Stewart DJ Dilacerate unerupted maxillary central incisors. Br Dent J. 1978; 145:229-233
Crescini A, Doldo T Dilaceration and angulation in upper incisors consequent to dental injuries in the primary dentition: orthodontic management. Prog Orthod. 2002; 3:29-41
Andreasen JO The influence of traumatic intrusion of primary teeth on their permanent successors. A radiographic and histological study in monkeys. Int J Oral Surg. 1976; 5:207-219
Andreasen JO, 2nd edn. St Louis: CV Mosby Co; 1972
McBride LJ Traction – a surgical/orthodontic procedure. Am J Orthod. 1979; 76:287-299
Hunt NP Direct traction applied to unerupted teeth using the acid-etch technique. Br J Orthod. 1977; 4:211-212
Chaushu S, Dykstein N, Ben-Bassat Y, Becker A Periodontal status of impacted maxillary incisors uncovered by two different surgical techniques. J Oral Maxillofac Surg. 2009; 67:120-124
Pearson MH, Robinson SN, Birnie DJ, Zaki GA Management of palatally impacted canines: the findings of a collaborative study. Eur J Orthod. 1997; 19:511-515
Parkin N, Benson PE, Thind B, Shah A Open versus closed surgical exposure of canine teeth that are displaced in the roof of the mouth (review). The Cochrane Library. 2008; 4
Kuchler EC, Tannure PN, Costa Mde C, Gleiser R Management of an unerupted dilacerated maxillary central incisor after trauma to the primary predecessor. J Dent Child. 2012; 79:30-33
Uematsu S, Uematsu T, Furusawa K, Deguchi T, Kurihara S Orthodontic treatment of an impacted dilacerated maxillary central incisor combined with surgical exposure and apicectomy. Angle Orthod. 2004; 74:132-136
Becker A, 3rd edn. Hoboken, New Jersey: Wiley-Blackwell; 2012
Chew MT, Ong MM Orthodontic-surgical management of an impacted dilacerated maxillary central incisor: a clinical case report. Pediatr Dent. 2004; 26
McDowall RJ, Yar R, Waring DT 2 ‘2’ 1: Orthodontic repositioning of lateral incisors into central incisors. Br Dent J. 2012; 212:417-423
Kokich VG, Spear FM Guidelines for managing the orthodontic-restorative patient. Semin Orthod. 1997; 3:3-20
Chaushu S, Becker A, Zalkind M Prosthetic considerations in the restoration of orthodontically treated maxillary lateral incisors to replace missing central incisors: a clnical report. J Prosthet Dent. 2001; 85:335-341
Newsome PR, Cooke MS Modifying upper lateral incisors to mimic central incisors: new ways to overcome old problems?. Rest Dent. 1987; 3:91-99
Schwaninger B, Shaye R Management of cases with upper incisors missing. Am J Orthod. 1977; 71:396-405
Stenvik A, Zachrisson BU Missing anterior teeth: orthodontic closure and transplantation as viable options to conventional replacements. Endod Topics. 2006; 14:41-50
Yau EC Tooth autotransplantation as a treatment option. The Hong Kong Medical Diary. 2009; 14:21-24
Slagsvold O, Bjercke B Autotransplantation of premolars with partly formed roots. A radiographic study of root growth. Am J Orthod. 1974; 66:355-366
Czochrowska EM, Stenvik A, Bjercke B, Zachrisson BU Outcome of tooth transplantation: survival and success rates 17–41 years posttreatment. Am J Orthod Dentofacial Orthop. 2002; 121:110-119
Kristerson L, Lagerström L Autotransplantation of teeth in cases with agenesis or traumatic loss of maxillary incisors. Eur J Orthod. 1991; 13:486-492
Kugelberg R, Tegsjö U, Malmgren O Autotransplantation of 45 teeth to the upper incisor region in adolescents. Swed Dent J. 1994; 18:165-172
Czochrowska EM, Stenvik A, Zachrisson BU The esthetic outcome of autotransplanted premolars replacing maxillary incisors. Dent Traumatol. 2002; 18:237-245
Cohen AS, Shen TC, Pogrel MA Transplanting teeth successfully: autografts and allografts that work. J Am Dent Assoc. 1995; 126:481-485
Pogrel MA Evaluation of over 400 autogenous tooth transplants. J Oral Maxillofac Surg. 1987; 45:205-211
Fowler PV Long term treatment planning for single tooth implants: an orthodontic perspective. Semin Orthod. 1997; 3:45-72
Kinzer GA, Kokich VO Managing congenitally missing lateral incisors. Part III: Single-tooth implants. J Esthet Restor Dent. 2005; 17:202-210
Creugers NH Resin-retained bridges in the treatment of traumatized dentition. Endod Dent Traumatol. 1993; 9:53-56
Durey KA, Nixon PJ, Robinson S, Chan MFW-Y Resin bonded bridges: techniques for success. Br Dent J. 2011; 211:113-118
Mayer TM, Hawley CE, Gunsolley JC, Feldman S The single-tooth implant; a viable alternative for single-tooth replacement. J Periodontol. 2002; 73:687-693
Jung RE, Pjetursson BE, Glauser R, Zembic A, Zwahlen M, Lang NP A systemic review of the 5-year survival and complication rates of implant supported single crowns. Clin Oral Implants Res. 2008; 19:119-130
Bernard JO, Schatz JP, Christou P, Belser U, Kiliaridis S Long-term vertical changes of the maxillary anterior teeth adjacent to single implants in young and mature adults. A restrospective study. J Clin Periodontol. 2004; 31:1024-1028
Jemt T, Ahlberg G, Henriksson K, Bondevik O Changes of anterior clinical crown height in patients provided with single implant restorations after more than 15 years of follow-up. Int J Prosthodont. 2006; 19:455-461
Zachrisson BU, Stenvik A Single implants – optimal therapy for missing lateral incisors? (Readers Forum). Am J Orthod Dentofacial Orthop. 2004; 126:13A-15A
