Kumar P, Alvi HA, Roa J, Singh BP, Jurel SK, Kumar L, Aggarwal H. Assessment of the quality of life in maxillectomy patients: a longitudinal study. J Adv Prosthodont. 2013; 5:29-35
Keyf F. Obturator prostheses for hemi-maxillectomy patients. J Oral Rehabil. 2001; 28:821-829
Ueda M, Hibino Y, Niimi A. Usefulness of dental implants in maxillofacial reconstruction. J Long Term Eff Med Implants. 1999; 9:349-366
Brown JS, Shaw RJ. Reconstruction of the maxilla and midface: introducing a new classification. Lancet Oncol. 2010; 11:1001-1008
Miller EL. Systems for classifying partially dentulous arches. J Prosthet Dent. 1970; 24:25-40
Okay DJ, Genden E, Buchbinder D, Urken M. Prosthodontic guidelines for surgical reconstruction of the maxilla: a classification system of defects. J Prosthetic Dent. 2001; 86:352-363
Ali R, Altaie A, Nattress B. Rehabilitation of oncology patients with hard palate defects Part 2: Principles of obturator design. Dent Update. 2015; 42:428-434
Walter J. Obturators for acquired palatal defects. Dent Update. 2005; 32:277-285
Kim DD, Ghali GE. Dental implants in oral cancer reconstruction. Dent Clin N Am. 2011; 55:871-882
Nelson K, Heberer S, Glatzer C. Survival analysis and clinical evaluation of implant-retained prostheses in oral cancer resection patients over a mean follow-up period of 10 years. J Prosthetic Dent. 2007; 98:405-410
Verdonck HW, Meijer GJ, Laurin T, Nieman FH, Stoll C, Riediger D, Stoelinga PJ, de Baat C. Implant stability during osseointegration in irradiated and non-irradiated minipig alveolar bone: an experimental study. Clin Oral Implants Res. 2008; 19:201-206
Linsen SS, Martini M, Stark H. Long-term results of endosteal implants following radical oral cancer surgery with and without adjuvant radiation therapy. Clin Oral Implants Res. 2012; 14:250-258
Zen Filho EV, Tolentino ES, Santos PS. Viability of dental implants in head and neck irradiated patients: a systematic review. Head Neck. 2016; 38:E2229-2240
Kovacs AF. Influence of chemotherapy on endosteal implant survival and success in oral cancer patients. Int J Oral Maxillofac Surg. 2001; 30:144-147
Vasant R, Vasant M. Retention systems for implant-retained overdentures. Dent Update. 2013; 40:28-31
Williams BH, Ochiai KT, Hojo S, Nishimura R, Caputo AA. Retention of maxillary implant overdenture bars of different designs. J Prosthetic Dent. 2001; 86:603-607
Elsyad M, Al-Mahdy Y, Salloum M, Elsaih E. The effect of cantilevered bar length on strain around two implants supporting a mandibular overdenture. Int J Oral Maxillofac Implants. 2013; 28:e143-150
Semper W, Heberer S, Nelson K. Retrospective analysis of bar-retained dentures with cantilever extension: marginal bone level changes around dental implants over time. Int J Oral Maxillofac Implants. 2010; 25:385-393
Eliasson A, Weennerberg A, Johansson A, Ortorp A, Jempt T. The precision of fit of milled titanium frameworks (I-bridge) in the edentulous jaw. Clin Implant Dent Relat Res. 2010; 12:81-90
Ortorp A, Jempt T. CNC-milled titanium frameworks supported by implants in the edentulous jaw: a 10-year comparative clinical study. Clin Implant Dent Relat Res. 2012; 14:88-99
Delvin H, Barker G. Prosthetic rehabilitation of the edentulous patient requiring a partial maxillectomy. J Prosthetic Dent. 1992; 67:223-227
Budtz-Jorgensen E, Bertram U. Denture stomatitis 1: The etiology in relation to trauma and infection. Acta Odontol Scand. 1970; 28:71-92
Garner S, Nobbs A, McNally L, Barbour M. An antifungal coating for dental silicones composed of chlorhexidine nanoparticles. J Dent. 2015; 43:362-372
An implant-retained obturator – a case study James Puryer Claire Forbes-Haley Dental Update 2024 44:5, 707-709.
