European Markets for Dental Implants, Final A butment and Computer Guided Surgery.Vancouver, BC: iData Research iNC2013;
Setzer FC, Kim S. Comparison of long-term survival of implants and endodontically treated teeth. J Dent Res. 2014; 93:19-26
Simonis P, Dufour T, Tenenbaum H. Long-term implant survival and success: a 10–16-year follow-up of non-submerged dental implants. Clin Oral Implants Res. 2010; 21:772-777
Pjetursson BE, Karoussis I, Bürgin W, Brägger U, Lang NP. Patients' satisfaction following implant therapy. Clin Oral Implants Res. 2005; 16:185-193
Papaspyridakos P, Chen C-J, Singh M, Weber H-P, Gallucci G. Success criteria in implant dentistry: a systematic review. J Dent Res. 2012; 91:242-248
Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants. 1986; 1:11-25
Consensus report of session IV. Proceedings of the First European Workshop on Periodontology. 1994;
Guckes AD, Scurria MS, Shugars DA. A conceptual framework for understanding outcomes of oral implant therapy. J Prosthet Dent. 1996; 75:633-639
Levi A, Psoter WJ, Agar JR, Reisine ST, Taylor TD. Patient self-reported satisfaction with maxillary anterior dental implant treatment. Int J Oral Maxillofac Implants. 2003; 18:113-120
Mills I. Person-centred approach to holistc assessment.: Holistic Patient Assessment in Dentistry; 2017
Bertakis KD, Azari R. Determinants and outcomes of patient-centred care. Patient Educ Couns. 2011; 85:46-52
Froum SJ. Dental Implant Complications: Etiology, Prevention, and Treatment.London: John Wiley & Sons; 2015
Sugerman PB, Barber MT. Patient selection for endosseous dental implants: oral and systemic considerations. Int J Oral Maxillofac Implants. 2002; 17:191-201
Zitzmann NU, Margolin MD, Filippi A, Weiger R, Krastl G. Patient assessment and diagnosis in implant treatment. Aust Dent J. 2008; 53:S3-10
Diz P, Scully C, Sanz M. Dental implants in the medically compromised patient. J Dent. 2013; 41:195-206
Bornstein MM, Cionca N, Mombelli A. Systemic conditions and treatments as risks for implant therapy. Int J Oral Maxillofac Implants. 2009; 24:12-27
Addy L, Korszun A, Jagger R. Dental implant treatment for patients with psychiatric disorders. Eur J Prosthodont Rest Dent. 2006; 14:90-92
Tanner T. Treatment planning for dental implants: considerations, indications, and contraindications. Dent Update. 1997; 24:253-260
Crisp A. Every family in the land.London: The Royal Society; 2004
Brown S, Greenwood M, Meechan JG. General medicine and surgery for dental practitioners. Part 5 – psychiatry. Br Dent J. 2010; 209:11-16
Lewer D, O'Reilly C, Mojtabai R, Evans-Lacko S. Antidepressant use in 27 European countries. Br J Psych. 2015; 207:221-226
Prescriptions Dispensed in the Community (England 2005–2015).London2016
Clinical Examination and Record Keeping; Good Practice Guidelines.London: FGDP (UK); 2016
Manwell LA, Barbic SP, Roberts K, Durisko Z, Lee C, Ware E What is mental health? Evidence towards a new definition from a mixed methods multidisciplinary international survey. BMJ Open. 2015; 5
NHS Five Year Forward View, 2014.London: HMSO; 2014
Mental Health Services: Achieving Better Access by 2020.London2014
Milgrom P, Newton JT, Boyle C, Heaton LJ, Donaldson N. The effects of dental anxiety and irregular attendance on referral for dental treatment under sedation within the National Health Service in London. Community Dent Oral Epidemiol. 2010; 38:453-459
Newton T, Asimakopoulou K, Daly B, Scambler S, Scott S. The management of dental anxiety: time for a sense of proportion?. Br Dent J. 2012; 213:271-274
Fundamental Facts about Mental Health 2016.London2016
Corrigan PW, Druss BG, Perlick DA. The impact of mental illness stigma on seeking and participating in mental health care. Psychol Sci Public Interest. 2014; 15:37-70
Professor of Oral Surgery, King's College London; Honorary Consultant in Oral Surgery, King's College Hospital NHS Foundation Trust and Guy's and St Thomas' NHS Foundation Trust, London
Until recently, dentists were not trained in psychology and access to education in psychiatry and mental health remained limited within the dental curriculum. A major obstacle for integrating mental health initiatives into primary healthcare services is the lack of consensus on a definition of mental health. Currently, there is widespread use of the term ‘mental health’ as a euphemism for ‘mental illness’. Mental health can be defined as the absence of mental disease, or it can be defined as a state of being that also includes the biological, psychological or social factors which contribute to an individual's mental state and ability to function within the environment. This lack of consensus on the definition of mental health has implications for research, policy and practice.
Mental health issues will impact significantly upon many aspects of patients' health, including: seeking care, presentation, compliance with treatment and providing additional complexities in delivering routine care. Significant issues can arise in relation to routine care but, as dental procedures become more complex in their delivery and maintenance, the impact of undiagnosed mental health issues are likely to increase in prevalence and impact not only on individual patients but also their treating clinicians.
CPD/Clinical Relevance: This case report provides an account of a case where early identification of the patient's mental health status may have prevented significant post-treatment sequelae.
