Gokcen-Rohlig B, Yaltirik M, Ozer S, Tuncer ED, Evlioglu G. Survival and success of ITI implants and prostheses: retrospective study of cases with 5-year follow-up. Eur J Dent. 2009; 3:42-49
Baig MR, Rajan M. Effects of smoking on the outcome of implant treatment: a literature review. Indian J Dent Res. 2007; 18:190-195
Zupnik J, Kim S-W, Ravens D, Karimbux N, Guze K. Factors associated with dental implant survival: a 4-year retrospective analysis. J Periodontol. 2011; 82:1390-1395
Abt E. Growing body of evidence on survival rates of implant-supported fixed prostheses. Evid Based Dent. 2008; 9:51-52
Han HJ, Kim S, Han DH. Multifactorial evaluation of implant failure: a 19 year retrospective study. Int J Oral Maxillofac Implants. 2014; 29:303-310
Warreth A, Boggs S, Ibieyou N, El-Helali R, Hwang S. Peri-implant diseases: an overview. Dent Update. 2015; 42:166-184
Buser D, Weber HP, Donath K, Fiorellini JP, Paquette DW, Williams RC. Soft tissue reactions to non-submerged unloaded titanium implants in beagle dogs. J Periodontol. 1992; 63:225-235
Weber HP, Buser D, Donath K, Fiorellini JP, Doppalapudi V, Paquette DW, Williams RC. Comparison of healed tissues adjacent to submerged and non-submerged unloaded titanium dental implants. A histometric study in beagle dogs. Clin Oral Implants Res. 1996; 7:11-19
Cochran DL. The scientific basis for and clinical experiences with Straumann implants including the ITI Dental Implant System: a consensus report. Clin Oral Implants Res. 2000; 11:33-58
Tarnow DP, Cho SC, Wallace SS. The effect of inter-implant distance on the height of inter-implant bone crest. J Periodontol. 2000; 71:546-549
Brånemark P-I. Osseointegration and its experimental studies. J Prosthet Dent. 1983; 50:399-410
Sennerby L, Ericson LE, Thomsen P, Lekholm U, Astrand P. Structure of the bone-titanium interface in retrieved clinical oral implants. Clin Oral Implants Res. 1991; 2:103-111
Clokie CML, Warshawsky H. Morphological and radioautographic studies of bone formation in relation to titanium implants using the rat tibia as a model. Int J Oral and Maxillofac Implants. 1995; 10:155-165
The glossary of prosthodontic terms. J Prosthet Dent. 2005; 94
Warreth A, Fesharaki H, McConville R, McReynolds D. An introduction to single implant abutments. Dent Update. 2013; 40:7-17
Thomas KA. Hydroxyapatite coatings. Orthopaedics. 1994; 17:267-278
Sykaras N, Iacopino AM, Marker VA, Triplett RG, Woody RD. Implant materials, designs, and surface topographies: their effect on osseointegration. A literature review. Int J Oral Maxillofac Implants. 2000; 15:675-690
Higuchi KW, Folmer T, Kultje C. Implant survival rates in partially edentulous patients: a 3-year prospective multicenter study. J Oral Maxillofac Surg. 1995; 53:264-268
Geckili O, Bilhan H, Geckili E, Cilingir A, Mumcu E, Bural C. Evaluation of possible prognostic factors for the success, survival, and failure of dental implants. Implant Dent. 2014; 23:44-50
Lekholm U, Zarb GA. Patient selection and preparation, 1st edn. In: Brånemark P, Zarb G, Albrektsson T. New Malden, UK: Quintessence Publishing Co; 1985
Jones AA, Cochran DL. Consequences of implant design. Dent Clin North Am. 2006; 50:339-360
Kim TH, Lee DW, Kim CK, Park KH, Moon IS. Influence of early cover screw exposure on crestal bone loss around implants: intra-individual comparison of bone level at exposed and non-exposed implants. J Periodontol. 2009; 80:933-939
Javed F, Romanos GE. The role of primary stability for successful immediate loading of dental implants. A literature review. J Dent. 2010; 38:612-620
Kim YS, Lim YJ. Primary stability and self-tapping blades: biomechanical assessment of dental implants in medium-density bone. Clin Oral Implants Res. 2011; 22:1179-1184
Morris HF, Winkler S, Ochi S, Kanaan A. A new implant designed to maximize contact with trabecular bone: survival to 18 months. J Oral Implantol. 2001; 27:164-173
Davies JE. Mechanisms of endosseous integration. Int J Prosthodont. 1998; 11:391-401
Warreth A, Ibieyou N, MacCarthy D. Bisphosphonates, oral implants and osteonecrosis of the jaw: a review and guidelines. J Dent Oral Hyg. 2010; 11:155-162
Schwarz F, Alcoforado G, Nelson K, Schaer A, Taylor T, Beuer F, Strietzel FP. Impact of implant-abutment connection, positioning of the machined collar/microgap, and platform switching on crestal bone level changes. Camlog Foundation Consensus Report. Clin Oral Implants Res. 2014; 25:1301-1303
Romanos GE, Basha-Hijazi A, Gupta B, Ren YF, Malmstrom H. Role of clinician's experience and implant design on implant stability. An ex vivo study in artificial soft bones. Clin Implant Dent Relat Res. 2014; 16:166-171
Menicucci G, Pachie E, Lorenzetti M, Migliaretti G, Carossa S. Comparison of primary stability of straight-walled and tapered implants using an insertion torque device. Int J Prosthodont. 2012; 25:465-471
Alves CC, Neves M. Tapered implants: from indications to advantages. J Periodont Rest Dent. 2009; 29:161-167
Warreth A, McAleese E, McDonnell P, Slami R, Guray SM. Dental implants and single implant-supported restorations. J Ir Dent Assoc. 2013; 59:32-43
Steigenga J, Al-Shammari K, Misch C, Nociti FH, Wang H-L. Effects of implant thread geometry on percentage of osseointegration and resistance to reverse torque in the tibia of rabbits. J Periodontol. 2004; 75:1233-1241
Rabel A, Köhler SG, Schmidt-Westhausen AM. Clinical study on the primary stability of two dental implant systems with resonance frequency analysis. Clin Oral Investig. 2007; 11:257-265
Yoon HG, Heo SJ, Koak JY, Kim SK, Lee SY. Effect of bone quality and implant surgical technique on implant stability quotient (ISQ) value. J Adv Prosthodont. 2011; 3:10-15
Cochran DL. A comparison of endosseous dental implant surfaces. J Periodontol. 1999; 70:1523-1539
Oue H, Doi K, Oki Y, Makihara Y, Kubo T, Perrotti V, Piattelli A, Akagawa Y, Tsuga K. Influence of implant surface topography on primary stability in a standardized osteoporosis rabbit model study. J Funct Biomater. 2015; 6:143-152
Novaes AB, Souza SL, de Oliveria PT, Souza AM. Histomorphometric analysis of the bone-implant contact obtained with 4 different implant surface treatments placed side by side in the dog mandible. Int J Oral Maxillofac Implants. 2002; 17:377-383
Klokkevold PR, Johnson P, Dadgostari S, Caputo A, Davies JE, Nishimura RD. Early endosseous integration enhanced by dual acid etching of titanium: a torque removal study in the rabbit femur. Clin Oral Implants Res. 2001; 12:350-357
Wong M, Eulenberger J, Schenk R, Hunziker E. Effects of surface topology on the osseointegration of implant in trabecular bone. J Biomed Mater Res. 1995; 29:1567-1575
Le Guehennec L, Goyenvalle E, Lopez-Heredia MA, Weiss P, Amouriq Y, Layrolle P. Histomorphometric analysis of the osseointegration of four different implant surfaces in the femoral epiphyses of rabbits. Clin Oral Implants Res. 2008; 19:1103-1110
Renvert S, Roos-Jansåker AM, Claffey N. Nonsurgical treatment of peri-implant mucositis and peri-implantitis: a literature review. J Clin Periodontol. 2008; 35:305-315
Misch CE. Short dental implants: a literature review and rationale for use. Dent Today. 2005; 24:64-68
Monje A, Fu JH, Chan HL, Suarez F, Galindo-Moreno P, Catena A, Wang HL. Do implant length and width matter for short dental implants (<10 mm)? A meta-analysis of prospective studies. J Periodontol. 2013; 84:1783-1791
Misch CE, Steignga J, Barboza E, Misch-Dietsh F, Cianciola LJ, Kazor C. Short dental implants in posterior partial edentulism: a multicenter retrospective 6-year case series study. J Periodontol. 2006; 77:1340-1347
Bahat O. Treatment planning and placement of implants in the posterior maxillae: report of 732 consecutive Nobelpharma implants. Int J Oral Maxillofac Implants. 1993; 8:151-161
Winkler S, Morris HF, Ochi S. Implant survival to 36 months as related to length and diameter. Ann Periodontol. 2000; 5:22-31
Jokstad A. The evidence for endorsing the use of short dental implants remains inconclusive. Evid Based Dent. 2011; 12:99-101
Monje A, Chan HL, Fu JH, Suarez F, Galindo-Moreno P, Wang HL. Are short dental implants (<10 mm) effective? A meta-analysis on prospective clinical trials. J Periodontol. 2013; 84:895-904
Lee JH, Frias V, Lee KW, Wright RF. Effect of implant size and shape on implant success rate: a literature review. J Prosthet Dent. 2005; 94:377-381
Allum SR, Tomlinson RA, Joshi R. The impact of loads on standard diameter, small diameter and mini implants: a comparative laboratory study. Clin Oral Implants Res. 2008; 19:553-559
Misch CE, Qu M, Bidez MW. Mechanical properties of trabecular bone in the human mandible: implications for dental implant treatment planning and surgical placement. J Oral Maxillofac Surg. 1999; 57:700-706
Renouard F, Nisand D. Impact of implant length and diameter on survival rates. Clin Oral Implants Res. 2006; 17:35-51
Ivanoff CJ, Sennerby L, Johansson C, Rangert B, Lekholm U. Influence of implant diameters on the integration of screw implants. An experimental study in rabbits. Int J Oral Maxillofac Surg. 1997; 26:141-148
Langer B, Langer L, Herrmann I, Jorneus L. The wide fixture: a solution for special bone situations and a rescue for the compromised implant. Part 1. Int J Oral Maxillofac Implants. 1993; 8:400-408
Davarpanah M, Martinez H, Tecuciana J-F, Celletti R, Lazzara R. Small-diameter implants: indications and contraindications. J Esthet Dent. 2000; 12:186-194
Suba C, Velich N, Turi C, Szabó G. Surface analysis methods of biomaterials used in oral surgery: literature review. J Craniofac Surg. 2005; 16:31-36
Mouhyi J, Sennerby L, Wennerberg A, Louette P, Dourov N, van Reck J. Re-establishment of the atomic composition and the oxide structure of contaminated titanium surfaces by means of carbon dioxide laser and hydrogen peroxide: an in vitro study. Clin Implant Dent Relat Res. 2000; 2:190-202
Cooper LF. A role for surface topography in creating and maintaining bone at titanium endosseous implants. J Prosthet Dent. 2000; 84:522-534
Blumenthal NC, Cosma V. Inhibition of apatite formation by titanium and vanadium ions. J Biomed Mater Res. 1989; 23:13-22
Siddiqi A, Payne AG, De Silva RK, Duncan WJ. Titanium allergy: could it affect dental implant integration?. Clin Oral Implants Res. 2011; 22:673-680
Javed F, Al-Hezaimi K, Almas K, Romanos GE. Is titanium sensitivity associated with allergic reactions in patients with dental implants? A systematic review. Clin Implant Dent Relat Res. 2013; 15:47-52
Alhag M, Renvert S, Polyzois I, Claffey N. Re-osseointegration on rough implant surfaces previously coated with bacterial biofilm: an experimental study in the dog. Clin Oral Implants Res. 2008; 19:182-187
Renvert S, Polyzois I, Maguire R. Re-osseointegration on previously contaminated surfaces: a systematic review. Clin Oral Implants Res. 2009; 20:216-227
Gineste L, Gineste M, Ranz X, Ellefterion A, Guilhem A, Rouquet N, Frayssinet P. Degradation of hydroxylapatite, fluorapatite, and fluorhydroxyapatite coatings of dental implants in dogs. J Biomed Mater Res. 1999; 48:224-234
Förster Y, Rentsch C, Schneiders W, Bernhardt R, Simon JC, Worch H, Rammelt S. Surface modification of implants in long bone. Biomatter. 2012; 2:149-157
Wie H, Herø H, Solheim T, Kleven E, Rørvik AM, Haanaes HR. Bonding capacity in bone of HIP-processed HA-coated titanium: mechanical and histological investigations. J Biomed Mater Res. 1995; 29:1443-1449
Cook SD, Salkeld SL, Gaisser DM, Wagner WR. The effect of surface macrotexture on the mechanical and histologic characteristics of hydroxylapatite-coated dental implants. J Oral Implantol. 1993; 19:(4)288-294
Osman RB, Elkhadem AH, Ma S, Swain MV. Titanium versus zirconia implants supporting maxillary overdentures: three-dimensional finite element analysis. Int J Oral Maxillofac Implants. 2013; 28:198-208
Kajiwara N, Masaki C, Mukaibo T, Kondo Y, Nakamoto T, Hosokawa R. Soft tissue biological response to zirconia and metal abutments compared with natural tooth: microcirculation monitoring as a novel bioindicator. Implant Dent. 2015; 24:37-41
Andreiotelli M, Wenz HJ, Kohal RJ. Are ceramic implants a viable alternative to titanium implants? A systematic literature review. Clin Oral Implants Res. 2009; 20:32-47
Özkurt Z, Kazazoğlu E. Zirconia dental implants: a literature review. J Oral Implantol. 2011; 37:367-376
Fuentealba R, Jofré J. Esthetic failure in implant dentistry. Dent Clin North Am. 2015; 59:227-246
McGlumphy EA, Mendel DA, Holloway JA. Implant screw mechanics. Dent Clin North Am. 1998; 42:71-89
Maeda Y, Miura J, Taki I, Sogo M. Biomechanical analysis on platform switching: is there any biomechanical rationale?. Clin Oral Implants Res. 2007; 18:581-584
