Muller M, Hansel M, Stehr S, Weber S, Koch T. A state-wide survey of medical emergency management in dental practices: incidence of emergencies and training experience. Emerg Med J. 2008; 25:296-300
Girdler N, Smith D. Prevalence of emergency events in British dental practice and emergency management skills of British dentists. Resuscitation. 1999; 41:159-167
Atherton G, Pemberton M, Atherton G. Medical emergencies: the experience of staff of a UK dental teaching hospital. Br Dent J. 2000; 188:320-324
Mighell A, Atkin P, Webster K, Thomas S, McCreary C, Healy C Clinical medical sciences for undergraduate dental students in the United Kingdom and Ireland – a curriculum. Eur J Dent Educ. 2011; 15:179-188
Clark A. Preparing for emergencies: resuscitation guidelines for general dental practice. Prim Dent J. 2014; 3:58-63
An update on current resuscitation council (UK) guidelines Sarah L McKernon Laura Kaura Kathryn H Taylor Samantha Reid Mary C Balmer Dental Update 2024 44:4, 707-709.
Authors
Sarah LMcKernon
BDS, MFDS RCS(Ed), FHEA
Clinical Lecturer/Hon StR Oral Surgery, Liverpool University Dental Hospital, Liverpool, UK
On 15 October 2015, The Resuscitation Council (UK) published new resuscitation guidelines following the review of resuscitation science by the International Liaison Committee on Resuscitation (ILCOR). The 2015 guidelines emphasize the importance of interactions between the emergency medical dispatcher, the bystander who provides cardiopulmonary resuscitation (CPR) and the prompt deployment of an automated external defibrillator (AED); the co-ordination of these three elements is crucial to improving out-of-hospital cardiac arrest survival. Medical emergencies in dental practices are thought to occur on average once every 3–4 years per dentist in primary care. The GDC consider medical emergencies as a highly recommended topic for Continuing Professional Development (CPD) and recommend at least 10 hours in every CPD cycle.
CPD/Clinical Relevance: The publication of the updated guidelines serves as a reminder to the clinical team of the importance of being up to date with recognition and treatment of cardiac arrest and choking and how seamless interaction between members of both the dental and medical teams improves long-term outcomes for patients.
Article
On 15 October 2015, The Resuscitation Council (UK) published new resuscitation guidelines following the review of resuscitation science by the International Liaison Committee on Resuscitation (ILCOR).1 These guidelines followed the same development process as in 2010 and the process is accredited by the National Institute for Health and Care Excellence (NICE).
Guideline changes are based on current scientific research and are aimed at simplifying clinical practice, enhancing education and improving outcomes. Unusually, for the first time in recent years, the new guidelines do not include any significant changes to core interventions or processes. The evidence would suggest that current practice is correct but, unfortunately, not consistent or to a high enough standard.1
The 2015 guidelines emphasize the importance of interactions between the emergency medical dispatcher, the bystander who provides cardiopulmonary resuscitation (CPR) and the prompt deployment of an automated external defibrillator (AED); the co-ordination of these three elements is crucial to improving out-of-hospital cardiac arrest survival.
Medical emergencies in dental practices
Medical emergencies are becoming more frequent in dental practices, with 57% of dental practitioners reporting up to three emergencies in a twelve month period,2 compared with approximately 0.7 cases per year reported ten years ago.3 The prevalence in a hospital setting is greater, at 1.8 cases per dentist per year.4 In patients with more complex medical histories (ie increasing ageing population), the likelihood of a medical emergency occurring is believed to be greater.5 Studies show that the most frequently occurring medical emergencies are vasovagal syncope (faint), asthma, angina, hypoglycaemia, seizures, anaphylaxis and choking.3 Fortunately, emergencies such as myocardial infarction and cardiopulmonary arrest are rare.6
It is important that members of the dental team are competent and adept at recognizing and managing medical emergencies. All members of the dental team should be familiar with their roles and responsibilities during a medical emergency scenario. This is primarily why team-based scenario training is recommended.
