Davies SJ, Gray RMJ, Whitehead SA. Good occlusal practice in advanced restorative dentistry. Br Dent J. 2001; 191:421-434
MacInnes A, Hall AF. Indications for cuspal coverage. Dent Update. 2016; 43:150-158
Ritter AV, Baratieri LN. Ceramic restorations for posterior teeth: guidelines for the clinician. J Esthet Dent. 1999; 11:72-86
Wirsching E, Loomans BA, Klaiber B, Dörfer CE. Influence of matrix systems on proximal contact tightness of 2- and 3-surface posterior composite restorations in vivo. J Dent. 2011; 39:386-390
Summit JB., Robins JW, Hilton HJ, Schwartz RS. Fundamentals of Operative Dentistry: A Contemporary Approach, 3rd edn. Chicago, US: Quintessence Publishing Co Ltd; 2006
This is the third, and final, part of this three-part series. The first paper discussed the occlusal and cracked tooth aetiological factors which may be responsible for restoration failure. The second paper discussed the restorative options with regards to cracked and root-treated teeth. This paper will provide an overview of the previous two papers and conclude with a case report.
CPD/Clinical Relevance: Failure of amalgam restorations is a commonly encountered clinical problem in general practice and no one case is the same. Therefore, a competent diagnosis and implementation of the most appropriate, minimally invasive treatment option requires an adequate knowledge of current literature.
Article
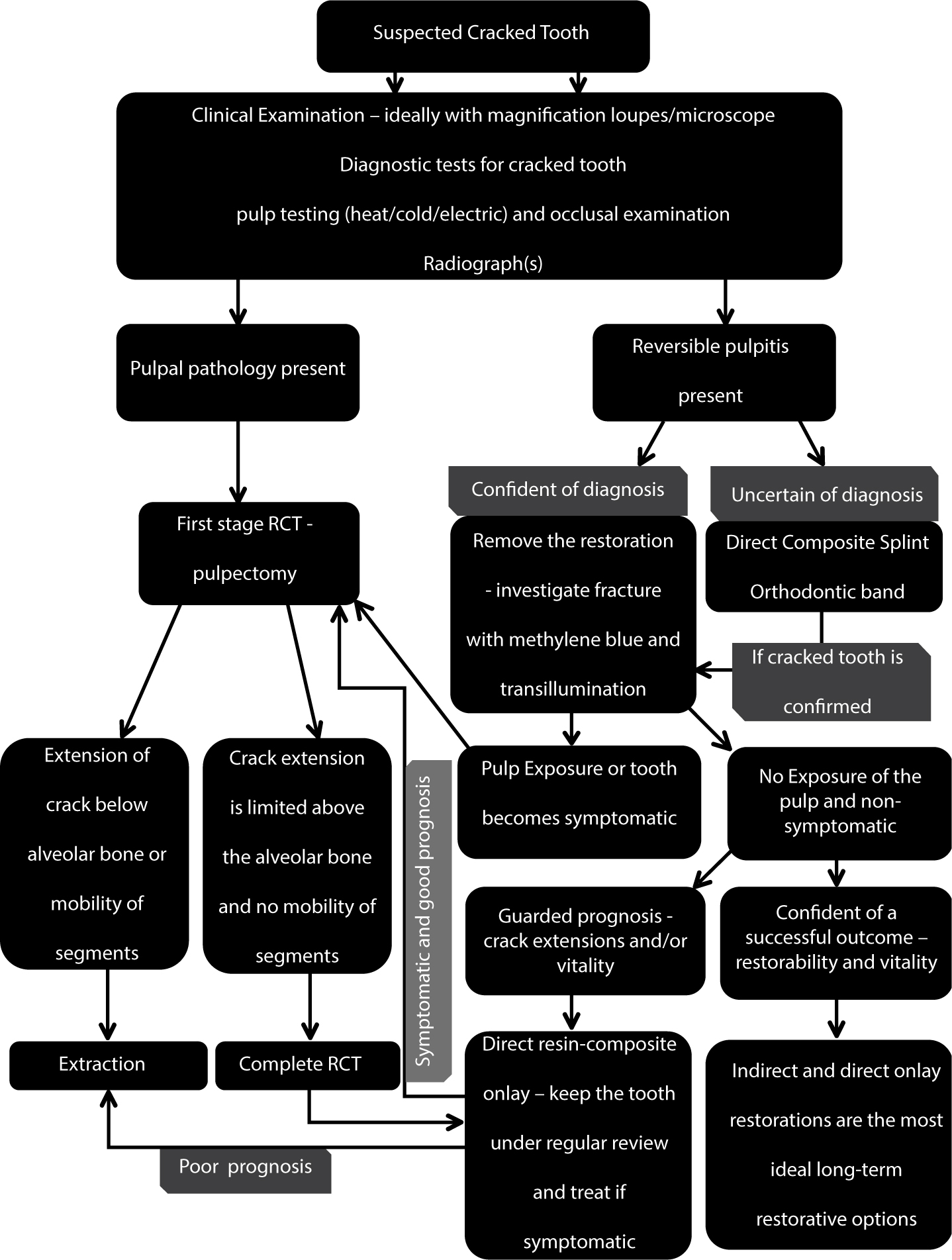
In the author's experience, clinicians usually find the area of cracked teeth confusing. Therefore, to help with this, a summary of the previous information discussed in the previous two papers has been provided in Figure 1. This flow chart aims to provide a logical, sequential approach when confronted with a cracked tooth. It is worth noting that the occlusal assessment takes place during the initial stages along with the normal clinical examination and pulp testing methods. It is important to consider occlusal trauma, endodontic pathology, chronic orofacial pain (eg atypical facial pain) and other dental pathologies (eg periodontal disease), as with the alternative aetiologies, without immediately assuming that there is a fracture within the tooth structure.
Figure 1. Cracked tooth approach.
Under specific circumstances, it may not be possible to diagnose each and every patient case at the first appointment. If the situation arises where there are doubts regarding the diagnoses, then the astute clinician will collect all the relevant clinical information at the initial visit and treat as he/she feels is most appropriate at the time of presentation, whilst being as conservative as possible. The following review appointment may confirm the provisional suspicion, or it will provide a new insight into the underlying cause. However, if there are any uncertainties with regards to the diagnosis, then the clinician should seek a second opinion from a suitably qualified colleague.