Article
Dental implants are widely acknowledged as an important treatment modality in the restoration of the failing or missing dentition. In that regard, there has been a considerable increase in the number of dental implants placed over the last 30 years with over four million implant fixtures placed annually in Europe.1 Success rates for implant treatment can vary widely,2 but are frequently reported as between 90% and 97% based on 5-year survival data.3 It is well documented that the level of implant success reported is dependent on the assessment criteria used.4 This can be highly variable, with the nature of the success criteria having a significant influence on the results reported.5
Success criteria for dental implants were previously aligned to survival rate, with assessment based on prosthesis stability, radiographic bone loss, and absence of infection in the peri-implant soft tissues.6 The importance of restorability, soft tissue aesthetics and patient satisfaction have since been acknowledged as key factors in the assessment of success.7
Inclusion of patient satisfaction demonstrates an appreciation of the importance of patient-reported outcomes in assessing the quality of care provided. This supports a move away from the biomedical measure of success that focuses on the technical outcome of treatment, and instead indicates a more patient-centred approach.4 Guckes et al8 recognized the importance of patient-centred outcomes and published a classification of implant success. This included consideration of the physiological and psychological impact of implant treatment. Levi et al9 highlighted the importance of patient-reported outcome measures in implant dentistry and suggested that patient satisfaction with overall treatment should be rated good or excellent for the treatment outcome to be considered successful.
Various factors have been identified in relation to the successful outcome of implant therapy. Bone density, primary implant stability, history of smoking, periodontal disease, and certain systemic conditions can all influence the predictability of implant treatment.5 Holistic assessment is a critical aspect in implant success and is absolutely key in identifying risk factors and supporting patients in making an informed decision about treatment. The factors detailed above predominantly relate to the technical outcome of treatment and do not necessarily take into consideration the patient's expectations. This is an important aspect of case selection as failure to identify and manage patient expectations can result in treatment failure, irrespective of the technical outcome.
Successful management of patient expectations is dependent on obtaining a thorough history, which should include the nature of the presenting complaint, history of the presenting complaint, and details of the patient's desired outcome. A patient-centred approach to holistic assessment is key in identifying the patient's needs and wishes10 and this has been reported to improve patient-reported outcomes and reduce complaints and litigation.11 In other words, the more time that is spent identifying the patient's expectations, the better the chance there is of meeting or exceeding them. The medical, dental and social histories are integral components of this assessment stage and provide important information, which is highly relevant in case selection. Holistic assessment of the dental patient involves understanding the needs of the individual and this includes physical, psychological, sociological and spiritual wellbeing of that person.10
Psychiatric disorders are common and diverse (Table 1) and have previously been suggested as a contra-indication to implant treatment,12 although the nature and severity of the condition should be taken into consideration. Sugerman and Barber13 state that ‘severe psychiatric disease’ should be considered a contra-indication to implant therapy, but do not offer any details on what this would include, or how the severity of the condition should be assessed. Zitzmann et al14 suggest that ‘severe psychosis’ should be considered an absolute contra-indication, and ‘depression’ a relative contra-indication. No further advice or information is provided on assessing the nature or severity of such conditions. This lack of information is recognized by Diz et al,15 who highlight the sparse and contradictory evidence that is currently available in assessing the risk of implant treatment in patients who have a history of mental health issues. Bornstein et al16 reported that there was no published evidence which assessed the risk of implant therapy in patients with a history of neuro-psychiatric disorders. Addy et al17 reported a series of three cases who were treated successfully with implant treatment.
Common Types of Mental Health Problem
Possible Symptoms
Overall
Change in appearance
Poor self-care
Withdrawal
Panic attacks
Self-harm
Suicidal feelings
Psychotic experiences may include:
delusions, such as paranoia
hallucinations, such as hearing voices
Depression
Feelings:
down, upset or tearful
restless, agitated or irritable
guilty, worthless and down on yourself
empty and numb
isolated and unable to relate to other people
finding no pleasure in life or things you usually enjoy
a sense of unreality
no self-confidence or self-esteem
hopeless and despairing
suicidal
Behaviour:
avoiding social events and activities you usually enjoy
self-harming or suicidal behaviour
finding it difficult to speak or think clearly
losing interest in sex
difficulty in remembering or concentrating on things
using more tobacco, alcohol or other drugs than usual
difficulty sleeping, or sleeping too much
feeling tired all the time
no appetite and losing weight, or eating too much and gaining weight
physical aches and pains with no obvious physical cause
moving very slowly, or being restless and agitated
Anxiety
Feeling restless
Being agitated
Struggling to sleep and eat
Body Dysmorphic Disorders (BDD)
Experience obsessive worries about one or more perceived flaws in your physical appearance; the flaw cannot be seen by others or appears very slight
Develop compulsive behaviours and routines, such as excessive use of mirrors or picking your skin, to deal with the worries you have about the way you look
If you have BDD, these obsessions and behaviours cause emotional distress and have a significant impact on your ability to carry on with your day-to-day life. In this way, BDD is closely related to obsessive-compulsive disorder (OCD)
Obsessive-Compulsive Disorder (OCD)
Obsessions are unwelcome thoughts, images, urges, worries or doubts that repeatedly appear in your mind. They can make you feel very anxious (although some people describe it as ‘mental discomfort’ rather than anxiety).
Compulsions are repetitive activities that you do to reduce the anxiety caused by the obsession. It could be something like repeatedly checking a door is locked, repeating a specific phrase in your head or checking how your body feels.