Medical emergency equipment and drugs
The Resuscitation Council (UK) published recommendations for standards in primary care and the minimum equipment that dental practices should have available (Table 1).7 It is advised that the responsibility for checking equipment and expiry dates should rest with a named individual. This should occur weekly, be recorded, and the process audited. The document ‘Medical Emergencies in General Dental Practice’ is no longer published by Resuscitation Council (UK). This document listed the emergency equipment and drugs required in dental practices. In addition to the required equipment, this document listed the recommended drugs required in dental practices. Since this document was superceded, readers are now advised to refer to the relevant section of the British National Formulary (BNF) for guidance. The list of recommended drugs found in the BNF is summarized in Table 2 in addition to their route of administration.
Salbutamol Aerosol Inhalation (100 μg per actuation)
Inhalation
Training and education
There is a public expectation that all dental care professionals should be competent in treating cardiorespiratory arrest and proficient in the use of an AED. The General Dental Council (GDC) stated in ‘Scope of Practice’ that ‘a patient could collapse on any premises at any time, whether they have received treatment or not. It is therefore essential that ALL registrants are trained in dealing with medical emergencies, including resuscitation, and possess up to date evidence of capability’.8 It is essential that regular staff training is undertaken using simulation-based cardiorespiratory arrest scenarios. As a minimum, this training should include cardiopulmonary resuscitation (CPR) including basic airway management and the use of an AED. This training should be updated at least annually.
The GDC consider medical emergencies as a highly recommended topic for Continuing Professional Development (CPD) and recommend at least 10 hours in every CPD cycle. Unfortunately, the topic is only recommended and the authors would strongly suggest that, as a profession, we consider medical emergencies training an essential topic. The importance of training as a team should not be underestimated and members of the team should be aware of their roles and responsibilities during a medical emergency. In the event of an emergency, it is recommended that each primary dental care facility has a protocol in place detailing who to contact (usually 999) and the instructions for ambulance crews, for example, will they be met on the road by a member of staff?