Authors
JamesPuryer
BDS DPDS MFDS RCS(Eng) MDFTEd MSc FHEA
Clinical Lecturer (Restorative), School of Oral and Dental Sciences, Bristol Dental Hospital, Lower Maudlin Street, Bristol BS1 2LY, UK (James.Puryer@bristol.ac.uk)
This case describes the oral rehabilitation of a patient following maxillary hemi-section due to squamous cell carcinoma of the palate. Planned treatment was construction of a maxillary implant-supported obturator. Two dental implants were placed in his maxilla to aid the support and retention of an obturator. However, owing to bone availability, their angulation was suboptimal and compromised the retention of the obturator. This case describes alternative implant attachments to aid the retention and stability of implant-retained dentures constructed in cases with suboptimal implant placement.
CPD/Clinical Relevance: This case highlights the importance of careful planning for implant placement, and reinforces the need to plan the prostheses before implant surgery. This case highlights possible difficulties that can arise if implants are non-ideally angulated, and how to adapt restorations to manage such difficulties in cases with maxillary removable prostheses.
Article
An obturator is a device constructed for occluding a cavity, usually in a patient's hard or soft palate. Palatal defects can either be congenital, ie cleft palate, or they may be acquired; as a result of trauma or surgical excision. The resultant oronasal communication and altered anatomy may leave a patient with functional problems including:
Mastication efficiency;
Deglutition;
Phonetics;
Breathing;
Aesthetics.
All of these problems can affect the mental and physical wellbeing of patients, and the provision of a successful obturator for patients can have a significant effect on their quality of life.1 Obturators can be supported and retained by the patient's remaining hard and soft tissues but, whilst the presence of some remaining teeth can facilitate the prosthodontic rehabilitation of maxillectomy patients, for those patients that are edentulous the treatment may be more challenging.2 The difficulty in managing these cases is not only dependent upon the number of natural teeth remaining, but the size and classification of the defect, presence or lack of undercut within the oral cavity/defect, decreased muscular control and reduced sensation. Increasingly, dental implants are being used to aid support and retention, and the overall survival rate for implants supporting maxillofacial prostheses has been reported to be as high as 96.1%.3
When planning dental implant placement to support an obturator, there are many factors that need to be taken into consideration (Table 1). It is important to remember that dental implants are a method of providing support and retention for a prosthesis, and it is the planning of their overall rehabilitation that is the key to success. Failure to plan the prosthesis before dental implant placement can lead to problems with:
Aesthetics;
Retention;
Support;
Stability;
Function.
General Patient Factors
Age
Medical history
Smoking
Motivation
Expectations
Oral hygiene
Anxiety
Financial constraints
Life expectation
Use of radiotherapy
Patient dexterity
Dental Factors
Quality of bone
Amount of bone
Space requirements
Proximity of vital structures
Prostheses (fixed or removable)
Number of implants
Periodontal status
Restorative status
Endodontic status
Occlusion
Hard and soft tissue profile
Xerostomia
Patient opening
Problems in any or all of these areas can contribute to both short-term and long-term failure of the prosthesis or implant with inevitable patient dissatisfaction.
This case describes a patient with a failing implant-supported maxillary obturator due to lack of retention from implant fixtures. The clinical management of this patient to improve the stability and retention of his obturator utilizing a milled titanium bar and definitive obturator is described.
The patient
The presenting complaint of the male patient aged 76 years old (PG) was one of a loose upper obturator. He had this original obturator made 6 years previously. The patient was generally fit and well, suffering from only mild asthma and rheumatoid arthritis. His medications included a salbutamol inhaler, ibuprofen as needed, and he was a non-smoker.
