The immune system: basis of so much health and disease: 3. adaptive immunity Crispian Scully Eleni A Georgakopoulou Yazan Hassona Dental Update 2024 44:4, 707-709.
The immune system is the body's primary defence mechanism against infections, and disturbances in the system can cause disease if the system fails in defence functions (in immunocompromised people), or if the activity is detrimental to the host (as in auto-immune and auto-inflammatory states). A healthy immune system is also essential to normal health of dental and oral tissues. This series presents the basics for the understanding of the immune system; this article covers adaptive immunity.
Clinical Relevance: Dental clinicians need a basic understanding of the immune system as it underlies health and disease.
Article
Crispian Scully Eleni A Georgakopoulou Yazan Hassona
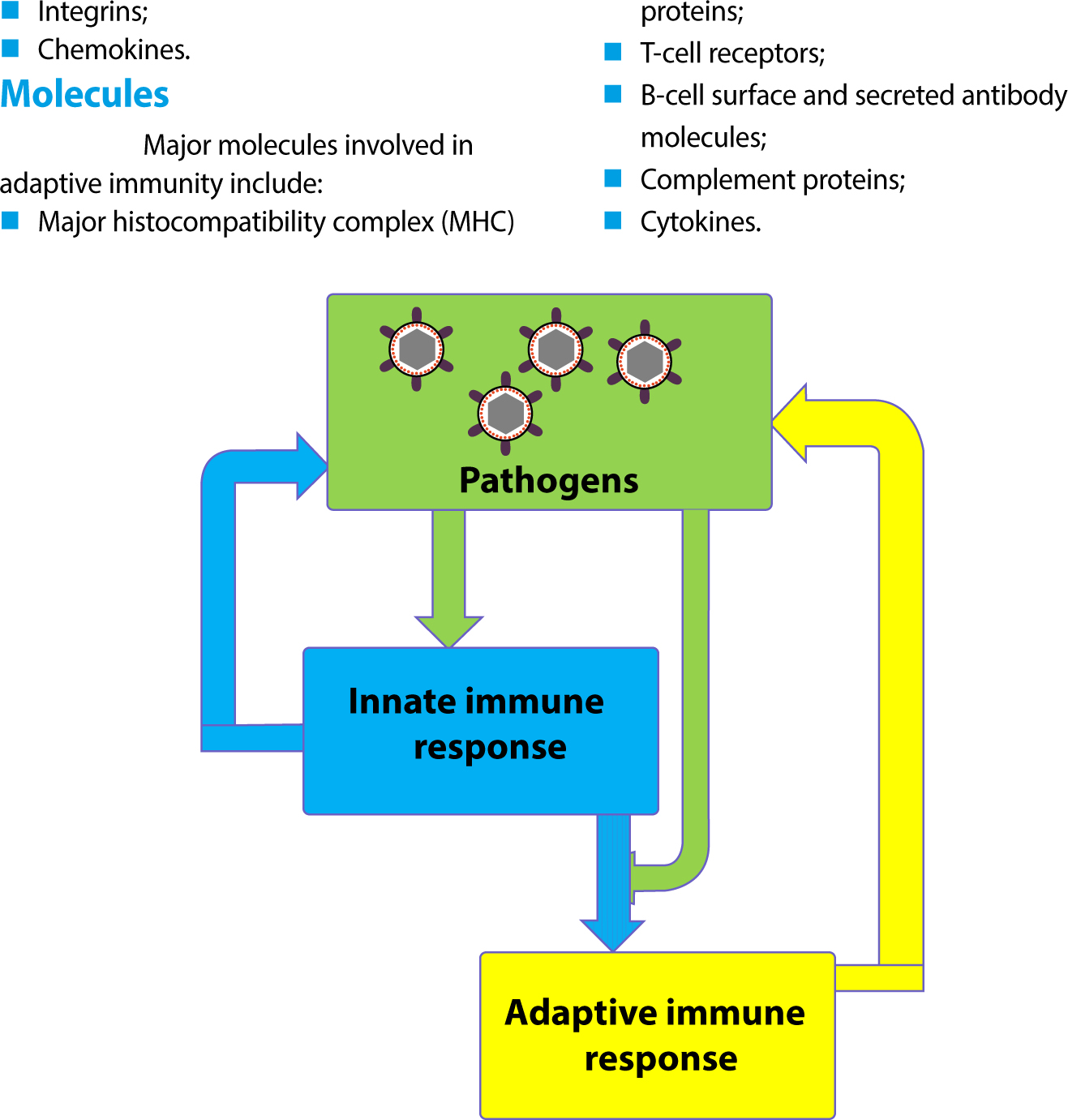
At times when ‘smart pathogens’ pass undetected through the innate immune barriers, the immune system reacts in a more complex defensive way, by launching the adaptive (acquired) immune response. The innate immune response (Article 2) calls the adaptive immune responses into play, and both then work together to eliminate pathogens (Figure 1). The adaptive immune responses react specifically and develop memory for subsequent exposure to the same pathogen.
