Finch RG Adverse reactions to antibiotics, 4th edn. In: Greenwood D Oxford: Oxford University Press; 2000
Davies SD Annual Report of the Chief Medical Officer Vol 2.London: Department of Health; 2011
Review on Antimicrobial Resistance. (Accessed 12 June 2016)
Health and Social Care Information Centre. Prescription Cost Analysis – data 2015. (Accessed 12 June 2016)
Palmer NO, Pealing R, Ireland RS, Martin MV A study of therapeutic antibiotic prescribing in National Health Service general dental practice in England. Br Dent J. 2000; 10:554-558
Palmer NO, Martin MV, Pealing R Paediatric antibiotic prescribing by general dental practitioners in England. Int J Paediatr Dent. 2001; 11:242-248
Palmer NO, Martin MV, Pealing R An analysis of antibiotic prescriptions from general dental practitioners in England. J Antimicrob Chemother. 2000; 46:1033-1035
Tulip DE, Palmer NO A retrospective investigation of the clinical management of patients attending an out of hours dental clinic in Merseyside under the new NHS dental contract. Br Dent J. 2008; 205:659-664
Cope A, Francis NA, Wood F Antibiotic prescribing in UK general dental practice: a cross-sectional study. Community Dent Oral Epidemiol. 2016; 44:145-153
English surveillance programme for antimicrobial utilisation and resistance (ESPAUR) 2010–2014. Report 2015 Public Health England. (Accessed 12 June 2016)
General Dental Council. Standards for the Dental Team 2013. (Accessed 12 June 2016)
General Dental Council. Guidance on prescribing medicines 2013. (Accessed 12 June 2016)
London: Department of Health; 2010
, 2nd edn. London: Faculty of General Dental Practice (UK); 2012
Nagle D, Reader A, Beck M Effect of systemic penicillin on pain in untreated irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 90:636-640
London: Royal College of Surgeons of England; 1997
Pogrel MA Antibiotics in general practice. Dent Update. 1994; 21:274-280
Blum IR Contemporary views on dry socket (alveolar osteitis): a clinical appraisal of standardization, aetiopathogenesis and management: a critical review. Int J Oral Maxillofac Surg. 2002; 31:309-317
Noroozi AR, Philbert RF Modern concepts in understanding and management of the “dry socket” syndrome: comprehensive review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 107:30-35
London: NICE; 2008
Johnson BD, Engel D Acute necrotizing ulcerative gingivitis. A review of diagnosis, etiology and treatment. J Periodontol. 1986; 57:141-150
Matthews DC, Sutherland S, Basrani B Emergency management of acute apical abscesses in the permanent dentition: a systematic review of the literature. J Can Dent Assoc. 2003; 69
Matthews DC, Sutherland S Clinical practice guidelines on emergency management of acute apical periodontitis and acute apical abscess. Evid Based Dent. 2004; 5:7-11
Herrera D, Sanz M, Jepsen S A systematic review on the effect of systemic antimicrobials as an adjunct to scaling and root planing in periodontitis patients. J Clin Periodontol. 2002; 29:136-159
Herrera D, Alonso B, Leon R Antimicrobial therapy in periodontitis: the use of systemic antimicrobials against the subgingival biofilm. J Clin Periodontol. 2008; 35:45-66
Sgolastra F, Gatto R, Petrucci A Effectiveness of systemic amoxicillin/metronidazole as adjunctive therapy to scaling and root planing in the treatment of chronic periodontitis: a systematic review and meta-analysis. J Periodontol. 2012; 83:1257-1269
Zandbergen D, Slot DE, Cobb CM The clinical effect of scaling and root planing and the concomitant administration of systemic amoxicillin and metronidazole: a systematic review. J Periodontol. 2013; 84:332-51
Bonito AJ, Lux L, Lohr KN Impact of local adjuncts to scaling and root planing in periodontal disease therapy: a systematic review. J Periodontol. 2005; 76:1227-1236
Guerrero A, Griffiths GS, Nibali L Adjunctive benefits of systemic amoxicillin and metronidazole in non-surgical treatment of generalized aggressive periodontitis: a randomized placebo-controlled clinical trial. J Clin Periodontol. 2005; 32:1096-1107
