Beal R. Clarke Dental Equipment Sales Ltd. Personal communication. 2015;
Gulson AD, Holroyd JR. PHE-CRCE-023 Guidance on the Safe Use of Hand-held Dental X-ray Equipment.Chilton, Oxford: Public Health England; 2016
McGiff TJ, Danforth RA, Herschaft EE. Maintaining radiation exposures as low as reasonably achievable (ALARA) for dental personnel operating portable hand-held x-ray equipment. Health Phys. 2012; 103:(2)S179-185
Gray JE, Bailey ED, Ludlow JB. Dental staff doses with handheld dental intraoral x-ray units. Health Phys. 2012; 102:137-142
Goren AD, Bonvento M, Biernacki J, Colosi DC. Radiation exposure with the NOMAD portable X-ray system. Dentomaxillofac Radiol. 2008; 37:109-112
Pittayapat P, Oliveira-Santos C, Thevissen P Image quality assessment and medical physics evaluation of different portable dental X-ray units. Forensic Sci Int. 2010; 201:112-117
Makdissi J, Pawar RR, Johnson B, Chong BS. The effects of device position on the operator's radiation dose when using a handheld portable X-ray device. Dentomaxillofac Radiol. 2016; 45 https://doi.org/10.1259/dmfr.20150245
Hosseini Pooya SM, Hafezi L, Manafi F, Talaeipour AR. Assessment of the radiological safety of a Genoray portable dental X-ray unit. Dentomaxillofac Radiol. 2015; 44
Kim E-K. Effect of the amount of battery charge on tube voltage in different hand-held dental x-ray systems. Imaging Sci Dent. 2012; 42:1-4
Berkhout WE, Suomalainen A, Brüllmann D, Jacobs R, Horner K, Stamatakis HC. Justification and good practice in using handheld portable dental X-ray equipment: a position paper prepared by the European Academy of DentoMaxilloFacial Radiology (EADMFR). Dentomaxillofac Radiol. 2015; 44
Hand-held dental X-ray equipment is increasingly being purchased for use in general dental practice. The aim of this paper is to update the practitioner with recently published recommendations on the requirements for hand-held devices. The article discusses the concerns often raised with the use of hand-held equipment including safety issues for the operator and the patient.
CPD/Clinical Relevance: It is important for dentists to be aware of the current guidance if considering the use of hand-held X-ray devices in their practice.
Article
Hand-held X-ray devices are becoming increasingly used in general dental practice. In the UK, one manufacturer has reported that they sold 385 units, with the majority being to dentists, with a smaller number being used for veterinary, forensic and industrial applications.1 The same manufacturer states that the total number of worldwide sales is approaching 20 000 units.1
Hand-held devices either resemble a gun and are held in one hand, or resemble a camera and are generally held with both hands. An example of each type is shown in Figures 1 and 2. The construction of the X-ray tube is similar to traditional intra-oral equipment. The most striking difference in the tubehead is a shield that is attached to the open-ended spacer cone. This is in place to protect the operator from backscatter.
Figure 1. Example of a gun style hand-held X-ray device – the Nomad Pro II. Note the unit has a backscatter shield and employs rectangular collimation. In clinical use the backscatter shield would be placed at the end of the spacer cone.Figure 2. Example of a camera style hand-held X-ray device – the Rextar X. Note again the unit has a backscatter shield and utilizes rectangular collimation.
Hand-held devices have the following potential advantages over traditional wall-mounted dental X-ray sets in the dental surgery:
A single unit could be used in a multi-surgery dental practice, cutting down on cost;
No installation is required;
As the operator remains next to the patient during the exposure, the operator can provide verbal reassurance throughout the procedure for nervous or anxious patients.
Public Health England recently advised that any hand-held equipment used for clinical use should fulfil certain requirements,2 including the following:
The unit should have rectangular collimation and be used in conjunction with an image receptor holder and beam aiming device. However, the arms on some holders clash with the protective shield on the end of the spacer cone so that the spacer cone has to be placed further from the skin surface. This is not desirable so some manufacturers now produce bespoke holders with shorter arms that allow the end of the spacer cone to be placed adjacent to the skin surface. Alternatively, the arm could be shortened on a standard holder to achieve the same result.
There should be safeguards to ensure that the equipment cannot be used by unauthorized users. This could be achieved by use of a PIN number to activate the control panel, or by a need to initiate exposures within a few seconds of enabling the exposure panel or by having an automatic ‘power off’ after a certain time of inactivity. Although at the present time none of the units has the pin number function, the Nomad Pro II (Figure 1) can be locked by pressing two separated buttons on the control pad. This ensures that X-ray exposures cannot be made. Most models also have an automatic power down/time out feature.
Sufficient lead shielding of the tubehead and backscatter shielding to restrict the annual effective dose to the operator below 0.25 mSv, and the annual equivalent dose to the hands of the operator to no more than 10 mSv.
A means of quickly and easily switching off the power or removing the battery without exposing the operator in an emergency situation.