Kokcih VG, Nappen DL, Shapiro PA Gingival contour and clinical crown length: their effect on the esthetic appearance of maxillary anterior teeth. Am J Orthod. 1984; 86:89-94
Kokich VG, Crabill KE Managing the patient with missing or malformed maxillary central incisors. Am J Orthod Dentofacial Orthop. 2006; 129:S55-S63
Sabri R Treatment of class I crowded malocclusion with an ankylosed maxillary central incisor. Am J Orthod Dentofacial Orthop. 2002; 122:557-565
Hellekant M, Twetman S, Carlsson L Treatment of a class II division 1 malocclusion with macrodontia of the maxillary central incisors. Am J Orthod Dentofacial Orthop. 2001; 119:654-659
Janson G, Valarelli DP, Valarelli FP, de Freitas MR, Pinzan A Atypical extraction of maxillary central incisors. Am J Orthod Dentofacial Orthop. 2010; 138:510-517
The management of the dilacerated impacted maxillary central incisor Naomi Prado Ovais Malik David Waring Dental Update 2024 43:7, 707-709.
Authors
NaomiPrado
BSc(Hons), BDS, MFDS RCPS(Glas)
DCT1 in Oral Surgery, Paediatrics and Orthodontics, University Dental Hospital of Manchester, Higher Cambridge Street, Manchester M15 6FH, UK (n_prado@live.co.uk)
The clinical problem of how best to manage a dilacerated, impacted maxillary central incisor will only be encountered rarely. The treatment aim should be to achieve results that are indistinguishable from normal appearance in a way that is appropriate for the patient. This article discusses the incidence of dilacerations in maxillary incisors and describes the treatment approaches available – orthodontic alignment or surgical removal and management of the resulting space, considering orthodontic repositioning, autotransplantation and various prosthetic replacements. Treatment indications, advantages and disadvantages, restorative and surgical implications, as well as the evidence-base relating to the various treatment modalities will be presented, along with clinical case examples.
CPD/Clinical Relevance: This paper discusses a problem that, if not managed appropriately, can lead to poor results for the patient. Even for practitioners who may not undertake the treatment mentioned, it will enable them to have more in-depth discussion with their patients should the situation arise.
Article
A dilacerated tooth is described when a crown or root form has been altered by way of an angulation or sharp curve.1 A dilacerated, unerupted maxillary central incisor may be associated with cysts, supernumerary teeth, developmental abnormalities, or trauma to the primary predecessor – the apices of which lie close to the permanent tooth germ. The incidence of each is shown in Table 1.2
Association
Incidence (%)
Cysts and supernumerary teeth
7
Trauma to primary predecessor
22
Developmental abnormalities
71
Dilacerations can occur in either the crown or the root of the developing permanent tooth. Crown dilacerations are the more uncommon presentation, occurring in only around 3% of cases3 and commonly associated with trauma to the primary dentition (especially intrusion injuries).
The severity of dilaceration caused by trauma will depend on a variety of factors. These include the stage of development of the permanent tooth when the trauma occurs, the direction and magnitude of the force of impact and the proximity of the apices of the primary predecessor to the permanent tooth germ.4
The literature suggests that 50% of teeth with crown dilacerations become impacted.5 The clinical management of the unerupted dilacerated tooth can be complicated, depending on the degree of dilaceration, and especially regarding space management.
Essentially there are two treatment approaches used to manage this:
Surgical exposure and orthodontic alignment;
Surgical removal of the dilacerated tooth and replacement via
- Orthodontic alignment of adjacent teeth;
- Autotransplantation;
- Prosthetic replacement.
Each of the two approaches has its own advantages and disadvantages, but the choice of which is the more appropriate solution is very much dependant on the specific characteristics of each case and the patients' wishes.
There is also an option of no treatment, accept the dilacerated tooth and monitor. However, this will prevent any other orthodontic treatment being performed and will also risk resorption of adjacent teeth, therefore it is not a recommended option.
Surgical exposure and orthodontic traction
In order to bring an unerupted maxillary incisor into a favourable position in the arch the tooth must be uncovered and orthodontically guided into position. This is done via one of the following surgical techniques:
Closed-eruption;
Open-eruption.
The closed-eruption technique involves raising a wide soft tissue flap followed by careful removal of bone overlying the most superficial surface of the impacted tooth.6,7 The opening of the crypt of the tooth may be minimal, only allowing space for a small eyelet attachment to be bonded during the surgical procedure. Keeping the surgical area small, and preserving optimum amounts of bone and soft tissue, will yield a more aesthetically pleasing result once the tooth has been brought into the line of the arch.7
Once the eyelet is bonded, a gold chain is attached and drawn into the oral cavity through the fully replaced flap.