PG was diagnosed with a squamous cell carcinoma of his upper right premolar region in 1994. He underwent a right hemi-maxillectomy with associated partial neck dissection under general anaesthesia soon afterwards. A surgical obturator was fitted at the time of initial surgery, followed by the provision of a definitive obturator 2 months later. In 2006, two standard 12 mm x 4.1 mm (Straumann, Switzerland) implants were placed in the UL3 and UL4 region of the maxilla to help aid the retention of this obturator using ‘Locator’ (Straumann, Switzerland) abutments. The current obturator was constructed by one of the authors (JP) following implant placement. Whilst this current obturator was initially successful, its retention was now reduced following the recent extraction of the upper left second molar (UL7) due to extensive caries, and its subsequent addition to the prosthesis.
On re-presentation, all extra-oral and intra-oral tissues appeared healthy. The patient had a right-sided 2 cm x 4 cm ‘Class 2b’ defect based upon Brown's classification4 of partially dentate maxillectomy patients (Table 2). Thus the defect was a ‘low level maxillectomy not involving the orbital floor’ and was ‘less than or equal to half the maxilla’. The only remaining teeth in the upper arch were the retained roots of both upper central incisors, which were now carious and unrestorable. The upper obturator was made of cobalt/chrome and acrylic, with a hollow Mucopren Soft (Kettenbach, Germany) bung. The fixtures in the UL3 and UL4 region were stable, but were proclined buccally with an acute emergence profile. As a result it was difficult for the Locator inserts to fully engage within the abutments, thus reducing the retentive nature of these attachments and compromising the overall retention of the obturator.
Vertical Classification
Horizontal Component
Class 1
Maxillectomy without an oral/antral communication
a
Palatal defect only, sparing the alveolus
Class 2
Low level maxillectomy not involving the orbital floor or contents
b
Less than or equal to half the maxilla, unilateral maxillectomy
Class 3
High level maxillectomy involving the orbital contents
c
Less than or equal to half bilateral or transverse anterior defect
Class 4
Radical maxillectomy involving orbital exenteration
d
Greater than half maxillectomy
PG was partially dentate in the lower arch, with LR3–LR1 present. Caries was present in the distal surface of LR3. He wore a Kennedy Class I5 acrylic removable partial denture that replaced LR7–LR4 and LL1–LL7. His BPE scores were recorded as:
-
-
-
-
1
-
Diagnoses
Localized chronic gingivitis;
Retained roots UR1/UL1 and LR3;
Loose upper obturator.
Treatment plan
To stabilize primary dental disease, prevent further disease and to provide the patient with a more retentive removable prosthesis. This was to be achieved by:
Oral hygiene instruction and dietary advice with F-supplementation;
Extraction of retained roots UR1/UL1;
Restoration of LR3;
Provision of an implant-retained milled titanium bar in the ULQ;
Provision of a new acrylic and Mucopren Soft upper obturator.
Treatment method
The initial phase of treatment was to stabilize and prevent further primary dental disease. LR3 was restored using a resin-modified glass-ionomer cement (FujI II, GC Europe). Oral hygiene instruction was given with respect to improving plaque control around the remaining lower anterior teeth, denture hygiene and dietary advice for caries prevention.
To facilitate the provision of the upper prostheses, primary impressions were taken with an impression of the lower arch, with the partial denture in situ. An impression of the upper defect was taken using a heavy-bodied silicone putty (Extrude XP, Kerr). This was manipulated by hand into the defect to better engage natural undercuts and creation of a seal. Locating grooves were cut into the base of this silicone bung and an alginate wash impression taken of the upper arch, in a rigid stock tray (Figure 1). Upper (Figure 2) and lower primary casts were constructed, along with a perforated ‘open’ upper special tray (Figure 3) and a Mucopren Soft bung for the defect. The UR1/UL1 retained roots were extracted under local anaesthesia.