Phobias
Most common phobia is that of dental treatment
The fear is out of proportion to the danger
It lasts for more than six months
It has a significant impact on how you live your day-to-day life
Eating Problems
An eating problem is any kind of relationship with food that you are finding difficult
Anorexia, bulimia
Bipolar Disorder
Manic or hypomanic episodes (feeling high)
Depressive episodes (feeling low)
Potentially some psychotic symptoms during manic or depressed episodes
Schizophrenia
A lack of interest in things
Feeling disconnected from your feelings
Difficulty concentrating
Wanting to avoid people
Hallucinations, such as hearing voices or seeing things others don't
Delusions (which could include paranoid delusions) – strong beliefs that others don't share
Disorganized thinking and speech
Not wanting to look after yourself
Personality Disorders
You feel very worried about people abandoning you, and would do anything to stop that happening
You have very intense emotions that last from a few hours to a few days and can change quickly (for example, from feeling very happy and confident in the morning to feeling low and sad in the afternoon)
You don't have a strong sense of who you are, and it can change depending on who you're with
You find it very hard to make and keep stable relationships
You act impulsively and do things that could harm you (such as binge eating, using drugs or driving dangerously)
You have suicidal thoughts or self-harming behaviour
You feel empty and lonely a lot of the time
You get very angry, and struggle to control your anger
When very stressed, sometimes you might:
feel paranoid
have psychotic experiences, such as seeing or hearing things other people don't
feel numb or ‘checked out’ and not remember things properly after they've happened
Five of these symptoms are needed to be given the diagnosis of PD
Tanner considers ‘a history of mental disorders’ as an absolute contra-indication to implant treatment, and relates this to an inability to have realistic expectations.18 Addy et al also highlight the importance of managing patient expectations but suggest that, if a patient's suitability is in question, a psychiatric opinion should be sought.17 It is clear from the literature that psychiatric disorders need to be taken into consideration as a risk factor, but that the risk is more likely to be related to patient-reported outcomes than implant survival.
This paper uses a single case report to highlight the importance of undertaking a thorough pre-operative assessment to include an adequate medical history which includes exploration of mental health issues. The case illustrates the risks involved in treating a patient with a history of mental illness and the dichotomy that can exist between the technical outcome and the patient's view of success.
Case report
A 55-year-old female was referred by her general dental practitioner to a private implant referral clinic. The patient presented with catastrophic failure of an existing 4-unit bridge that was replacing UL1, UL2, UL3, UL4. Her primary concern was loss of the bridge and she declared that her reason for attending was ‘they (the teeth on the bridge) were falling out’. She was adamant that she did not want to wear a denture and was anxious to proceed with treatment as soon as possible as she had two family weddings later that year. The patient declared that she was ‘very unhappy’ about her smile and rated this as a 2 on a scale of 1 to 10, (with 10 being excellent) (Figures 1 and 2).
Figure 1. Smile at initial presentation.Figure 2. Teeth at initial presentation.
No relevant medical history was declared, although the patient indicated that she was anxious about dental treatment. Despite her anxiety she had managed to cope with some advanced and complex dental treatment in the past under local analgesia, including endodontics, bridge preparation and tooth extraction. In answering the question ‘how do you feel about going to the dentist?’ she responded ‘terrified, but needs must’.
Clinical and radiographic examination (Figure 3) revealed that the abutment teeth (UL1/UL3) were in a compromised state and beyond restoration. Examination also revealed that an existing 3-unit bridge on the upper right was severely compromised, with secondary caries undermining the distal bridge abutment and apical areas associated with the post-retained bridge abutment (UR4) and the upper right second molar (UR7). The patient was informed of this and provided with a detailed treatment plan including various treatment options. She was advised to return to her own GDP to discuss management of the bridge on the upper right.
Figure 3. Intra-oral radiographs at initial presentation.
Following further discussion between the patient and her own dentist a decision was made to sacrifice the bridge on the upper right at the same time as the bridge on the upper left, with an immediate acrylic partial denture being provided. A treatment plan was subsequently formulated based on replacement of the missing teeth with a fixed implant solution to a reduced dental arch, and the patient returned to her own dentist for extraction of the failing teeth and provision of an immediate partial denture.
A post-extraction review was arranged in order to assess healing and complete the final diagnostic stages, including CBCT imaging. At that stage, the patient described how she had found the extractions a particularly difficult experience. As a consequence, she requested that implant surgery be conducted with intra-venous sedation. At the post-extraction review appointment, the patient also mentioned that she had been having headaches since the extractions and that she felt that her head shape had changed. At that stage she was advised to contact her GP should the symptoms persist.
Implant treatment was uneventful from a technical perspective, and healing proceeded normally. At subsequent appointments, the patient became increasingly anxious about treatment and, shortly after the fitting of her provisional implant-retained bridge, she returned feeling very low and negative about a number of aspects about her treatment. At a review two months later, the patient explained that she had experienced a number of mental health issues over the Christmas period, but was now feeling better and insisted that she wished to complete treatment as soon as possible.
Fitting of the final bridge was uneventful and the patient appeared delighted with the final result (Figures 4 and 5). Advice regarding oral health maintenance was provided and the patient was discharged back to her own dentist, with provision made for a review appointment one year later.
Figure 4. Smile following completion of treatment.Figure 5. Completed treatment.