Varela VM, Heller D, Silva-Senem MX Systemic antimicrobials adjunctive to a repeated mechanical and antiseptic therapy for aggressive periodontitis: a 6-month randomized controlled trial. J Periodontol. 2011; 82:1121-1130
Preshaw PM, Hefti AF, Bradshaw MH Adjunctive subantimicrobial dose doxycycline in smokers and non-smokers with chronic periodontitis. J Clin Periodontol. 2005; 32:610-616
Sgolastra F, Petrucci A, Gatto R Long-term efficacy of subantimicrobial-dose doxycycline as an adjunctive treatment to scaling and root planing: a systematic review and meta-analysis. J Periodontol. 2011; 82:1570-1581
National Institute of Health and Clinical Excellence (ESMPB1). Clostridium difficile infection: risk with broad-spectrum antibiotics. 2015. (Accessed 12 June 2016)
Martin MV, Longman LP, Hill JB Acute dentoalveolar infections: an investigation of the duration of antibiotic therapy. Br Dent J. 1997; 183:135-137
Slots J, Pallasch TJ Dentists' role in halting antimicrobial resistance. J Dent Res. 1996; 75:1338-1341
Scottish Intercollegiate Guidelines Network (SIGN). 2008. (Accessed 12 June 2016)
Siddiqi A, Morkel JA, Zafar S Antibiotic prophylaxis in third molar surgery: a randomized double-blind placebo-controlled clinical trial using split-mouth technique. Int J Oral Maxillofac Surg. 2010; 39:107-114
Lodi G, Figini L, Sardella A Antibiotics to prevent complications following tooth extractions. Cochrane Database Syst Rev. 2012; (Issue 11)
Lindeboom JA, Frenken JW, Valkenburg P The role of preoperative prophylactic antibiotic administration in periapical endodontic surgery: a randomized, prospective double-blind placebo-controlled study. Int Endod J. 2005; 38:877-881
Ireland RS, Palmer NO, Lindenmeyer A An investigation of antibiotic prophylaxis in implant practice in the UK. Br Dent J. 2012; 213:(8)
Abu-Ta'a M, Quirynen M, Teughels W Asepsis during periodontal surgery involving oral implants and the usefulness of peri-operative antibiotics: a prospective, randomized, controlled clinical trial. J Clin Periodontol. 2008; 35:58-63
Esposito M, Cannizzaro G, Bozzoli P Effectiveness of prophylactic antibiotics at placement of dental implants: a pragmatic multicentre placebo-controlled randomised clinical trial. Eur J Oral Implantol. 2010; 3:135-143
Esposito M, Grusovin MG, Worthington HV Interventions for replacing missing teeth: antibiotics at dental implant placement to prevent complications. Cochrane Database Syst Rev. 2013; (Issue 7)
Gould FK, Elliott TS, Foweraker J Guidelines for the prevention of endocarditis: report of the Working Party of the British Society for Antimicrobial Chemotherapy. J Antimicrob Chemother. 2006; 57:1035-1042
National Institute of Health and Clinical Excellence. CG64: Prophylaxis against infective endocarditis: antimicrobial prophylaxis against infective endocarditis in adults and children undergoing interventional procedures. NICE guidelines [CG64].2015. (Accessed 12 June 2016)
Dayer MJ, Jones S, Prendergast B Incidence of infective endocarditis in England, 2000–13: a secular trend, interrupted time-series analysis. Lancet. 2015; 385:(9974)1219-1228
British National Formulary. 2016. (Accessed 12 June 2016)
Berbari EF, Osmon DR, Carr A Dental procedures as risk factors for prosthetic hip or knee infection: a hospital-based prospective case-control study. Clin Infect Dis. 2010; 50:8-16
Lockhart PB, Loven B, Brennan MT The evidence base for the efficacy of antibiotic prophylaxis in dental practice. J Am Dent Assoc. 2007; 138:458-474
Bamias A, Kastritis E, Bamia C Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: incidence and risk factors. J Clin Oncol. 2005; 23:8580-8587
Hellstein JW, Adler RA, Edwards B Managing the care of patients receiving antiresorptive therapy for prevention and treatment of osteoporosis: Executive summary of recommendations from the American Dental Association Council on Scientific. J Am Dent Assoc. 2011; 142:1243-1241
Antimicrobial stewardship: systems and processes for effective antimicrobial medicine use. (Accessed 12 June 2016)
Antimicrobial resistance and antibiotic prescribing in dental practice Nikolaus O A Palmer Dental Update 2024 43:10, 707-709.