A patient case will now be presented which highlights some of the difficulties that the clinician may face when large restorations fail. The complexity of this case was further compounded by the fact that all the heavily restored teeth were on the same arch and adjacent to one another. The author aims to demonstrate the importance of a thorough understanding of the aetiological factors which can contribute to restoration failure; without this knowledge an accurate diagnosis can never be made. The most appropriate treatment approach and restorative options can then be considered, including any potential long-term complications which are anticipated in advance. This greatly enhances patient consent and avoids difficult conversations in the future if failure does occur.
Patient case
This was a medically fit and well 62-year-old female patient. She was complaining of symptoms from the lower right side, ‘somewhere’ at the back of the mouth, with extreme sensitivity to cold and heat lasting several minutes and tenderness during eating, with the occasional dull background ache. These symptoms had been fairly consistent and manageable over the past six months, but they had recently become more intense.
A diagnosis of dentine hypersensitivity was made by the previous clinician regarding the LR6. The patient had been given dietary advice, 1.1% sodium fluoride toothpaste (5000 ppm) and high strength fluoride varnish was placed over the exposed root surfaces. Unfortunately, none of these treatments successfully alleviated the patient's symptoms.
She had previously worked as a secretary for 25 years and was currently a part-time, self-employed local artist. She had a relatively non-stressful lifestyle, was a non-smoker and drank alcohol on very rare occasions.
The patient had been a regular attender to her previous dental practitioner, brushed twice per day with an electric toothbrush, using fluoride toothpaste, and flossed daily.
Acute apical periodontitis – this has most likely resulted from a leaking restoration, which ultimately led to a necrotic pulp over time.
LR6
Occlusal trauma with incomplete fractures on the buccal and lingual tooth surfaces – signs and symptoms of reversible pulpitis.
LR7
Cracked tooth – currently has signs and symptoms of reversible pulpitis. However, this tooth has a higher risk of endodontic treatment in future.
