McCafferty IJ, Jones RG Imaging and management of vascular malformations. Clinical Radiol. 2011; 66:1208-1218
Kilcline C, Frieden IJ Infantile hemangiomas: how common are they? A systematic review of the medical literature. Pediatr Dermatol. 2008; 25:168-173
Chang LC, Haggstrom AN, Drolet BA Growth characteristics of infantile hemangiomas: implications for management. Pediatrics. 2008; 122:360-367
Dubois J, Garel L, David M, Powell J Vascular soft-tissue tumors in infancy: distinguishing features on Doppler sonography. Am J Roentgenol. 2002; 178:1541-1545
Patino-Seijas B, Lorenzo-Franco F, Rey-Sanjurjo JL, González-Cuesta M, López-Cedrún Cembranos JL Vascular lesions: GLUT-1 expression as a diagnostic tool to discriminate tumours from malformations. J Oral Maxillofac Surg. 2012; 70:2333-2342
Mussalli NG, Hopps RM, Johnson NW Oral pyogenic granuloma as a complication of pregnancy and the use of hormonal contraceptives. Int J Gynaecol Obstet. 1976; 14:187-191
Sternberg SS, Antonioli DA, Carter D, Mills SE, Oberman H, 3rd edn. Philadelphia: Lippincott Williams & Wilkins; 1999
Sills ES, Zegarelli DJ, Hoschander MM, Strider WE Clinical diagnosis and management of hormonally responsive oral pregnancy tumour (pyogenic granuloma). J Reprod Med. 1996; 41:467-470
Taira JW, Hill TL, Everett MA Lobular capillary haemangioma (pyogenic granuloma) with satellitosis. J Am Acad Dermatol. 1992; 27:297-300
White JM, Chaudhry SI, Kudler JJ, Sekandari N, Schoelch ML, Silverman S Nd: YAG and CO2 laser therapy of oral mucosal lesions. J Clin Laser Med Surg. 1998; 16:299-304
Ishida CE, Ramos-e-Silva M Cryosurgery in oral lesions. Int J Dermatol. 1998; 37:283-285
Moon SE, Hwang EJ, Cho KH Treatment of pyogenic granuloma by sodium tetradecyl sulphate sclerotherapy. Arch Dermatol. 2005; 141:644-646
Izikson L, Nelson JS, Anderson RR Treatment of hypertrophic and resistant port wine stains with a 755nm laser: a case series of 20 patients. Lasers Surg Med. 2009; 41:427-432
Chapas AM, Eickhorst K, Geronemus RG Efficacy of early treatment of facial port wine stains in newborns: a review of 49 cases. Lasers Surg Med. 2007; 39:563-568
Garro SJ, Bradshaw WT Sturge-weber syndrome: a case study. Adv Neonatal Care. 2014; 14:96-102
Vikkula M, Boon LM, Mulliken JB Molecular genetics of vascular malformations. Matrix Biol. 2001; 20:327-335
Dubois J, Soulez G, Olivia VL, Berthiaume MJ, Lapierre C, Therasse E Soft-tissue venous malformations in adult patients: imaging and therapeutic issues. Radiographics. 2001; 21:1519-1531
Legiehn GM, Heran MK Classification, diagnosis and interventional radiologic management of vascular malformations. Orthop Clin North Am. 2006; 37:435-474
Cohen MM Vascular update: morphogenesis, tumours, malformations, and molecular dimensions. Am J Med Genet A. 2006; 140:2013-2038
Jussila L, Alitalo K Vascular growth factors and lymphangiogenesis. Physiol Rev. 2002; 82:673-700
Emery PJ, Bailey CM, Evans JN Cystic hygroma of the head and neck. A review of 37 cases. J Laryngol Otol. 1984; 98:613-619
Puig S, Casati B, Studenherz A, Paya K Vascular low-flow malformations in children: current concepts for classification, diagnosis and therapy. EurJ Radiol. 2005; 53:35-45
Kim SW, Kavanagh K, Orbach DB, Alomari AL, Mulliken JB, Rahbar R Long-term outcome of radiofrequency ablation for intraoral microcystic lymphatic malformation. Arch Otolaryngol Head Neck Surg. 2011; 137:1247-1250
Houdart E, Gobin YP, Casasco A, Aymard A, Herbreteau D, Merland JJ A proposed angiographic classification of intracranial arteriovenous fistulae and malformations. Neuroradiology. 1993; 35:381-385
Vascular anomalies constitute a diffuse group of conditions which can range in their significance from being completely harmless and of little clinical relevance to being potentially life threatening. It is important that dentists have a good understanding of these conditions so that the risk of potential complications of dental treatment in affected patients is reduced as much as possible. This article focuses on the pathogenesis, diagnosis and treatment of these conditions, with explanation on their relevance to the practising dentist.