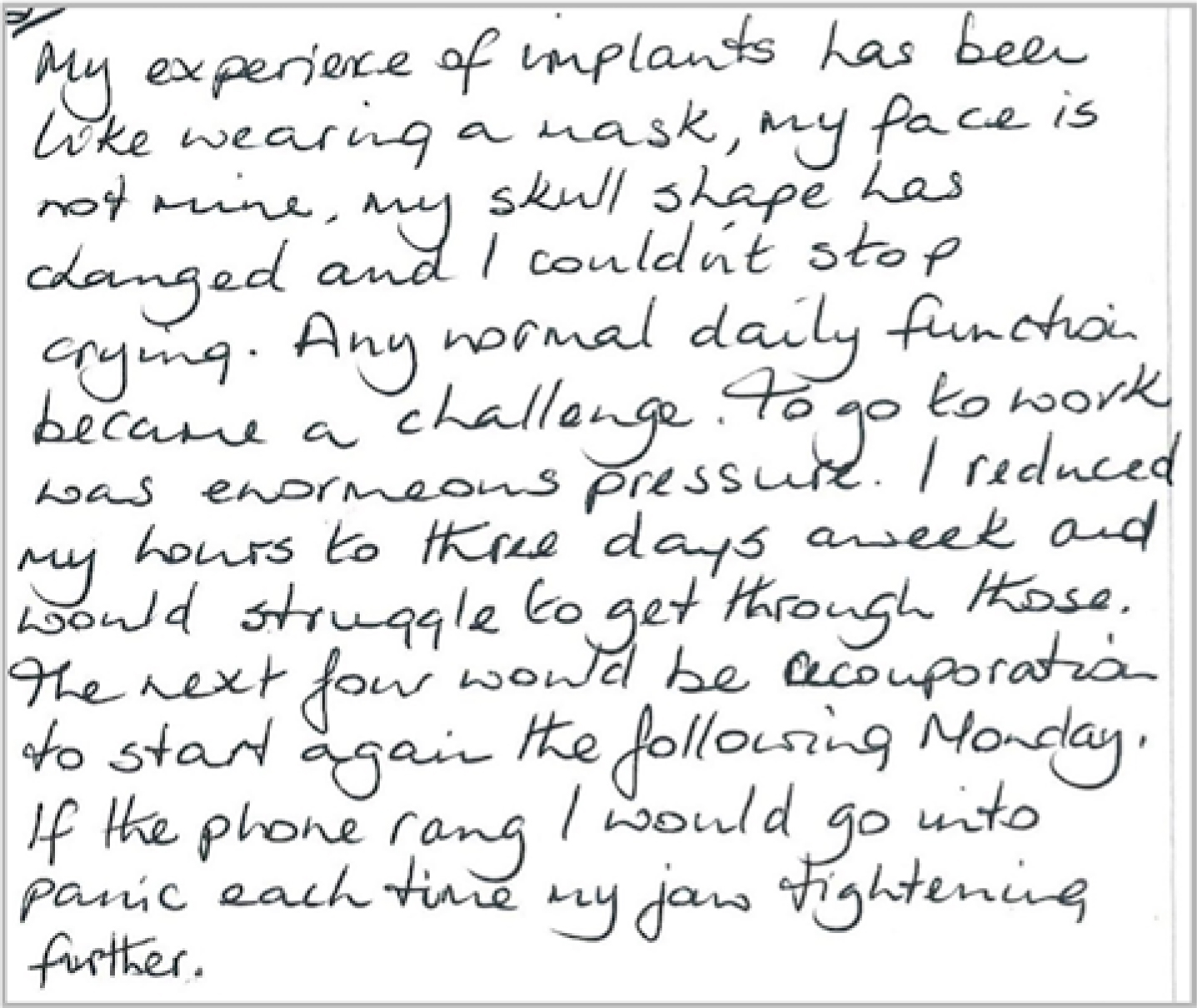
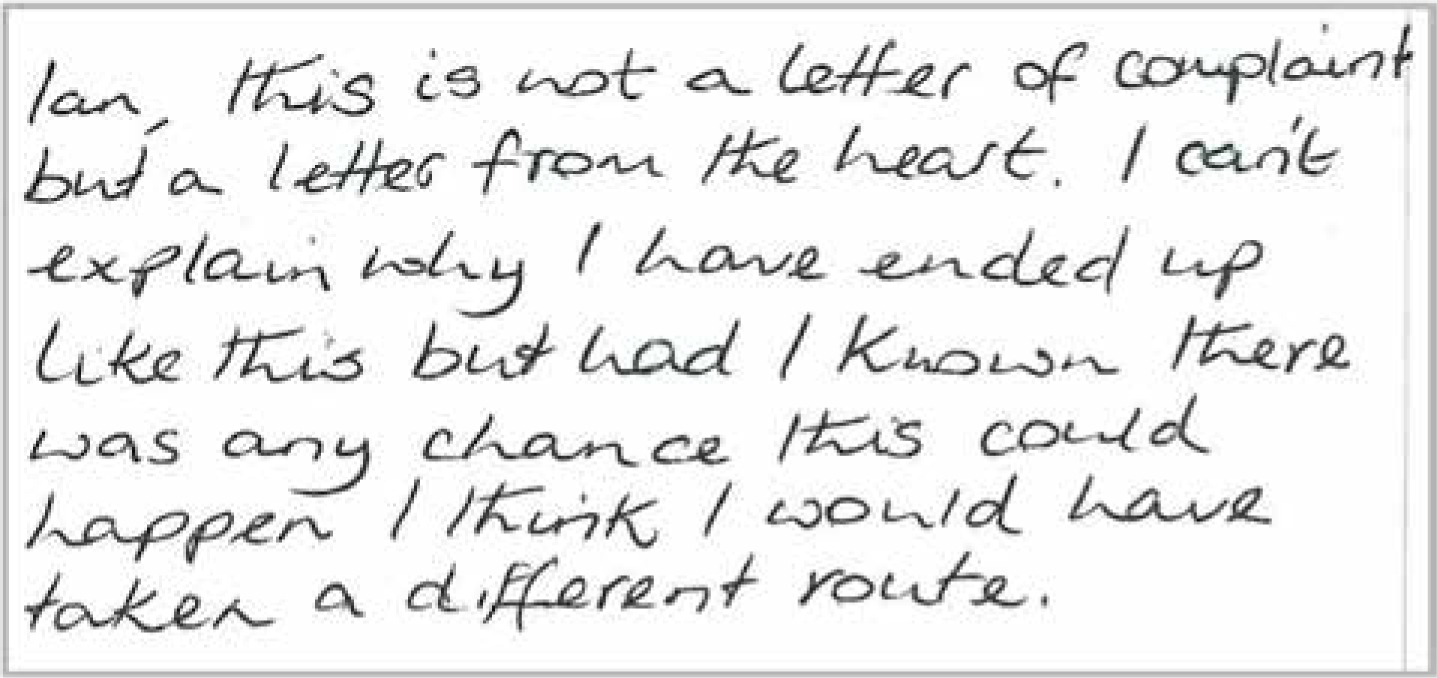
Three months after fitting the final bridge, a letter was received from the patient explaining in considerable detail the psychological difficulties that she had faced in coming to terms with the new bridge (Figure 6).