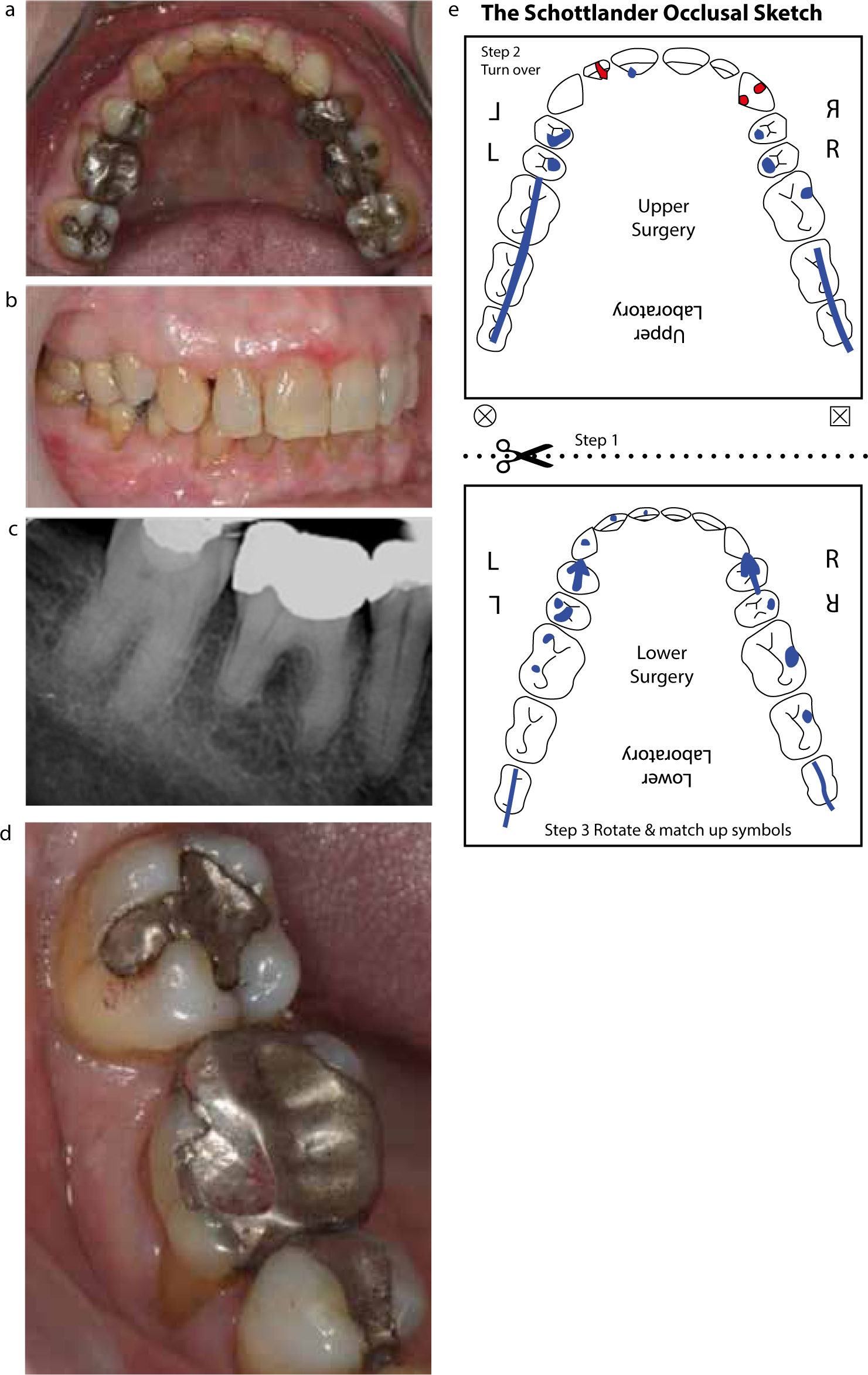
Heavily restored dentition on the lower arch (Figure 2a);
Adequate oral hygiene: calculus deposits were present on the lower anteriors;
Evidence of lichen planus which had been previously investigated and was being managed with topical steroids;
Upper and lower fixed orthodontic retainers were present – these were fitted post-orthodontic treatment which had been performed 15 years previously;
The patient occluded in centric relation, without any discernible RCP-ICP slide, and had even protrusive contacts on the upper central incisors;
No working or non-working side interferences were present;
No signs or symptoms of temporomandibular dysfunction;
The LR5 was tender to palpation, tender to percussion and no responses to heat, cold or electric pulp sensibility testing.
Figure 2. A heavily restored lower arch dentition (a). Right lateral view in ICP (b). Pre-operative peri-apical radiograph (c). Signs of occlusal trauma on mesio-buccal cusp of the LR6 with shimstock hold. Crack lines evident on the LR7 marginal ridges, including the buccal and lingual surfaces (d). Pre-operative ‘Occlusal Sketch’, blue represents ICP and red marks the excursive movements (e).