CPD/Clinical Relevance: The paper describes several vascular anomalies that may be encountered in clinical practice with information that is relevant to their diagnosis and management.
Article
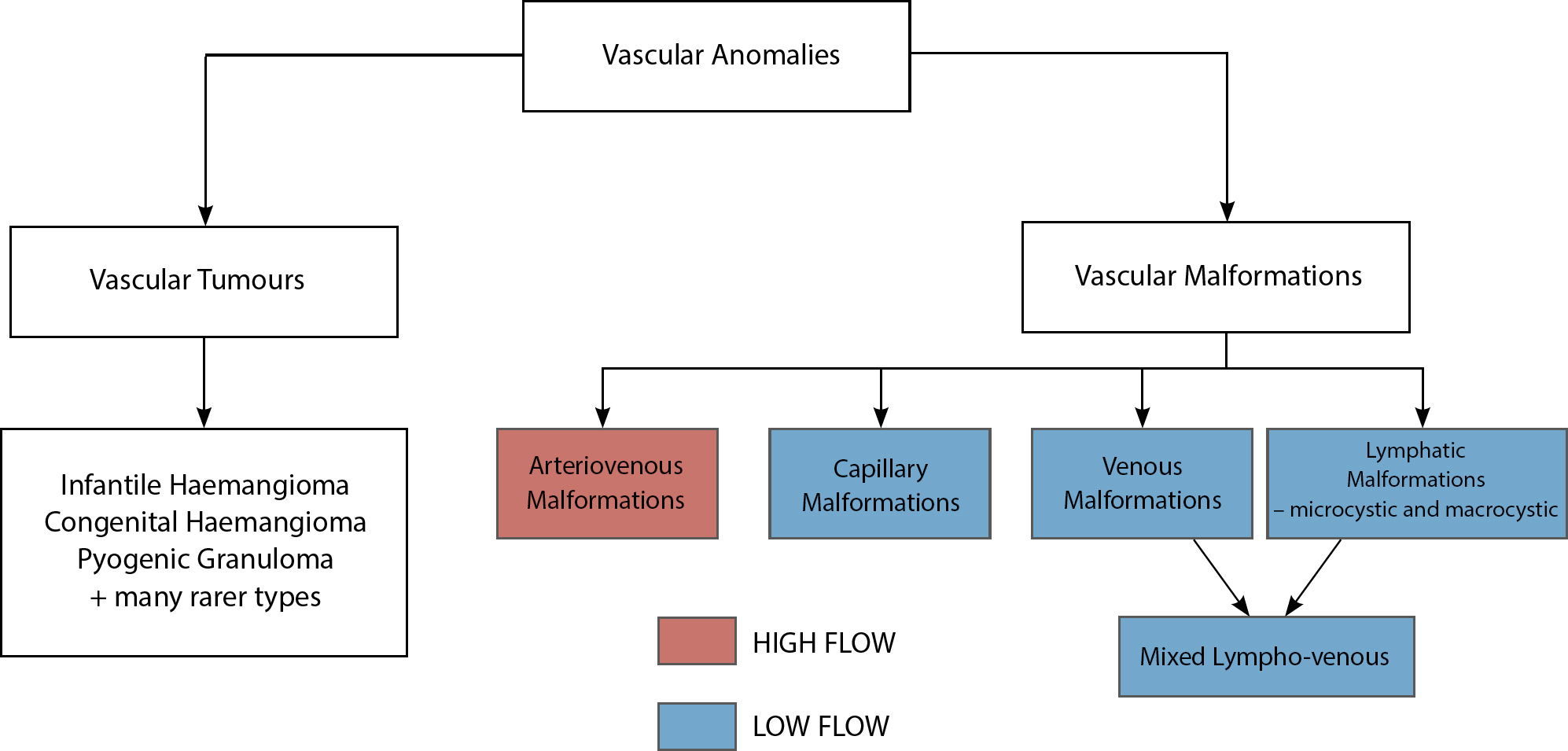
The umbrella term ‘vascular anomalies’ encompasses both ‘vascular malformations’ and ‘vascular tumours’ which are clinically distinct entities. Historically, there has been some confusion around the terminology used to describe the lesions and various attempts have been made to come up with a definitive classification of the conditions. The most widely accepted classification today is the ‘modified Mulliken Classification’1 (Figure 1).