The tooth is no longer in view and the gold chain is used for orthodontic traction to begin movement into the arch.8
An alternative to the closed technique is the open-eruption technique. This involves exposing the impacted tooth as above but removing more bone and soft tissue to create a ‘window’. The flap is then apically positioned to allow the tooth to remain visible9 and a surgical pack is placed to prevent the area closing over during healing.8
There are advantages and disadvantages to each technique and this has been documented in the literature. The closed-eruption is thought to increase the need for repeat surgery due to the fact that the flap is fully repositioned therefore, should there be failure of the bonded attachment, repeat surgery is usually required to replace it. This was discussed in a study by Pearson et al which compared 52 cases treated with the closed-eruption technique with 52 cases treated with the open-eruption technique.10 They found that 31% of those treated using closed-eruption required repeat surgery; whereas only 15% of cases treated using open-eruption required a second operative procedure.
The open-eruption technique has previously been less favoured as the removal of more bone and soft tissue is associated with poorer periodontal prognosis of the impacted tooth.11 Despite the many documented disadvantages and advantages of each technique, a Cochrane review in 2008 concluded that there is currently not enough evidence to support one surgical technique over the other with regards to dental health, aesthetics, economics and patient factors.11
Success vs failure
It has been widely reported that the success of the above techniques in treating a dilacerated, unerupted maxillary incisor depends on a number of factors. These include:
A tooth with an obtuse angle dilaceration, with incomplete root formation, a lower position and sufficient space in the arch will give a better prognosis for orthodontic traction.12
Both of the surgical techniques discussed above are not without their risks of failure. Failure could occur following traction of the dilacerated tooth due to:
Ankylosis;
External inflammatory root resorption;
Root exposure through the labial cortical plate.13
All of these possibilities must be discussed in-depth with the patient as part of the consent process before treatment is undertaken.
Is it worth it?
Although orthodontic alignment of dilacerated maxillary central incisors may be successful, the long-term prognosis for the tooth may be poor and extraction and prosthetic replacement could well be part of the long-term treatment plan.14 With this being said, the question is often asked whether there is justification for carrying out orthodontic alignment in the first place?
Every clinical case is different and therefore should be measured on its own merits. However, it is important to take into account the following points when treatment planning:14
The decision to extract the dilacerated tooth at an early stage will lead to resorption of the alveolar ridge. This will result in a deficiency both vertically and labio-lingually which could impact implant placement in the future.
An implant-based prosthesis could not be considered until early adulthood when full facial growth has occurred. This will be many years from when the tooth was reported as unerupted and so missing from the arch.
A tissue-borne form of replacement, for example a partial acrylic denture, will likely be less acceptable to the patient. Long-term wear also poses the risk to the health of the palatal and gingival soft tissues in contact and will also create a significant plaque trap with the possibility of caries initiation.
A tooth-supported structure (eg resin-bonded bridge) may be an option for restoring the space whilst waiting for sufficient growth for implant placement. However, this is unreliable in the long-term and may require invasive preparation of an adjacent tooth. The restoration would also need long-term maintenance and so requires a lifetime commitment from the patient.
On reflection of the points above, orthodontic repositioning of the dilacerated tooth, even with poor prognosis, will serve to preserve the architecture of the alveolar ridge. This will ensure that, in the long-term treatment plan, there are more restorative options available to help yield an acceptable result.14
Surgical removal of the dilacerated tooth
In some cases, orthodontic repositioning of the unerupted dilacerated maxillary central incisor is not possible. In these situations the most favourable treatment plan may be surgical removal of the tooth followed by methods either to close the space orthodontically, autotransplantation with a developing tooth, or maintenance of the space until the patient comes of suitable age for prosthetic replacement.15
Orthodontic space closure
Using orthodontic space closure to manage a missing maxillary central incisor will result in the lateral incisor taking the place of the central incisor (including both the aesthetic and functional roles). The canine will subsequently assume the role of the lateral incisor and the first premolar that of the canine.16
Once orthodontically repositioned the affected teeth will need to be restoratively modified and camouflaged in order to suit their new identity both aesthetically and functionally.
This type of management will involve a multidisciplinary approach with the input of the restorative dentist and/or paediatric dentist.17 Orthodontic considerations will include:
Tooth positioning in the vertical, mesio-distal and labio-palatal planes;
On the other hand, restorative considerations will include:
The timing of restoration;
Type of restoration;
The shape, size and colour of the canine tooth;
The resulting functional occlusion;
The gingival margins and periodontal health.18,19,20
As with any procedure, there are advantages and disadvantages to orthodontic repositioning, which must be discussed fully with the patient before beginning treatment. The main advantage in this case is the biocompatibility and permanence of the treatment. Repositioning of the lateral incisor into the central incisor space allows maintenance of the alveolar bone height and soft tissue profile during growth of the dentofacial complex.21 It also eliminates the need for temporary and permanent prosthetic tooth replacements prior to implant consideration, along with their associated maintenance.16
The disadvantages associated with this treatment approach include: the need for close multidisciplinary care, increased complexity of treatment, overall aesthetics, increased functional load on the lateral incisor root and a risk of relapse involving anterior space re-opening.16
Autotransplantation
Tooth autotransplantation refers to a process that involves the extraction of a tooth from one location and its re-implantation into a different location in the same patient. The new location may be an artificially drilled space in an edentulous ridge or the fresh socket of a recently extracted tooth22 (as would be the case for removal of an impacted dilacerated maxillary central incisor).