The LR6 had a wear facet present on the mesio-buccal cusp, enamel craze lines and extreme discomfort to cold. There was a broad rubbing contact in ICP, which was also a shimstock hold. Normal responses to pulp testing and no other signs or symptoms were present.
The LR7 gave a sharp pain upon release of pressure following application of a Tooth Slooth® (Professional Results Inc, Laguna Niguel, CA). Tactile evaluation with a straight probe elicited sharp pain on the buccal and lingual surfaces. Transillumination and removal of the old restoration also assisted with the diagnosis. Crack lines were noted on both marginal ridges, buccal and lingual surfaces. In particular, the buccal and lingual surfaces were extremely sensitive to cold air, demonstrating that the fracture had extended through enamel with leakage into the underlying dentine layer. There was also an exaggerated response to ethyl chloride.
Nothing abnormal was noted on the pre-operative peri-apical radiograph (Figure 2c).
Treatment
The conformative occlusal scheme was adopted using the ‘Occlusal Sketch’ as a pre-operative record of the occlusion (Figure 2e).1 Improvements were made to the occlusion where possible, ie multiple simultaneous contacts which are in line with the long axis of the teeth.
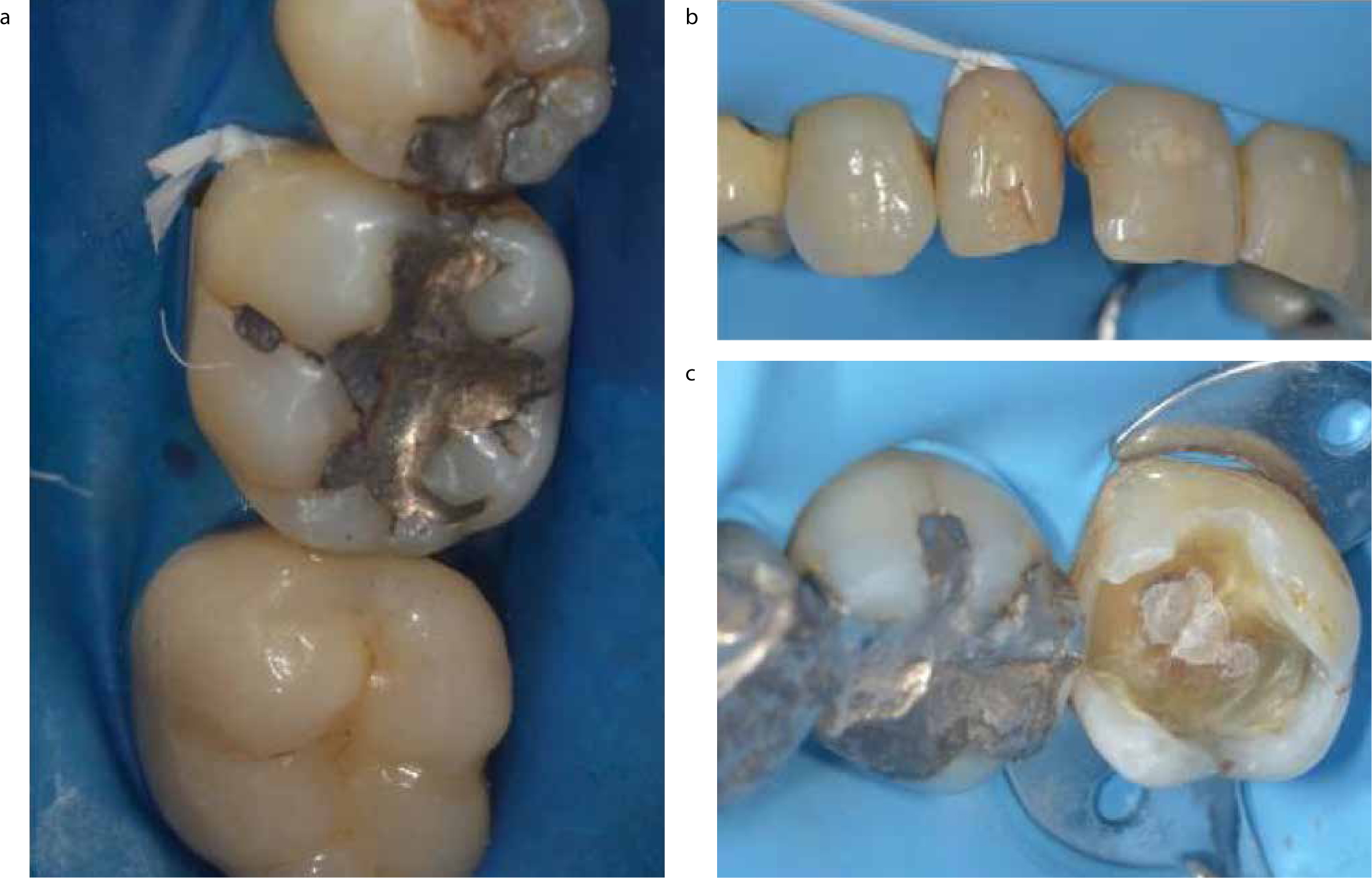
The patient was insistent that only ‘white’ restorations were placed during her treatment. Therefore, a minimum 1.5–2 mm occlusal reduction is necessary for the ceramic restorations.2 The use of rubber dam was mandatory for the placement of resin-composite and bonded indirect restorations; isolation is necessary prior to bonding any adhesive restorations within the mouth (Figure 3).3
Figure 3.