Gracis S, Michalakis K, Vigolo P, Vult von Steyern P, Zwahlen M, Sailer I. Internal vs. external connections for abutments/reconstructions: a systematic review. Clin Oral Implants Res. 2012; 23:202-216
Akça K, Cehreli MC, Iplikçioğlu H. Evaluation of the mechanical characteristics of the implant-abutment complex of a reduced-diameter morse-taper implant. A nonlinear finite element stress analysis. Clin Oral Implants Res. 2003; 14:444-454
Segundo RM, Oshima HM, da Silva IN, Burnett LH, Mota EG, Silva LL. Stress distribution of an internal connection implant prostheses set: a 3D finite element analysis. Stomatologija. 2009; 11:55-59
Keating K. Connecting abutments to dental implants: ‘an engineer's perspective’. Irish Dentist. 2001; 43-46
Jung SW, Son MK, Chung CH, Kim HJ. Abrasion of abutment screw coated with TiN. J Adv Prosthodont. 2009; 1:102-106
Jo JY, Yang DS, Huh JB, Heo JC, Yun MJ, Jeong CM. Influence of abutment materials on the implant-abutment joint stability in internal conical connection type implant systems. J Adv Prosthodont. 2014; 6:491-497
Satterthwaite J, Rickman L. Retrieval of a fractured abutment screw thread from an implant: a case report. Br Dent J. 2008; 204:177-180
Drago CJ. A clinical study of the efficacy of gold-tite square abutment screws in cement-retained implant restorations. Int J Oral Maxillofac Implants. 2003; 18:273-278
Byrne D, Jacobs S, O'Connell B, Houston F, Claffey N. Pre-loads generated with repeated tightening in three types of screws used in dental implant assemblies. J Prosthodont. 2006; 15:164-171
Binon PP. Evaluation of three slip fit hexagonal implants. Implant Dent. 1996; 5:235-248
Binon PP, McHugh MJ. The effect of eliminating implant/abutment rotational misfit on screw-stability. Int J Prosthodont. 1996; 9:511-519
Cantwell A, Hobkirk JA. Pre-load loss in gold prosthesis-retaining screws as a function of time. Int J Oral Maxillofac Implants. 2004; 19:124-132
Winkler S, Ring K, Ring JD, Boberick KG. Implant screw mechanics and the settling effect: overview. J Oral Implantol. 2003; 29:242-245
Kim KS, Han JS, Lim YJ. Settling of abutments into implants and changes in removal torque in five different implant-abutment connections. Part 1: Cyclic loading. Int J Oral Maxillofac Implants. 2014; 29:1079-1084
Tan KB, Nicholls JI. Implant-abutment screw-joint pre-load of 7 hex-top abutment systems. Int J Oral Maxillofac Implants. 2001; 16:367-377
Lang LA, May KB, Wang RF. The effect of the use of a counter-torque device on the abutment-implant complex. J Prosthet Dent. 1999; 81:411-417
Gratton DG, Aquilino SA, Stanford CM. Micromotion and dynamic fatigue properties of the dental implant-abutment interface. J Prosthet Dent. 2001; 85:47-52
Haack JE, Sakaguchi RL, Sun T, Coffey JP. Elongation and pre-load stress in dental implant abutment screws. Int J Oral Maxillofac Implants. 1995; 10:529-536
Quek HC, Tan KB, Nicholls JI. Load fatigue performance of four implant-abutment interface designs: effect of torque level and implant system. Int J Oral Maxillofac Implants. 2008; 23:253-262
Goheen KL, Vermilyea SG, Vossoughi J, Agar JR. Torque generated by handheld screwdrivers and mechanical torqueing devices for osseointegrated implants. Int J Oral Maxillofac Implants. 1994; 9:149-155
Khraisat A, Abu-Hammad O, Al-Kayed AM, Dar-Odeh N. Stability of the implant/abutment joint in a single-tooth external-hexagon implant system: clinical and mechanical review. Clin Implant Dent Relat Res. 2004; 6:222-229
Monje A, Pommer B. The concept of platform switching to preserve peri-implant bone level: assessment of methodologic quality of systematic reviews. Int J Oral Maxillofac Implants. 2015; 30:1084-1092
de Almeida FD, Carvalho AC, Fontes M, Pedrosa A, Costa R, Noleto JW, Mourão CF. Radiographic evaluation of marginal bone level around internal-hex implants with switched platform: a clinical case report series. Int J Oral Maxillofac Implants. 2011; 26:587-592
Strietzel FP, Neumann K, Hertel M. Impact of platform switching on marginal peri-implant bone-level changes. A systematic review and meta-analysis. Clin Oral Implants Res. 2015; 26:342-358
Linkevicius T, Apse P, Grybauskas S, Puisys A. Influence of thin mucosal tissues on crestal bone stability around implants with platform switching: a 1-year pilot study. J Oral Maxillofac Surg. 2010; 68:2272-2277
Maeda Y, Satoh T, Sogo M. In vitro differences of stress concentrations for internal and external hex implant-abutment connections: a short communication. J Oral Rehabil. 2006; 33:75-78
Cimen H, Yengin E. Analyzing the effects of the platform-switching procedure on stresses in the bone and implant-abutment complex by 3-dimensional fem analysis. J Oral Implantol. 2012; 38:21-26
Hebel KS, Gajjar RC. Cement-retained versus screw-retained implant restorations: achieving optimal occlusion and aesthetics in implant dentistry. J Prosthet Dent. 1997; 77:28-35
Warreth A, Ramadan M, Bajilan MR, Ibieyou N, El-Swiah J, Elemam RF. Fundamentals of occlusion and restorative dentistry. Part I: basic principles. J Ir Dent Assoc. 2015; 61:201-208
Feine JS, Carlsson GE, Awad MA, Chehade A, Duncan WJ The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Montreal, Quebec, May 24–25, 2002. Int J Oral Maxillofac Implants. 2002; 17:601-602
The York consensus statement on implant-supported overdentures. Eur J Prosthodont Restor Dent. 2009; 17:164-165
Agar JR, Cameron SM, Hughbanks JC, Parker MH. Cement removal from restorations luted to titanium abutments with simulated subgingival margins. J Prosthet Dent. 1997; 78:43-47
Burns DR. Mandibular implant overdenture treatment: consensus and controversy. J Prosthodont. 2000; 9:37-46
Sakka S, Baroudi K, Nassani MZ. Factors associated with early and late failure of dental implants. J Investig Clin Dent. 2012; 3:258-261
Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants. 1986; 1:11-25
Marsh PD. Dental plaque: biological significance of a biofilm and community life-style. J Clin Periodont. 2005; 32:7-15
Mombelli A, Lang NP. The diagnosis and treatment of peri-implantitis. Periodontol 2000. 1998; 17:63-76
Lang NP, Berglundh T. Periimplant diseases: where are we now? – Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol. 2011; 38:178-181
Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg. 1981; 10:387-416
Adell R, Lekholm U, Brånemark PI, Lindhe J, Rockler B, Eriksson B, Lindvall AM, Yoneyama T, Sbordone L. Marginal tissue reactions at osseointegrated titanium fixtures. Swed Dent J. 1985; 28:175-181
Adell R, Lekholm U, Rockler B, Brånemark PI, Lindhe J, Eriksson B, Sbordone L. Marginal tissue reactions at osseointegrated titanium fixtures (I). A 3-year longitudinal prospective study. Int J Oral Maxillofac Surg. 1986; 15:39-52
Kracher CM, Smith WS. Oral health maintenance dental implants. Dent Assist. 2010; 79:27-35
Lang NP, Berglundh T, Heitz-Mayfield LJ, Pjetursson BE, Salvi GE, Sanz M. Consensus statements and recommended clinical procedures regarding implant survival and complications. Int J Oral Maxillofac Implants. 2004; 19:150-154
Stoumpis C, Kohal RJ. To splint or not to splint oral implants in the implant-supported overdenture therapy? A systematic literature review. J Oral Rehabil. 2011; 38:857-869
Warreth A, Byrne C, Alkadhimi AF, Woods E, Sultan A. Mandibular implant-supported overdentures: attachment systems, and number and locations of implants – Part II. J Ir Dent Assoc. 2015; 61:144-148
Dental implants are widely used and are considered to be one of several treatment options that can be used to replace missing teeth. A number of implant-supported treatment options have been used successfully to replace a single tooth and multiple teeth, as well as a completely edentulous jaw. However, as the number of patients who have dental implants is increasing, dental personnel are more likely to see patients with implant-supported restorations or prostheses. Nevertheless, dental implants may fail as a result of mechanical complications, such as screw loosening or due to biological causes like peri-implant diseases. As a result, dental personnel should be able to recognize these complications and the factors that have negative effects on the success of such implant-supported restorations or prostheses. Therefore, a basic knowledge of dental implants is necessary for every dental student, hygienist and dentist.
CPD/Clinical Relevance: Maintenance of implant-supported restorations and prostheses requires long-term follow-ups. It is the responsibility of the patient to maintain good oral hygiene and also of the dental personnel who look after the patient to ensure a durable restoration and prosthesis.
Article
Dental implants (also known as oral or endosseous implants) have been used to replace missing teeth for more than half a century. They are considered to be an important contribution to dentistry as they have revolutionized the way by which missing teeth are replaced with a high success rate.1,2,3 This success depends on the ability of the implant material to integrate with the surrounding tissue. However, this integration is influenced by several factors, such as implant material, bone quality and quantity, and the implant loading condition.2,3
As the use of dental implants has become much more common, dental personnel are more likely to see patients who have implant–supported/retained restorations. Nevertheless, dental implants are affected by diseases in a similar manner to teeth and may also fail after several months or years in service.4,5,6 Therefore, it is not unreasonable to suggest that the implant and the peri-implant tissue should be examined on a routine basis in a similar manner to that which is carried out for periodontal examination.7 So, when a deviation from the norm is found, the treatment may be carried out in practice or by a specialist, depending on the severity of the condition. Accordingly, the dentist should be equipped with basic knowledge of dental implants. Hence, it is the aim of this article to provide this basic information which is needed by every dental student and dentist alike.
Implant-soft tissue interface
The tissue that surrounds implants is known as peri-implant tissue and is comprised of soft (mucosa) and hard (bone) tissues. The peri-implant soft tissue has similar features to the soft tissue that surrounds teeth.7,8,9,10 It consists of a junctional epithelium and connective tissue. The junctional epithelium is attached to the implant and/or abutment surface through a hemi-desmosomal attachment. Connective tissue is present apical to the junctional epithelium and coronal to the crest of alveolar bone.10 Connective tissue fibres are found to be positioned close to the implant surface but not attached to it, and predominantly arranged in a circular manner. Connective tissue fibres also arise from the crest of alveolar bone and from the periosteum and are oriented parallel to the implant/abutment surface and extend towards the oral epithelium. Thus, the junctional epithelium and connective tissue form a protective seal between the oral environment and the peri-implant bone which plays a vital role in the success of the implant treatment outcome. The junctional epithelium and the connective tissue are collectively known as the biologic width, which is comparable to that found around teeth.11
Implant-bone interface and osseointegration
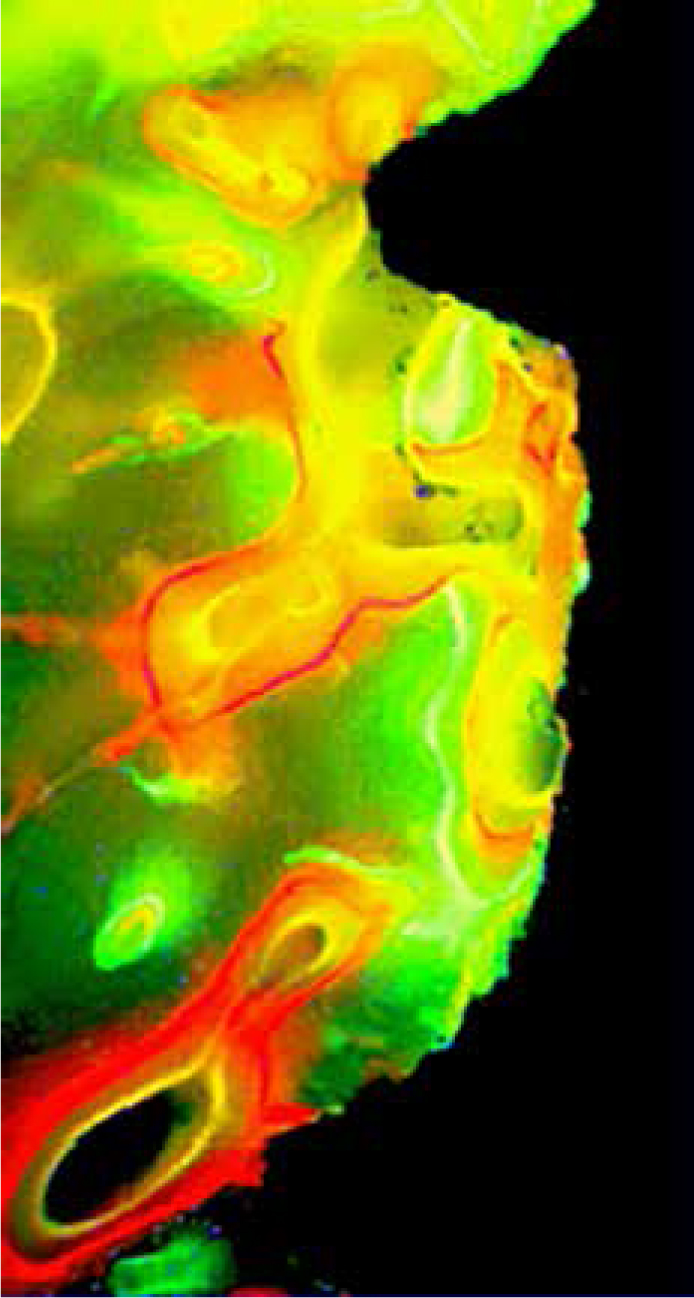
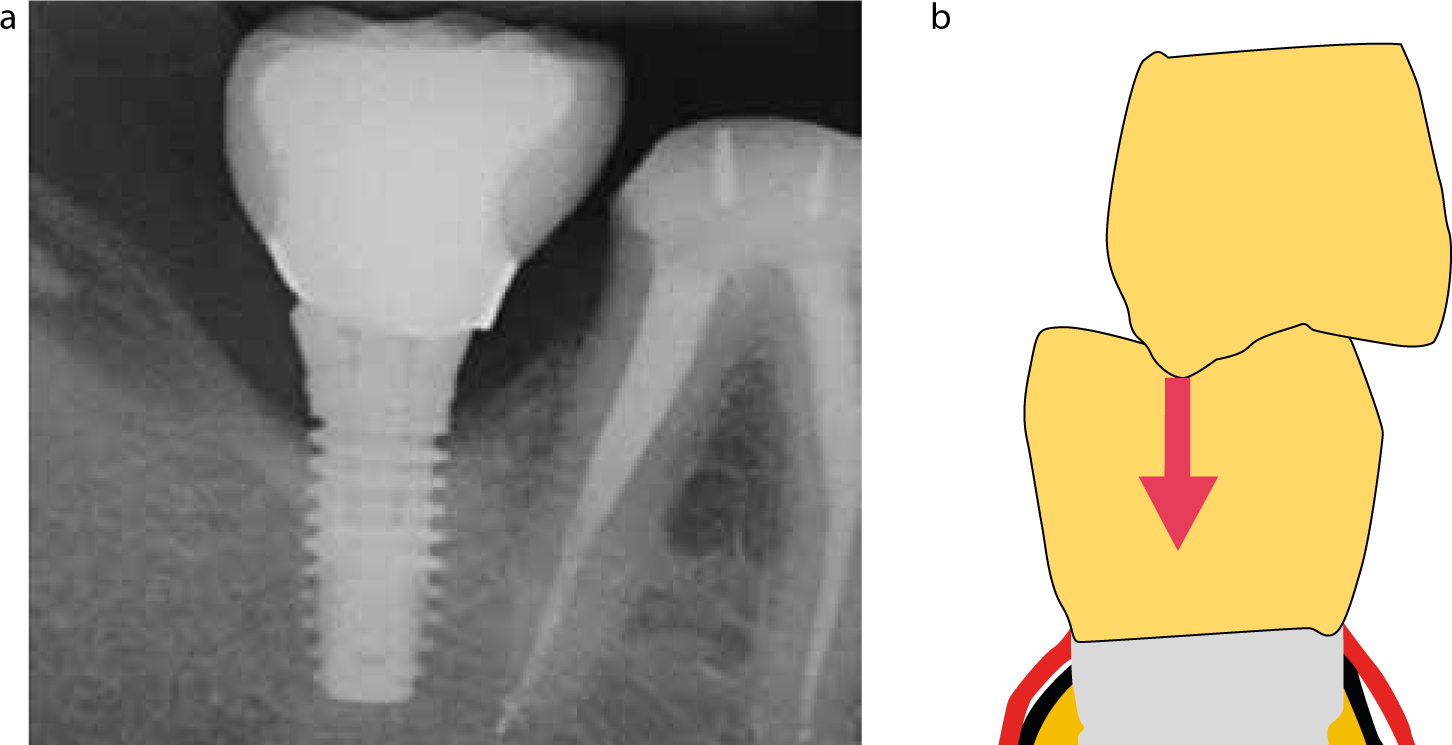
For dental implants to succeed, intimate contact between the peri-implant bone and the implant surface should be achieved and maintained. Therefore, an integration between the implant surface and the bone is required for the success of any implant system. This integration is known as osseointegration, and is defined as a direct structural and functional connection between ordered living bone and the surface of a load-carrying implant.12 Under light microscopy, successful osseointegration shows direct apposition of bone on implant surface (Figure 1). However, when the bone-implant interface is examined using electron microscopy, the implant surface is found to be separated from the surrounding bone by an amorphous layer, a granular electron-dense layer, or a layer of uncalcified collagen fibrils13,14 with a thickness that ranges from 100 nm to 400 nm.13 Nevertheless, this layer appears not to have a negative impact on the success of the osseointegration. Inversely, when the connection between implant surface and bone is mediated by a layer of connective tissue, osseointegration fails to occur.5,15,16
Figure 1. A histological image of bone-implant interface. Bone formation around the implant labelled with different chelating agents (fluoro-chromes). The implant is the large black area.