It is important to note, given the recent publication from the Intercollegiate Advisory Committee for Sedation in Dentistry (IACSD), that those practitioners undertaking sedation are expected to hold an immediate life support (ILS) qualification or the paediatric equivalent9 and have training in sedation-related emergencies.
Human factors
Human factors within team members have been proven to play a significant role in the outcome of medical emergency situations.10 Within this, leadership and team roles play a significant role.11 Therefore, to help minimize the effect that human factors have on performance in a medical emergency, the Resuscitation Council have recommended the following be adapted into training:12
Situational Awareness – All team members should be aware of and have an understanding of the current event.
Decision making – The team leader should make decisions and communicate these clearly to team members.
Team working – Evidence demonstrates the effect good leadership and team working has on successful management of critical situations.
Task Management – Co-ordinating tasks and knowing roles and responsibilities.
Chain of surviva
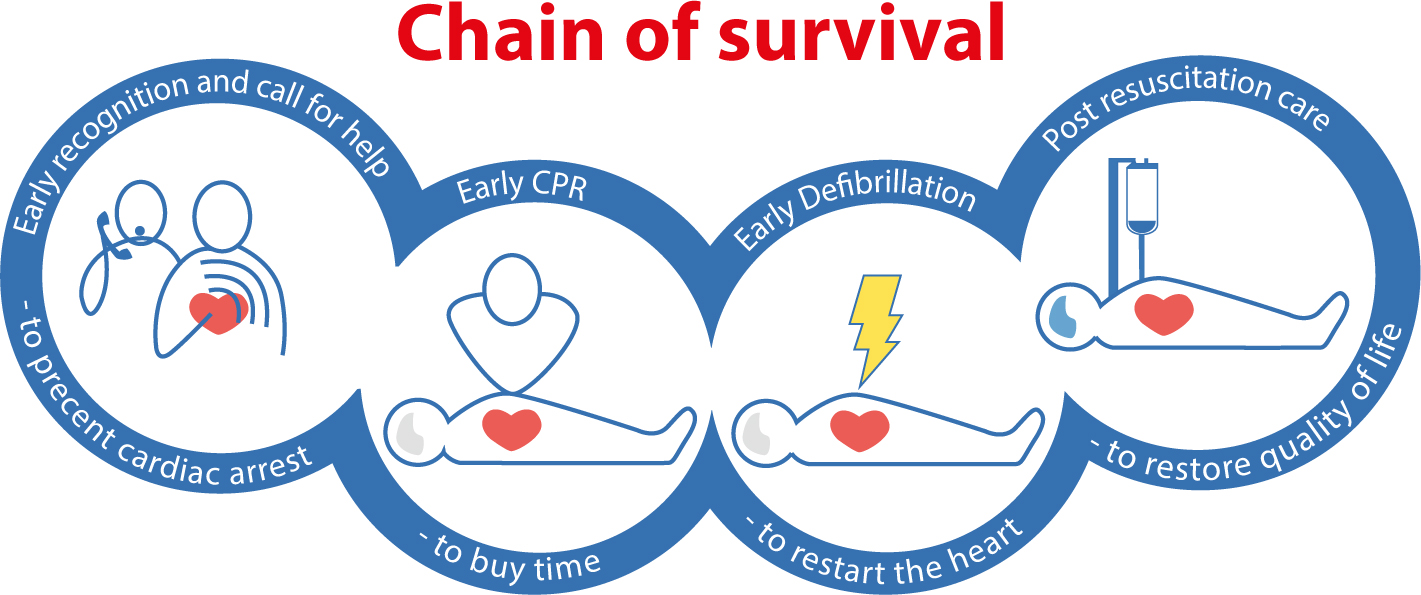
The updated Resuscitation Council (UK) guidelines stress the importance of four steps that improve the chances of survival in out-of-hospital cardiac arrest as detailed in Figure 1:
Figure 1. The Chain of Survival (Reproduced with the kind permission of the British Heart Foundation).
Early recognition and call for help;
Early bystander CPR;
Early defibrillation;
Early advanced life support and standardized post-resuscitation care.
In order to ensure that these steps are carried out effectively and efficiently, the dental team must be well prepared to deal with any emergency that may occur in the dental practice. The first link in this chain is early recognition, and this includes recognizing potential arrest signs and symptoms and calling expert help and support, eg worsening angina despite intervention, anaphylaxis, choking, steady decline in breathing, pulse and blood pressure. All members of the team should also be cognizant of how to diagnose an actual cardiac arrest, ie loss of effective cardiac output and recognize a deteriorating patient. A thorough up-to-date medical history for every patient is essential as this may make the team more aware of patients that are likely to develop cardiac arrest, for example, those with angina, hypertension and chronic heart disease/failure.