Figure 1. Innate immune responses are activated directly by pathogens and defend organisms against infection. Pathogens, together with the innate immune responses they activate, stimulate adaptive immune responses, which then help fight the infection.
There are two broad classes of adaptive immune responses; antibody responses (humoral) and cell-mediated responses.
Humoral immunity deals with extracellular pathogens (ie most bacteria) and involves the production and release of antibodies (immunoglobulins) that bind and destroy target antigens.
Cell-mediated immunity deals with intracellular pathogens (ie viruses, fungi and some bacteria such as mycobacteria, eg tuberculosis), and involves direct lysis of infected cells and release of a wide range of proteins (cytokines) that also enhance antibody production and phagocytosis.
Cells and organs
The main cells that mediate adaptive immunity are white blood cells (leukocytes) termed immunocytes – mainly lymphocytes:
B lymphocytes mediate the humoral immune response through secretion of antibodies; while
T lymphocytes mediate the cell-mediated immune response.
B-cells and T-cells derive their names from the organs in which they develop:
B-cells develop in the liver in the foetus and bone marrow in adults;
T-cells develop in the thymus.
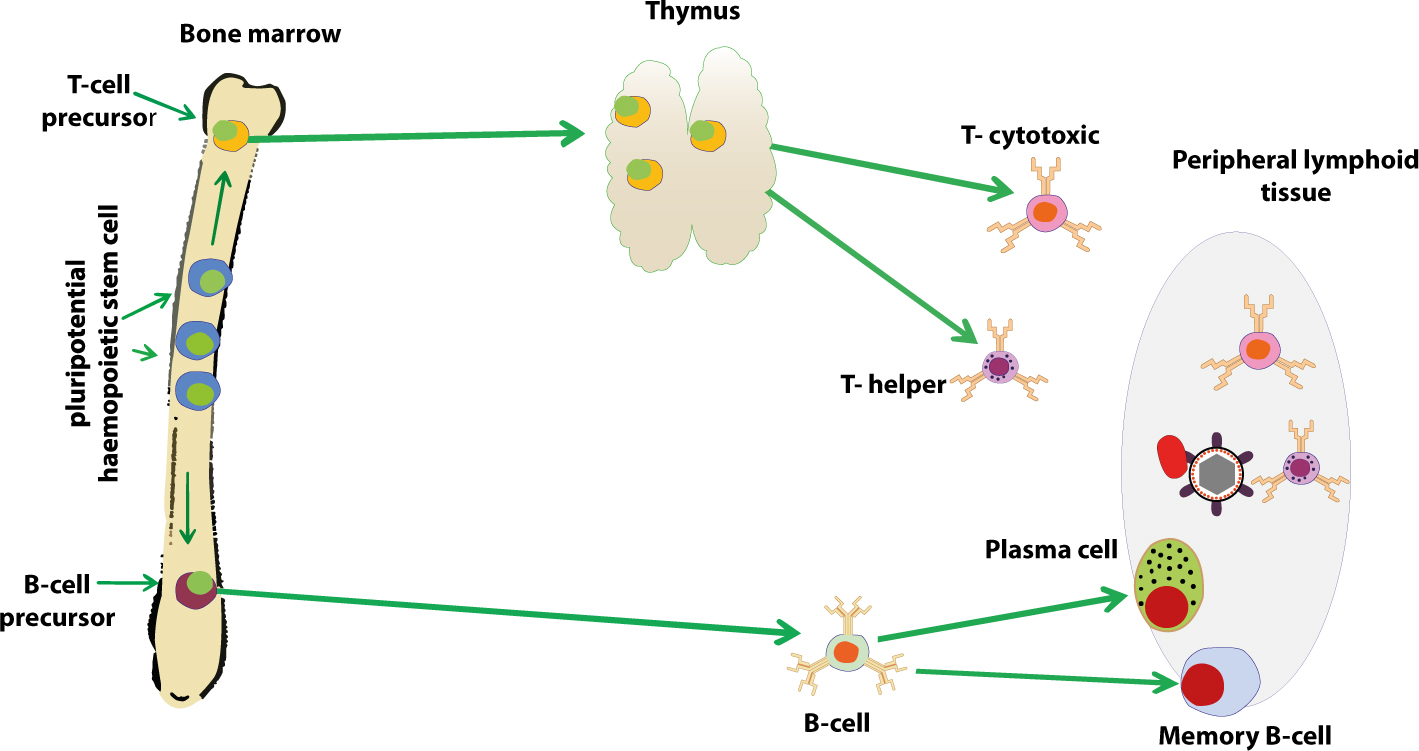
Despite their different origins, both B- and T-cells develop from the same pluripotential bone marrow haemopoietic stem cell (Figure 2).
