World Health Organization. 2011. (Accessed on 27 May 2015)
2013. (Accessed on 27 May 2015)
Office for National Statistics. 2012. (Accessed on 27 May 2015)
2014.
2008. (Accessed 27 May 2015)
Mulsant BH, Pollock BG, Kirshner M, Shen C, Dodge H, Ganguli M Serum anticholinergic activity in a community-based sample of older adults: relationship with cognitive performance. Arch Gen Psychiatry. 2003; 60:198-203
Nabi G, Cody JD, Ellis G, Hay-Smith J, Herbison GP Anticholinergic drugs versus placebo for overactive bladder syndrome in adults. Cochrane Database Syst Rev. 2006; 4
Bostock CV, Soiza RL, Mangoni AA Association between prescribing of antimuscarinic drugs and antimuscarinic adverse effects in older people. Expert Rev Clin Pharmacol. 2010; 3:(4)441-452
Rudolph JL, Salow MJ, Angelini MC, McGlinchey RE The Anticholinergic Risk Scale and anticholinergic adverse effects in older persons. Arch Intern Med. 2008; 168:(5)508-513
Casarosa P, Keichle T, Sieger P, Pieper M, Ganter F The constitutive activity of the human muscarinic M3 receptor unmasks differences in the pharmacology of anticholinergics. J Pharmacol Exp Ther. 2010; 333:201-209
Lowry E, Woodman RJ, Soiza RL, Mangoni AA Associations between the Anticholinergic Risk Scale score and physical function: potential implications for adverse outcomes in older hospitalized patients. J Am Med Dir Assoc. 2011; 12:(8)565-572
Many common prescription and over-the-counter medications have antimuscarinic effects. Antimuscarinics are a well recognized cause of dry mouth, with potential to cause other physical and cognitive adverse effects. A comprehensive medication review in a patient presenting with dry mouth can lead to overall health improvements. Scoring systems can be helpful in identifying antimuscarinic drugs and their adverse effects.
CPD/Clinical Relevance: Antimuscarinic drug use is prevalent and a common cause of dry mouth. Older people are particularly susceptible to antimuscarinic adverse effects.
Article
The number of older people worldwide is increasing. By 2050, 16% of the global population will be over 65.1 Approximately one-fifth of people in the United Kingdom are now aged 65 or older.2,3 Most people over 65 live with a long-term medical condition and most people over 75 live with two or more long-term medical conditions.4 Older people are more likely to take multiple medications. Around 20% of people over 70 take at least five medications, and 16% take 10 or more medications.4
Antimuscarinics are commonly prescribed drugs with significant oral effects. This is illustrated in the following case study and review. Following recognition of a drug-related oral problem, it is advisable to ask patients to attend their general medical practitioner for a medication review. A medication review is a ‘structured, critical examination of a patient’s medicines with the objective of reaching an agreement with the patient about treatment, optimizing the impact of medicines, minimizing the number of medication-related problems, and reducing waste'.5 Key points for general dental practitioners can be summarized as follows:
Anticholinergic (antimuscarinic) drugs are a well-recognized and common cause of dry mouth;
About half of the older population use at least one antimuscarinic medication. Around 30% of these people report a dry mouth. They may also experience other physical or cognitive adverse effects;
Many common prescription and over-the-counter medications have antimuscarinic effects, including many drugs that are not classically considered to be antimuscarinics;
Consulting a drug formulary or antimuscarinic scoring system, or liaison with a community pharmacist or general medical practitioner, can help identify antimuscarinic medications contributing to dry mouth;
Medication review in a patient presenting with dry mouth can lead to overall health improvements.
Case study part 1
A 75-year-old gentleman presented to his general dental practitioner with symptoms of dry mouth. His mouth felt uncomfortable and his dentures felt loose (Figure 1). Past medical history included ischaemic heart disease, post-herpetic neuralgia and gastro-oesophageal reflux disease. Further questioning revealed that he recently started taking oxybutynin for bladder urgency. His wife reported that he had been muddled and constipated.
Figure 1. Patient with dry mouth and unable to wear his dentures.
On examination, he was found to have a dry mouth with some areas of atrophic mucous membranes (Figure 2). His full upper denture fitted quite well but was poorly retained in position due to lack of saliva film. His lower denture fitted less well due to more advanced ridge resorption.
Figure 2. View of lower jaw demonstrating some dryness of the mucosa.
Why are antimuscarinic medications important to dental practitioners?