In order to deliver early defibrillation, one must have access to a defibrillator (Figure 2). The guidelines encourage the use of Public Access Defibrillation (PAD) programmes in public areas where there is a high volume of people and CPR providers can be quickly on the scene or in remote locations where ambulance services are likely to be delayed, eg aeroplanes or boats. The guidelines also recommend registration of defibrillators so that ambulance dispatchers can direct CPR providers to the nearest AED.
Figure 2. Automated External Defibrillator (AED);
Adult Basic Life Support (BLS) sequence
The updated guidelines suggest the following steps once cardiac arrest has been recognized:
Safety
Response
Airway
Breathing
Dial 999
Send for AED
Circulation
Give rescue breaths
AED
Continue CPR
Recovery position
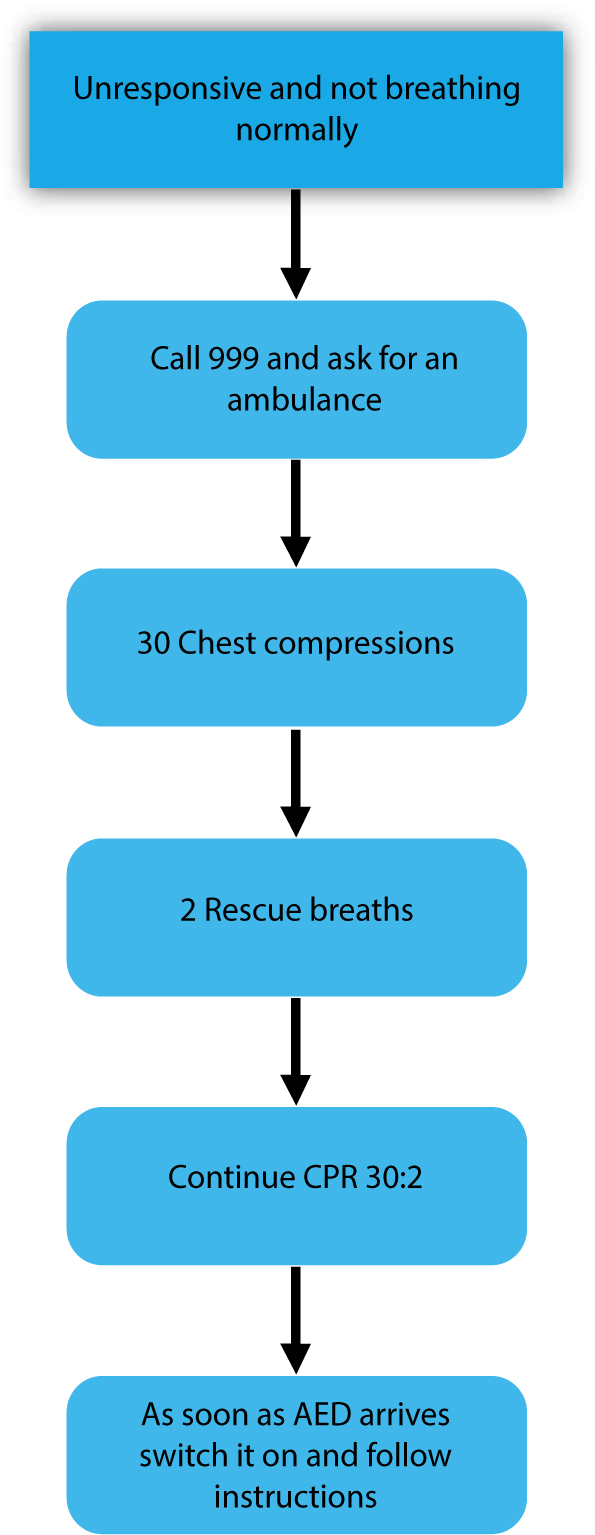
The BLS algorithm comes into effect once the patient has been deemed unresponsive and not breathing normally (Figure 3). The guidelines draw the readers' attention to agonal breaths – irregular slow deep breaths often accompanied by snoring sounds. These breaths originate from the brainstem that may still continue to function for some minutes after being deprived of oxygen. It is also noted that, when blood flow to the brain is significantly reduced, a seizure like episode may occur, therefore it is important that the team suspect cardiac arrest in patients presenting with seizures. After assessing airway and breathing in the usual way an ambulance should be called.
Figure 3. Adult BLS algorithm. (Reproduced with the kind permission of the Resuscitation Council (UK)).
Chest compressions should be started without delay and should only be interrupted if changing rescuers or assessing rhythm with an AED. Chest compressions should be administered in the centre of the chest to a depth of 5–6 cm at a rate of 100–120/min (Figures 4 and 5). After 30 compressions, two rescue breaths should be given. The guidelines recommend changing CPR providers if possible every 2 minutes. Comparing compression only versus standard CPR that includes ventilation, the guidelines suggest that there is insufficient evidence in equivalence between both methods and therefore they continue to recommend that chest compressions should be performed in all those with cardiac arrest, and CPR providers trained and able to provide chest compressions and rescue breaths should do so as there is an additional benefit in children and those in asphyxia cardiac arrest. The risk of serious harm in delivering CPR to a person later found not to be in cardiac arrest is rare. Those in cardiac arrest have a risk of rib or sternal fracture or, rarely, internal organ damage, but the benefits of CPR far outweighs these risks. Performing CPR is safe to the person administering it in most circumstances.