The current method of autotransplantation was proposed around 40 years ago by Slagsvold and Bjercke and involved the transplantation of teeth with incompletely developed roots into the space of a missing or recently extracted tooth.23 Following transplantation, the growth of the donor tooth root continues, endodontic treatment is not usually needed and so the tooth retains its functional ability.24 The donor tooth can then be restoratively modified to replicate the tooth it is replacing aesthetically.
The most favourable donor graft is the premolar tooth, as the root development is one of the latest in the arch, the root morphology is straight and conical and the extraction space may be utilized to relieve crowding.21
With this type of management, careful treatment planning is paramount and must take into account the following:21
Donor tooth with up to ¾ root length;
Creation of sufficient space at recipient site;
Careful surgery to avoid damage to root surface of donor tooth;
Management of residual space at donor site;
Orthodontic adjustment of the transplanted tooth to allow optimal aesthetic result following restoration.
Although one of the more complex treatment modalities, autotransplantation of premolars to replace incisors has been shown in systematic reviews to have long term (>25 years) survival rates of over 90%, with generally satisfactory aesthetic results.25,26,27 As with orthodontic space closure, one of the biggest advantages to autotransplantation as a treatment option for missing maxillary incisors is the biocompatibility and permanence of treatment once completed, particularly in growing individuals. Treatment via autotransplantation requires extensive multidisciplinary care involving the teams in orthodontics, oral surgery and restorative dentistry, as well as exceptional compliance from the patient to ensure the success of the procedure. One of the most obvious disadvantages to using this technique is the risk of failure. If the periodontal ligament of the transplanted tooth is traumatized during the procedure, then external inflammatory root resorption and ankylosis is often noted.28,29 The surgical procedure involved is technique sensitive and success relies on the preservation of the apical Hertwig's epithelial sheath of the donor tooth to ensure pulpal regeneration and root maturation once transplanted.22
Surgical removal and space maintenance/prosthetic replacement
In cases where orthodontic repositioning is contra-indicated and tooth autotransplantation not possible, the remaining treatment option may be surgical removal of the dilacerated tooth and space maintenance until the patient is suitable for prosthetic replacement.
A tissue-borne form of replacement, such as a removable partial denture or an orthodontic retainer, is generally not well tolerated by young patients and may pose a risk to the health of the palatal and gingival soft tissues.14 For this reason, it is not usually the treatment option of choice in cases where it may be many years until definitive treatment is provided to fill the space (ie in young children awaiting completion of growth for implant provision), however, it may be an option for cases in which only short-term space maintenance is required.31
In the patient whose remaining anterior adult teeth have fully erupted and are favourable as abutments, resin-bonded bridges may be a suitable space maintainer.32 As bridges are not tissue-borne and are fixed, they eliminate complications such as compliance and risk of prolonged damage to the soft tissues. Resin-bonded bridges should also be considered as a good prosthetic replacement option for patients who are not suitable for implant placement due to the contra-indication of surgical procedures (eg if medically compromised or severely dental phobic).
Although there are many good indications to using resin-bonded bridges as space maintainers or final prosthetic replacements, it must be remembered that this kind of restoration may require preparation of an adjacent, healthy tooth for retention.14 Even with minimal/no preparation, the abutment tooth will consequently have a poorer long-term prognosis33 and the likelihood of need for further restorations in the future is higher. Bridges will also not maintain alveolar bone height and so may have implications if implant placement is to be considered in the future.
Recently, the single-crown implant has become one of the most common treatment modalities for the replacement of missing teeth.34 As well as having continued evidence of high success rates (94.5% success rate over 5 years35), another advantage of implants as a prosthetic replacement is the fact that the surrounding teeth do not require preparation. This is of particular benefit in young patients, many of whom have unrestored dentitions31 and larger pulp horns vulnerable to any tooth preparation. However, as previously mentioned, implants cannot be placed until facial growth is complete and so careful treatment planning with multidisciplinary teams is paramount to ensure future success.
