during socket healing followed by the final bridge.Figure 8.
(a, b) Case D: Although the site had developed well with the temporary, and UR1 continued to drain, the patient stated that she had ‘had enough for now’ and was in no pain and since she manifested several signs of Burnout and was stable, we gave her 6 months off before the next phase.Figure 9.
(a–d) Case D: After 6 months the treatment was resumed and completed uneventfully. The patient was very grateful for the ‘time off’.Figure 10.
(a–d) Case D: UR2 fractured sub-gingivally and was non-restorable. The plan was revised to place an immediate implant in the UR2 site to cantilever UR1. Due to Patient Burnout, extraction of UR1 was delayed by 6 months.
This 47-year-old female had an extensive upper and lower ‘Smile Makeover’ completed in a few weeks. Unfortunately, this was completed on top of suboptimal endodontics on several teeth and a likely root fracture on tooth UR1, which had previously had an apicectomy. At presentation, several restorations had required re-cementation and tooth UR1 and 3 lower incisors were tender to percussion. Tooth UR1 was assessed as having a hopeless prognosis and implant replacement was planned. The patient embarked on extensive endodontic retreatment in advance of implant and restorative care. During this preparatory treatment, UR2 fractured within the Biologic Width and the treatment plan was changed so that an immediate implant was placed in the UR2 site and, after integration, the UR1 was to be removed and a cantilever temporary fitted during socket heal, followed by the final bridge. Once integration of UR2 was confirmed, the removal of UR1 could proceed, however, the patient stated that she had ‘had enough for now’ and was in no pain. Since she manifested several signs of Burnout and was stable, she was given 6 months off before the next phase. When she returned, treatment was completed without incident.
Conclusions
This article has introduced the concept of Patient Burnout in Dentistry and has proposed some common diagnostic signs and symptoms manifest in this condition. Some preventive and management approaches for patients, who show the potential for developing, or are diagnosed with this condition, were recommended.
In the previous article, the authors discussed the Burnout phenomenon in dentists, and proposed the possible relationship whereby, managing a number of patients who are experiencing Burnout, may precipitate the condition in dentists. It seems likely that early identification and management of potential Patient Burnout could reduce the likelihood of the dentist developing this problem.