Figure 2. The central lymphoid organs, where lymphocytes develop from precursor cells, are the bone marrow and the thymus. Lymphocytes respond to antigen in peripheral lymphoid organs, such as lymph nodes or spleen where they differentiate and become activated cells.
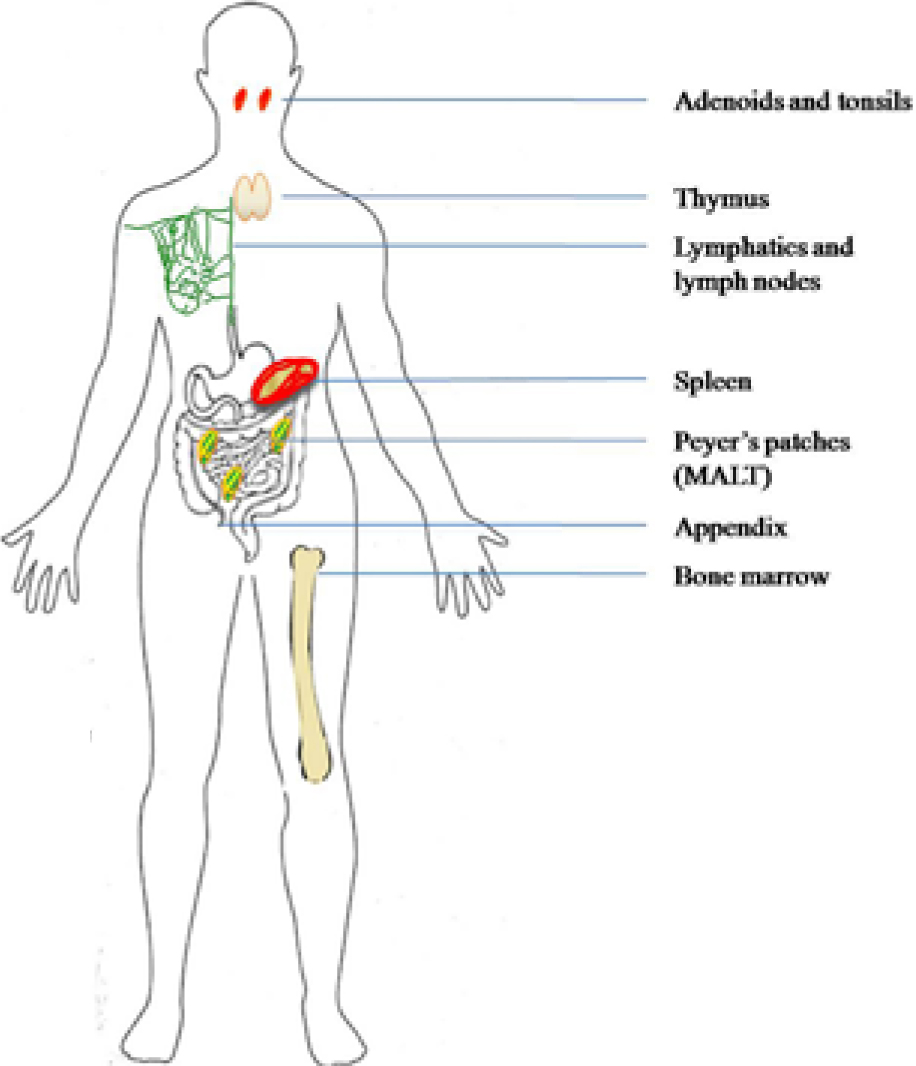
The bone marrow and the thymus are thus referred to as central (primary) lymphoid organs because they are sites where lymphocytes develop from precursor cells (Figure 3).
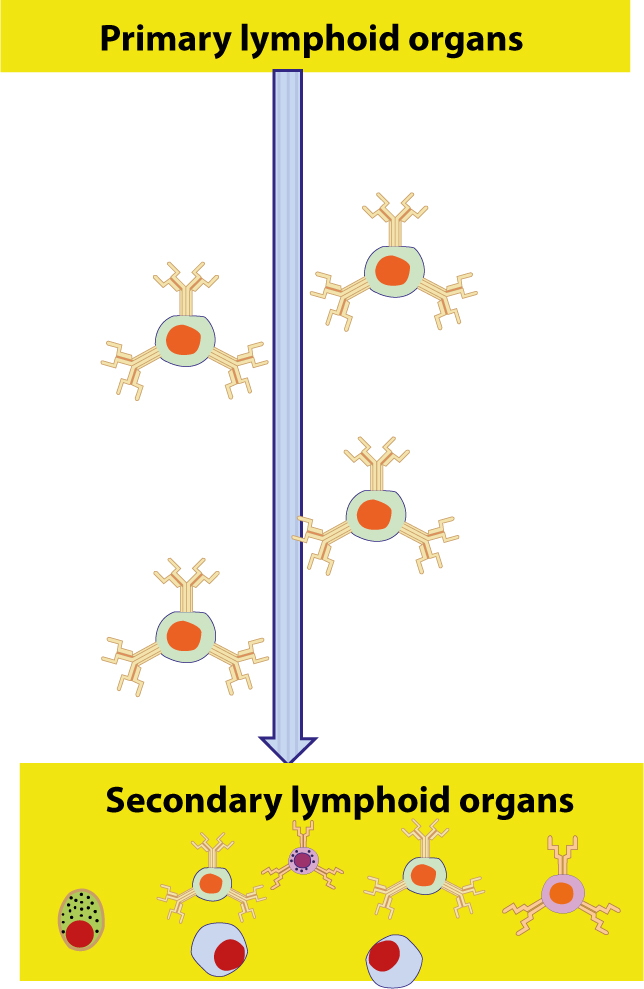
Figure 3. Lymphocytes develop in the thymus and bone marrow which are therefore called central (or primary) lymphoid organs. The newly formed lymphocytes migrate from these primary organs to peripheral (or secondary) lymphoid organs, where they can react with foreign antigens.