Authors
Nikolaus O APalmer
BDS, MFGDP(UK), PhD, FDS RCSEng, FFGDP(UK)
Research Fellow and Clinical Adviser in Dental Education Health Education England North West, Honorary Lecturer, School of Dentistry, University of Liverpool, Pembroke Place, Liverpool L3 5PS, UK (nikolaus.palmer@me.com)
The purpose of this paper is to review the principles of antibiotic prescribing in light of the increasing worldwide problem of antimicrobial resistance and the evidence of inappropriate use of antibiotics in dentistry. Guidance on the management of dental infections and antibiotic prophylaxis based on a review of the scientific evidence will be given to ensure good patient care.
CPD/Clinical Relevance: To discuss the relevance of legislation around antimicrobial prescribing and antimicrobial stewardship for dentists.
Article
Dentists prescribe antibiotics to manage oral and dental infections. The benefits of prescribing antibiotics are, however, limited by a number of problems associated with their use, eg side-effects, allergic reactions, toxicity and the development of resistant strains of microbes.1
Within the last few decades antimicrobial resistance (AMR) has become a worldwide problem and constitutes a major threat to public health. The Chief Medical Officer recently highlighted the level of this threat by describing it as ‘a ticking time bomb’ that should be put on the government's national risk register along with terrorism.2 AMR has increased as a result of widespread use providing greater opportunity for bacteria to exchange genetic material, so that resistant genes can spread between bacterial populations. The indiscriminate prescribing of antibiotics by healthcare professions continues to be targeted as a major factor to be addressed,2 especially as fewer and fewer new antibiotics are being developed. Although there are new agents in development, no new class of antibiotic has been brought into clinical use since the 1980s. As antibiotics become less effective, the healthcare gains such as organ/stem cell transplants, major surgery and chemotherapy, will be lost, leaving these patients with a higher risk of mortality. It is estimated that 700,000 people die of antibiotic resistant infections each year and that, by 2050, the cumulative global cost will be 30 million lives and between $60 and $100 trillion.3
Dentists working in NHS primary care prescribe nearly 9% of all the oral antimicrobials prescribed in primary care in England.4 The antibiotics prescribed by NHS dental practitioners are shown in Table 1. There is little robust data of dental antibiotic prescribing in secondary care. Although there is evidence of reduced antibiotic prescribing over the last few years in NHS primary care, evidence of the inappropriate use of antibiotics in dentistry is well documented and this contributes to the problem of increasing AMR.5,6,7,8,9 With this evidence and the clear link between the consumption of antibiotics in both primary and secondary care and the higher rates of resistance,10 it is imperative to ensure appropriate prescribing of antibiotics in dental practice.
Antibiotic
No of items
Percentage of all antibacterials
Penicillins
2,278,942
66.3
Metronidazole
972,869
28.3
Macrolides
149,996
4.4
Clindamycin
16,524
0.5
Cephalosporins
11,202
0.3
Tetracyclines
10,153
0.2
Total
3,439,686
100
What influences dentists' prescribing of antibiotics? Is it applying what was learnt as a student, an individual's clinical judgement, peer pressure, or is it based on scientific evidence and expert opinion? Whatever the influences, dentists have an ethical, legal and moral responsibility to prescribe antibiotics appropriately.11,12,13
What are the indications for prescribing antibiotics?
Antibiotics can be of benefit and may even be life-saving in medical and dental treatment, eg Ludwig's angina, brain abscess. The decision to use antibiotics, however, must be based on a thorough medical history, physical examination and a diagnosis. The indications for prescribing antibiotics in dental practice are listed below:
As an adjunct to surgical treatment of an acute or chronic infection;
To treat active infective disease, eg necrotizing ulcerative gingivitis;
Where definitive treatment may be delayed due to referral to specialist services, eg inability to establish drainage in an unco-operative patient requiring sedation or general anaesthetic;14
Rarely for prophylaxis.