However, there are four major concerns regarding the use of hand-held X-ray devices:
Operator safety;
Patient safety;
Image quality;
Security of unit.
Operator safety
There have been a number of publications relating to operator safety.3,4,5,6,7 These papers conclude that the operator dose using these systems is similar to the doses an operator would receive if using traditional X-ray equipment. One paper showed that the measured doses received by operators was actually lower than that received using a wall-mounted system.4 However, another paper measured the backscatter received by the operator and concluded that, in order to keep the received whole body dose below the 20 mSv per annum limit set by the International Commission on Radiological Protection, the number of exposures an operator could undertake would be 210, which is around 4 exposures per week.8 In addition, the maximum number of exposures that can be taken to keep the dose to the lens of the eye below the new recommended dose limit set by the International Commission on Radiological Protection (ICRP) is 180 exposures per annum.8 It should be pointed out, however, that this particular unit did not have the recommended backscatter shield.
The annual dose limit for an unclassified worker is 6 mSv per annum. The HPE guidelines suggest setting an annual dose constraint of 0.25 mSv for hand-held devices. The HPE tested five devices and only three of the models tested complied with this dose constraint.2
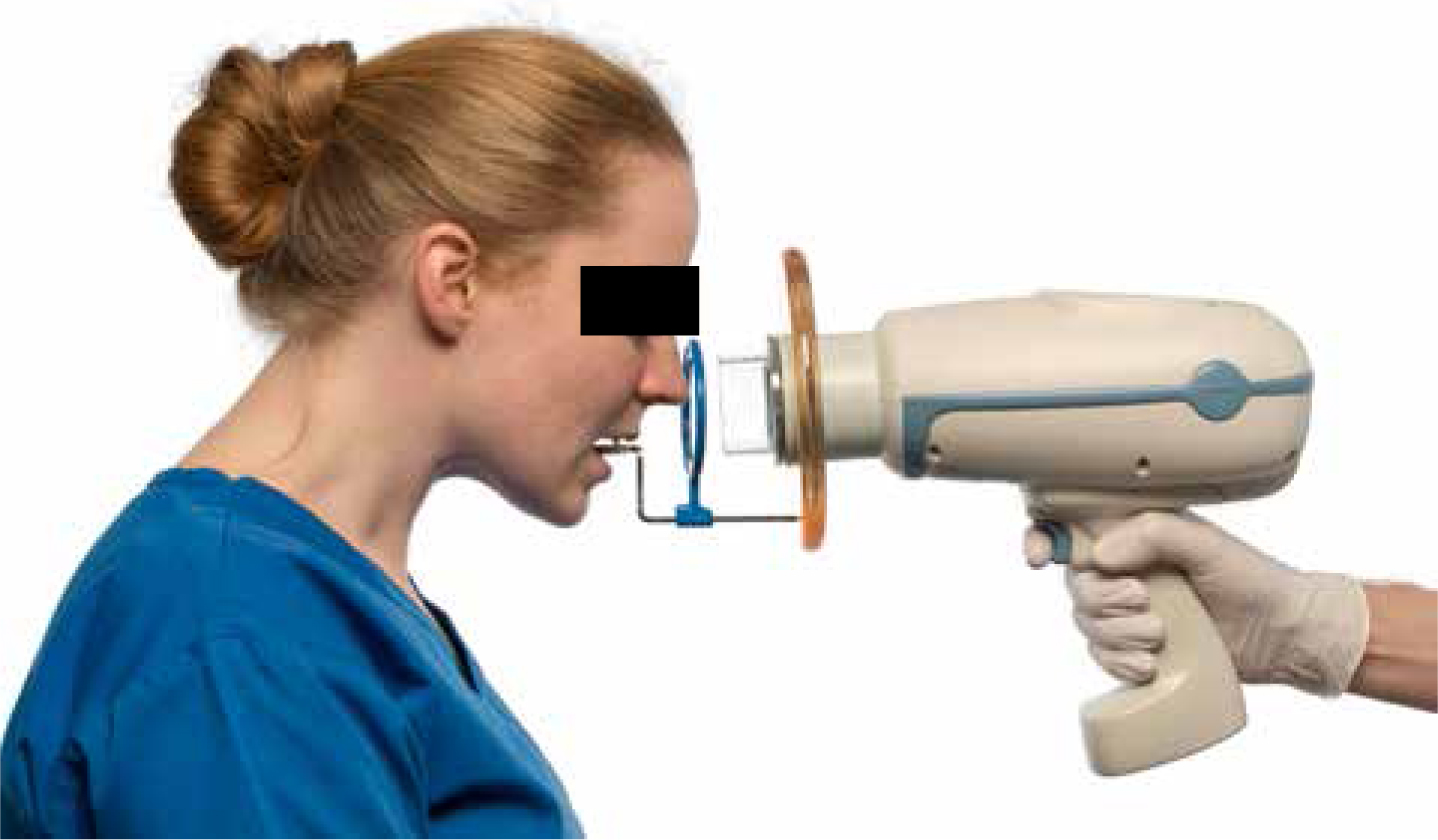
It seems that, overall, the doses to the operator can be kept below the dose limits set by the ICRP as long as the technique used by the operator is good. The operator should always have the backscatter shield on the unit and it should be placed to within 1 cm of the end of the spacer cone. The X-ray unit should be kept horizontal to ensure that the whole body of the operator is protected by the shield during the exposure. This may require the technique to be modified slightly, particularly in the positioning of the patient's head. Examples of this are shown in Figures 3 and 4. Most radiographic views taken in general dental practice can be acquired with hand-held units. However, views such as the lower 90 degree occlusal view cannot be carried out because the shield interferes with the positioning of the spacer cone underneath the patient's chin.