Lymphocytes mature and migrate via the blood and lymphatics to the peripheral (secondary) lymphoid organs where they react with foreign intruders (pathogens). These secondary lymphoid tissues include (Figure 3):
Lymph nodes: host the response to lymph-borne antigens;
Spleen: hosts the response to blood-borne antigens;
Mucosa-associated lymphoid tissue (MALT): includes all the lymphoid tissues associated with mucosae (eg skin, respiratory tract, gastro-intestinal tract) and protects mucosal surfaces. Peyer's patches, for example, are a major site of lymphocyte priming to antigens crossing the small intestinal mucosa.
Table 1 summarizes the main functions of immune organs involved in adaptive immunity.
Organ
Functions
Bone marrow
Haematopoiesis: production of blood cells including immunocytes
Spleen
The largest and most prominent lymphoid organ which has an important role in monitoring blood cell integrity, filtering and processing foreign material, and providing an environment for generation of immune responses
Thymus
The nursery for T lymphocyte maturation
Lymphatics
Remove excess fluids from tissues, circulate immunocytes, and absorb fatty acids and subsequently transport fat, as chyle, to the vasculature
Lymph nodes
A lymph node consists of a cortex, paracortex and medulla and is enclosed by a capsule
The tissue fluid drains via afferent lymphatics to lymph nodes to be ‘filtered’ and pass out from the lymph node medulla through the efferent lymphatics
The lymph node cortex contains B lymphocytes aggregated into primary follicles which, following stimulation by an antigen, develop a focus of active proliferation (germinal centre) and are then termed secondary follicles. These follicles are in intimate contact with antigen presenting cells (APCs).
The lymph node paracortex contains T-cells
The lymph node medulla contains both T- and B-cells
After leaving the primary lymphoid organs, lymphocytes present as:
Naïve cells that have matured and left the bone marrow or thymus, have entered the lymphatic system, but have yet to encounter their cognate antigen. After this, lymphocytes become either:
Effector (activated) cells actively involved in eliminating pathogens; or
Memory cells – survivors of past infections – which remain for a considerable period of time (Figure 4).
Figure 4. Naïve lymphocytes have matured and left the bone marrow or thymus, and have entered the lymphatic circulation system, but have yet to encounter their cognate antigen. After encountering antigens in the peripheral lymphoid organs, naïve lymphocytes become activated and known as effector cells. Memory cells are lymphocytes that survived past infections. These cells remain for a considerable period of time.
B- and T-cells become morphologically distinguishable from each other only after they have been activated by an antigen; non-activated B- and T-cells look very similar.
Effector B-cells, also known as plasma cells, secrete antibodies that circulate and coat pathogens – targeting them for phagocytosis and complement activation;
There are two main classes of effector T-cells:
Cytotoxic T-cells (Tc): kill infected cells by means of proteins that they either secrete (cytokines) or display on their surface; and
Helper T-cells (Th): help to activate B-cells, macrophages and Tc cells through cell surface and secreted proteins (cytokines).