Figure 1. Diagram of the modified Mulliken Classification.1
Vascular tumours
Vascular tumours are true neoplasms that exhibit pathologic vascular endothelial cell proliferation. Most of these are either infantile haemangiomas or congenital haemangiomas which differ in their clinical course.
Infantile haemangiomas
Infantile haemangiomas are the most common tumours of the head and neck in infants, affecting around 3–5% of children, females being affected more than males with a ratio of 3:1.2
At birth they are either undetectable or visible only as a precursor lesion. Typically, they manifest themselves clinically several weeks after birth, proliferating rapidly. In 80% of cases, the lesions finish growing by the time the child is 5 months old.3 When located superficially they appear as firm, isolated, raised, dark red lesions of the skin. If located as deeper masses in subcutaneous tissue, they may produce a blue hue in unaffected overlying skin. Colour Doppler ultrasound imaging is useful to visualize the features of these lesions and distinguish them from other vascular tumours.4 Immunohistochemistry can distinguish infantile haemangiomas from other vascular tumours or malformations due to the fact that infantile haemangiomas show positivity for the protein ‘glucose transporter-1’.5
In the head and neck they most commonly affect the lips, cheek and tongue. After a period of initial rapid growth they tend to undergo spontaneous regression over several years without leaving residual scarring. As a result most haemangiomas do not require surgical or interventional treatment and should solely be monitored. Treatment is usually reserved for rapidly growing lesions to prevent permanent anatomic distortion, scarring or functional impairment.1 These cases can be treated angiographically by embolization of feeding arteries which leads to regression of the lesions. Other treatments include the use of topical or systemic steroids, the beta-blocker Propanolol or surgical intervention, but these treatments are not without their side-effects. As they are typically diagnosed in infancy and may regress relatively quickly, infantile haemangiomas are unlikely to be seen by the practising dentist.
Congenital haemangiomas
Congenital haemangiomas are distinct from infantile haemangiomas in that they are already mature at birth and do not proliferate. They account for only 3% of all haemangiomas. Congenital haemangiomas may involute spontaneously and disappear by about one year of age. Non-involuting congenital haemangiomas are present at birth and remain stable, with no future growth or involution.
Figure 2. A pyogenic granuloma of the maxillary gingivae.
Pyogenic granulomas are true vascular tumours which most commonly affect the gingivae. The term ‘pyogenic granuloma’ is misleading as these lesions are neither pus producing nor granulomatous. A more appropriate term, which is histologically accurate and increasingly being used, is ‘lobular capillary haemangioma’. They are benign vascular tumours which usually develop following localized chronic irritation, traumatic injury or altered hormonal environment.6 Within the oral cavity they appear as smooth or lobulated exophytic erythematous papules, on either a pedunculated or sessile base. They are the most common intra-oral tumour, accounting for 75% of all cases, with the lips, tongue and buccal mucosa the other most commonly affected sites.7 Clinical development of the lesion is slow and painless; however, minor trauma can cause pronounced bleeding due to their highly vascular makeup. Although pyogenic granulomas may affect all ages, they most commonly affect females in the second decade of life, possibly due to the vascular effects of female hormones.8 Pyogenic granuloma of the gingivae is seen in around 5% of pregnancies.9 It is thought that poor oral hygiene, and localized factors such as improperly fitting restoration margins or calculus, can increase the likelihood of the lesions developing.