Therapeutic antibiotic prescribing
The clinical indications for the therapeutic use of antibiotics are well documented and defined, namely, where there are signs of spreading infection, the patient feels unwell, is pyrexic (temperature over 38°C) and tachycardic (pulse over 100) and where there is marked regional lymphadenitis.14,15,16
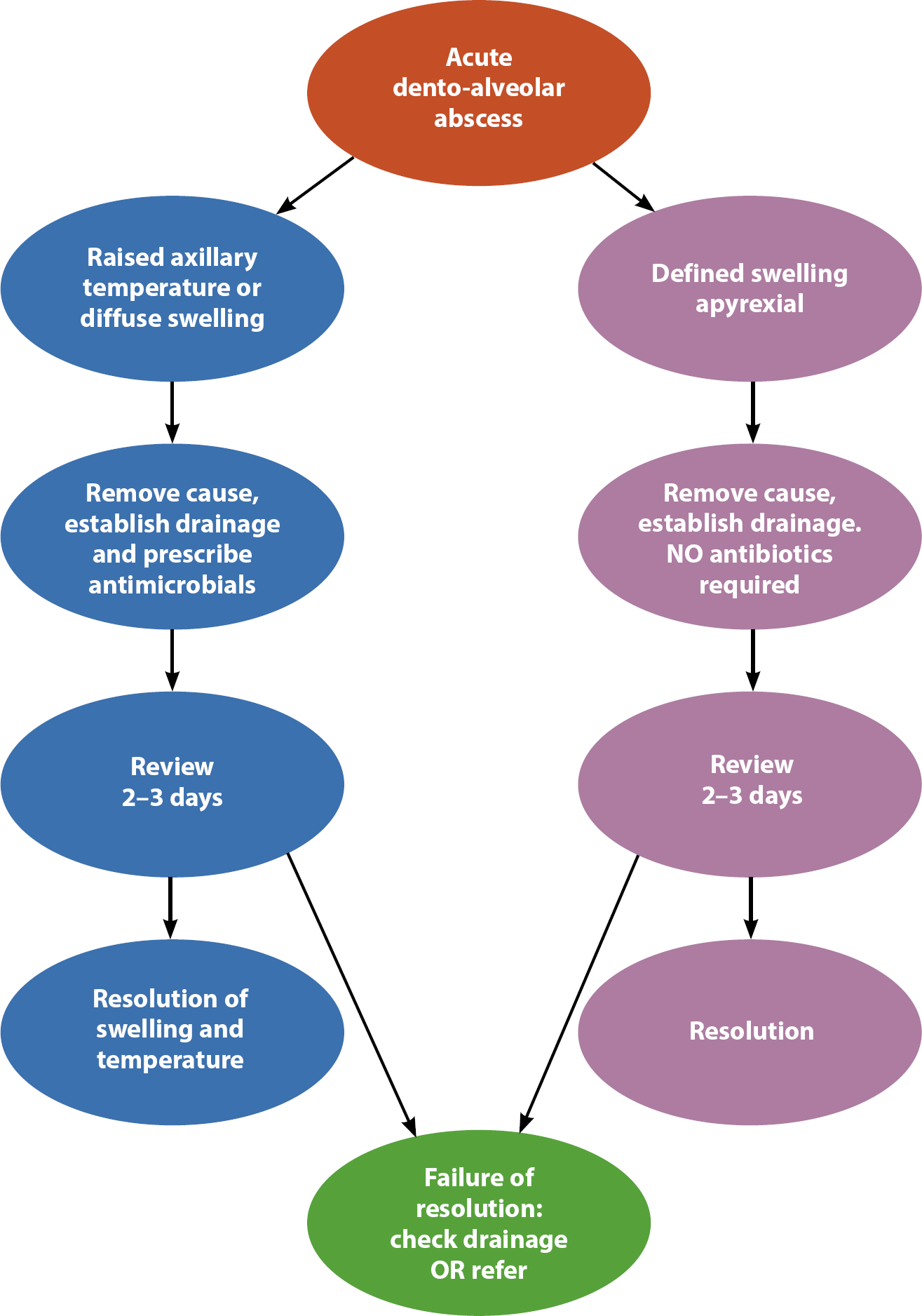
The majority of uncomplicated infected swellings of dental origin can be successfully treated by removal of the source of the infection by drainage of the associated abscess, removal of infected pulp contents or by extraction of the tooth. Unless the source of the infection is eradicated, any other mode of treatment will ultimately fail. The management of acute dento-alveolar infections is shown in Figure 1. Prescribing antibiotics as a temporary substitute for eradication of the cause of an infection also cannot be justified, except on rare occasions when it is impossible to remove the cause or establish drainage immediately.14
Figure 1. Management of acute odontogenic infections. Reproduced with kind permission of FGDP(UK).