It is important to mention that, as a result of the absence of periodontal ligaments between the implant and its surrounding bone, when the implants are loaded, they move within the bone due to bone elastic deformation.6 Furthermore, osseointegrated implants cannot be moved orthodontically.
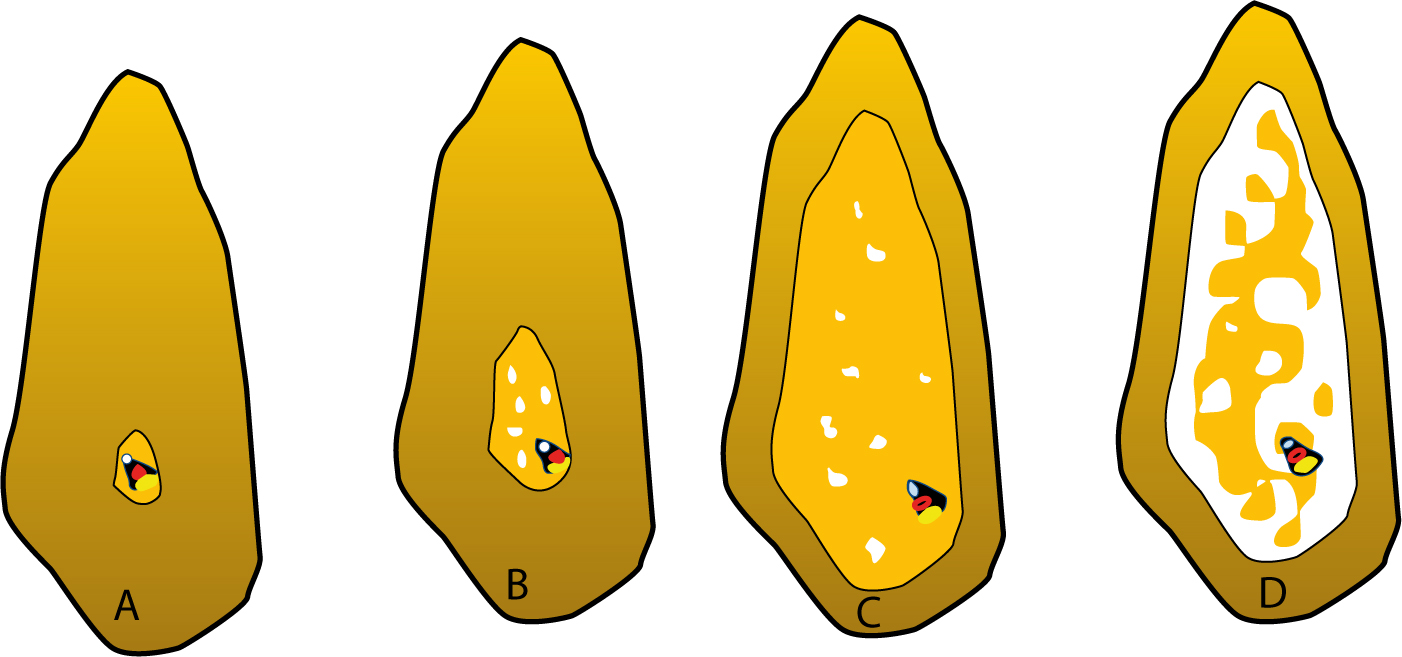
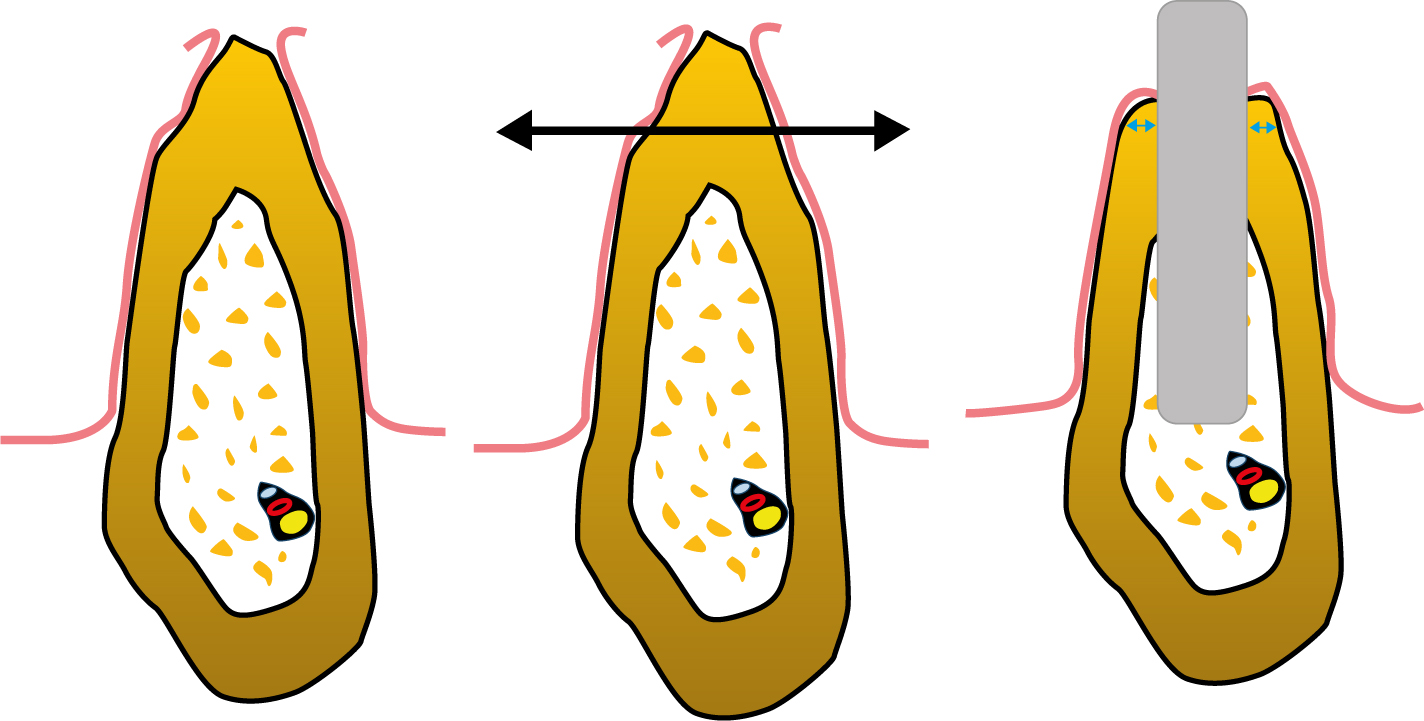
Several factors are reported to play a role in obtaining osseointegration.17,18 As an example, poor bone quality was found to be associated with a high implant failure rate when compared with bone of a high quality.19 Clinical studies have reported that dental implants in the maxillary arch (especially for the posterior maxilla) have lower survival rates than those in the mandibular arch.19 This is usually attributed to the differences in bone quality between the two arches.20 Bone quality, as classified by Lekholm and Zarb,21 is based on radiographic assessment as well as resistance during the implant drilling procedure. Accordingly, bone is categorized into four classes, as described in Figure 2 and Table 1. Some factors which affect osseointegration are discussed below and summarized in Table 2.
Type I: almost the entire bone is composed of homogeneous compact bone;
Type II: a thick layer of compact bone surrounds a core of dense trabecular bone;
Type III: a thin layer of cortical bone surrounds a core of dense trabecular bone; and
Type IV: a thin layer of cortical bone surrounding a core of low density trabecular bone.
Bone quality and quantity
Implant shape
Implant surface macro-structure
Implant micro-structure (roughness)
Material biocompatibility
Surgical techniques
Heat generation during the implant placement surgery
Implant primary (initial) stability
Implant loading
Figure 2. The classification of bone according to its quality: Class I (A), Class II (B), Class III (C) and Class IV (C).
Implant placement methods
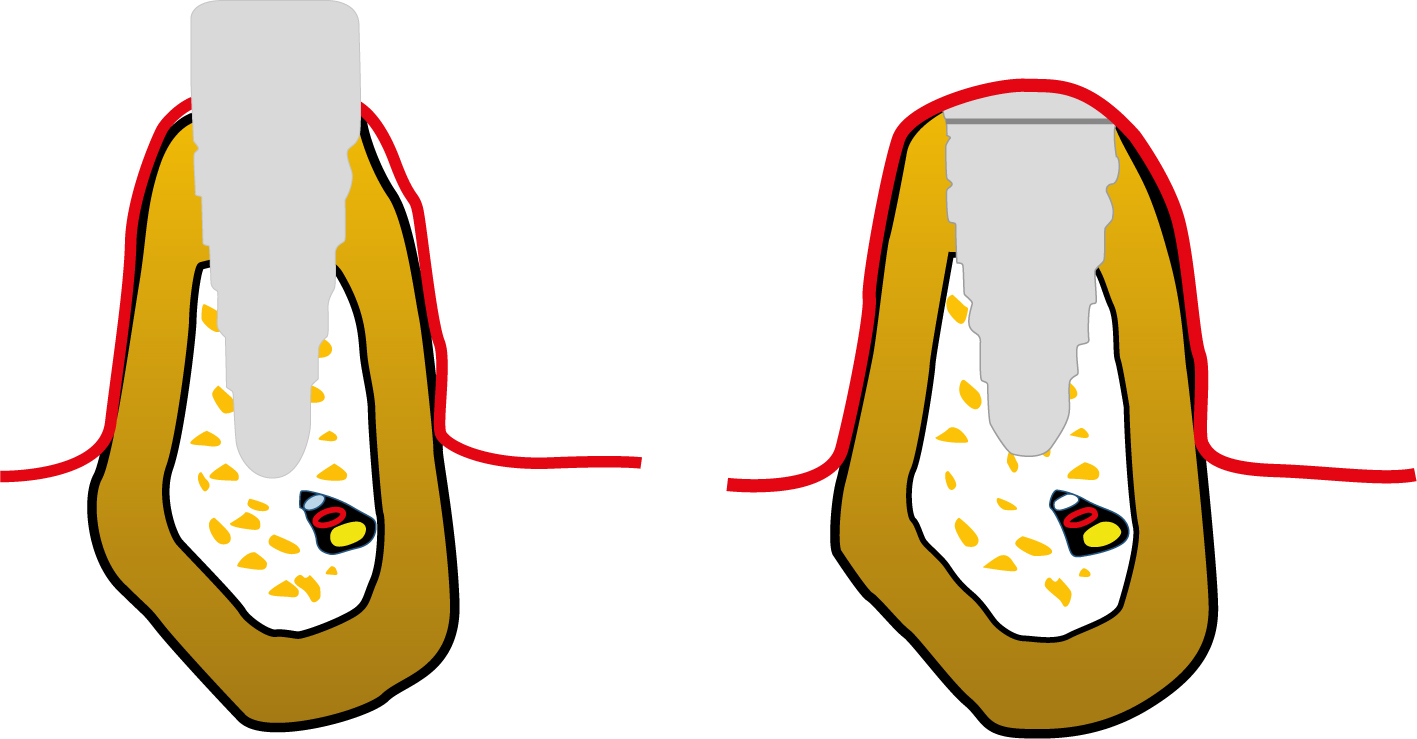
Surgical implant placement may be carried out in one- or two-stage methods (Figure 3). The one-stage method is also known as the non-submerged method. Using this technique, the bone is prepared to receive the implant. The implant is fitted into the prepared bone (osteotomy). However, the coronal part of the implant is kept above the bone crest, protruding through the soft tissue, and is exposed to the oral environment during the healing stage.22 The restoration can be attached immediately after the implant placement surgery or may also be delayed.
Figure 3. A schematic presentation of an implant placed according to the one-stage (left) and two-stage (right) implant placement methods. Note the transmucosal part (the neck) penetrating the peri-implant mucosa in the one-stage method.
The lack of a micro-gap between the implant and the abutment at the alveolar bone crest level, resulting in a less crestal bone resorption;
The prosthetic procedure is simplified and less chair time per patient is required; and
A non-loaded, immediate, or delay-loaded protocol can be implemented.
One of the drawbacks that may be associated with this surgical protocol is that the implant is exposed to the oral environment, which may lead to contamination of the surgical site. Furthermore, the implant may be exposed to undue trauma which can negatively affect the healing. However, bone with optimum quality and quantity is a prerequisite for this method to be used. Nevertheless, the method can be clinically successful. Examples of the implants that can be placed using the one-stage technique include the Solid-Screw Implant® (Straumann UK, Crawley, W Sussex), AdVent Implant® (Zimmer, FLA, USA) and Single-stage Implant System® (BioHorizons, AL, USA).