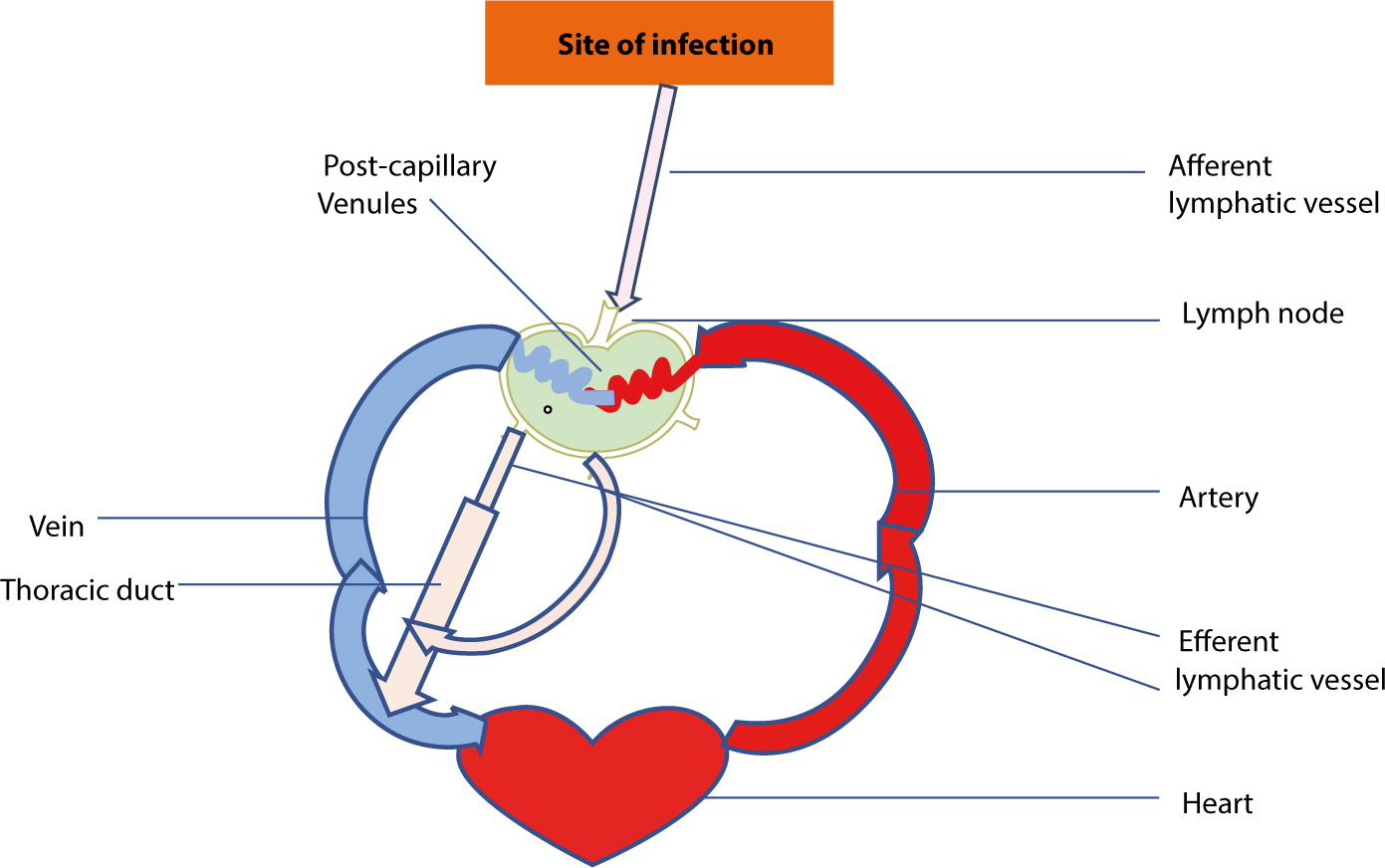
Lymphocytes continuously circulate between the lymph and blood until they encounter their antigen. Resting or naïve lymphocytes leave the bloodstream moving into lymphatic tissues (eg lymph nodes) by squeezing across post-capillary venules. After moving through the node, lymphocytes connect with other lymphatic vessels that pass through other lymph nodes. Eventually, lymphocytes pass through the main lymphatic vessels (thoracic duct and right lymphatic duct) which carry them back into the blood. This continuous re-circulation ends only when the lymphocyte encounters its specific antigen in a peripheral lymphoid organ where it proliferates and differentiates into effector cells (Figure 5).