If a vascular tumour is suspected, the dentist should arrange for histological examination to establish an exact diagnosis. Differential diagnosis of pyogenic granuloma involves a number of different lesions, such as peripheral giant cell granuloma, peripheral ossifying fibroma, metastatic cancer, haemangioma, granulation tissue, Kaposi's sarcoma and Non-Hodgkin's lymphoma.8
Management of pyogenic granulomas depends on the severity of symptoms. When the lesion is small, painless and not causing problems by bleeding, it can be clinically observed and followed up without the need for surgical intervention. In pregnant women, treatment may not be needed owing to lesional shrinkage in the postpartum period.
If surgical excision is carried out it should be done in combination with thorough scaling to remove causative irritants, such as calculus and plaque or another source of trauma. Surgical excision should be down to the periosteum to prevent recurrence which has been reported in as many as 16% of cases.10 This is thought to be a result of incomplete excision, failure to resolve aetiologic factors or persisting injury to the area.8 Careful oral hygiene, removal of plaque and use of a soft toothbrush are important in preventing recurrence. Other treatment modalities include cryotherapy, laser excision or sclerotherapy; however, these are not commonly used.11,12,13
Vascular malformations
Vascular malformations are congenital defects of vascular morphogenesis and, unlike vascular tumours, show no endothelial cell proliferation. Although vascular malformations are clinically diverse, they share a common embryology and pathogenesis. They do not exhibit hyperplasia (as seen in vascular tumours) and are characterized histologically by a single layer of endothelial cells.
Vascular malformations broadly break down into either high flow or low flow lesions. They can involve arteries, veins, capillaries, lymphatic vessels, or a combination of these. Their clinical presentation depends upon the underlying vessel type and the anatomical site. They can result in minor cosmetic problems, ischaemic skin conditions, bleeding, pain or more disfiguring cosmetic or functional impairments.
Assessment and treatment of patients with vascular malformations should ideally be carried out in the multidisciplinary team setting. Key input should be sought from interventional radiology as well as departments of Oral and Maxillofacial surgery or Plastic surgery, as appropriate.
Some patients will not require active treatment for their condition, and explanation of the diagnosis and reassurance may be all that is needed. Treatment is generally reserved for those patients with significant symptoms and cases where the cosmetic impact of the lesions causes distress.
Low flow malformations
Low flow vascular malformations can be subdivided into capillary, venous, lymphatic or mixed (lymphovenous) malformations.
Capillary malformations
Capillary malformations, commonly termed ‘port wine stains’ or ‘naevus flammeus’ are congenital anomalies of capillary development and commonly appear in the superficial dermis. They are present at birth, gradually increasing in size with the growth of the child and are usually present for life without any tendency to involute. They occur in 0.3% of newborns14 and most commonly present in the head and neck region as pink macular lesions in the distribution of one or more divisions of the trigeminal nerve dermatomes. The lesions may change from pink in infancy to red in early adulthood to purple in middle age. They can evolve in later life to give a raised nodular cobblestone appearance which has a rubbery feeling upon palpation. The underlying cheek, lip or gingivae may also be affected presenting as gingival hypertrophy and chronic bleeding.