Figure 1. The primary impression taken in Extrude XP (Kerr) and alginate.Figure 2. The upper primary cast showing the size of the surgical defect, retained roots UR1/UL1 and the poorly angulated implants and abutments UL3 and UL4.Figure 3. The upper special tray with open window on the left side to allow the ‘pick-up’ impression of the fixtures UL3 and UL4.
The next stage of treatment was to obtain a master impression for the construction of the milled titanium bar and obturator. The Locator abutments were removed from UL3 and UL4, and the Mucopren Soft bung was tried into the defect to verify fit, retention and patient comfort. A master ‘pick-up’ impression of the bung, and upper arch and fixtures was taken with Impregum Penta (3M ESPE, UK) medium body polyether material using the upper special tray. The resultant master cast (with analogues in situ) can be seen in Figure 4.
Figure 4. The upper mast cast with the fixture analogues in situ. Again, the poor angulation of the two implant fixtures is evident.
Jaw relationship records were obtained using an upper wax rim that incorporated the Mucopren Soft bung and implant fixtures. The wax rim and bung were checked for fit, stability, retention and comfort, and then adjusted in the conventional manner. An alginate impression was taken of the existing upper obturator to help guide the technicians with regards tooth size and form.
A wax trial denture was constructed, again incorporating the Mucopren Soft bung and implant attachments. The design of the obturator would allow replacement of the Mucopren bung in future. The trial denture was used to confirm the tooth set-up, especially with relation to upper lip support, occlusion and aesthetics. The trial obturator had improved retention at this stage, even without the benefit of the additional retention that was expected from the milled bar.
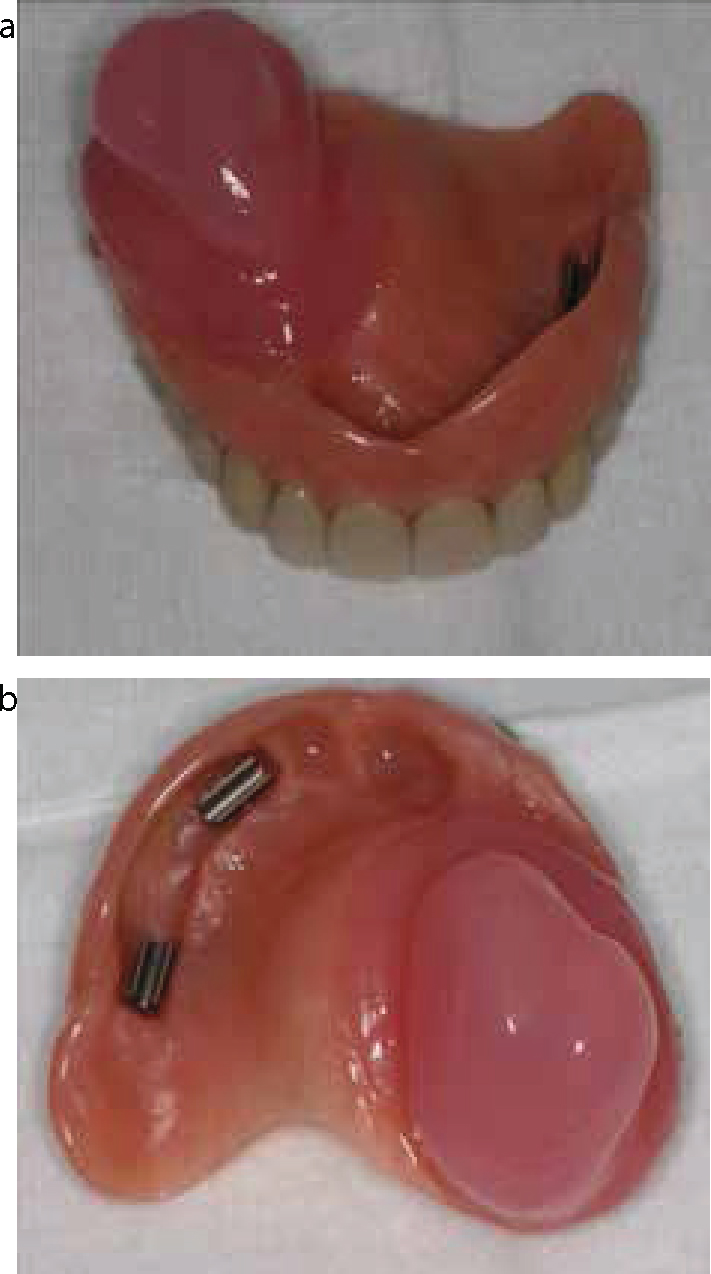
The milled titanium ATLANTISTM ISUS (Dentsply, UK) bar was constructed (Figure 5) and tried for fit. Passive fit was checked on the master cast before verifying intra-orally; bridge screws were hand-tightened in order to confirm the fit. Figure 6 shows the bar in situ. Note the change in angulation of the bar from the abutments of approximately 45°. At the final fit stage, the ATLANTISTM ISUS bar was fitted, and the bridge screws torqued to 20N (as per manufacturer's guidance). The processed obturator (Figures 7a and b), complete with metal clips to engage the implant superstructure, were fitted and checked for stability, retention, occlusion, comfort and aesthetics. It was confirmed that the patient could insert and remove the obturator without difficulty. Post-insertion instructions were given with respect to insertion and removal of the obturator, along with reinforcement of oral hygiene measures. A review appointment was arranged.