Where there is an absence of infection there is no justification for the therapeutic prescribing of antibiotics. Antibiotics, for example, are not effective in the management of pain associated with irreversible pulpitis.17 The therapeutic prescribing of antibiotics ‘just in case’ problems may arise from recent treatment and can lead to serious problems in delaying diagnosis and subject patients to side-effects or toxicity.15
Inappropriate prescribing of antibiotics could amount to negligence or impairment of fitness to practise, particularly if there were no indications for antibiotics and a serious clinical outcome ensued.18 It is important that clinicians consider carefully the rationale for antibiotic use and balance this against alternative treatment approaches based on evidence, guidelines and best practice.11,14,19
Chronic dento-alveolar infections rarely require antibiotics unless there is evidence of gross local spread; extraction or root-canal therapy are the definitive treatment options.20 The routine use of antibiotics for acute pericoronitis is not required in the majority of these patients who can be treated effectively with local measures. These include irrigation of the pericoronal space, removal of the opposing tooth, or easing the occlusion, if there is trauma to the pericoronal tissues, and the use of appropriate analgesics. Following resolution of the acute phase, soft tissue surgery or removal of the associated tooth should be considered. Antibiotics should only be prescribed for pericoronitis when there is evidence of a spreading infection or systemic involvement is present.19
Evidence suggests that local measures also suffice in the treatment of dry socket.21,22 It is inappropriate for dentists to prescribe antibiotics routinely for dry socket as the benefit to risk ratio is unfavourable. There is also little indication for dentists to prescribe for uncomplicated sinusitis. Research has shown that antibiotics do not affect the clinical course of this condition.23
The use of systemic antibiotics in the treatment of periodontal disease remains controversial. The use of antibiotics for necrotic ulcerative gingivitis is recommended as part of the initial therapy only in the presence of systemic involvement.24 Chronic marginal gingivitis responds well to good plaque control and periodontal therapy and by its very nature is not an acute or spreading infection and does not require antibiotics. The majority of uncomplicated swellings of periodontal origin can be successfully treated by drainage of the associated abscess, by root surface debridement or extraction of the tooth.25,26
A review of current evidence shows that the routine use of systemic27,28,29,30 or local antimicrobials,31 as an adjunct to root surface debridement and good plaque control in the treatment of chronic periodontitis, produces no added clinical benefit. There is, however, evidence that systemic antibiotics may be of use in aggressive periodontitis in improving pocket depth reductions and gains in clinical attachment.28,32 These improvements though may only be short term.33
Host modulation therapy, in the form of sub-antimicrobial doses of tetracycline, has been suggested as an adjunct to root surface debridement in the management of periodontal disease. There is little evidence of an improvement in clinical outcomes when this therapy is used in primary care.34,35
Where there is an indication for therapeutic use of antibiotics the regimens to be employed are shown in Table 2. The first choice is a penicillin, such as amoxicillin.14 Phenoxymethylpenicillin is as effective but less reliably absorbed and needs to be taken on an empty stomach. Metronidazole is an excellent first line treatment for patients allergic to penicillin, or who have recently completed a course of penicillin, or if a predominantly anaerobic infection is suspected. A macrolide, such as azithromycin or clarithromycin, can be used as an alternative to penicillin. These are better tolerated than erythromycin, which causes nausea, vomiting and diarrhoea in some patients, and many organisms are resistant to it. It is calculated that NHS dentists prescribe 18% of all clindamycin prescribed in primary care.4 The prescribing of clindamycin, cephalosporins or co-amoxiclav offers no advantage in the management of dento-alveolar infections and could contribute to the development of resistance. Prescribing of these antibiotics has also been associated with the increased clostridium infections in primary and secondary care.36
First choiceAmoxicillin 500 mg three times daily for up to 5 days
OR
Phenoxymethylpenicillin 500 mg four times daily for up to 5 days If a predominately anaerobic infection is suspected then: Metronidazole 400 mg three times daily for up to 5 days
Second choiceMetronidazole 400 mg three times daily for up to 5 days
Third choiceClarithromycin 250 mg twice daily up to five days or Azithromycin 500 mg once daily for 2–3 days
Paediatric dosages should be based on the age and/or body weight of the patient-consult the British National Formulary50
Whenever managing a dental infection it is important to review after 2–3 days to assess whether the patient is responding to treatment. If antibiotics have been prescribed with definitive management, then the swelling should be resolving and the temperature of the patient returned to normal. If this is the case, antibiotics can be discontinued.37
Prophylactic prescribing of antibiotics
Prophylactic antibiotics have been recommended for patients who are susceptible to infection because of a preexisting disease and for the prevention of post-operative infection for procedures that carry a high risk of infection.
