The clinical presentations of oral malignancy are diverse. This short article discusses a case of a late-presenting oral malignancy and signifies the importance of general dental and medical practitioners' knowledge in the diagnosis of oral malignancy.
CPD/Clinical Relevance: Oral malignancy is a life-threatening diagnosis. The importance of a structured systematic approach in the diagnosis is discussed.
Article
Case report
A 65-year-old male presented to the emergency department with pain on the left-hand side of his mandible after feeling a ‘crack’ whilst eating cornflakes. The patient was a retired builder living with his wife and had an unremarkable medical history with the exception of spinal stenosis. He was a non-smoker and consumed a minimal alcoholic intake. On presentation, he was examined by an A&E doctor who requested an orthopantomogram (Figure 1) which was reported by a non-dental radiologist. No fracture or change in bone density was noted and an appointment with the maxillofacial department was organized without prior request for maxillofacial review.
Figure 1. Orthopantomogram taken at A&E.
At the maxillofacial review, the patient complained of a dull pain in the left side of his mandible which was much worse when chewing food. He denied otalgia or dysphagia and was managing to eat a good diet. On inspection, there was an extra-oral swelling involving the left body of mandible and intra-oral examination revealed an irregular, ulcerated, exophytic, granular lesion of the mandibular alveolus in the left premolar region and extending laterally to the buccal sulcus. There was associated grade II mobility of the LL7 and LL8, and neither the lingual nerve nor the inferior alveolar nerve had altered sensation at this point. The orthopantomogram was reviewed and reported by a dental clinician who commented on the area of radiolucency within the left body of the mandible and associated undisplaced pathological fracture. Additional imaging was ordered. At the next appointment, the patient's history had evolved to symptoms of numbness of the lower lip and the spontaneous exfoliation of a molar on the left side of the mandible. On examination, this evolution in clinical symptoms was accompanied by a dramatic increase in bony expansion of the left body of the mandible.
Examination under general anaesthesia revealed a mass extending from the LR2,3 to the retromolar area of the left mandible with associated grade III mobile teeth. The mass was invading the buccal tissues and clinically represented a stage IV tumour. An incisional biopsy was taken which confirmed the diagnosis of a well to moderately differentiated squamous cell carcinoma of the left mandible negative for p16.
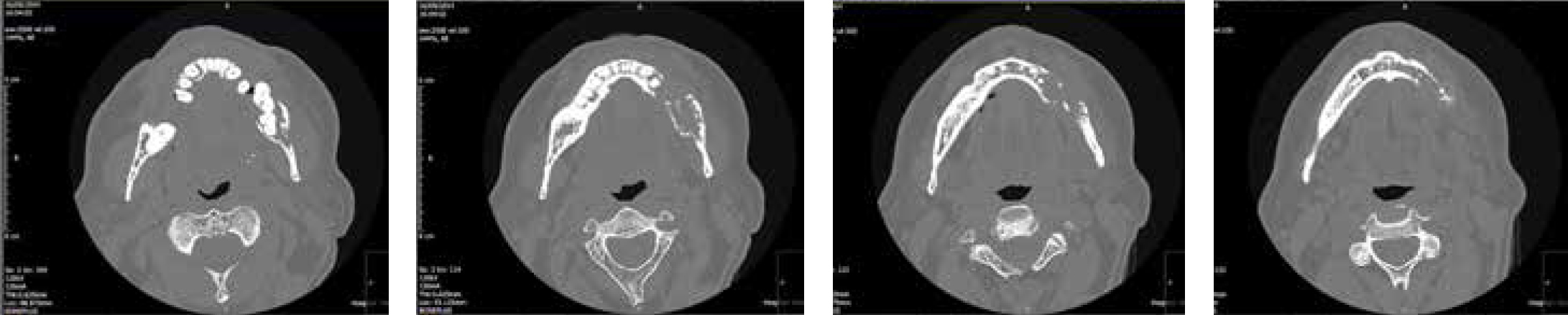
Computed tomography (Figure 2) of the facial bones prior to biopsy reported: ‘a large destructive lesion in the left side of the mandible associated with a soft tissue mass. As a result, several teeth are ‘floating’. There is lymphadenopathy at levels I and II on the left side of the neck…in keeping with primary or secondary malignancy.'
Figure 2. Computed tomography sections.
A magnetic resonance imaging scan of the neck with contrast reported: ‘an extensive tumour involving the left hemi-mandible, with probable invasion of the muscles of mastication, and ipsilateral lymphadenopathy. Radiological TNM stage tumour (T) 4b, nodes (N) 2b and metastasis (M) 0.'
The patient underwent a left hemi-mandibulectomy and reconstruction with a pectoralis major flap and reconstruction plate along with adjunctive radiotherapy. He is currently under the care of the multidisplinary team.
Discussion
Recent literature highlights a consistently increasing trend in the incidence of oral malignancy since the mid-seventies; this increase was 32% and 33% in male and female, respectively, between 2000–2002 and 2009–2011 within Europe.1 Oral cancer is now the ninth most common malignancy in men within the UK2 and it is vital that both general dental and medical practitioners are aware of the red flags of oral malignancy.