Figure 4. Correct hand position for chest compressionsFigure 5. Correct arm position for chest compressions
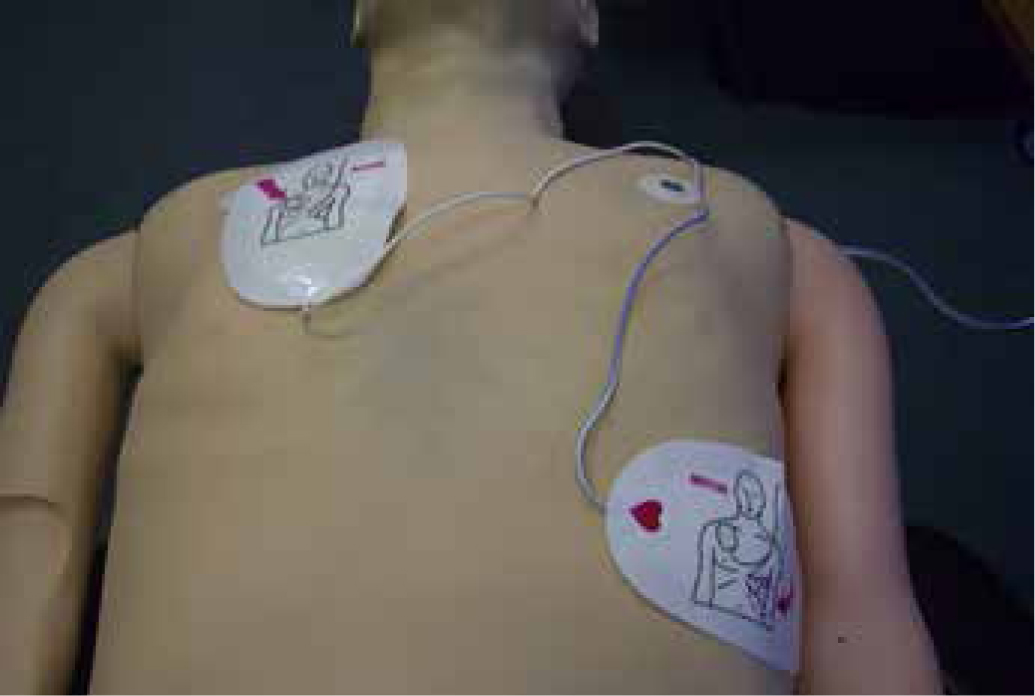
The AED electrode pads should be attached to the victim's bare chest whilst CPR is continuing (Figures 6 and 7). Visual/spoken directions are given and CPR should only be stopped when the AED is analysing the heart rhythm. If a shock is indicated, no one should touch the victim, the button should be pressed to deliver the shock and then CPR is recommenced immediately as per the prompts. If no shock is advised, CPR should be continued. The guidelines recommend that CPR should only be stopped if a health professional tells you to stop, the CPR provider becomes exhausted, or the victim is definitely wakening up, moving, opening eyes and breathing normally. In this instance the victim should be placed in the recovery position.
Figure 6. AED electrode pads before opening.Figure 7. AED electrode pads should be attached to the victim's bare chest as shown.
Choking
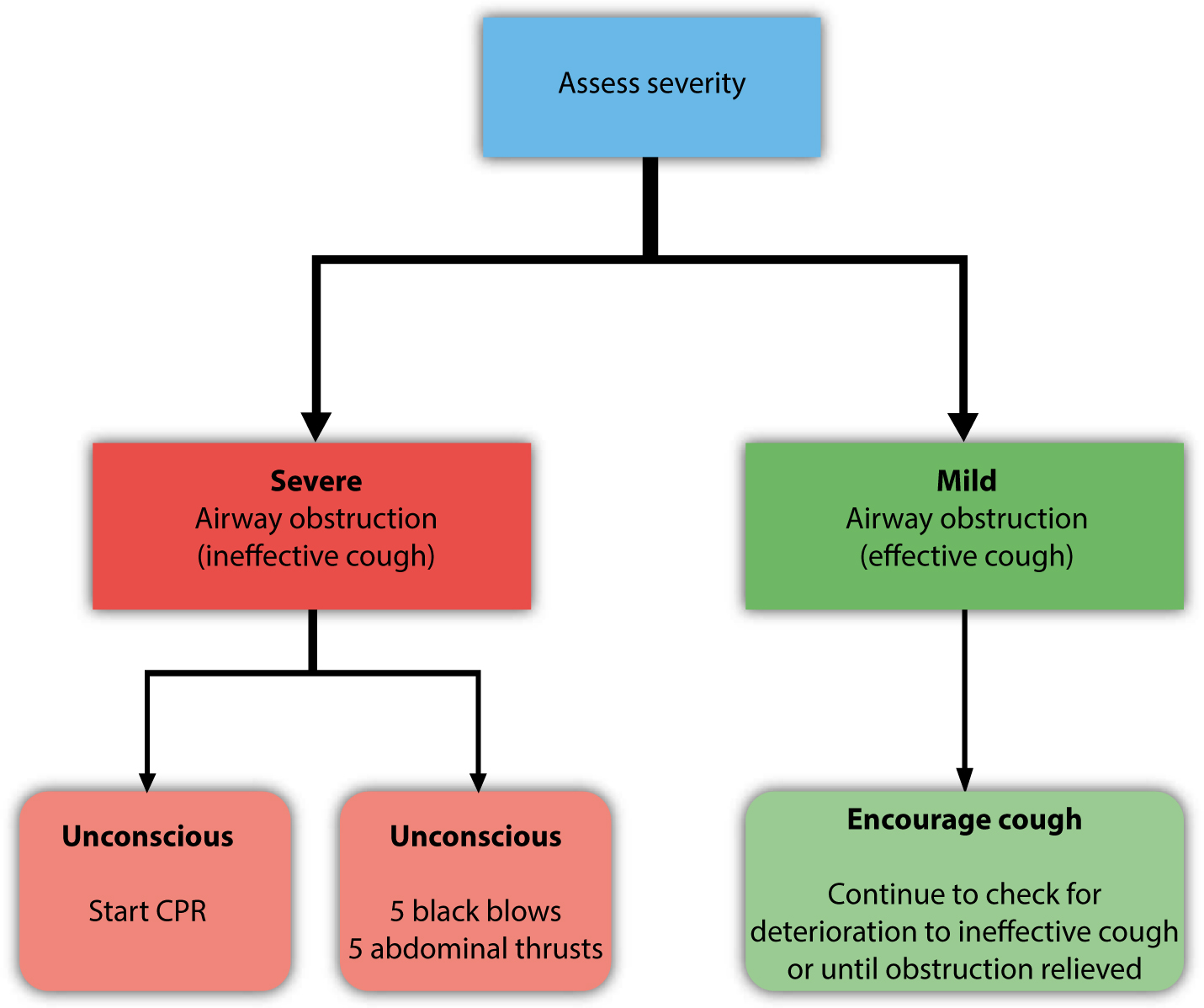
Victims are initially conscious and responsive therefore early intervention is imperative. Resuscitation Council (UK) guidelines stress the importance of early identification of a blocked airway and highlight groups of patients at increased risk of choking, including those with reduced consciousness (eg sedated patients), drug and/or alcohol intoxication, neurological impairment with reduced swallow and cough reflex, respiratory disease, mental impairment, dementia, poor dentition and older age. The choking algorithm presented in Figure 8 divides choking into mild and severe. For mild airway obstruction the Resuscitation Council (UK) recommends encouraging the patient to cough. For severe airway obstruction they recommend back blows, abdominal thrusts and chest thrusts. Anecdotal and retrospective data show that a combination of these techniques are usually utilized. For an unresponsive patient the Resuscitation Council (UK) recommends chest compressions and CPR. The