In contrast, the two-stage method is also known as the submerged technique (Figure 3). In this method, two surgical procedures are carried out. The first surgery involves installing the implant into the bone, and a cover-screw (also known as a sealing-screw) is attached to the implant platform. A countersink bone preparation that allows for placement of the implant platform below the bone crest may be implemented. The countersink allows the placement of the cover-screw level with the bone crest. The raised flap is then repositioned and sutured to conceal the cover-screw and the implant (Figure 3). After a few months, the second stage surgery is carried out. In this stage, the implant site is re-opened, the cover-screw is accessed and then replaced with a healing abutment, which is also known as a sulcus former or transmucosal abutment (Figure 4). Afterwards, the healing abutment is replaced with a provisional or final restoration. This surgical protocol is suitable for use when the quality of bone is not optimum and when bone graft materials are used in conjunction with the implant. Examples of an implant system used for the two-stage procedure include the Fixture MK III® (Nobel Biocare, Uxbridge, UK), MAX 2.5® Implant (Bicon Inc, Boston, MA, USA) and OSSEOTITE® 2 Certain Implant (BIOMET 3i, Maidenhead, UK).
Figure 4. An image of a cover–screw (left) and healing abutments (middle and right)
It is important to mention that the cover-screw is used to prevent tissue growth into the implant or over its platform. It is attached to the implant using a screw-driver with a light finger force. It is essential to confirm that the cover-screw is fully seated and no gap is left between the cover-screw and the implant platform. The cover-screw has a low profile which facilitates the suturing procedure and allows the two edges of the cut mucosa to be brought close together without undue tension. If there is too much tension, it may deteriorate and preclude the healing.23 Conversely, the healing abutment has a high profile and protrudes through the peri-implant mucosa to the oral cavity. Therefore, the healing abutment is available in different lengths, depending on the distance between the implant platform and the surface of the peri-implant mucosa. It is also available in a variety of diameters, which is selected according to the implant diameter. The cover-screw and the healing abutment are shown in Figure 4.
Implant stability
Implant stability (lack of mobility) is divided into primary and secondary. The primary, also known as initial stability, is achieved during implant placement surgery. It is believed that primary stability plays a vital role in reaching osseointegration, upon which secondary stability depends.
Implant stability is produced by close contact between the implant and the host bone. The factors that may affect primary stability may be categorized into three factors; those related to surgical site (local) or related to implant or surgical method used in placement of the implants. Local factors, such as bone quality and volume, may affect the degree of bone-to-implant contact and consequently affect primary stability. As an example, larger bone-to-implant contact fractions were observed in bone sites of higher density. The implant factors include shape, length, diameter and surface texture. For instance, tapered implants lead to higher insertion torque values than cylindrical implants, which was considered to be due to the greater frictional surface of the tapered implants and associated with high primary stability (see below). A surgical technique, such as that which leads to bone condensation during implant placement surgery or a mismatch between the osteotomy and implant diameter (with the implant diameter being slightly greater than the osteotomy), results in satisfactory primary stability.24 Also, the use of implants with self-taping blades results in a lower primary stability in medium-density bone when compared with those without such blades.25 However, this issue is contradictory.
Secondary stability represents integration of the implant as a result of new bone formation through its remodelling.2627,28 Therefore, this stability depends on bone activities and factors that influence such activities throughout the patient's life.27 The general consensus is that peri-implant bone is in a continuous active remodelling state which maintains osseointegration and provides secondary stability.27,28,29
It is important to mention that, when the implant is inserted into the host bone, spaces may exist in the bone-implant interface. These spaces are initially filled with blood that comes from injured blood vessels, forming a fibrin network which is the important step towards the formation of osseointegration.
Dental implant types
In the worldwide market, there is a wide range of dental implant systems available, but only a few brands are American Dental Association (ADA) approved. The most commonly used implant systems include Nobel Biocare, Straumann, AstraTech, Bicon, BioHorizon, BIOMET 3i, Intralock, and Zimmer. All are constructed on the same basic concepts but there are differences in the patented technology and materials.
In general, dental implants may be classified as a one- or two-piece implant.
The one-piece implant
In the first type, the implant and the abutment are formed as a single solid unit. In this case, there is no screw-joint between the implant and the abutment. The lack of a screw-joint is considered an advantage as there is no screw-loosening, dangerous fracturing or micro-motions between the abutment and the implant. The one-piece implants may be used when narrow implants are indicated, such as in the replacement of the maxillary lateral incisors and lower incisors, or when bone volume is limited and the use of standard implants is not suitable. These types of implants are installed only with the one-stage implant placement method. Examples of a one-piece implant are the one-piece 3.0 Dental Implant® (BioHorizons) and Y-TZP Ceramic Implant® (Nobel Biocare).
The two-piece implant
The two-piece implant type consists of an implant to which an abutment or a restoration/attachment is connected, usually with a screw. It is more commonly used than the one-piece implant type. With this implant type, both the one- and the two-stage implant surgery protocol can be implemented.
Angled implants in which their coronal part is angled in relation to the main implant body are also available. These angled implants are useful in the anterior region when placing non-angled implants in their optimum position is not possible. An example of angled implants is the Co-axisä implant (the Southern Implants, UK) in which the neck is at an angle to the long axis of the implant body. It is useful to use when the long axis of a prospective implant is not along the long axis of the potential restoration. An angled abutment, such as Regular Neck synOcta® angled abutment (Straumann), is also available and can be used to overcome angle mismatching problems.
Implants are also available as hollow and solid. Hollow implants allow more contact with bone but are weaker than solid implants, which makes them more susceptible to mechanical failure and fracture. An example of a hollow implant is the Hollow Cylinder Implants® made by Straumann and ITI (Basel, Switzerland).
Irrespective of the implant type and for descriptive purposes, the implant usually consists of an implant body and neck. The implant body is the part of the implant that is buried in the osteotomy. The coronal part of the implant is denoted as the neck, through which the abutment/attachment is connected to the implant. The coronal part may be smooth (one- and two-piece) and placed above the crest of the bone, or roughened (two-piece), in which the platform is usually placed below or level with the crestal bone. When the coronal part is smooth and placed above the crest of the bone and penetrates peri-implant mucosa, it is known as the transmucosal part. The surface of the transmucosal part is usually highly polished and is available in different lengths. It may also have a straight or a bevel profile and may be augmented with micro-grooves in order to optimize healing around the implants.
Placing the smooth (machined) part of the implant below the bone crest may lead to its resorption.29 However, fewer crestal bone changes were observed when the smooth part was located above the crestal bone level, irrespective of the implant type; one- or two-piece implants.29 Accordingly, it has been recommended that the smooth-rough border should coincide with the alveolar bone crest.29
Features to consider when choosing an implant system
Five features can be used to describe the dental implant body: shape, surface macro- and micro-structure, length and diameter. These features are important when an implant system is chosen.
Shape (geometry)
Implant shape may generally be tapered or parallel (straight-walled). The tapered type in general has more primary stability than the parallel type.30 The use of tapered implants results in lateral compression of bone and increased stiffness of the interfacial bone, which is reported to increase the implant primary stability.13 Tapered implants were found to require a higher insertion torque and less insertion time than parallel implants. A higher insertion torque gives a better implant primary stability.31 Tapered implants are also used to avoid damaging the converging roots of adjacent teeth that bind the edentulous space and in softer bone, such as type IV (Figure 2), where primary stability is not always easy to achieve.32 They may also be used immediately or early after tooth extraction.32,33 The use of a tapered implant with a wide platform achieves a satisfactory emergence profile of the restoration.
Surface macro-structure (threads)
The implant macro-structure is represented as threaded or non-thread (thread-less). The threaded type is the most commonly used implant design. The threads are usually incorporated into the implant design to improve the initial stability and dissipate interfacial stress in a more favourable way. As the threaded implants provide better mechanical and biological outcomes, non-thread implants, such as cylinder (press-fit) implants, are less likely to be used and are replaced by the threaded type. Thread features such as thread depth, thread thickness, face angle, pitch and helix angle are considered to be factors that determine the functional thread surface and affect the biomechanical load distribution of the implant.
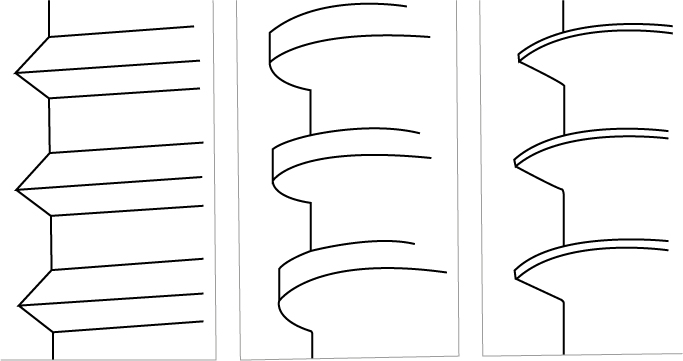
There are three thread shapes which are most regularly used when a dental implant is described (Figure 5). These are V-shaped, square-shaped or reverse buttress.34,35 An animal study conducted by Steigenga and colleagues36 revealed the effects of thread type on peri-implant bone formation. The study showed that implants with a square thread design had significantly more bone-implant contact and greater reverse-torque measurements than observed when the V-shaped and reverse buttress thread designs were tested.
Figure 5. A representation of the most commonly used implant threads: V-shaped thread (left); square thread (middle) and a reverse buttress (right).
A threaded implant may also be classified as a self-taping or pre-taping implant.37 A self-taping implant is an implant which is designed to make its own threads as it is being placed into the prepared osteotomy. On the other hand, in pre-taped implants, threads are prepared on the surface of the osteotomy using a tap drill (taper). The produced threads will accommodate the threads of the implant. The pre-taping method is sometimes recommended, such as in the case of dense bone (type I and II) (Figure 2). However, pre-taping implants achieved lower primary stability than the self-taping implants.38
Surface texture (micro-structure)
Implant surface texture describes the roughness of the implant surface. Therefore, the implant surface is either smooth (machined) or can be of a variety of roughness. A rough-surfaced implant has a larger surface area than that of its counterpart smooth implant. It is found to be associated with positive healing of peri-implant tissue and encourages the formation of osseointegration.39 The increase in surface area distributes forces to which the implant is exposed in a more favourable manner. It also provides better primary stability than that attained when the implant surface is smooth.40 Histomorphometric and removal torque studies with roughened implant surfaces have revealed greater bone apposition41 and higher removal torque values than implants with smoother surfaces.42
In general, two methods for the alteration of implant surface texture have been described in the literature: subtractive and additive methods. In the subtractive method, the implant surface is roughened by removal of its surface materials usually by blasting and/or acid etching.42,44 In the additive method, a biocompatible material, such as titanium or hydroxyapatite, is added to the surface42 (see below). Some examples of rough surface implants include: grit blasting with titanium oxide produced by Astra Tech (Mannheim, Germany); Sand-blasted Large-grit Acid-etched (SLA®) implants from Straumann (Basel, Switzerland); Acid-etched Implants® from BIOMET 3i (Florida, USA); and Plasma-sprayed® (molten titanium sprayed on the implant surface) produced by Straumann and Dentsply Sirona Implants (Weybridge, UK).
It is important to note that, if the rough implant surface is exposed to the oral environment, it may encourage plaque accumulation and interfere with its removal, and subsequently may induce peri-implant disease (see below).6,45
Implant length
Implant length is determined by the distance between the top surface of the implant platform and the apex. In general, the length of the standard implant ranges from 7–18 mm.33 Selection of an implant of the required length is governed by the available vertical bone height, width and quality which will accommodate the implant (Figure 6). As implant primary stability is a function of contact between the implant surface and bone, the longer the implant, the greater the surface contact and primary stability. However, the increase in implant stability does not occur linearly to the increase of the implant length. For instance, a 10 mm implant has about 30% more surface area than a 7 mm implant, while a 13 mm implant has 20% more surface area than a 10 mm implant.46
Figure 6. Bone resorption at alveolar crest occurs after tooth extraction which may preclude the use of a long implant as the crestal bone has to be trimmed down to maintain at least one millimetre of bone buccally and lingually at the bone crest region.
The bone of the edentulous ridge may not be sufficient for placing an implant with the optimum length. Therefore, several techniques have been suggested to compensate for the deficiency in the residual ridge, either before or simultaneously with implant placement. Among these methods are guided bone regeneration, block grafts, sinus lifting procedures, inferior alveolar nerve repositioning methods, and bone distraction.47 These surgical methods are successful and can be used to increase bone height.47 However, they are not without risks and may lead to several complications and undesirable treatment outcomes.5,47 This may encourage the dentist and patient to avoid such surgical methods and to use short implants, therefore the implant is installed with less invasive surgical procedure and the cost is reduced. Nevertheless, when a short implant is used, factors that affect the osseointegration, such as implant shapes, surface texture, and thread designs, should be carefully selected to achieve a satisfactory long-term outcome.47,48 However, earlier studies have reported that shorter implants are unpredictable and fail more frequently than longer implants.46,49 In addition, longer implants had statistically higher survival rates when compared with shorter implants.50 For instance, it has been reported that survival rates after two years were 93.1% for 5 mm implants and 98.6% for 9.5 mm implants.51 Furthermore, short implants may fail at an earlier stage than standard implants,20 as peak failure rates of short dental implants were 4–6 years, and 6–8 years for the standard implants.52
It is important to note that bone resorption following tooth extraction may result in the thinning of the alveolar bone crest, which may preclude placement of an implant with an adequate length and diameter, as shown schematically in Figure 6. Therefore, bone mapping and a CT-scan or Cone-Beam Computed Tomography may be required.
Implant diameter
The implant diameter is measured from the crest of the widest thread to the same point on the opposite side of the implant.53 According to the diameter, implants may be classified as mini when diameter is ≤2.7 mm; narrow when the diameter is >2.7 mm but ≤3.75 mm; regular when it ranges from 3.75–5 mm; and wide when the diameter is >5 mm.