Figure 5. The path followed by lymphocytes as they continuously circulate between the lymph and blood. T- and B-cells enter the lymph node via an artery and migrate out of the bloodstream through post-capillary venules. Unless they encounter their antigen, the T- and B-cells leave the lymph node via efferent lymphatic vessels, which eventually join the thoracic duct. The thoracic duct empties into a large vein carrying blood to the heart.
Lymphocyte migration is controlled by adhesion molecules and chemokines expressed on endothelial surfaces. Adhesion molecules which control leukocyte migration include:
Cell adhesion molecules (CAMs);
Selectins and their carbohydrate ligands;
Integrins;
Chemokines.
Molecules
Major molecules involved in adaptive immunity include:
Major histocompatibility complex (MHC) proteins;
T-cell receptors;
B-cell surface and secreted antibody molecules;
Complement proteins;
Cytokines.
Major histocompatibility complex proteins (MHC)
These bind to antigens on cell-associated microbes, such as viral proteins, and display them on the cell surface for recognition by T-cell receptors. In addition to the direct binding of antigens on the surface of foreign pathogens, B-cell receptors can be secreted from activated B-cells (plasma cells) to create soluble antigen receptors termed antibodies.
Antibodies (immunoglobulin proteins)
Antibodies can bind with specificity and high affinity to pathogen antigens and either neutralize them or aid in their killing (see Article 7). Antibodies bind to bacteria and the antigen-antibody complex (immune complex) is then phagocytosed by phagocytic leukocytes (macrophages and polymorphonuclear neutrophilic leukocytes [PMNLs]), and also activates complement.
Complement
Complement is a complex system of plasma proteins which largely functions to kill bacteria and virally-infected cells directly and causes blood vessel dilatation (vasodilatation) and attracts defensive leukocytes to the area (this is inflammation) (see Article 9). Inflammation is utilized by ‘immunity’ to help combat infections; where complement is activated inflammation usually results and, conversely, where there is inflammation, complement has usually been activated. Inflammation is typically protective but can also cause disease.
Cytokines
Cytokines are various protein molecules secreted by immune cells that serve to regulate the immune system and the inflammatory process. Cytokines include the many:
Interleukins (ILs);
Tumour necrosis factor (TNF) proteins;
Chemokines – control the many leukocytes involved in immunity which have to communicate with each other and with other key cell populations such as vascular endothelial cells (Article 6).
Characteristics
Features of acquired immune responses include:
Specificity;
Memory of previous antigenic exposure;
Memory B-cells.
Specificity is a major feature
The major power of the acquired (adaptive) immune system is its ability to induce clonal proliferation and thus dramatically increase the number of specific B- or T-cells needed to deal with a specific pathogen.
Memory of previous antigenic exposure
This is achieved by some B- and T-cells transforming into memory cells (distinguishable from naïve cells by different cell-surface markers). Memory cells can respond in an accelerated fashion to a cognate antigen, and others home to the lymph nodes where they provide a reservoir of cells able to proliferate (resulting in lymphadenitis) and re-inforce the response against a further challenge with the same antigen. Homing of lymphocytes is determined by chemokines receptors and other cell surface transmembrane proteins.
Memory B-cells
These also respond in an accelerated manner to a second antigenic challenge. Their receptors have an increased affinity for antigen, and the B-cells are activated by lower concentrations of antigen. Thus antibody titres rise faster, and reach higher levels in the secondary immune response, than in the primary response and, as the B-cells have been through the process of affinity maturation, the antibody produced is of greater specificity.
Conclusion
The adaptive (acquired) immune response is thus characterized by:
Second exposure to the same agent producing a qualitatively (faster) and quantitatively (larger) response from that made in the first (initial) immune response;
Response being highly discriminatory;
Response anticipating all possible variants of the original stimulus;
Response involving lymphoid cells such as B and T lymphocytes:
B lymphocytes produce humoral responses (antibody–mediated) via plasma cells;
T lymphocytes are central to cell-mediated immunity.