(a–c) Examples of rubber dam isolation prior to direct resin-composite bonding procedures.
The LR7 amalgam restoration was removed to investigate the extent of the fracture fully. The patient travelled over five hours for each dental appointment and it was decided that each appointment would be used with maximum productivity. Therefore, the amalgam restoration and crack lines were removed and replaced with a definitive direct composite onlay at one sitting (Figures 4 a–d, k). The cavity was restored using a sectional matrix and separation ring, providing a tight and anatomically correct inter-proximal contact area.4
Root canal treatment was performed on the LR5. The residual cavity was >1/2 of the tooth width, with evidence of weakened cusps and craze lines. Therefore, it was decided to place a lithium disilicate onlay to prevent future crown fracture (Figures 4e, i–k).
The LR6 was given a minor occlusal adjustment to the mesio-buccal cusp region by gently grinding the heavy, broad rubbing contact; the occlusal contacts were assessed with 8 µm Shimstock metal foil (Hanel) before and after. The aim was not to remove the contact entirely, but rather to reduce the applied axial forces and achieve even ‘shimstock holds’ on the other posterior teeth. The symptoms improved significantly, but the sensitivity did not fully resolve due to the presence of the cracks. The amalgam core was replaced with resin-composite (nanofill) and prepared for a monolithic yttrium stabilized zirconium oxide crown, due to its outstanding mechanical properties and high biocompatibility (Figures 4 f–k).5
Figure 4. Removal of the restoration at LR7, including the buccal and lingual cracks. Transillumination highlights the underlying incomplete fracture lines (a). Rubber dam isolation and 1.5 mm occlusal reduction (b). Composi-Tight 3D XR matrix, ring and wedge placement (Garrison); removal of the remnant lining material still to take place (c). Air abrasion was used to augment micro-mechanical retention prior to placement of the direct resin-composite onlay (d). RCT performed on the LR5 (e). Occlusal adjustment to mesio-buccal cusp LR6 (f). Amalgam core removed, the weakened mesio-lingual cusp fractured during the procedure (g). Resin-composite core build-up, prior to crown preparation (h, i). Monolithic zirconia crown LR6 and lithium disilicate onlay LR5 bonded (j). The conformative approach with simultaneous contacts and even shimstock holds, one month post-operatively (k).
Conclusions
Amalgam has clearly proven its long-term reliability as a restoration over the generations. However, its over-prescription in the past, and even to present day, has left many clinicians in the difficult situation of maintaining and restoring large, failing restorations; each patient presenting with a unique set of signs and symptoms for each diagnosis. A thorough clinical and radiographic assessment must take precedence before contemplating the use of a high-speed handpiece. Once a confident diagnosis has been established, one must then consider the implications associated with each material used for restoration of the tooth. The clinician must also incorporate the most appropriate occlusal relationship as part of the treatment plan, which includes: the conformative, re-organized and Dahl Concept approaches. The patient must be made aware of any potential complications associated with the diagnoses and how this will be addressed in the future. The temptation to save a tooth with a hopeless prognosis is not in anyone's interest and the dentist should know when to accept that the battle has been lost. However, with this newly acquired knowledge, it is clear that early intervention will help to win the war.