Figure 6. Letter received from patient.
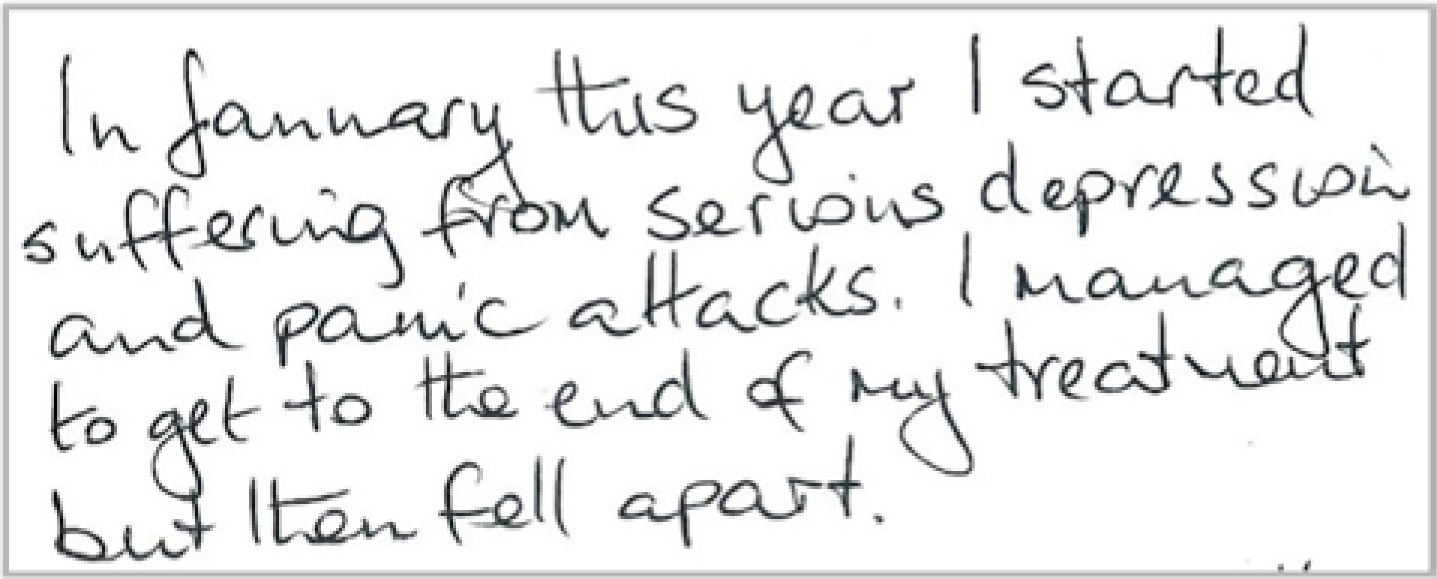
The patient explained that she had been suffering from depression during the course of implant treatment, and this had got steadily worse over the preceding months (Figure 7). The patient felt that the cause of her depression was related to the loss of her teeth and the subsequent course of complex restorative care.
Figure 7. Letter received from patient.
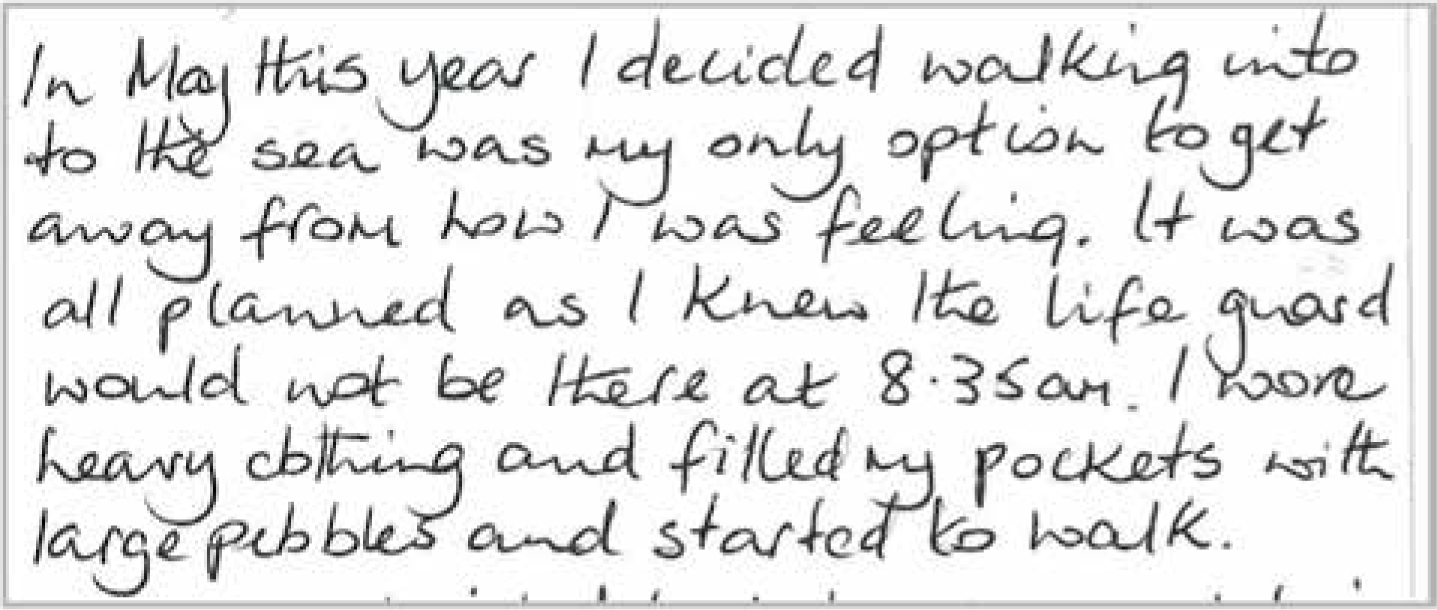
Following completion of the implant treatment, the depressive state became steadily worse, culminating in an attempted suicide by drowning (Figure 8).