Cases
Case 1: Surgical exposure and orthodontic alignment
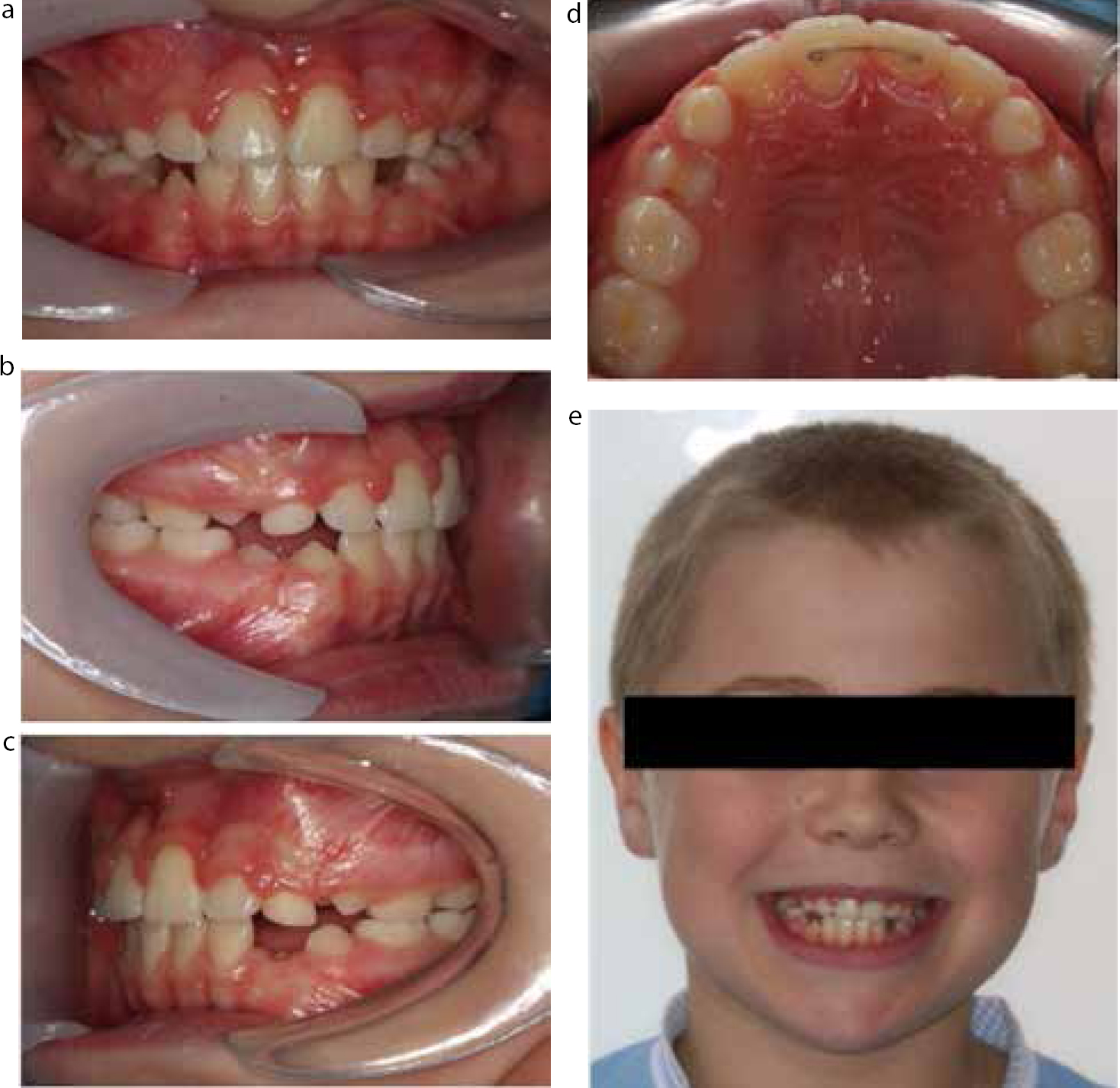
A 10-year-old boy presented with a missing upper central incisor. There was no relevant medical or dental history or history of trauma to the dentition. The upper right central incisor had erupted uneventfully at age 7 years and the patient's parent had become concerned about the missing upper left incisor (UL1).
On examination, the patient had a Class I incisor relationship (Figure 1) on skeletal 1 bases with average vertical proportions.
Figure 1. Case 1: Extra-oral view showing the young patient presenting with a missing UL1.
An OPG radiograph revealed the presence of the unerupted and dilacerated upper left central incisor. The tooth was in a reasonable position vertically for alignment. The patient was referred to the oral surgery department for exposure and placement of a gold chain (Figure 2 a–d). The post-op OPG radiograph shows the UL1 in a reasonable position for alignment and highlights the gold chain in position (Figure 3).
Figure 2. Case 1: (a–d) Intra-oral views showing a space in the anterior maxilla caused by the impaction of dilacerated UL1: the surgical procedure has been undertaken and the gold chain attached to UL1 can be seen bonded to UR1, ready to allow for orthodontic traction.Figure 3. Case 1: Post-operative OPG radiograph showing UL1 in a reasonable position for alignment and highlighting the gold chain attachment.
A sectional fixed appliance was placed (Figure 4) and the treatment progressed well with the UL1 being aligned into the correct position. The patient and parents were happy with the outcome and on subsequent reviews the UL1 maintained this good position (held by a fixed retainer) (Figure 5 a–e).
Figure 4. Case 1: Intra-oral view showing the dilacerated UL1 being orthodontically moved into position using a sectional upper fixed appliance.Figure 5. Case 1: (a–e) Intra-oral views showing the final position of UL1 following orthodontic movement: the patient's oral hygiene was not optimum, leading to gingival inflammation. This was addressed with extensive oral hygiene instruction.