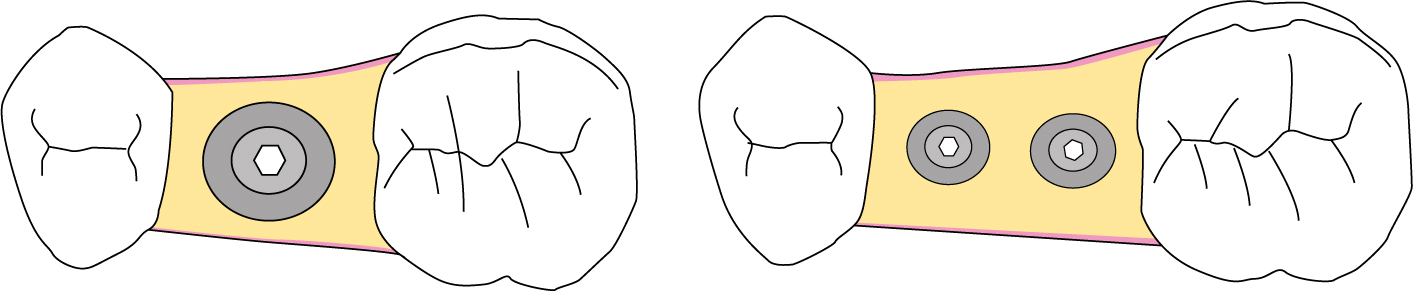
The implant diameter plays an important role in the success of oral implants and has a major impact on the implant's ability to withstand occlusal load.54 Selecting an implant of a suitable diameter is governed by the dimensions of the edentulous space (bucco-lingual and mesio-distal) (Figure 7), as well as the bone quality. Moreover, it is also affected by the type of tooth being replaced.
Figure 7. The implant should be placed in the site that was previously occupied by the tooth being replaced, and surrounded by an adequate amount of bone. Two implants may be used to replace a molar tooth, which results in the dissipation of the occlusal forces in a satisfactory manner (right).
An increase in the diameter of an implant is associated with an increase in its surface area. For instance, increasing the diameter in a 3 mm implant by 1 mm increases the surface area by 35% over the same length.55 Also, a 3.75 x 10 mm implant has 61% less surface area than a 6 mm diameter implant of the same length.33 Furthermore, an increase in the diameter and a change in the threads may lead to an increase in the implant surface area of more than 300%. This increase in the surface area may lessen stresses to the crestal bone areas and reduce both crestal bone loss and early loading implant failure.55
It is important to mention that, when the implant is installed, it should be in close contact with the surrounding bone of not less than 1 mm thickness on its buccal and lingual surface, and preferably 1.5 mm or more between the implant surface and its adjacent tooth (Figure 7). For instance, when an implant of 4 mm is selected, the bucco-lingual and mesio-distal dimensions of the edentulous space should be a minimum of 6.0 and 7.0 mm, respectively. However, it has been suggested that, in the aesthetic zone, maintaining a minimum of 3 mm of bone between adjacent implants is beneficial, as bone height as well as the inter-dental papilla are more likely to be maintained.11 Consequently, implants with a smaller diameter at the implant-abutment interface may be used when multiple implants are to be placed.11
The diameter of the roots is usually estimated at 2 mm apical to the cemento-enamel junction. With this measurement, an implant with a diameter that matches, or is slightly smaller than, the tooth being replaced is selected. In order to obtain a restoration with an optimal emergence profile, the implant platform is usually placed at about 2 mm apical to the cemento-enamel of the adjacent teeth. If an implant is placed deeply below the crest of bone, the crown height is increased, which may lead to mechanical failure of implant components and compromise aesthetic treatment outcomes. When the implant is placed more superficially, restoration may be deemed impossible and aesthetic treatment outcome is also compromised.33
When a molar tooth is replaced, the use of two implants may be an option, as dissipation of occlusal loads are favourable. However, placement of implants close to each other is associated with difficulty in obtaining an optimal emergence profile, interferes with oral hygiene and leads to chronic inflammation and bone resorption.
Short and wide implants may be used to compensate for the decrease in the vertical bone height of the edentulous space when surgery cannot be considered. They may also be used when the quality of the bone bed is not optimal.56 Wide implants can be used to increase implant stability,57 thus improving stress distribution within the surrounding bone.47 Furthermore, the use of a wide diameter implant may reduce the stress on the retained screws. Wide implants are also used for the replacement of posterior teeth and immediately after tooth extraction (Table 1).58
Several situations do not allow the use of wide diameter implants59 and narrow implants are an alternative. For example, narrow implants are suitable for replacing maxillary lateral incisors and mandibular incisors. They are also suitable when bone quantity is insufficient, or when the roots of adjacent teeth are converging. They may also be used with a removable implant-supported overdenture. However, the use of an implant with a small diameter is not without disadvantages, such as mechanical failure of the implant component. Furthermore, obtaining a good emergence profile of the restoration may also be a problem. Hence, a detailed examination of each patient's condition should be taken before a specific implant is selected, and alternative treatment options, such as a fixed (conventional or resin-bonded) prosthesis, may be considered.
It is important to distinguish between the implant diameter and platform diameter as they may not be equal. The implant platform represents the part of the implant that is connected to the prosthetic (abutment) counterpart. Table 3 displays examples of implant features that should be considered when an implant is selected.
Implant length: a long implant should be considered whenever the condition permits.
Implant diameter: ideally, the implant should be approximately the same diameter as the root of the tooth it is replacing.
Wide implant:
Poor quality bone;
Limited ridge height with adequate mesio-distal and bucco-lingual width; and
When it is not possible to achieve good emergence profile with a wide implant body; and
Converging adjacent tooth roots.
Tapered implant:
In type IV bone, where primary stability is difficult to achieve;
Narrow or concave bone;
Converging adjacent roots; and
Immediate and early implant placement.
Implant materials
The most commonly used materials in dental implants are either bio-inert, such as commercially pure titanium (Cp Titanium) and titanium alloy, or bio-active ceramics such as hydroxyapatite, tri- and tetra-calcium phosphate and bio-glass.18
For more than five decades, titanium was the most commonly used material in dental implants due to its bio-compatibility, as well as its mechanical and physical properties, such as resistance to corrosion, high strength and low weight.60 Depending on its oxygen content, Cp titanium may be categorized into four grades; grade I contains the least oxygen while grade IV contains the most (0.18% versus 0.4%).18 Titanium alloy consists of 90% titanium, 6% vanadium, and 4% aluminium and is classified as grade V.34
Titanium is a non-noble metal which has the ability to form a very adherent self-repairing and protective surface oxide layer, which prevents further titanium corrosion. This layer forms immediately when the titanium is exposed to oxygen. The formed oxide layer on Cp titanium is similar to that which is formed on titanium alloys.34 Titanium dioxide (TiO2) forms the main constituent of this oxide layer, however, other oxides, such as Titanium oxide (TiO) and Titanium pentoxide (Ti2O5) may also exist. Incorporation of other chemical elements, such as carbon, traces of nitrogen or chlorine, into the oxide layer have been reported.61
The release of metallic ions from the titanium implant surface may occur and increase as the implant surface area increases.62 It has been suggested that ionic release may interfere with the normal peri-implant bone mineralization and remodelling, which could lead to the failure of the implant.63 Furthermore, titanium release may induce hypersensitivity in susceptible patients, which may have an undesirable impact on implant success.64 However, this issue is still debatable and more clinical and further laboratory investigations are required.24,64 Nevertheless, available literature indicates that Cp titanium has a long-term successful performance. In addition, the surface of the titanium implant, which was previously contaminated in the peri-implantitis case, was found to reintegrate with bone which was treated to remove the contaminant.65,66,67
Cp titanium and titanium alloys can make up the entire implant or can be used as a substrate to which a coating of bio-active material, such as hydroxyapatite, is attached.
To speed up the healing process and osseointegration, implant surfaces are coated with ceramics.68 The ceramics may be bio-active, such as calcium phosphates, or inert, such as aluminium oxide and zirconium oxide. Examples of calcium phosphate coating materials are hydroxyapatite and fluorapatite.68 The bio-active ceramics are reported to act as osseoinductive materials which encourage and accelerate bone apposition around the implants. Furthermore, coatings that have similar properties to that of the extra-cellular matrix provide a favourable environment for osteoblasts, osteoclasts and their progenitor cells, that are responsible for the healing of bone.69 Therefore, an early and strong implant stability is achieved and the risk of implant failure is reduced.69
Ceramics are initially used in the additive methods in which ceramic coatings are added to the metal implant. However, high bond strength between the coating material and the substrate is required to withstand functional stresses and to avoid fragmentation of the coating materials.70 It is found that hydroxyapatite mechanical failure occurs primarily at the interface between the metal substrate and hydroxyapatite coat (adhesive failure), irrespective of the implant design. This may have a negative effect on implant osseointegration.71 Nevertheless, the risk for hydroxyapatite-coat degradation and loosening (delamination) are still a remaining concern.
With improvement in technology, ceramic materials are extended for use as implant substrates. This is because ceramics such the yttrium-stabilized tetragonal zirconia polycrystalline has improved mechanical properties, superior wear and corrosion resistance, with a high flexural strength. These characteristics may make them a potential alternative to conventional titanium implants for supporting overdentures.72 Three types of zirconia-containing ceramic systems are most commonly used in dentistry; yttrium-stabilized tetragonal zirconia poly-crystals, alumina-toughened zirconia and zirconia-toughened alumina. However, these non-metallic materials are expected to replace Cp titanium and its alloys.73 Nevertheless, based on their systematic review of literature, Andreiotelli and colleagues74 concluded that ceramic, in particular zirconia, implants are not yet suitable as an alternative to titanium implants. Nevertheless, they potentially could be a successful material for use in implants, but this has not yet been supported by clinical investigations.75 However, ceramics such as zirconia are used nowadays as abutments and crowns as they have good clinical outcomes.73
It is not unreasonable to conclude that the prospective implant should be selected carefully and a restorative driven approach should be implemented to avoid an unwanted result.76 Thus, thorough investigation should be carried out to guarantee the best possible outcome. The edentulous area should be viewed in three dimensions: mesio-distal, bucco-lingual and corono-apical. The mesio-distal dimension of the edentulous space should also be thought of as two interrelated spaces (inter-radicular and restorative). The inter-radicular space holds the implant and can be found between the roots of the two adjacent. Hence, a precise radiograph image of the area is important. The restorative space should be carefully investigated as it extends between the two adjacent teeth and accommodates the prospective restoration.
Abutment-implant connections (interfaces)
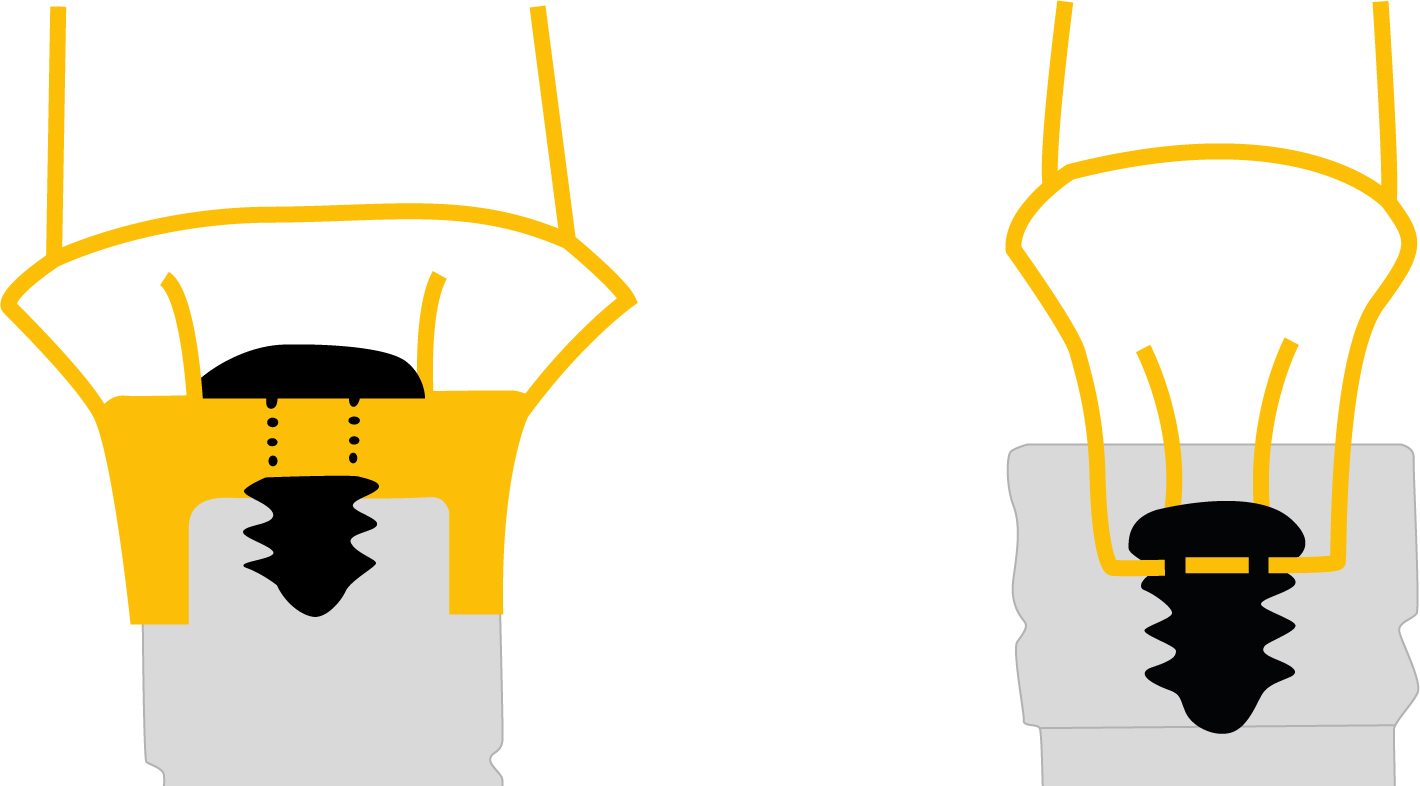
When an implant is put to function, it is connected with the restorative/prosthetic components. The connection type can be classified as internal or external. In the internal connection systems, the apical part of the abutment is inserted into an access hole in the implant platform. In the external systems, a protrusion located above the implant platform is inserted into a recess in the apical part of the abutment (Figure 8). The connection is also classified as a slip joint; when there is a space between opposing mating surfaces, and a friction fit when such space does not exist. The connection may be further categorized as a bevel (conical) joint or a butt joint (Figure 8).
Figure 8. A schematic representation of the screw-joint connections: the external connection and the butt joint (left) and the internal connection and the slip joint (right).
The connection may have an anti-rotational component, such as hexagonal, octagonal, cone hex, cylinder hex, cam tube and pin/slot or be without an anti-rotational device, such as a cone (Morse taper). The function of the anti-rotational component is to stabilize and prevent abutment rotation.77,78 Likewise, the connection usually has a screw but is sometimes screw-less and relies entirely on the friction fit for its stability, such as Bicon® dental (Bicon Inc, Boston, MA, USA).
The first implant connection type used with a dental implant was described by P-I Brånemark.12 It was an external hex, therefore consisting of six sides, each two adjacent sides make a 60-degree angle and had a height of 0.7 mm. The hex was originally used to carry and insert the implant into the prepared host bone (osteotomy). The hex was not aimed for use as an anti-rotational device, as the implants were mainly used to restore completely edentulous dental arches with implant-supported overdentures with multiple implants. Consequently, rotational displacement of the overdenture was not an issue. However, as the use of dental implants progressed and extended for use in replacing single and multiple missing teeth, the use of a guiding index and an anti-rotational device is needed. To fulfil this requirement the original external hexagonal connections were modified and are now available in different heights including 0.9, 1.0 and 1.2 mm and with various sizes. Furthermore, several types of internal connections were also introduced and are widely used nowadays.