Figure 3. Patient positioned for a periapical view of the upper incisors. Note that the head has to be tipped forward so that the X-ray beam remains horizontal.Figure 4. Patient positioned for a periapical view of the upper left molars. Note that the head has to be tipped to the side so that the X-ray beam remains horizontal.
If a hand-held unit is chosen that meets the requirements of both the 2001 guidance notes for dental practitioners and the HPE guidelines on the safe use of hand-held X-ray equipment, and it is used correctly, then there is no need for the operator to wear Personal Protective Equipment (PPE), such as a lead apron or thyroid shield.
When buying new X-ray equipment, a prior risk assessment should be carried out and a full discussion should be carried out with the Radiation Protection Adviser as to the suitability of the equipment. When purchasing equipment, it should be sourced from a reputable dealer. Unfortunately, it is possible to buy cheap imported hand-held equipment over the internet. One particular piece of equipment was tested by the Health Protection Agency and it was found that, if it was used with a high workload, potential doses could be up to 40 Sv (equivalent dose) to the hands and 30 mSv (effective dose) to the body.9 These are clearly above the dose limits set by the ICRP. One unit had been purchased by a UK dentist. The HPA subsequently issued a medical device alert on this piece of equipment.9
Ideally, when using a hand-held unit in a surgery, the whole surgery should be designated a controlled area. Only the patient and the operator should be inside the controlled area when the exposure button is pressed. Access to the room should be restricted by either locking access doors or asking another member of staff to guard the entrance to the room.
Patient safety
In order to restrict the dose to the patient, equipment should be chosen that complies with the 2001 guidance notes for dental practitioners wherever possible.10 Equipment that operates at a high keV (between 60–70 KeV) and has a constant potential output should be selected. There should be no less than 1.5 mm aluminium filtration for X-ray sets operating up to 70 KeV. In addition, a long focus to skin distance (fsd) is advised.
This produces a near parallel beam that reduces the volume of the patient irradiated, reducing effective dose, and it also improves image geometry. A unit with an fsd of at least 200 mm should be chosen. As already discussed, rectangular collimation should be used in combination with image receptor holders and beam aiming devices. Rectangular collimators should be designed so that the beam size does not exceed 40 mm x 50 mm and preferably should not exceed 35 mm x 45 mm.
Hand-held units are battery operated and the units can make at least 100 exposures before the need for recharging. However, when low on charge the output can fall by as much as 10%.11 It is therefore suggested that units are kept fully charged to ensure optimal output.
A fast image receptor should be used – either a digital receptor or F-speed film. This ensures that the exposure times and subsequent radiation dose is kept as low as possible.
Image quality
To ensure consistent acceptable image quality, image receptor holders and beam aiming devices should always be used. As previously stated, the holder may need to be modified to ensure that the end of the spacer cone can be placed next to the skin surface and to ensure correct centring and angulation of the spacer cone. This ensures that the beam is perpendicular to both the tooth and image receptor.
As the unit is hand-held, there is a potential for movement of the unit during the exposure (particularly as the exposures can be longer than with wall-mounted units). Therefore, exposures of longer than one second should not be selected. However, the image quality of radiographs seems similar to that of conventional X-ray equipment,5 but the data to support this finding was not presented in the paper. One study tested three different devices used with four different image receptors. All the images were of acceptable quality but there were significant differences in image quality between the combinations of the X-ray devices and the sensor types studied.
Security
As the units are portable, there is potential for the units to be stolen and used without authorization outside the surgery. For this reason, the unit should be stored in a locked cupboard. If the unit is stolen, then the use of a PIN to activate an exposure would ensure that the unit cannot be used.
Indications
In a position statement prepared by the European Academy of DentoMaxillofacial Radiology it is stated that these devices should only be used in specific situations where the use of wall-mounted installations are either not possible or impractical.12 The indications for use are:
Intra-operative radiography when the patient is under general anaesthesia or sedation;
In emergency rooms if the patient is immobile;
When carrying out domiciliary visits to nursing homes or residential facilities;
In detention centre facilities;
When working in remote areas such as military operations abroad;
Dental support in rural areas in developing countries or isolated areas without dental facilities.
Conclusion
Although the indications in general dental practice are limited, there has been an increase in the number of units purchased. Therefore, if a dentist is considering buying one of these units, he/she is directed to the recent Health Protection England document which provides invaluable advice.2