Figure 5. The milled titanium ATLANTISTM ISUS (Dentsply) bar.Figure 6. The milled titanium ATLANTISTM ISUS (Dentsply) bar in situ at the trial stage. The change in angulation of the bar from the abutments of approximately 45° is evident.Figure 7. (a, b) The processed obturator ready for fitting complete with metal riders to fit the implant superstructure.
At the review, the patient was happy with the new upper obturator and no adjustments were required. However, LR2 had fractured and was deemed unrestorable. The tooth was dressed temporarily and the decision was made to construct a new lower cobalt/chrome removable partial denture, with the addition of LR2 at the ‘fit’ stage. The lower partial denture was constructed in a conventional manner. The LR2 was uneventfully extracted under local anaesthesia at the next visit, and the new denture fitted.
On subsequent review, the patient reported no problems, and was happy with both the new upper obturator and new lower partial denture.
Discussion
This case highlights different techniques available for increasing the support and retention of a maxillary prosthesis when implant positioning may be compromised. Small maxillectomy defects can be successfully repaired by surgical reconstruction combined with prosthetic rehabilitation in order to close the oronasal communication.6 When an obturator is considered the more appropriate oral rehabilitation, its design is dependent upon the patient's defect and residual denture-bearing anatomy.7 Larger palatal defects may make provision of an obturator more challenging due to tooth loss, limited bony support and the need to restore large areas of oral and/or facial soft tissues. For some patients, other than providing dental implants, the only option to achieve good retention is to fully engage the available soft-tissue undercuts found within the defect space and on the non-resected site. The ability of a prosthesis to fully engage these undercuts may be limited by the path of insertion and restricted mouth opening.8 Whilst there are numerous designs and materials that a clinician may choose from, most definitive obturators are made in combination with a denture, and so it is essential to consider the basic qualities of a successful removable prosthesis:9
Support;
Retention;
Stability.