In general, when the connection is an internal type, the occlusal load is usually dissipated through the implant body and the screw is more likely to be protected from the imposed load. Loose screws were reported to occur less frequently with internal connections than with external ones.79 However, the implant neck should be strong enough to resist such loads. Nevertheless, when the internal connection is used with a narrow implant, the connection is exposed to vertical or oblique loads. Although the screw itself may be protected from loading, the implant neck may not be able to resist such a load and will mechanically fail80.81 as most of the occlusal forces are transferred to the implant walls.81
Screw-joint
When the implants and the restoration/prosthesis are connected together by a screw, the connection is known as a screw-joint.16,77,82 For example, when the single restoration (crown) is screw-retained, one screw-joint is usually found to connect the restoration to the implant. When the restoration is cement-retained, there is also one screw-joint, but it is between the abutment and the implant (see below). The screw-joint is also found with the fixed implant-supported prosthesis in a similar way as that described for the cement- and screw–retained single implant-supported restoration. In the fixed implant-supported overdentures (FISOs), there is a screw-joint between the frame-work and the implants, whereas in the removable implant-supported overdentures (RISOs), there is a screw-joint between the attachment system and the implant.6,16The attachment systems are discussed later in the article. In some situations when a screw-retained restoration is used, there may be two screw-joints: one between the implant and the abutment, and one between the abutment and the restoration/prosthesis.
When the screw is tightened, there are two opposing forces that act on the implant platform and the abutment or restoration/attachment that form the joint. One of these forces tries to hold the joint together and is known as the clamping force. The other force is called the separating force as it tries to disengage the screw-joint components away from each other. Hence, the two forces are acting against each other. As a tightening torque is applied to the screw, a tension (pre-loaded) is generated in the screw. Consequently, the screw shank and threads are tense and an elastic recovery is generated, thus creating the clamping force between the mating surfaces.16,77,82
To obtain an effective clamping force, the tension created in the screw material should be less than that of the material's elastic limit (Young's modulus) so no permanent plastic deformation or screw fracture occurs. Maximum screw-joint stability can be achieved with a maximum pre-load when the proportional limit of the screw is approached. Thus, to obtain this, the applied torque should be 75% of the torque required to cause screw permanent deformation. In order to hold the implant components together, a maximum clamping force and a minimal separating force are required. Therefore, the clamping force overcomes the separating force.
Factors affecting screw-joint stability
Lack of screw-joint stability is reflected in loosening of the screw. It is considered as one of the most common problems associated with the use of implant-supported restorations.83 One of many factors that play a role in the stability of the screw-joint is the friction coefficient of the materials used in the fabrication of the implant components, such as the abutment, implant and screw. The friction coefficient has an effect on the generated pre-loading. Tightening torque and consequently the developed pre-load is inversely affected by the friction between the mating surfaces.84 In general, during screw torqueing, friction occurs between the implant surface and the opposing abutment surface, between the head screw and the abutment surface and between the screw threads (male) and the implant threads (female). As such, when a screw is tightened, only 10% of the torque is converted into screw pre-load, while the other 90% of the tightening torque is lost as friction.84,85In order to maximize pre-loading, the friction between mating surfaces should be reduced. This can be achieved by coating the mating surfaces with other materials, such as carbon film or the screw with tungsten carbide. This process is known as dry lubrication and the coating material is denoted as a dry lubricant. Both carbon and tungsten carbide coatings were reported to reduce the friction coefficient and improve pre-loading.84Torq-Tite® abutment screws (Nobel Biocare, Uxbridge, UK) are made of titanium alloys and are coated with a carbon layer and Gold-Tite® abutment screws (BIOMET 3i) are titanium screws with a gold-plated surface. Both screw types were found to be associated with lower friction coefficients and greater pre-load values than the conventional gold alloy and titanium alloy screws.86 Likewise, higher pre-loads were associated with gold-coated screws when compared with that obtained from screws made of uncoated gold or titanium alloy for all insertion torques, as well as when the screws were re-tightened.87
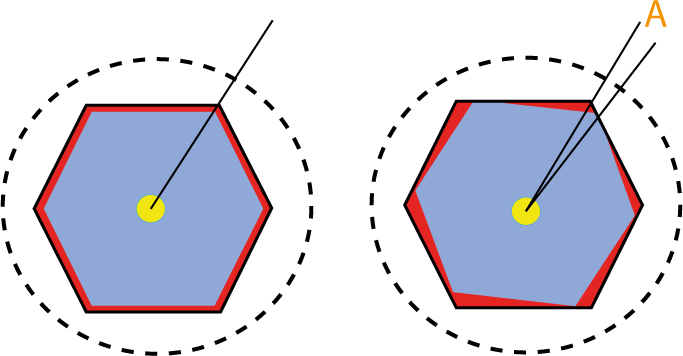
Manufacturing tolerance is another factor that affects the screw-joint stability. It is defined as unplanned deviations from the theoretical dimension of the shaft and its mating recess as some deviations from a perfect fit are expected, but not planned. Hence, this indicates an insignificant value of misfit between the matting surfaces. This misfit allows for what is known as rotational freedom (play) to occur. The rotational freedom is calculated by the formed angle between the clockwise and anti-clockwise rotation of the anti-rotational components of the screw-joints (Figure 9). The rotational freedom may vary from 1.6 to 5.3 degrees.88 The most stable and predictable screw-joint may be expected when the rotational freedom is lower than two degrees.89 Hence, the produced rotational freedom affects the stability of the screw-joint.
Figure 9. Measurement of rotational freedom. A passive fit of the abutment (blue) into a recess (hexagonal) in the implant platform (a dotted circle). The space between the two components is represented by the red area. The rotational freedom degree during abutment rotation is indicated by the letter ‘A’.
Furthermore, the presence of a micro-roughness on the implant and abutment mating surface, which is worn away as a result of screw torqueing, leads to what is called settling (embedment relaxation). Consequently, part of the clamping force is lost and the screw becomes loose. The mean loss of pre-load may be up to 40% of the original pre-load value 15 hours after screw torqueing.90 To reduce the settling effect, it has been suggested that the implant screws should be retightened ten minutes after the initial torque application as a routine clinical procedure.91.92 All screw types were reported to display some decline in pre-load with repeated tightening. This decline occurs irrespective of the insertion torque and abutment type.87 As screws lose pre-load following placement, their re-tightening is required from time to time during the restoration's life.
The screw pre-load should be high enough to maintain the joint integrity and reduce the possibility of the screw loosening and fracturing.93 However, when excessive torque is applied, slippage between the screw threads (male) and the implant internal threads (female) occurs, which consequently leads to screw loosening.94 Inversely, too little torque or a lower torque value which cannot produce the required screw pre-loading needed to hold the mating surfaces together exhibits greater micro-motion at the screw-joint,95 which consequently causes screw loosening and may lead to its fatigue and fracture. Therefore, it is vital to use the manufacturer's recommended tightening torque, which should be within the elastic range of the screw's materials, as mentioned earlier.96,97 It is also essential to ensure consistent tightening torque values are applied. Therefore, torque gauges (control) should be used and manual torqueing should be avoided.91 It is also important to calibrate the torqueing devices to obtain consistent torqueing.98
Torqueing the screw should be carried out carefully and a counter-torque device should be used to avoid disturbing the osseointegration. Hence, the use of a counter-torque device is recommended as it reduces transmission of the tightening torque to the implant-bone interface. On average, about 90% of the recommended pre-load tightening torque is transmitted to the implant-bone interface when the counter-torque device is not used. This value is reduced to only 10% when the counter-torque device is used.94
Overloading of the restoration may lead to screw loosening and failure. Therefore, the occlusion should be adjusted and occlusal forces should be directed along the long axis of the implant, whenever possible (Figure 10). This can be achieved by construction of a restoration in which its occlusal morphology is constructed according to the mechanical principals that favour this concept. For instance, the cuspal inclination should be flattened and the incisal guidance made shallow to avoid bending moments caused by the lateral component of the occlusal forces.99 The occlusal table of the prospective restoration may be reduced by 30–40% of the tooth being replaced (Figure 10) and cantilevering the restoration should be avoided. Use of an occlusal splint is recommended for patients with parafunctional habits such as bruxism. The implant should be placed in the site that was previously occupied by the tooth being replaced, and surrounded by an adequate amount of bone (Figure 7). It should also be oriented along the long axis of the tooth being replaced and within the occlusal table. However, when a molar tooth is replaced, the use of two implants may be considered in order to dissipate the occlusal loads satisfactorily, as mentioned earlier (Figure 7).
Figure 10. An intra-oral radiograph showing a single implant-supported crown replacing the right second molar (a). The cuspal inclinations are lowered and flattened, but the occlusal table is widened which creates a cantilevering effect and exposes the restoration, the screw and the implant to high tipping forces that may lead to their mechanical failure. A diagram of an implant-supported restoration; the implant is oriented so occlusal loading is directed along its long axis (b).
Some of the other factors that may affect the screw-joint stability are displayed in Table 4.
Implant-abutment interface design/type.
Rotational freedom (misfit).
Manufacturing allowances (tolerance).
The settling (embedment).
Repeated opening and closing of the screw.
The applied torque value: over and under torqueing the screw.
Loading of restoration.
Prefabricated metal- and costume-made cylinders.
The casting process:
Casting alloy;
Investment; and
The finishing/polishing method.
Screw design and materials:
Shank or shank-less screws (a shank-less screw is usually less resilient than that with a shank);
Shape and diameter of screw's head;
Materials from which a screw is made of such as gold, titanium and gold-coated screws.
Platform switching concept
This concept was based on clinical observations where the implant platform diameter was wider than the abutment.100 It is assumed that, when this principle is used, the crestal bone loss after implant placement is less than when the implant platform and the abutment pose a similar diameter.100 This concept is theoretically explained on the bases of moving the micro-gap between the platform and the abutment inward from the outer edge and consequently away from the bone.101 It also results in an increase in horizontal soft tissue dimension, which may protect the bone crest and limits its resorption.102 It also shifts the stress between the implant and abutment away from the cervical bone-implant interface, which may also help in maintaining the crestal bone level.
A recent meta-analysis,102 including 13 human randomized clinical trials (RCTs), has shown a significantly less mean crestal change at platform-switching implants, compared with when the implant platform dimensions matches the abutment (0.49 mm versus 1.01 mm). However, the use of platform-switch did not preserve the crestal bone better than when the switching concept was not used, when thin mucosal tissues on crestal bone were present.103 Furthermore, the stress within the screw-joint was found to increase when the platform-switching concept is implemented. This may lead to failure of the screw-joint connection.104,105 Therefore, this concept should be used with substantial care.
Types of restorations/prostheses for missing teeth
Implant-supported restorations (prostheses) may be used to replace a single or multiple missing teeth, as well as completely edentulous mandible and maxilla. Therefore, when a patient whose missing teeth were replaced with an implant-supported restoration attends the dental clinic, one of the following restoration/prosthesis is usually present:
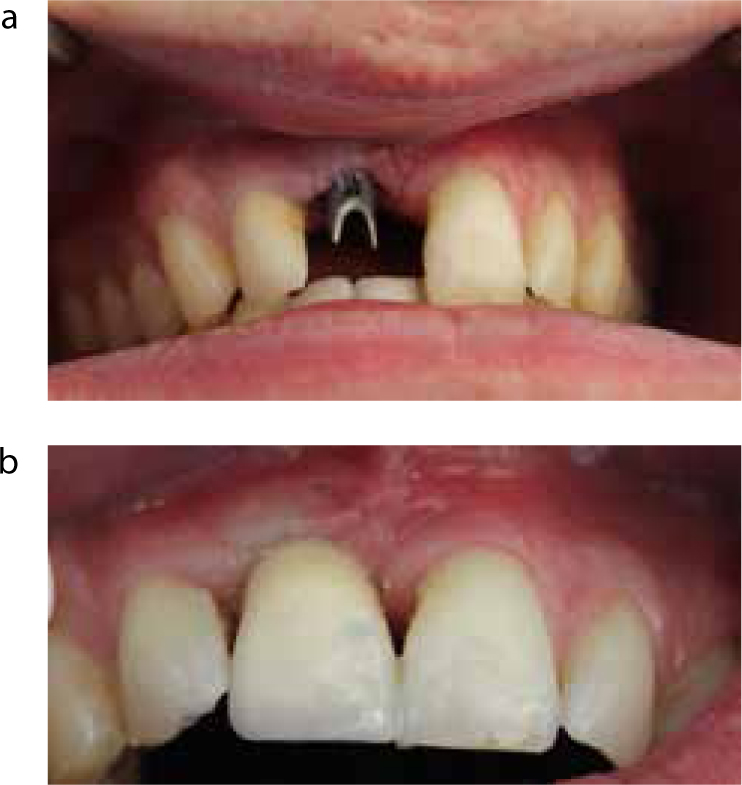
An implant-supported single restoration (crown) (Figure 11);
A fixed implant-supported prosthesis;
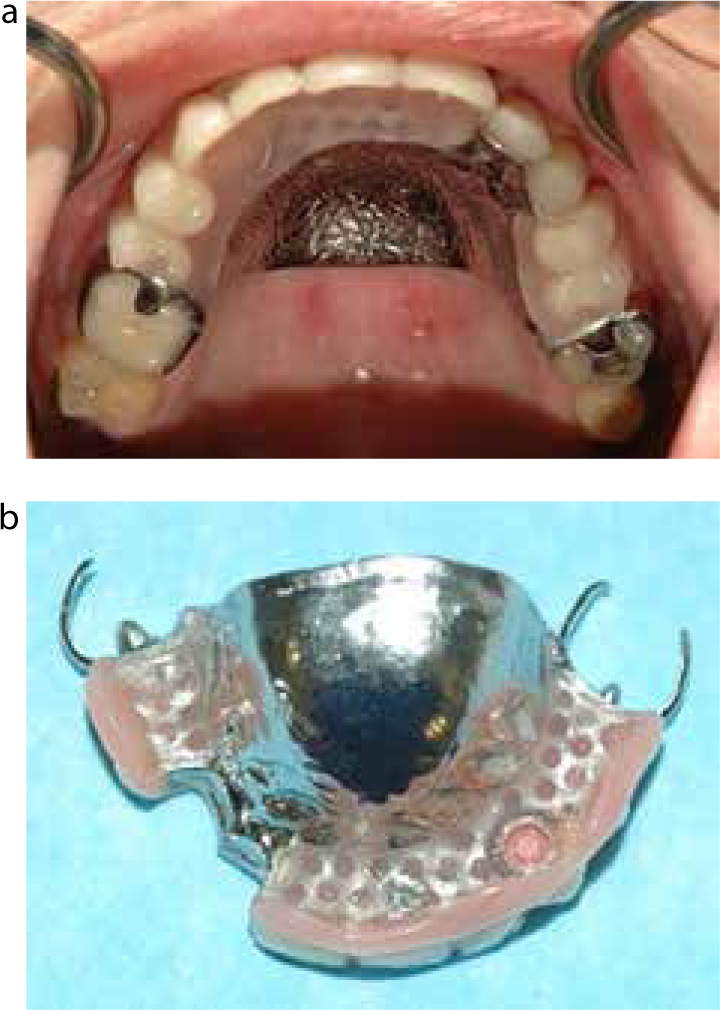
A removable implant-supported partial denture (Figure 12); and
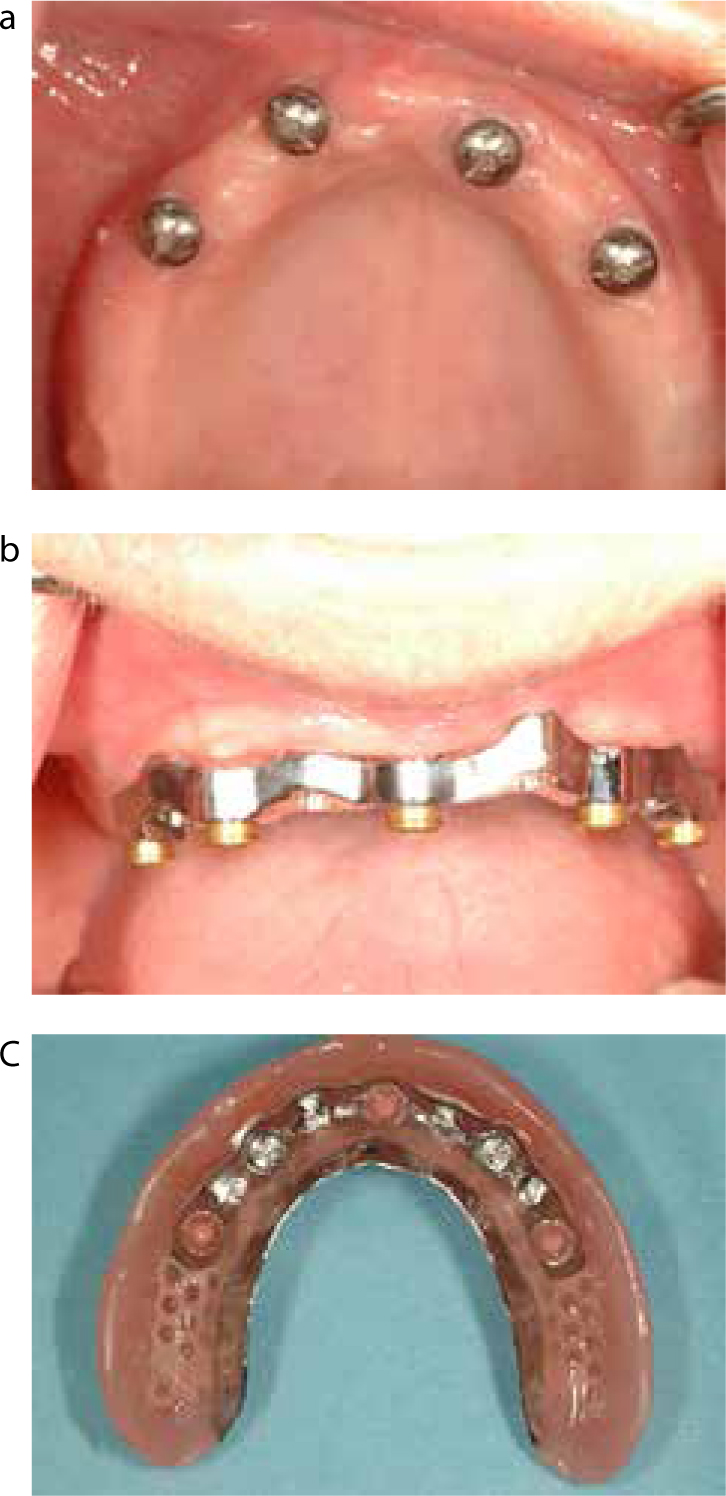
A fixed or removable implant-supported prosthesis (overdenture) (Figure 13).