Figure 8. Letter received from patient.
Fortunately, the patient did not follow through with her planned suicide and was stopped by her dog barking on the beach. She was subsequently able to find help and is in the process of piecing her life back together with professional support and the care of her family and friends. Sadly, the situation has placed an incredible strain on the patient and her family, and she has lost her job as a consequence. The experience has resulted in a significant increase in her level of dental anxiety, but she is managing to address this with the support of her own dentist.
Discussion
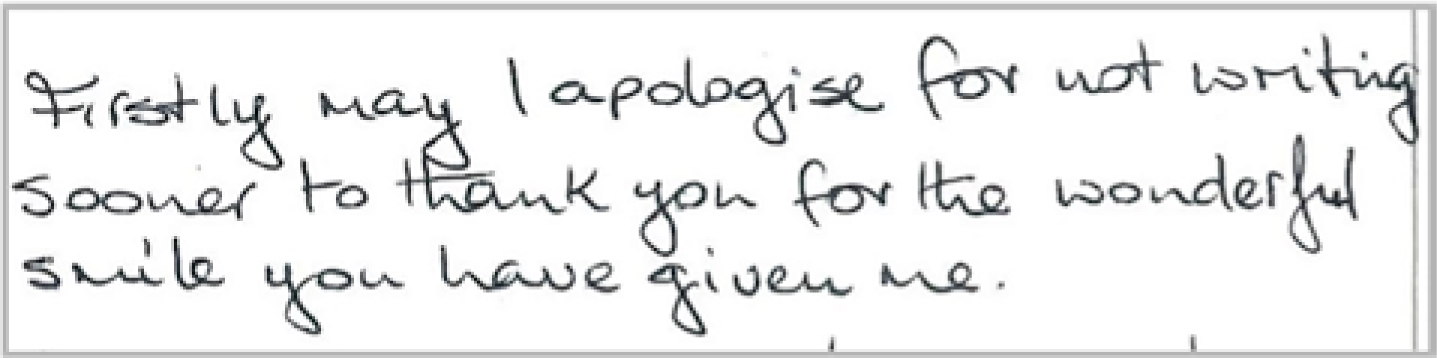
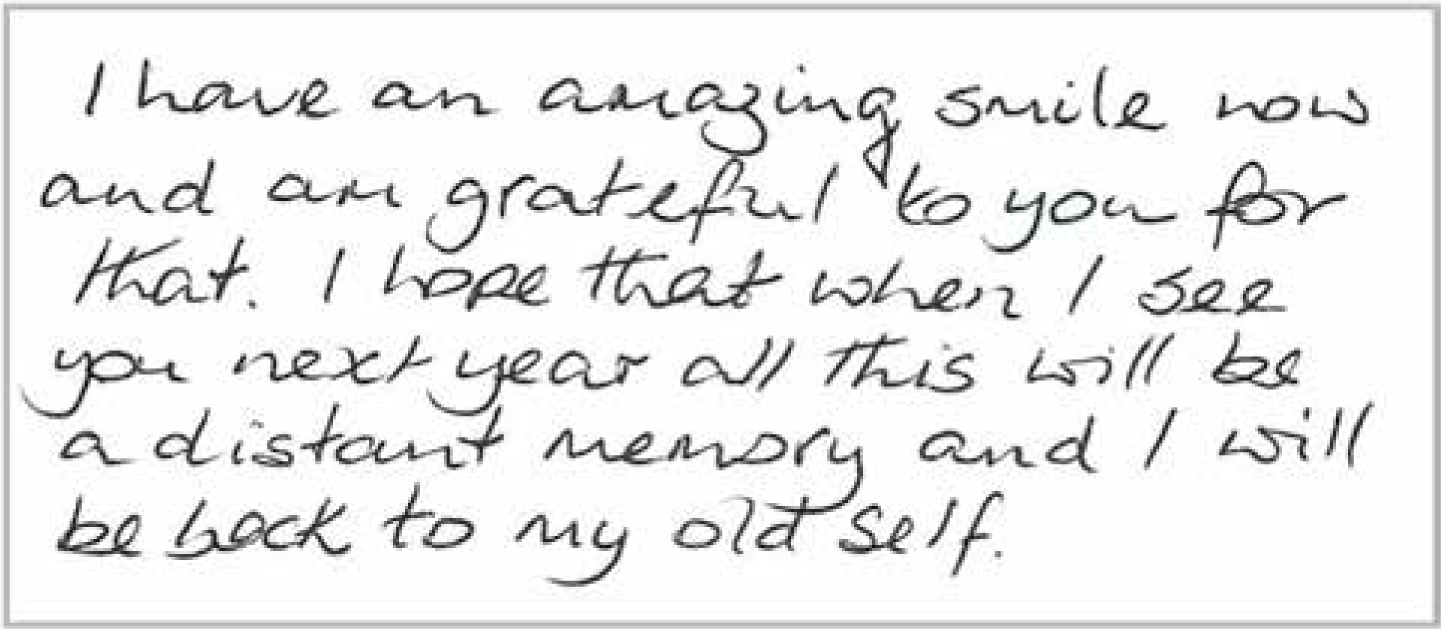
This case history presents a number of discussion points, which are worthy of further consideration. The final treatment has been a technical success and has provided the patient with an aesthetic and functional dentition. The original presenting complaints were addressed successfully and the patient expressed genuine appreciation for the result achieved (Figure 9). In many ways this treatment could be considered a success.