Case 2: Surgical removal and prosthetic replacement
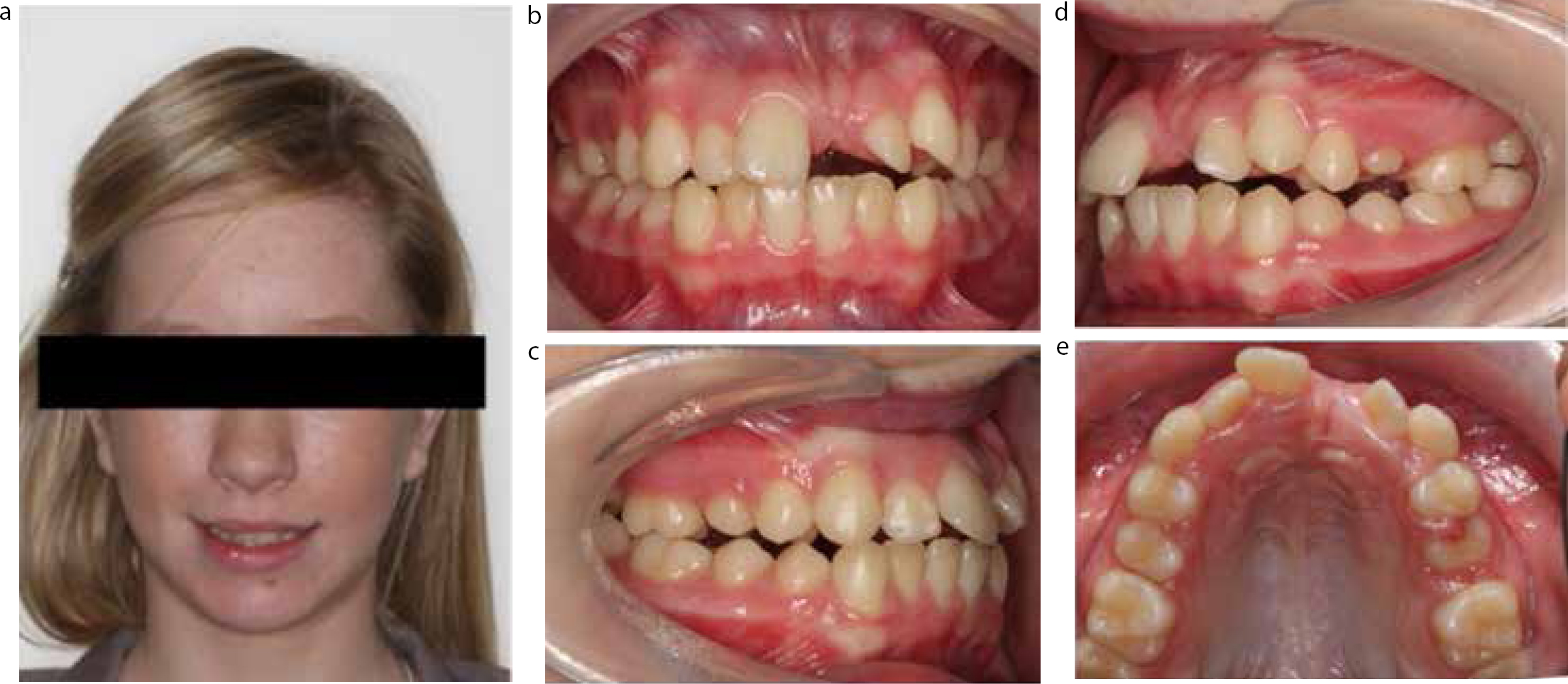
A 13-year-old girl was referred to the orthodontic department regarding the unerupted upper left central incisor (UL1). The primary incisor had been retained for several years but eventually exfoliated leaving an unsightly gap that the patient was very self-conscious about.
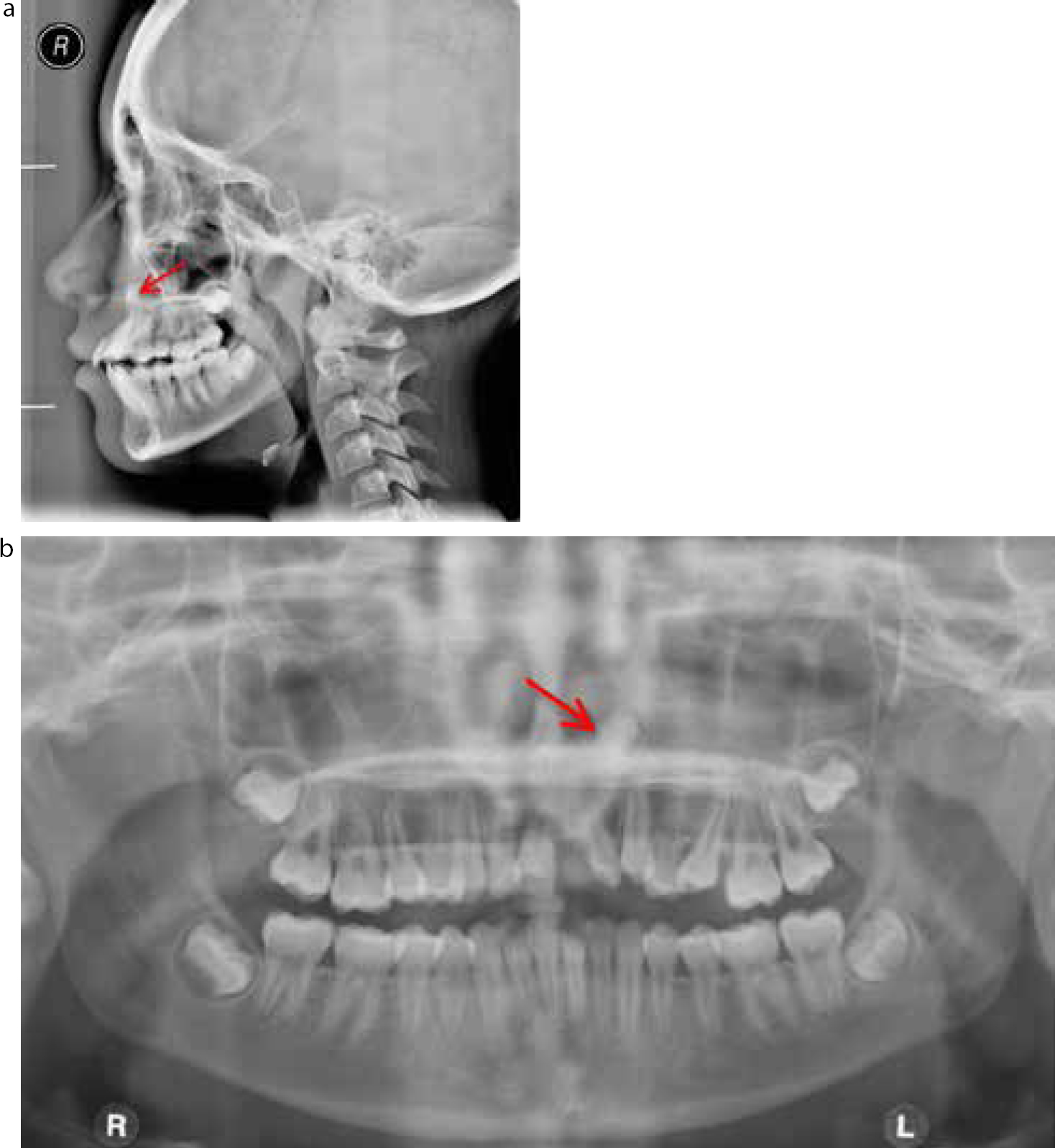
Clinical and radiographic examination reveals a Class I malocclusion with Class I molar relationship bilaterally (Figure 6 a–e). There was spacing in the UL1 region with displaced UL2 and UL3. The OPG and lateral cephalogram radiograph (Figure 7a, b) indicate a dilacerated incisor in a very high position. The tooth was not deemed suitable to attempt alignment and a treatment plan was discussed to create the correct space in the UL1 region for prosthetic replacement. The patient was seen on the joint orthodontic-restorative clinic where a discussion was undertaken regarding eventual replacement. Although space would be created to