Figure 11. A clinical image of a missing upper right centre incisor replaced with a single cement-retained, implant-supported crown. The abutment (a) and the restoration (b) is made of porcelain fused to metal. The papilla failed to fill the inter-dental space on the mesial and distal aspect of the restoration. This may have a negative effect on the aesthetic outcome if the patient has a high lip-line.Figure 12.
(a, b) Clinical images of multiple missing maxillary teeth restored with a partial denture, which gains its support/retention from the teeth and alveolar ridge, as well as from an implant placed in the right canine region. The fitting surface of the denture shows the patrix of a locator attachment.Figure 13. Clinical views of an upper edentulous maxilla restored with a RISO. (a) Four dental implants placed in the anterior region. (b) The implants are connected with a CAD/CAM designed and fabricated bar. Four locator attachments (matrices) are attached to the bar. (c) The fitting surface of the RISO showing the patrices of the attachment.
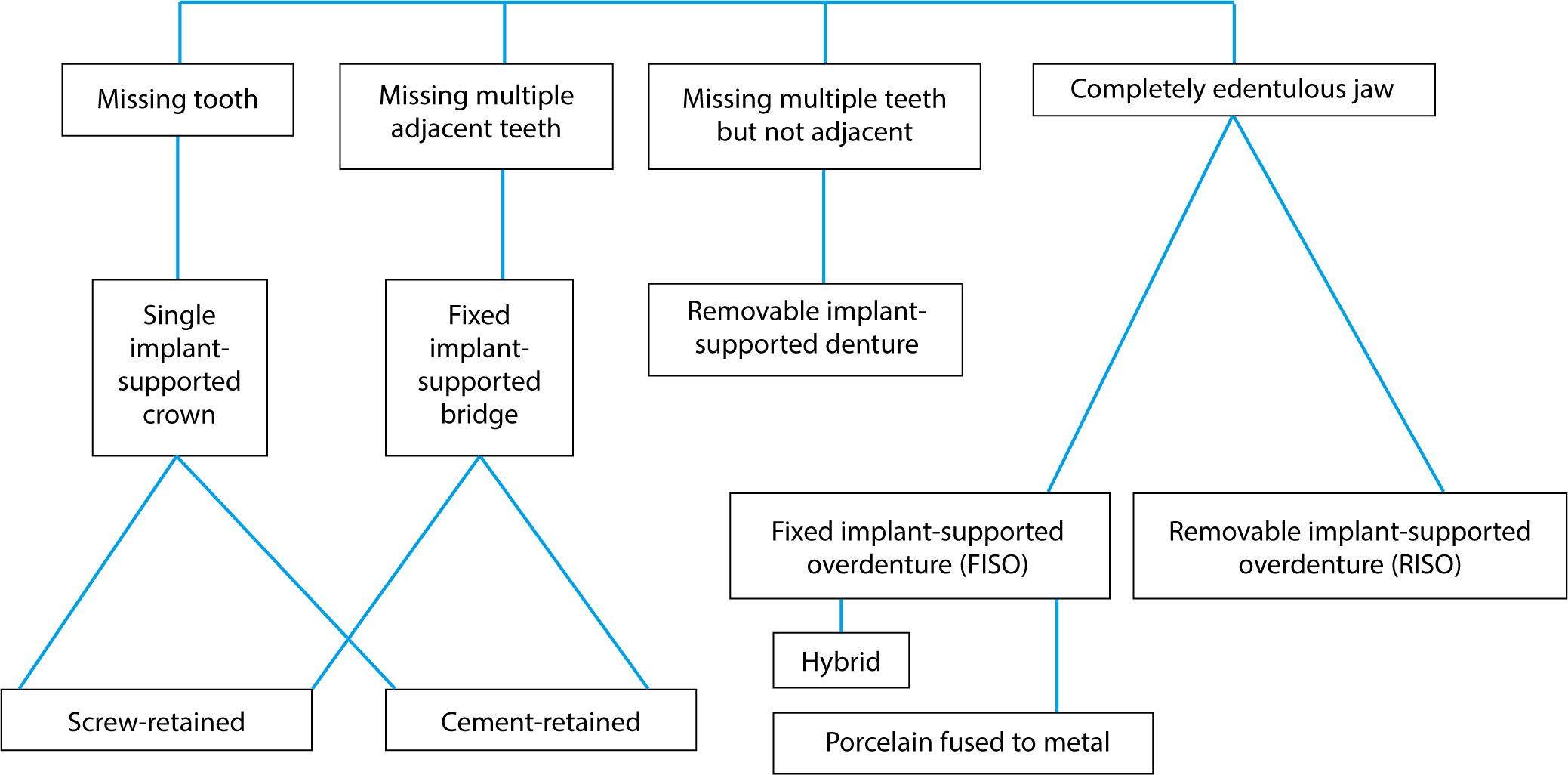
Treatment options for replacement of missing teeth with dental implants are shown in Figure 14.
Figure 14. Treatment options for replacement of missing teeth with dental implants.
An implant-supported single restoration (crown)
When a single tooth is replaced, the restoration is usually either cemented to the abutment or screwed to the implant (Figure 11). This is known as a cement-retained restoration and a screw-retained restoration, respectively. As mentioned earlier, in the cement-retained restoration, the abutment is attached to the implant body through a screw-joint and the restoration is cemented to the abutment in a similar fashion to that which is used in the conventional crown. Therefore, the abutment is used to connect the crown to the implant. In the screw-retained implant restorations, the restoration and the abutment are a single unit which is attached to the implant directly by a screw.16,106,107
A fixed implant-supported prosthesis (fixed bridge)
This is when multiple teeth are missing and replaced with a prosthesis that cannot be removed by the patient. In principle, this type of restoration resembles that described for a single-implant supported crown: cement- or screw-retained restorations.
A removable implant-supported prosthesis
In certain clinical situations, multiple missing teeth cannot be restored with a fixed implant-supported restoration. Instead, they are restored with a removable prosthesis which is fundamentally similar to that which is used in replacing a completely edentulous jaw with a removable implant-supported overdenture (RISO) (Figure 12). In this case, in addition to the available teeth, one or more implants with attachment systems are usually used. The attachment systems are discussed later in the article.
Implant-supported overdenture for completely edentulous jaws
When the jaw is completely edentulous, there are two treatment options for its restoration; namely a fixed or a removable implant-supported overdenture (FISO or RISO). A FISO is when the prosthesis is permanently fixed to the implants through screw-joints between the prosthesis and the implants.108 This is so it cannot be removed by the patient. The prosthesis is supported by several implants (usually four or more). When such prostheses are indicated, it is a favourable option for many patients. The volume of the prosthesis, and consequently the tissue coverage by the prosthesis, are reduced. However, this type of prosthesis is more expensive than removable ones. It also requires more implants to support and retain the prosthesis.
FISOs are of two basic types: hybrid and porcelain fused to metal. The hybrid prosthesis is made of a metal substructure, acrylic and denture teeth. The porcelain fused to metal prosthesis is made of a metal substructure and porcelain in a similar way to that used in the fabrication of the conventional porcelain-fused-to-metal restoration. It is more expensive than the hybrid and is difficult to make, but it is the better option when the vertical restorative space is limited.
Conversely, the RISOs are removable prostheses that can be removed and replaced by the patients. They are used in combination with attachment systems (see below).
The number of implants used with the RISOs may be reduced. For instance, in the case of edentulous mandible, the number may be reduced to two implants, which are usually placed in the anterior region of the mandible. The two-implant supported overdenture option is recommended as the first-choice standard of care for an edentulous mandible.108,109,110 When two-implant supported overdentures are used, the attachments permit movement of the overdenture during function and allow the mucosa of the residual ridge to be involved in dissipating the imposed force. Therefore, it is important to note that, in order to obtain good support from the residual ridges, the RISOs should extend to cover the supporting tissues in a similar fashion as that covered when the conventional complete denture is used.
The abutments
The restorations that consist of crowns or fixed prostheses (bridges), and that are supported by implants, may be divided into two types, depending on how they are connected to the implants; cement-retained and screw-retained. As mentioned earlier, in the cement-retained restoration the abutment is required to connect the restoration to the implant, while in the screw-retained restoration the abutment and the restoration form one unit. In addition, there are five types of abutments which are available for use in single and fixed implant-supported restorations.16,35 A summary of these abutment types can be found in Table 5.
Custom-made abutments
They are made of a plastic/wax pattern with/without a metal-machined interface ring;
The pattern is made (wax) or adjusted (plastic) to the required form, shape and angle;
The pattern is then used to create a metal abutment in a similar procedure to the conventional lost-wax technique;
An abutment plastic/wax pattern is attached to the implant analogue, which is submerged in a working cast;
The restoration is then made to fit the abutment also in the conventional method;
UCLA plastic patterns are an example of these types of abutments;
They require an impression of the implant platform.
Pre-machined (prefabricated/ready-made) modifiable metal abutments
They are prefabricated abutments;
They are adjustable and modifiable intra- and extra-orally;
They cannot be used when the implant is placed in an improper position or with improper angulation;
An impression of the abutment, not the implant, is taken using a manufactured impression coping;
The conventional crown and bridge procedures are used when provisional or final restorations are made.
Pre-machined (pre-fabricated/ready-made), non-modifiable metal abutments
They are pre-fabricated abutments that cannot be modified or altered;
The abutment that is suitable for the specific clinical condition is selected;
The abutment is attached to the implant body;
An impression of the abutment, not the implant, is taken using a manufactured impression coping;
The conventional crown and bridge procedures are used when provisional or final restorations are made.
All-ceramic abutments
They are made entirely of ceramic;
They are available in ready-made or customizable forms;
They are indicated for use in cases when aesthetics are essential, and when thin biotype gingiva exists so that metal show through is avoided.
CAD/CAM milled abutments
They are made from a block of titanium or ceramic;
An implant platform level impression may be required depending on the manufacturers;
A working cast is fabricated then scanned optically to generate exact 3D images of the region;
The information is sent to the milling machine to produce the abutment;
It eliminates certain negative factors that may be associated with the conventional method of abutment fabrication, such as an improper fit and incorporation of porosity;
This type of abutment is more expensive than the other abutment types.
Screw-retained restorations
In this case, the retention of the restoration relies on the retaining screw. Nevertheless, the restoration can be removed and/or replaced when required, without damage or need for a new restoration. The adaptation between the restoration and the underlying implant is usually better than that in the case of its cement-retained counterpart. It can be used when the vertical restorative space is limited as the retention depends on the screw, but is contra-indicated when mouth opening is limited, as the use of the different tools required for screwing and torqueing the screws may not be possible. However, the use of a screw-retained restoration may be considered when the implant platform is situated deep sub-mucosally, as complete removal of cement is not always possible when a cement-retained restoration is used. The screw type is not indicated when the screw hole is pointed at the labial surface as this compromises the aesthetics. Hence, the implant should be placed in its optimal position and angulation to avoid negative effects on aesthetics, otherwise an angled abutment may provide an acceptable alternative. In the posterior region, the occlusal morphology of the restoration may be difficult to obtain as the hole through which the screw is tightened occupies a major part of the occlusal table of the restoration. Furthermore, the access hole may weaken the porcelain and lead to its fracturing. It is important to mention that, if screw loosening of one restoration occurs in a fixed-implant supported restoration, a cantilevering effect can arise and put the other abutment, implants, screw and the peri-implant bone at risk as they are exposed to tremendous forces. Also, the screw loosening is not an unreal problem with the screw-retained restoration. However, the ability to retrieve the restoration/prosthesis easily to allow its cleaning (and of the peri-implant tissues) is a significant advantage of screw-retained restorations.