Small capillary malformations are benign and often do not require treatment. Larger capillary malformations may be treated as they can cause tissue hypertrophy in the skin, leading to substantial disfigurement. Treatment of large capillary malformations should be carried out before the age of 6 months, and usually involves pulse-dye laser photocoagulation.15
These lesions are also associated with a rare condition called ‘Sturge-Weber syndrome’ which has autosomal dominant inheritance with an incidence of approximately 1 in 20,000–50,000.16 It is characterized by its classic appearance as a ‘port wine stain’ usually unilaterally in the ophthalmic division of the trigeminal nerve. It is also associated with intracranial and ocular vascular malformations which may require urgent brain imaging and ophthalmologic investigation and treatment to prevent any life- or sight-threatening complications.
Venous malformations
Venous anomalies constitute the most common type of vascular malformation. They vary in morphology, being made up of abnormal venous channels of varying size and thickness which can predispose to local thrombosis. Their exact aetiology is unclear. Although present at birth (with an incidence of around 1–2 per 10,000), they often do not manifest themselves until later childhood.17 They may occur anywhere in the body with 40% in the head and neck region, 40% in the extremities and 20% in the trunk.18
Depending on their size and site, these venous malformations may have negative functional or cosmetic effects. Although usually painless, symptoms of pain and swelling can develop due to venous engorgement, localized thrombosis, a mass effect or localized haemorrhage. They are soft compressible masses, which may be bluish in colour if present on the skin or oral mucosa. On palpation, no pulsation or thrill is present. They classically empty on pressure and with elevation. Radiologically, 20% of these lesions will exhibit the presence of phleboliths which are pathognomic of venous malformations.19
These lesions quite frequently present to dentists as worrying ‘lumps’ or ‘growths’ within the oral cavity (Figure 3) and dentists should therefore be able to diagnose and reassure patients accordingly. The vast majority of patients with low flow lesions simply require education and reassurance that the lesions are completely harmless. Treatment is offered only for lesions where their intermittent expansion, contraction and localized thrombosis cause symptoms. The primary treatment of choice is sclerotherapy where agents, such as 3% sodium tetradecyl sulphate or ethanol, are injected into the lesion to cause destruction of endothelial cells and subsequent luminal obliteration, fibrosis and shrinkage of the lesion. Cryotherapy and irradiation can also be applied. Surgery tends to yield less satisfactory results except in cases where the lesion is small and well circumscribed.
Figure 3. A small venous malformation on the dorsum of tongue.
Lymphatic malformations
Lymphatic malformations are the second most common after venous malformations. They are often misnamed as ‘lymphangioma’ or ‘cystic hygroma’ but crucially lymphatic malformations are entirely distinct from those conditions. Lymphatic malformations do not exhibit cellular hyperplasia and are not neoplasms, neither do they have proliferative and involutive phases.20 They arise from defects in morphogenesis of the lymphatic vessels and consist of vessels and large chambers lined by a single layer of endothelial cells. They may form in the first few years of life and grow rapidly, thus requiring treatment. Lymphatic malformations can be subdivided into macro-and microcystic lesions, however, some are a combination of the two.
Microcystic lesions are composed of small channels and cysts measuring less than 2 mm in diameter lined by a single-layered endothelial lining on a background of solid matrix. They can be histologically diagnosed due to the fact that they express vascular endothelial growth factor receptor 3.21 They often involve the skin or buccal mucosa but can also affect the tongue (Figure 4), appearing as very small vesicles.
Figure 4. A microcystic lymphatic malformation of the tongue.
Macrocystic lesions contain lymphocytes and proteinaceous fluid in large spaces often divided by thick intralesional septae. Macrocystic lesions commonly occur in the first 2 years of life, primarily in the head and neck (70%), but can also occur in the trunk, limbs, mediastinum and abdomen.22 Macrocystic lymphatic malformations are typically subcutaneous, translucent in appearance with normal overlying skin and can be surgically removed. However, the appearance of these lesions is extremely variable. In extreme cases it can diffusely infiltrate adjoining anatomic regions and cause elephantiasis, and severe disfigurement. There can be bony distortion in cases of moderate to major facial involvement. The tongue can typically be affected where ‘mass effect’ causes mandibular overgrowth asymmetry and subsequent functional problems.
Both microcystic and macrocystic lymphatic malformations are prone to superimposed infection or spontaneous haemorrhage, leading to pain or rapid expansion.