The use of conventionally placed dental implants can aid the success of an obturator by increasing all three of these basic qualities, and have been used successfully in oral cancer patients.10,11 However, compromised blood supply and potentially impaired osseointegration12 in irradiated bone can increase early failure rates;13 although implants in irradiated bone still show high success rates,14 chemotherapy for oral cancer does not seem to increase implant failure.15 Rigid fixation of the prosthesis is essential to minimize technical and biological complications11 and, in the case described, the failure of the Locator inserts to fully engage within the abutments compromised the prosthesis retention and the patient's function. The provision of a milled bar for this patient has increased support, stability and retention, and has improved the path of insertion of the obturator, allowing more natural undercuts to be engaged within the palatal defect. There are different methods of increasing retention and stability for a removable prosthesis utilizing dental implants. Common methods include magnets, ball abutments and locators. The effectiveness of these methods of retention can, however, be limited by implant positioning and angulation. There are different inter-occlusal space demands, depending on the choice of implant abutment. Bars are another method of retention which can provide increased stability, and bars can be cast or milled. There are different shapes available; micro-Dolder/macro-Dolder (egg or ‘U’), Hader, primary bar (a milled bar with reduced taper), 2-in-1 prosthesis and combination bar (2 types of bar or primary bar with accessories).16 There can be additional retentive features incorporated into a bar such as Riders (metal or plastic clips), Locators, Cekas, balls (Dalbo or Clix) and Conus abutments. Therefore bars can be very versatile, but usually require more inter-occlusal space and ridge width than the more common retentive abutments. If there is sufficient space then their versatility and ability to provide increased stability, as well as retention, can give superior results for an implant-supported removable prosthesis. However, for the patient described in this case, these alternative designs were rejected either because of his inability to change the implant angulation, or the demand for greater space within the prostheses which was not available.
When designing a bar, planning for its length, angulation and the direction of any occlusal forces should be taken into consideration. In addition, the space requirements for a dental bar needed to be assessed. Different bar designs, combined with the selection and position of specific attachment systems, can affect the retention and clinical performance of implant-retained prostheses.17 A rigid bar is essential. Bars with cantilevers (either with or without clips) demonstrate a significant increase in strain compared to bars without cantilevers and, furthermore, the longer the length of the cantilevered sections of the bar, the greater stress this places.18 However, it has been found that the use of cantilever bars up to 12 mm in length did not increase marginal bone loss around implants.19
The ATLANTISTM ISUS (Dentsply) bar uses CAD/CAM technology, and this technique can produce a better passive fit than when superstructures bars are produced by conventional casting methods.20 A cold milling technique from a block of alloy avoids the dimensional changes of the metal associated with the casting technique. In addition, clinical studies21 with a follow-up period of 10 years showed a reduced number of technical complications with CAD/CAM vs cast structures. From a practical viewpoint, the use of CAD/CAM technology can allow dental laboratories to concentrate on the production of the superstructure rather than on the milling process itself.
The use of a Mucopren Soft bung allows engagement into undercuts within the palatal defect and can achieve better retention.22 However, as silicone flexes under load, the seal that it forms may be compromised. Other problems associated with bungs constructed from resilient soft lining materials include cleaning issues for patients, with surface irregularities shielding micro-organisms from physical oral hygiene measures. Therefore bungs can become prone to fungal infection.22 Bungs need regular replacement and can be difficult to adjust, with any adjustment potentially leading to a roughened surface which again facilitates the retention of micro-organisms, and acts as a reservoir for bacteria. This may be worsened by the material having a relatively high surface porous texture, and from saliva being prevented from cleansing the bung.23 Anti-fungal agents have previously been incorporated into resilient soft lining materials with limited success, but recent research has shown that the use of chlorhexidine nanoparticles may be a useful strategy in the design of antifungal coatings for these materials.24 Ultimately, the decision to choose between using a soft lining material or hard acrylic resin lies with the clinician, based upon an individual patient's needs, and replacement of this bung at regular intervals should be carefully considered in the design of the prosthesis.
Conclusion
It is essential to plan the final prosthesis prior to implant surgery. Assessment of the following should all be carried out prior to surgery in order to allow optimal placement of implants:
Occluding vertical dimension;
Height available for restoration on the implants;
Tooth position/size/shape;
The need to replace missing soft tissues;
Choice of fixed or removable prosthesis.
This case describes the successful prosthetic rehabilitation of a patient with a maxillectomy defect and adaptions made to the removable prosthesis to allow more strategic use of sub-optimally positioned dental implants. The use of a milled titanium bar superstructure offered a practical method for improving the support and retention of a prosthesis for this patient in conjunction with using basic principles of removable prosthesis construction.