This case report demonstrates the importance of a good clinical history, clinical examination and judicious use of radiology in the diagnosis of oral malignancy. It also highlights the important role of general dental practitioners and the importance of an awareness of oral malignancy. The fact that the patient's mandible fractured whilst eating cornflakes exemplifies the extent of the lesion and minimal force needed to fracture the weakened bone. Several papers describe the key symptoms and high-risk factors within the history3,4,5 (Table 1) and clinical signs3,6,7,8,9,10,11 of oral malignancy (Table 2), however, the red flag warning of unexplained mobility of teeth which often precedes a pathological fracture, a sign of oral malignancy, is not often emphasized.
Presenting symptoms
SIZE:
Increasing size often in the absence of trauma or other exacerbating factors
CHRONOLOGY:
Rapid onset of symptoms
Lesion persistent >3 weeks
Persistent ulceration
Non-healing extraction socket
ASSOCIATED WITH:
Lack of pain
Otalgia
Dysphagia
Odynophagia
Numbness/paraesthesia
Swelling
Voice change (hoarseness)
Weight loss
Chronic trauma
Social history
Tobacco/betel quid consumption
Excessive alcohol consumption
UV light exposure
Medical history
Immunocompromised (pathological or iatrogenic)
Human papilloma virus (HPV) infection
Dietary factors - deficiencies of vitamin A, E or C
Site
Floor of mouth
Lateral sides of tongue
Retromolar pad
Lower lip
Colour
Red patch (erythroplakia)
White patch (leukoplakia)
Mixed red and white patch (erythroleukoplakia/speckled leukoplakia)
Ulceration
Granular appearance
Indurated
Rolled margins
Hard tissue
Swelling
Bony expansion
Loose adjacent teeth
Lymph nodes
Cervical node enlargement (>1 cm)
Firm
Fixed
Non-tender
Premalignant lesions
Leukoplakia
Erythroplakia
Lichen planus
Submucous fibrosis
Discoid lupus erythematosus
Dyskeratosis
Epidermolysis bullosa
This case highlights the importance of good documentation in the requesting of appropriate special investigations in any case of oral malignancy. The correct selection of radiological investigation is essential, as demonstrated here, because the limited view of a peri-apical radiograph would not suffice to rule out periodontal disease as the cause of any tooth mobility and show the full extent of any pathology or potential fractures. In addition, The Ionizing Radiation (Medical Exposure) Regulations 2000 state: ‘doses arising from the exposure should be kept as low as reasonably practicable consistent with the intended purpose',12 therefore the exposure of orthopantomograms can be justified in confidence. Furthermore, an orthopantomogram would also reveal any secondary head and neck metastases which would include malignancy of the lung, prostate, thyroid, kidney and breast, most commonly presenting as a unilocular lesion within the ramus of the mandible.
The chance of correctly identifying oral malignancy is increased when a systematic and thorough diagnostic approach is applied at initial presentation. At an assessment by a general dental or medical practitioner, the history of symptoms, in particular the noting of key red flags coupled with a systematic clinical examination of neck, extra-oral tissues and the whole oral cavity are essential and aid in the justification of appropriate adjunctive special investigations. The inspection of radiographs is assisted by the detailing of clinical findings at request. Inspection of radiographs should also be systematic and knowledge of key red flag features can assist with this process13 (Table 3). In this case, the systematic sequence described above was incomplete and resulted in a late referral to the hospital. Inadequate history-taking and examination resulted in insufficient information being given to the reporting radiologist and an incorrect report. Referral to the specialist maxillofacial team was consequently not expedited and diagnosis was delayed, yet this case highlighted many of the key red flag signs and symptoms that should precipitate a two-week wait referral.
Key radiological characteristics
Patient's orthopantomogram
Site/anatomical position
Posterior body/angle/ramus of mandibleMaxilla if originating in the antrum
Yes ✓
Size
Variable - rapid growth is a feature but size depends at what stage radiograph taken
Yes ✓
Shape
Irregular shape of bone destruction
Yes ✓
Outline/periphery
Irregular and moth-eaten Poorly defined and not corticated
Yes ✓
Relative radiodensity
RadiolucentRadiodensity depends on degree of destruction
Yes ✓
Effects on adjacent structures
Loss of lamina duraAdjacent teeth displaced, loosened and/or resorbed or left ‘floating in space’Destruction of surrounding bone may lead to pathological fracture
Yes ✓
Conclusion
This case report highlights several key steps to prevent missing a diagnosis of oral malignancy. A structured systematic approach is essential in the diagnosis of oral malignancy and the case presented emphasizes the importance of good documentation and the selection of appropriate special investigations. In addition, the significant value of a general dental practitioner in the diagnosis of oral malignancy is highlighted. In many parts of the UK patient attendance with dental practitioners is, sadly, often at best sporadic for many of the more at-risk members of the population, and the knowledge base and systematic approach highlighted in this article is also essential for the general medical practitioner. For this reason, we recognize the responsibility of maxillofacial departments to provide regular educational updates to local general medical and dental practitioners in their local community to help in the prevention of any delays in the referral of patients with oral malignancy.