Figure 9. Letter received from patient.
However, the dental treatment provided has had a significant adverse impact on the life of that individual, and of those around her. The patient states in her letter, that if she had been aware of the potential consequences beforehand, she would not have proceeded with implant treatment (Figure 10). This is clearly a sad and upsetting situation and, irrespective of the technical result, the clinician failed to meet the patient's expectations, and treatment must therefore be considered a failure.
Figure 10. Letter received from patient.
The experience has also had a profound impact on the implant dentist involved and this has led him to reflect on how this could have been handled differently in order to avoid such a potentially catastrophic outcome.
Psychiatric illness or mental health conditions have previously been considered as a potential contra-indication in implant treatment.12 The challenge is assessing what patients are at risk, and what is that risk. It is estimated that 25% of the UK population will suffer from a mental health condition at some stage in the course of their lives.19 Psychiatric disorders are common and a significant proportion of patients attending for dental treatment will be affected. There is a wide range of conditions classified as psychiatric disorders and these include anxiety, depression, eating disorders and schizophrenia.20
Depression is particularly common, and affects up to 20% of women and 10% of men at some stage in their lives.20 The use of antidepressants is widespread and it is reported that 9% of adults in the UK are currently being prescribed such medication.21 This has been steadily increasing and it is estimated that there has been a 20% increase in the use of antidepressants between 2000 and 2010.21 A recent report published by the Health and Social Care Information Centre (HSCIC) reveals that the number of antidepressant items prescribed and dispensed in England has more than doubled in the last decade.22
It is therefore clear that a large number of patients attending for dental treatment will have a history of depression, with a significant number being treated with antidepressant therapy. Patients on antidepressant drugs will be readily identified from a routine medical history, such as that recommended by the Faculty of General Dental Practice (UK).23 It is important to understand the reasons why patients take these drugs, how long they have been taking them for and whether there have been any recent changes. People with mental health problems frequently feel stigmatized and there is often an unwillingness to discuss the condition openly. This is likely to be reflected in the dental environment where neither patient nor clinician is likely to discuss mental health issues with the same level of openness as they might hypertension or diabetes. This can lead to reluctance to explore mental health issues in detail, which can potentially be a risk.
In this particular case, the patient was not taking any antidepressants and there was no disclosure of mental illness on the medical history form. On reflection, the potential failings within this case appear to be related to three specific factors:
Failure to identify a previous mental health history;
Failure to acknowledge any mental health risk associated with the treatment;
Failure to recognize the signs and symptoms of clinical depression and refer appropriately.
Identification
The routine medical history commonly used in the UK will not necessarily identify patients who have previously had mental health issues. The British Dental Association (BDA) and Faculty of General Dental Practice (UK) medical history proformas do not include a specific question on mental health. In the case reported within this paper, the patient completed a medical history form which was then validated orally by the clinician. The patient was not taking any medication and did not divulge any history of mental health problems in the past. At a subsequent stage of treatment, when the patient showed signs of depression, she revealed that she had previously experienced post-natal depression (PND) which had been severe and prolonged. There was no recent history of depression, but such information may have had a bearing on subsequent discussions, treatment planning and the level of support provided.
Identification of a current or previous mental health history must be seen as a key aspect in taking an effective history and it would therefore seem appropriate to include a specific question relating to mental health within a medical questionnaire. The authors would suggest that the following question would be considered appropriate:
Have you experienced any mental health issues in the past which have required you to seek advice from a healthcare professional?
Manwell et al (2015) proposed a Transdomain Model of Health, which is helpful in thinking through the interplay between physical, psychological and social factors for an individual patient. Further papers exploring this interplay with specific reference to dental patients are proposed by the authors.24
Risk assessment
An affirmative answer to such a question is likely to be of limited value unless additional information is obtained. As previously stated, approximately one quarter of all adults may be in a position to answer ‘yes’ to this question, yet this is likely to have little impact on decisions about their dental treatment or any subsequent outcome. It is therefore necessary to obtain additional information to allow an effective assessment of risk to be made.
Public Health England is focused on making mental health a priority,25,26 and general dental services could be instrumental in helping to break down the artificial barriers between mental and physical health. Routine dental procedures can be extremely traumatic for certain individuals and anxiety is recognized as a key reason for patients failing to return for treatment.27,28 Some psychological preparation, eg by a dental nurse, could aid and support attendance in addition to identifying vulnerable individuals who may be at risk.