On palpation they typically lack the pulsatile thrill of high-flow lesions, and do not compress. Ultrasound and MRI are used to assess these low flow lesions. MRI gives accurate imaging of all vascular anomalies and provides clear differentiation between the lesion and surrounding structures, enabling its exact extent and relationship to adjacent structures, such as neurovascular bundles, to be established.
Sclerotherapy is considered the primary treatment choice for treating macrocystic lymphatic malformations, and aims to obliterate the cystic spaces and achieve shrinkage.23 Microcystic lymphatic malformations tend to respond better to plasma radiofrequency ablation or intralesional bleomycin injections.24 Even so, treatment of both kinds of lesions often requires surgery.
High flow arteriovenous malformations
Arteriovenous malformations (AVM) are abnormal connections between arteries and veins which permit blood within an organ or tissue to bypass the capillary network, thus resulting in loss of the pressure down regulation that normally occurs. The dilated segment of vein distal to this connection is termed a ‘nidus’. Such high flow lesions can involve several arteries shunting to a single vein or multiple shunts between arteries and venules. Arteriovenous malformations can form during foetal development or develop after birth.25 They are rare and account for just 5% of mandibular vascular malformations.
Clinical history and examination can usually differentiate high and low flow lesions from one another, with various imaging techniques then being used to determine their morphology and aid with treatment planning.
Clinical features
Although usually slow growing, arteriovenous malformations may grow rapidly within a short period of time or following localized trauma. Symptoms may involve pain, hypertrophy of the perfused organ or tissue, or bleeding. They may present as a pulsatile mass with associated thrill, and bruit. An arteriovenous malformation involving the skin usually exhibits a reddish or blue discoloration. In two thirds of affected patients lesions present within the mandible. The lesion causes enlargement of the bone, mobility of surrounding teeth and associated gingival bleeding. Although rare, the practising dentist should be aware of these lesions as they may be located in close proximity to teeth and to the oral mucosa (Figure 5). Dental extractions or incisional biopsies carry a risk