The use of antibiotics to prevent post-operative infection in healthy patients is not supported by experimental evidence and is inconsistent with the established principles of surgical antibiotic prophylaxis. It has been recommended that prophylaxis should only be for surgical procedures with high infection rates, eg open reduction fractures, orthognathic surgery and intra-oral bone grafting.38,39 Fortunately, within routine dentistry, in the presence of good infection prevention, there are no procedures recorded as having high rates of post-operative infection. Uncomplicated surgical removal of teeth and apicectomies rarely give rise to post-operative infections. Evidence exists showing that the prophylactic use of antimicrobials has little effect on post-operative pain, swelling, infection or wound healing.40,41,42
Prescribing prophylactic antimicrobials for implant placement remains controversial and research has shown a plethora of regimens used in the absence of guidelines.43 It has been shown that antimicrobials do not provide any significant advantage with regard to post-operative infections in the presence of good asepsis.44,45 A recent Cochrane review concluded that the oral administration of two grams of amoxicillin one hour before placement of dental implants to 25 people will prevent one person experiencing early implant loss.46
In the past, prophylactic antimicrobials have been prescribed to prevent bacteraemias and metastatic infection in medically compromised patients. Review of the research evidence has shown that the frequency of bacteraemias from normal oral function is greater than from dental procedures.47 Prior to the publication of NICE guidelines, patients with acquired or congenital endocardial disease were required to have antimicrobial prophylaxis before a number of dental procedures. NICE guidelines advise antimicrobial prophylaxis is no longer required for these patients.48 The recent publication of evidence of rising numbers of cases of infective endocarditis since adoption of NICE guidelines49 led to a review by NICE. This review showed no causal relationship and NICE reaffirmed that antimicrobial prophylaxis is not routinely required for dental procedures to prevent infective endocarditis.48
Medically compromised patients fall into a number of groups:
Patients who have prosthetic implants;
Patients who are immunocompromised;
Patients who have had radiotherapy to the jaws; or
Patients who are receiving bisphosphonates.
The Working Party of the British Society of Antimicrobial Chemotherapy advises that patients who have total joint implants do not require antibiotic prophylaxis prior to dental treatment.50 A recent case-controlled study confirmed that dental treatment is not a risk factor for subsequent joint replacement infections.51 Patients with cardiac pacemakers, penile, breast or intra-ocular implants and prosthetic grafts also do not need antimicrobial prophylaxis prior to dental treatment.52
Immune function of patients may be impaired by a range of conditions, such as leukaemia, immunosuppressive drugs following transplants, lymphomas, chemotherapy, poorly controlled diabetes and HIV. The importance of good dental health and treating odontogenic infections aggressively for these patients cannot be overemphasized. There is no clear evidence that these patients are at risk of infection as a result of routine dental procedures and, as such, antimicrobial prophylaxis is not required.50,52 It is important that all emergency treatment for immunocompromised patients should be carried out in conjunction with advice from the patient's specialist.
Osteoradionecrosis is a serious outcome of extractions in patients who have undergone radiotherapy to the head and neck region. It is known that this risk increases with time. Patients on bisphosphonate medication, particularly intravenous zoledronic acid, are also at risk of osteonecrosis.53 The efficacy of prophylactic antimicrobials for dental treatment is questionable due to poor blood flow and tissue penetration in both these groups of patients. Nevertheless, antimicrobial prophylaxis has been recommended by some authorities and these patients are best managed in a hospital environment. Patients on oral bisphosphonates do not require antimicrobial prophylaxis for routine dental treatment and can be managed in primary care.54
With the increasing problems of antimicrobial resistance, dentists should embrace NICE guidance on antimicrobial stewardship.55 Dentists, when considering prescribing of antimicrobials, should follow this guidance and take account of the risk of AMR, both for individual patients and the population as a whole, recording signs, symptoms, diagnosis and, if prescribing an antimicrobial, the clear reasons for prescribing.
All dentists in England have to follow the Health and Social Care Act code of practice which provides guidance on compliance in relation to antimicrobial prescribing (Criterion 3). The code of practice states that dentists must optimize patient outcomes, reduce the risk of adverse events, reduce the risks of AMR and have systems in place to manage and monitor prescribing to ensure appropriate use, eg clinical audit.13
Conclusion
Dentists should be aware of the increasing problem of AMR and be prudent in their prescribing of antibiotics. Wherever possible, dental practitioners should surgically manage dental infections and antibiotics should only be prescribed when necessary, based on patient symptoms, diagnosis and current guidelines. Dentists should also ensure that there are systems in place to monitor appropriate use.