The IMPARTS data collected at King's College Hospital suggests that 20–25% of patients are experiencing mental health difficulties.28 A series of questionnaires enables patients to be classified as low, medium or high distress. Pathways are in place for referral onto Liaison Psychiatry or Clinical Psychology as appropriate. This model of care could be applied to general dental practice with very little additional burden to the dental team. The CORE-10 is a screening measure which could potentially be used in practice and this is explored in a subsequent paper.29
Recognition of signs and appropriate referral
The patient in this case study reported specific symptoms following extraction of her teeth. These included severe headaches, a change in the shape of her skull and an awareness of a ridge on the apex of her cranium. This information was reported at a pre-operative implant review, but little additional information was sought concerning her general wellbeing or psychological state. The patient was simply advised to seek advice from her GP as the symptoms were not considered relevant at that time.
At this stage, the history of PND had not been disclosed and the symptoms were not considered to be suggestive of deterioration in the patient's mental health, nor were they seen as a contra-indication to implant treatment. A change in the patient mood during treatment had been evident, although this was simply considered to be a result of her underlying dental anxiety which had been exacerbated by her recent experience of tooth extraction.
Symptoms of depression are variable and wide ranging, but can include:
Feeling sad or ‘empty’;
Feeling hopeless, irritable, anxious, or guilty;
Aches or pains, headaches, cramps, or digestive problems;
Thoughts of death or suicide.
These symptoms were present at the time of the pre-operative implant assessment but were not identified as such, and no risk assessment was made. If these symptoms had been recognized and a risk was considered to be present, appropriate referral should have been actioned with the patient's consent.30
The patient subsequently explained that she had found the initial extractions and loss of the upper bridgework particularly traumatic, and she considered this to be the trigger for the deterioration in her mental health. The level of anxiety and depression gradually increased during the course of her implant treatment and the patient viewed this as being a highly stressful period which had contributed to her decline and subsequent attempted suicide.
If any staff member or patient expresses suicidal tendencies or attempts, this is a notifiable event and the dental team is obligated to ensure that the patient is followed up appropriately (Table 2).
A number of scenarios may arise in dental practice:
▪ New presentation of psychiatric illness – such patients should be encouraged to speak to their general medical practitioner (GMP) about whatever symptoms have been noticed. It is not necessary to suggest it may be due to psychiatric illness
▪ Deterioration of existing illness – these patients should be asked to speak to their GMP or existing psychiatric services
▪ Overt suicidal ideation (either as new or altered presentation) is a notifiable event and the dental team is obligated (CQC Duty of Candour Reg 20): such patients should be advised to speak to their GMP or go to A&E, or the on-call psychiatric services or police should be contacted directly
If the patient refuses then the dental team must contact:
– A member of their care team or the centre or clinic where patient was treated.
– If you don't have these details, contact your nearest accident and emergency (A&E) department and ask for the contact details of the nearest crisis resolution team (CRT). CRTs are teams of mental healthcare professionals, such as psychiatrists and psychiatric nurses, who work with people experiencing severe psychological and emotional distress
▪ Patient presenting an immediate danger to others – call the police
▪ You or a colleague need help – a GMP or A&E should be able to help, or contact the confidential Dentists' Health Support Programme
One year after treatment
At twelve month review, the implant treatment could be considered a success when viewed against Albrektsson et al's criteria.7 The clinical treatment had been provided to an acceptable standard and the patient declared that she was delighted with the result (Figure 11). However, the patient is still being treated for depression, has been unable to return to work and has high levels of dental anxiety. In terms of patient-reported outcome measures, this treatment cannot be considered to have been a success, based on patient experience or improved quality of life outcomes.
Figure 11. Letter received from patient.
Conclusions
This case report highlights a number of important issues:
Success of implant treatment cannot be assessed simply on the technical or clinical outcome;
Patient-reported outcomes are an important measure in the assessment of success;
Mental health can have a profound impact on patient-reported outcomes;
Clinicians can place their patients, and themselves, at significant risk by failing to obtain a comprehensive medical history which includes details relating to mental health.
These issues are not simply related to implant treatment and must be considered equally relevant to any aspect of dentistry. Mental health problems are common and a significant proportion of our patients will have a pre-existing condition, which may or may not have been diagnosed previously.29
A significant level of prejudice, discrimination and ignorance surrounds mental illness and, as a consequence, there is a reluctance to disclose or discuss such issues.30 Patients are concerned about how they will be viewed or judged; and individuals, including dentists, feel uncomfortable in discussing what they perceive to be a highly sensitive subject. As a consequence, mental health issues are often treated very differently from those of physical illness; there is an unwillingness to discuss or broach the subject. This is gradually changing as patients, clinicians and advocates try to inform, educate and break down the barriers which currently exist.
As healthcare professionals we need to lead this change by acknowledging the prevalence of mental illness in the population and the relevance which this has in providing care for our patients. We need to identify the patients at risk, assess the risks, and be able to offer support and advice as necessary. Failure to do so can have potential catastrophic consequences for all those involved.
This paper aims to highlight the importance of identifying patients at risk, and the potential consequences if this is ignored. In sharing this case report it is hoped that GDPs will pause and reflect on their own practice, and how they collect information about the mental health of their patients. The authors are conscious of the increasing healthcare responsibilities placed on general dental practitioners, particularly within the NHS, and appreciate that further recommendations or guidance may be viewed as a burden. We propose that inclusion of a simple additional question within the medical history form will be all that is required for 75–80% of all patients.
Additional information may need to be collected for the remaining 20–25% of patients who have a history of mental illness. In a subsequent paper, we will discuss a simple and practical approach which can be implemented within your practice to support these patients appropriately, while minimizing the impact on your practice. Such an approach will provide additional safeguarding for you and your patients, which will reduce the risk of an avoidable incident such as the one detailed in this case report.