Cement-retained restorations
The cement-retained restoration is indicated when mouth opening is restricted, and when the implant angulation is not optimal without a major negative effect on the aesthetic outcome of the restoration.106,107,108 The occlusal morphology can be easily constructed in the normal way, as in conventional restorations. The materials and techniques used for the fabrication of the cement-retained restoration are similar to those used in the fabrication of conventional restorations. The trial stage and the final cementation procedure are almost identical to those used in conventional restorations. However, it may not be possible to remove the cement-retained restorations if permanent cementing media is used. Therefore, restorations have to be cut in order to remove them. The removal of excess cement may be not possible, which may result in soft tissue problems and to peri-implant disease (see below).16,106,107 Therefore, its use should be avoided when the implant-abutment connection is deeply embedded sub-mucosally, which may preclude its removal. Furthermore, removing the cement is not a predictable procedure and may cause the abutment/restoration to be scratched,111 leading to plaque accumulation. Marginal adaptation between the abutment and the restoration may also be inferior to that obtained when the screw-retained restoration is used. It is also not suitable when the vertical restorative space is limited, as retention may be compromised.
The attachment systems
An attachment is defined as a mechanical device used for the fixation, retention and stabilization of a dental prosthesis.112 It is used with implant-supported removable partial dentures and overdentures. The attachment usually consists of two parts. One part is attached to the implant, while the other part is attached to the prosthesis. Five types of attachment systems are available and compatible with the main implant systems. The attachment systems that are commonly used with RISOs include: bar/clip, balls, locators, magnet and telescopic crown.108,112 The use of a bar system allows splinting of two or more implants together. The other attachment types may be used individually and also in combination with the bar system. The attachments are attached to the implant by screws, resulting in a screw-joint. Features of attachment systems used for RISOs are displayed in Table 6.
The different designs of the attachment systems are used to gain retention, support and stability of the overdenture.
They consist of a matrix (female) and a patrix (male):
The matrix accommodates the patrix; and
The patrix frictionally fits and engages the matrix.
The joint that is made between the patrix and the matrix may be rigid (when no movements exist between the patrix and matrix) or resilient (when there are movements).
The involved dental implants are either splinted or non-splinted.
A bar is usually used to connect the implants (splinted).
Bars may be custom-made, pre-fabricated (ready-made) or CAD/CAM milled.
An individual attachment system is usually used in a non-splinted manner or combined with a bar system.
Peri-implant tissue response to bacterial insult and peri-implant diseases
Despite their high success rate, implant failures are also reported to occur. Several factors that have already been mentioned earlier which influence such success should be considered when treatment is planned.7 The implant may fail before it is put to function as a result of its failure to integrate with the peri-implant tissue during the healing stage. This type of failure is categorized as an early failure. The implant may also lose its integration and fail at a later stage, months or even years after implant placement. This is known as late failure.113 The criteria for dental implant success are displayed in Table 7.
That an individual, unattached implant is immobile when tested clinically.
That a radiograph does not demonstrate any evidence of peri-implant radiolucency.
That vertical bone loss is less than 0.2 mm annually following the implant's first year of service.
That individual implant performance is characterized by an absence of signs and symptoms, such as pain, infections, neuropathies, paresthesia or violation of the mandibular canal.
One of the complications that is reported to affect the peri-implant tissue is caused by the inflammatory response of this tissue to bacteria that forms a biofilm on the implant surface.114,115 It occurs when the balance between the host's defence and the bacterial load shifts in favour of the bacteria. This tissue response may be limited to the peri-implant soft tissues (mucosa) or may also extend to and affect the peri-implant bone and lead to its resorption.
Both tissue responses to bacterial insult are collectively known as peri-implant diseases, and are classified as peri-implant mucositis or peri-implantitis.116 In peri-implant mucositis, the inflammatory response is not essentially different from that which occurs in gingiva when it is exposed to pathogenic bacteria and leads to gingivitis.117 Therefore, in principle, peri-implant mucositis resembles gingivitis.
The onset and progression of mucositis may be affected by a decrease in the vascularity and an increase in collagen to fibroblast ratio in the peri-implant connective tissue, and by the way they are arranged around the implant surface.117 Clinically, peri-implant mucositis is characterized with bleeding on gentle probing. It is a treatable disease and the damage is reversible. However, it may progress into peri-implantitis if untreated.6,7 There are no major differences in the bacteria that were found to be associated with mucositis and peri-implantitis. This may indicate that mucositis is the origin of peri-implantitis.117
On the other hand, peri-implantitis occurs when both the peri-implant mucosa and bone are affected. It resembles chronic periodontitis in natural teeth. However, some differences do exist. For instance, the crestal bone loss occurs in a circumferential fashion around the affected implant, unlike bone resorption seen in chronic periodontitis. The circumferential shape of the peri-implantitis lesions may be attributed to the lack of periodontal ligament, and to the surface topographies of the involved implants which facilitate the spread of infection apically as well as laterally.6,117 The extent and the composition of cells in the peri-implantitis, as well as its progression rate, may differ from that which is commonly seen in chronic periodontitis.6,7.117 For instance, the protective connective tissue capsule, which was found to separate the periodontal lesion from the alveolar bone around teeth in the case of chronic periodontitis, does not exist around implants.7 Therefore, the self-limiting process is not present around implants, which may provide an explanation for the fast development and progression of the peri-implant disease.
It should be mentioned that dental implants may fail as a result of these diseases if they are not treated as they lead to bone resorption, and eventually to mobility and failure of the affected implant.8,9,10
It is important to remember that resorption of peri-implant crestal bone occurs within the first year of implant placement and continues to occur to a lesser degree afterwards. It occurs irrespective of the implant placement method (sub-merged or non-submerged). Based on a 15-year retrospective study, Adell and colleagues119 reported that crestal bone loss during the healing period and the first year after connecting the prosthesis, was about 1.5 mm. Thereafter, there was only 0.1 mm bone loss annually. In another study, an average of 0.9 mm crestal bone was lost during the first year and no more than 0.07 mm annually in the following years.120,121 The exact cause of this bone loss is still debatable. Nevertheless, the current literature presents several factors which may contribute to this loss, such as surgical trauma, reformation of a ‘biologic width’ and presence of a rough/smooth interface. However, the factors that are most commonly cited to cause such bone resorption are displayed in Table 8.
Bone remodelling after implant placement
Reformation of a ‘biologic width’
Presence of rough/smooth interface
Presence of a micro-gap at implant-abutment/restoration interface
Surgical trauma
Occlusal overloading
A ‘stress shielding’ phenomenon
Incomplete removal of luting cement 9. Peri-implant disease
Role of the patient and the dental professionals
Each dental implant and restoration/prosthesis should be evaluated clinically and radiographically in a similar manner to the treatment of periodontal disease. Oral hygiene should be observed and regular check-ups should be scheduled. Therefore, after a physiologic tissue remodelling period and at the time of prosthesis installation, clinical and radiographic examinations of the peri-implant tissue should be carried out and used as a baseline to monitor any change in the tissue and to intervene if required. When any deviation from the norm is found, intervention is then considered and carried out. In general, oral hygiene should be monitored and different oral hygiene aids should be demonstrated and the patient encouraged to use them as often as required.
In general, care for dental implants has two phases: patient self-care and professional clinical maintenance aspects.122 It is the responsibility of the patient to maintain good oral hygiene. Patient self-care consists of a daily oral hygiene procedure in which toothbrush (manual/powered and single tufted ones), auxiliary aids such as inter-proximal brushes, dental floss/tape and mouthrinses may be used. A combination of these aids, whenever it is necessary, should be considered and demonstrated. For instance, powered toothbrushes, which have different interchangeable bristle heads (flattened, rubber cup-like, short- and long-pointed in shape) that suit different clinical situations may be used. When they are used properly, the result is a healthy environment around the implant. However, it is important to mention that limiting the number of auxiliary aids, their simplicity and the time required for their use are important for patients' compliance as they play a vital role in this aspect.123
As already mentioned, dental implants are affected by and may fail as a result of the peri-implant disease which can be detected only by regular clinical and radiographic examinations. Therefore, when an implant is affected by the peri-implant disease, the patient should be made aware of the situation and a treatment plan should be implemented and regular follow-ups arranged. However, there is a lack of consensus on how peri-implant disease is treated. Nevertheless, the Cumulative Interceptive Supportive Therapy (CIST) protocol that was presented by Lang and colleagues123 may be followed when peri-implant disease is found. The CIST is a systemic comprehensive protocol. This protocol is based on clinical parameters such as peri-implant pocket depth (PIPD), bleeding on probing (BoP) and peri-implant bone loss on which clinical diagnosis is made. Accordingly, a treatment plan and continuous follow-up strategy are constructed. A summary of this protocol is presented in Table 9. However, the management of peri-implant diseases is not within this article's scope.
D. Same as treatment C combined with surgery (access flap, resective method or regenerative technique)
*Peri-Implant Pocket Depth;
Complications associated with implant-supported restorations and prostheses
Several biological and mechanical complications are reported with the use of dental implants to support/retain restorations and prostheses. For instance, screws used to connect different combinations of the implant-supported restorations/prostheses may become loose and need to be retightened or replaced. Screw loosening may be due to it not being adequately torqued or over-torqued or due to micro-movements that occur as a result of the manufacturing tolerance.33,35 An under-torqued screw fails to deliver the tension that is required to produce the optimum clamping force between the screw-joint components. Re-tightening is there for required. Screw re-tightening can be easily achieved when the restoration is a screw-retained type. However, when the restoration is cement-retained, cutting the restoration to gain access to the screw may be the only solution, especially when permanent cement is used. When a provisional cement is used, the use of crown removal may be tried.35
When the screw is over-torqued to a degree which places the screw material in tensile stress that exceeds its elastic limit, the screw may be plastically elongated. This leads to screw loosening or even to its fracture. In the former situation, the screw may be replaced, but in the latter situation the removal of the screw may not be possible and the treatment is complicated, which is beyond the scope of this article. To minimize the occurrence of screw-loosening or fracture, the recommended torque should be implemented using a torque driver that ensures that the right amount of torque is achieved.33
Mechanical superstructure failure may also occur when the material's mechanical properties and/or thickness is not optimum or when the occlusal design is not correctly designed. The superstructure failure may also occur as a result of lack of passivity when several implants are connected together. The lack of passivity may overload the implants and place the superstructure under tremendous pressure, that may lead to its failure. To check for passivity a test called a ‘Sheffield test’ or a ‘one-screw test’ is usually carried out. However, the passivity problem may be avoided by the use of computer-aided design/computer-aided manufacture (CAD/CAM) technology.
Acrylic or porcelain veneer may also fail when the bulk of these materials are inadequate. For instance, when a limited vertical restorative space does not allow the use of the optimum thickness of the material. Depending on the degree of mechanical damage of the restoration/prosthesis, fracture of porcelain may be repaired intra-orally using the Co-Jet® system (3M ESPE, St Paul, Mn, USA) and composite resin material. It is considered as a reliable method for such repairing. Fracture of acrylic may also be repaired using composite resin materials. However, when the metal frame-work is fractured, the only solution is its removal.
RISO attachment failure and complications are mostly of a mechanical nature and include:35
Fracture of the acrylic base, teeth and retentive clip;
Reduction of retention as a result of wear of the retentive elements or loosening of matrices and screws;
Fracture or wear of the clip and matrix;
Fracture of solder joints; and
Dislodgement of the attachments.
Wear of the attachment component is a problem that may reduce the overdentures' retention and, consequently, a replacement of the worn attachment becomes a necessity. Less prosthetic maintenance was required with the splinted (bar/clip) designs than with the unsplinted ones.124 Nevertheless, the use of bars may complicate the hygiene matter125 and it may be associated with a misfit of the framework, which has the potential to generate unwanted stress on the attachment, the implant, the retained screw and also the peri-implant bone.
Relining of the denture is also required regularly and may need to be carried out every few years to compensate for the changes in the alveolar ridge that may occur. Failures of the implant-supported fixed dental prosthesis also occur. The failures include screw loosening and fracture of the superstructure. Speech may be affected when tissue loss is severe. The compensation of lost tissue with acrylic or porcelain is usually required. This compensation may lead to an increase in plaque accumulation and tissue inflammation as the oral hygiene procedure is compromised. Meticulous effort from the patient is required. Calculus deposition once formed cannot be removed by a daily oral hygiene. Therefore, professional intervention is necessary. This intervention consists of the use of scalers with plastic tips to avoid scratching the implant components.33
Conclusion
Dental implants are widely used and considered as one of the options by which missing teeth are replaced. They are used successfully to replace single and multiple missing teeth as well as a completely edentulous jaw. The use of dental implants are increasing and dental professionals are more likely to see patients who have implant-supported restorations/prostheses. Therefore, basic knowledge of dental implants is necessary for dental personnel. Several factors are known to affect success of any implant system. These factors may be related to features locally, such as bone quality and quantity. Other factors are related to the surgical method by which an implant is placed or which are related to the implant system used, such as length and diameter of the implant. Furthermore, dental implants are affected by peri-implant diseases which, if not treated, can cause the implant to fail. It requires continuous monitoring, regular check-ups and may require professional interventions, the time of intervention being vital.
The success of any implant-supported restoration/prosthesis is dependent on the interaction between the patient and the dental personnel. Therefore, maintaining good oral hygiene and committing to regular check-ups are the responsibility of the patient. On the other hand, it is the responsibility of the dental personnel to examine the implants and the restorations/prostheses clinically and radiographically. It is also the responsibility of the dental practitioner to demonstrate and educate the patient on how to look after the implant and to tailor check-up recall visits according to the patient's needs.
Mechanical failures associated with implant-supported restorations/prostheses, such as screw loosening or fracture and chipping of porcelain veneer and fracture of the superstructure, are not uncommon. Loss of retention of the implant-supported overdenture are common clinical findings which may make the patient seek treatment. On the other hand, plaque accumulation and mucosal hyperplasia in the per-implant site do not necessarily promote the patient to look for treatment. Consequently, professional evaluation and assessment are required to discover such conditions. This necessitates recall visits and check-ups which allow the dental personnel to intervene in the proper time and to rescue the implant and its restoration/prosthesis. Therefore, the dental personnel should be prepared and able to diagnose and to deal with such complications and to refer the patients when required.