of significant haemorrhage. Dentists should be prepared to deal with this. In those patients who have known vascular malformations in close association with teeth, dentists need to be aware of the need to avoid extractions and should plan treatment accordingly. In the event of a torrential haemorrhage following an extraction, if possible the tooth should be re-implanted into the socket and pressure applied before the patient is urgently transferred to secondary care.
Figure 5. An arteriovenous malformation (AVM) extending along the right buccal sulcus.
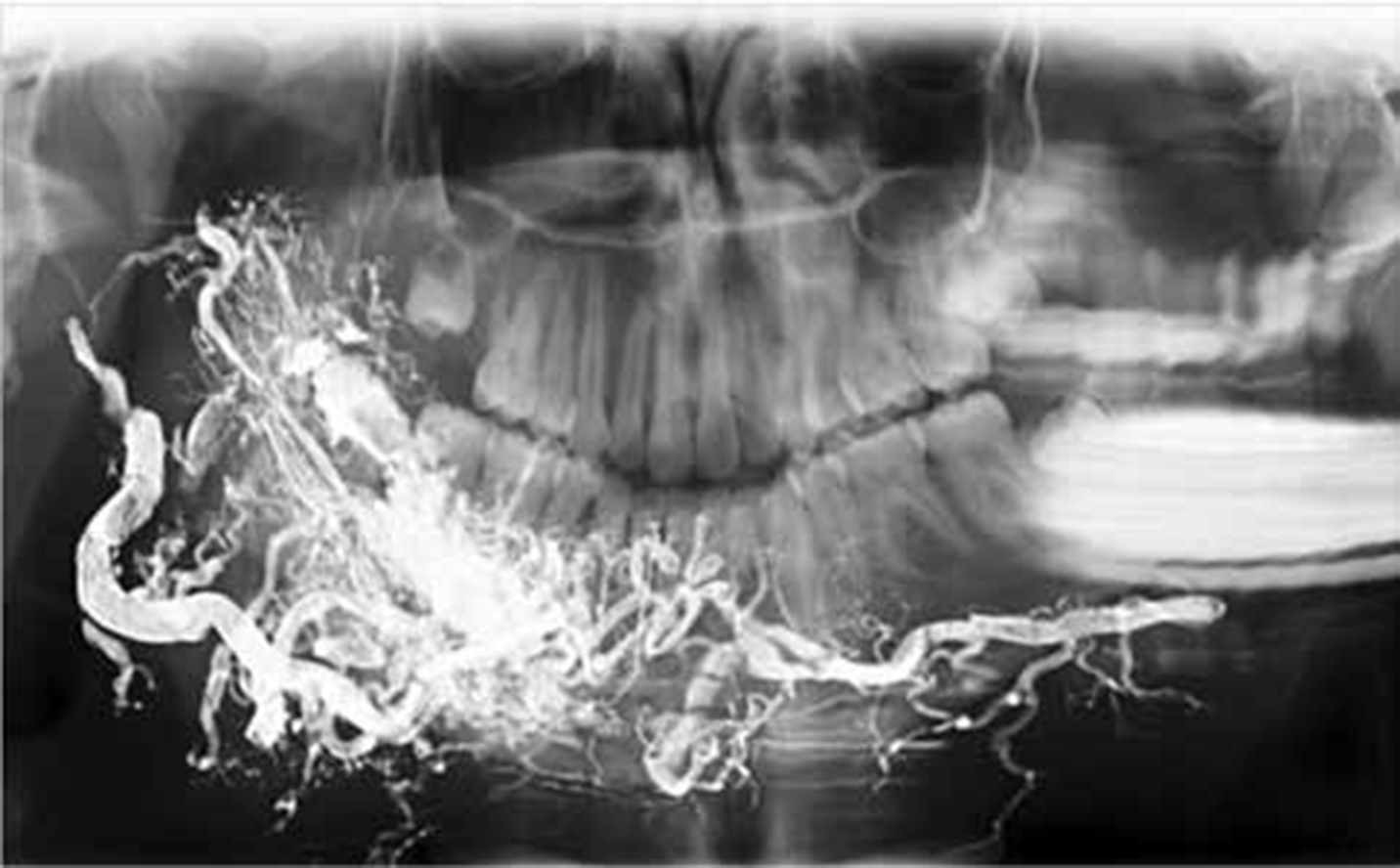
Ultrasound and MRI imaging can be used to assess the lesions further, with angiography being used to characterize the detailed morphology and function of the vascular channels. Once angiography has identified feeding vessels, embolization can be used to ablate or downgrade the lesion (Figure 6). Surgery is not usually the first line of treatment owing to the risks of haemorrhage and damage to adjacent structures, but is frequently required following embolization procedures.
Figure 6. An AVM after embolization with Onyx®.
Conclusion
It is important that dentists and doctors alike have diagnostic awareness and understanding of the various types of vascular anomalies, and the importance of differentiating between tumours and malformations. Early and accurate diagnosis is required for patient reassurance when appropriate and, in those requiring intervention, optimal management including choice of modality and its timing to achieve the desired outcomes. Where appropriate, it is essential that dentists refer cases for specialist treatment and maintain an alertness to the potential risks involved and complications that may ensue when providing dental treatment to these individuals (Table 1).
Condition
Referral to secondary care?
Safe for injections?
Safe for extractions?
Safe for scaling?
Infantile haemangiomas
Refer if patient has not already been seen by specialist
N/A
N/A
N/A
Congenital haemangiomas
Yes
✓
✓
✓
Pyogenic granulomas
Refer for assessment
✓
✓
✓
Capillary Malformations
If causing cosmetic problem / concern
✓
✓
✓
Venous Malformations
Consider referral if causing symptoms or if some ambiguity over exact nature of lesion
DO NOT INJECT INTO LESION
Safe if lesion is not in close association with tooth
Avoid scaling if near lesion
Lymphatic Malformations
Refer if lesions have not been previously assessed by specialist