facilitate an implant, the patient was happy with a resin-bonded bridge as a first line of treatment. Should this be unsuccessful long term, an implant may be considered. The orthodontic treatment plan required extraction of upper 1st premolars (UR4, UL4) and lower 2nd pre-molars (LR5, LL5).
Figure 6. Case 2: (a–e) Pre-operative views showing a 13-year-old female patient with spacing in the UL1 region. UL2 and UL3 have also been displaced.Figure 7. Case 2: (a, b) OPG and lateral ceph radiographs showing dilacerated UL1 (red arrow) in an unfavourable, high position, unsuitable for orthodontic alignment.
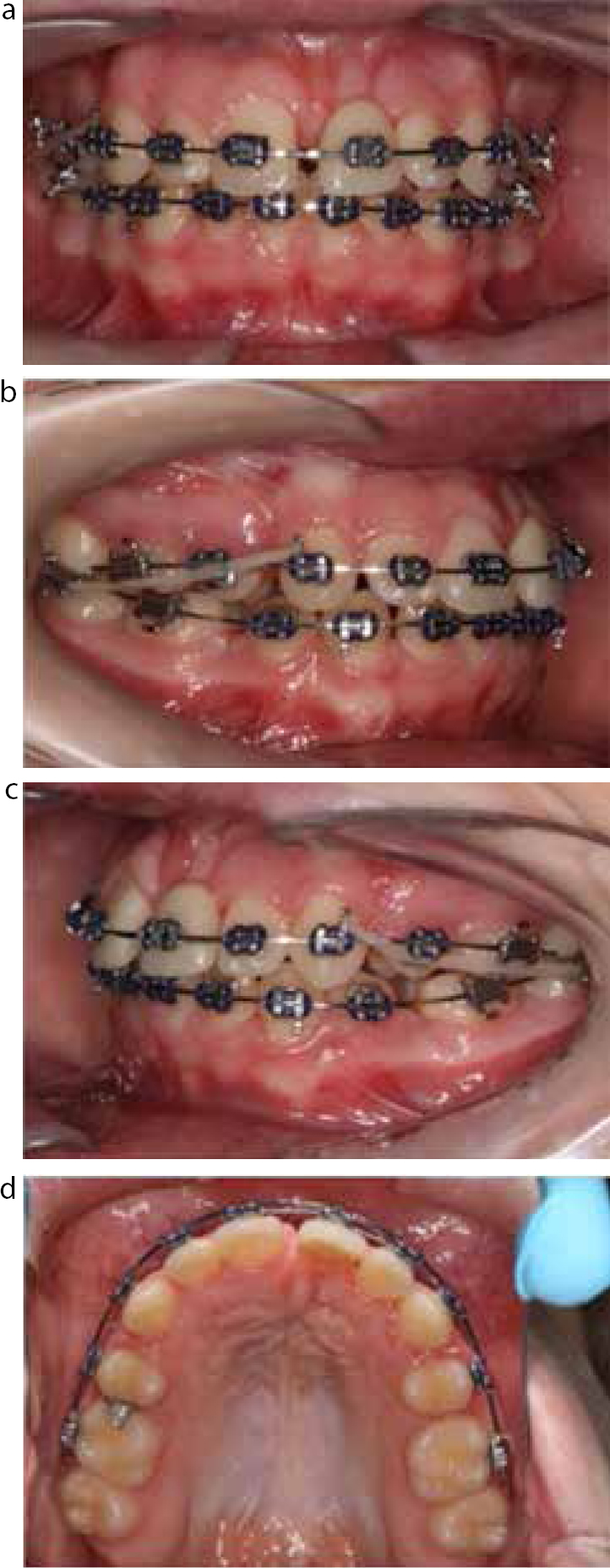
A fixed appliance system was fitted in the upper and lower arches and a pontic was ligated to the wire (Figure 8 a–d), providing a number of benefits for both patient and clinician:
Improved appearance;
Assessment of space requirement;
Allowing orthodontic space closure to correct dimension;
Assessing shape and colour of tooth in ‘real life’ situation;
Improved function – speech and mastication.