guidelines recommend that medical advice is sought following recovery for those who have a persistent cough, have difficulty swallowing or the sensation that something is still in their throat, as there is a risk that some material may still remain in the upper or lower airways. Those who have received abdominal thrusts or chest compressions should also seek medical advice owing to the risk of serious internal injuries.
Figure 8. The choking algorithm. (Reproduced with the kind permission of the Resuscitation Council (UK)).
Resuscitation of children
For ease of teaching, the guidelines recommend the adult BLS sequence is utilized, however, they also recommend that it may be useful to give five rescue breaths initially before delivering chest compressions. If you are on your own, perform CPR for one minute before seeking help and compress the chest by 4 cm for infants with 2 fingers, or 5 cm for older children with one or two hands (Figure 9).
Figure 9. Correct hand position for CPR in an infant.
Summary
The new Resuscitation Council UK guidelines highlight certain aspects with regards to BLS and AEDs. They emphasize the critical importance of the interactions between the emergency medical dispatcher, the bystander performing CPR and deployment of an AED in order to have an optimal outcome for out of hospital cardiac arrest. Interestingly, the Resuscitation Council UK suggests the possible registration of AEDs with emergency services so that a CPR provider may be directed to the nearest one, thereby facilitating early deployment of an AED and a better outcome for the victim. The guidelines also highlight the importance of early recognition of cardiac arrest in the presence of seizures or agonal breathing. The publication of the updated guidelines serves as a reminder to the clinical team of the importance of being up to date with recognition and treatment of cardiac arrest and choking and how seamless interaction between members of both the dental and medical teams improves long term outcomes for patients.