Figure 8. Case 2: (a–d) Intra-oral views showing a fixed appliance system fitted in the upper and lower arches. A pontic was ligated to the wire in the position of UL1 to aid with aesthetics and space maintenance.
A peri-apical radiograph (Figure 9) was taken to assess the root position of the UR1 and UL2 to ensure adequate apical space was created should an implant be required in the future. It is important to ensure that patients are aware that an implant may not be a viable option if correct space is not created and this may increase the duration of the orthodontic treatment time. Treatment duration was 20 months before debond and placement of a Hawley type retainer with a pontic to replace UL1. The retainer was worn for 6 months to allow the tissues to settle before placement of a resin-bonded bridge. The patient was very happy with the outcome (Figure 10 a–e).
Figure 9. Case 2: Peri-apical view showing the space between UR1 and UL2. This was taken to assess the root position of the UR1 and UL2 to ensure adequate apical space was created should an implant be required in the future.Figure 10. Case 2: (a–e) Intra-oral and extra-oral views showing the final result following debond. A Maryland bridge was used to replace UL1.
Discussion
This article describes the management of the impacted dilacerated maxillary central incisor. The goal for these patients should be to achieve a treatment result that is indistinguishable from normal appearance.
Traditional management for this condition includes removal of the affected tooth and replacement with partial dentures, resin-bonded bridges or implants. Although orthodontic alignment, orthodontic space closure and autotransplantation may be considered more complex treatments, they constitute relevant alternatives that the clinician must bear in mind.
Where orthodontic alignment is not possible and the affected dilacerated tooth is removed, the challenge in treating patients is how to achieve a result that is aesthetic and functional, especially in the long term.
Although there is favourable data for the survival of single-crown implants, long term there may be aesthetic problems such as:36,37,38
Infraocclusion;
Shrinkage of the gingival margins and root exposure;
Resorption of the buccal bone and the subsequent darkened appearance of overlying gingiva.
Alongside this there is the complication that implants cannot be placed until facial growth is complete, meaning that the patient will need to wear an alternative prosthetic replacement in the interim.
The most evident advantage of using orthodontic space closure or autotransplantation to replace the missing incisor is the biocompatibility and permanence of the treatment result. Following treatment, normal gingival tissues and papillae will surround each tooth,21 therefore giving a better soft tissue aesthetic that is not achievable with prosthetic tooth replacement.
However, orthodontic space closure and substitution of central incisors by lateral incisors is sometimes questioned.39 There are concerns that the treatment result may not look ‘natural’, especially in patients where there is a unilateral missing tooth, as is usually the case with an impacted, dilacerated maxillary central incisor. In response to this, many papers have documented that a desirable result can be achieved, as long as the appropriate clinical indications are met and there is meticulous attention to detail throughout the treatment.18,40,41,42,43
It is important to use evidence-based clinical practice whenever possible. Unfortunately, there is currently a lack of research, with regards to the management of missing maxillary central incisors, comparing the aesthetic and functional results of the various treatment approaches. This may be due to difficulty in collecting sufficient sample size data for follow-up and analysis and is further complicated by the fact that optimum treatment results may require integrated interdisciplinary teamwork.21 If this research is done in the future, it will provide us with a better understanding of the long-term outcomes of each treatment modality and enable us to make more informed clinical decisions.
Conclusion
The clinical problem of a dilacerated, impacted maxillary central incisor tooth may not be encountered frequently, but when it does it may pose treatment-planning complications for the clinician if not assessed appropriately. The treatment approaches of orthodontic alignment, or surgical removal and space closure (using either orthodontics, autotransplantation or prosthetic replacement) are varied and each has its own advantages and disadvantages. Functional and aesthetically satisfactory results are achievable as long as specific indications for treatments are assessed, attention to detail is exercised throughout and appropriate interdisciplinary support is available.