Anticholinergic (antimuscarinic) drugs are a well recognized and common cause of dry mouth. It has been estimated that around 50% of the general elderly population use at least one antimuscarinic medication.6 Around 30% of these people report experiencing dry mouth.7 If a patient with dry mouth presents to a dental practitioner there is an opportunity to communicate with his/her general medical practitioner and trigger a medication review. Greater awareness of antimuscarinic medications, uses and adverse effects can prompt intervention with positive health benefits.
What are antimuscarinic drugs and what are the therapeutic indications?
Antimuscarinic drugs are antagonists of the muscarinic acetylcholine receptor (mAChR). mAChRs are G-protein coupled receptors located in the central nervous system (hippocampus, cortex, thalamus) and peripherally (mainly autonomic effector cells of the parasympathetic nervous system).8
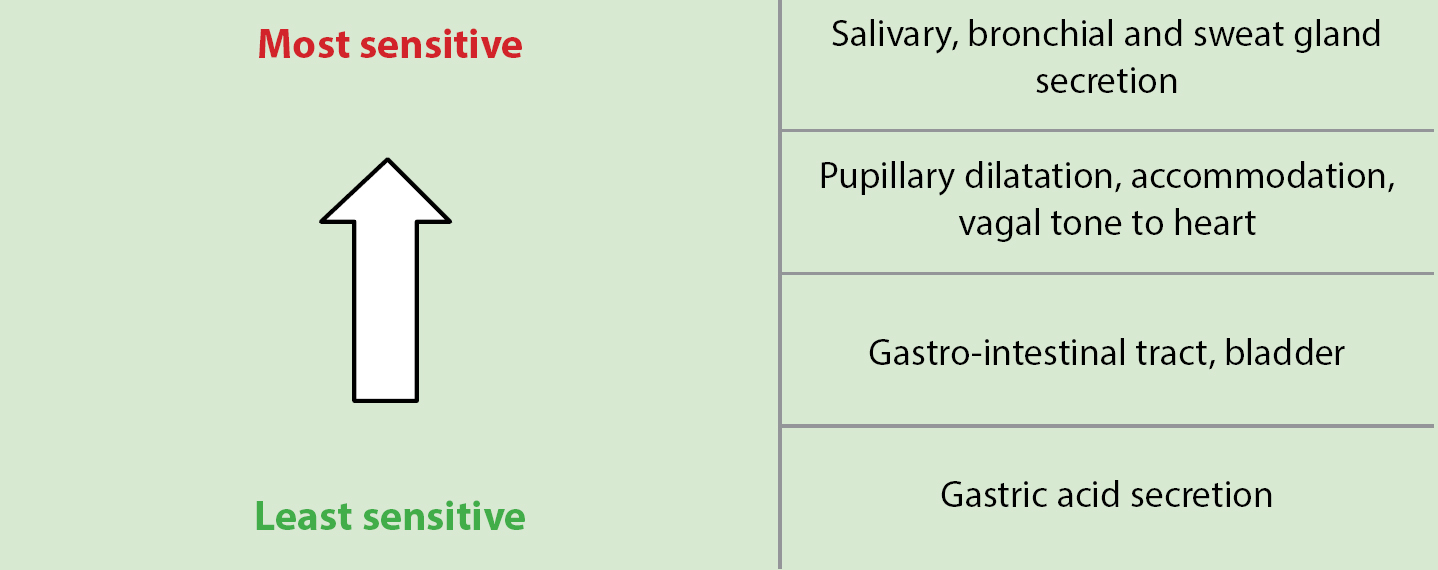
Atropine is a naturally occurring antimuscarinic which blocks all mAChRs. Peripheral antimuscarinic effects are parasympatholytic because they block the actions of parasympathetic nerve activity. Different organs vary in their sensitivity to antimuscarinic actions (Figure 3). Dry mouth is one of the most common antimuscarinic effects.
Figure 3. Sensitivity of parasympathetic receptor organs to antimuscarinics.
Antimuscarinic drugs have a variety of important therapeutic indications (Table 1).
Management of tremor in Idiopathic Parkinson’s disease
Trihexyphenidyl hydrochloride
Management of drug/neuroleptic induced extrapyramidal symptoms
Procyclidine hydrochloride
Pupillary dilatation for opthalmological examination
Tropicamide
What are antimuscarinic adverse effects, and why are older people particularly susceptible?
Despite a number of important and useful clinical applications, antimuscarinic drugs have a number of unfortunate peripheral and central adverse effects (Table 2). Older people are more likely to be taking multiple medications, and polypharmacy carries an increased risk of adverse drug reactions. Older people are more susceptible to medication adverse effects due to changes in pharmacokinetics and reduced hepatic and renal function. Older individuals are at particular risk of central antimuscarinic effects, such as falls and confusion, which is in part due to disruption of the blood brain barrier with age.
PERIPHERAL
CENTRAL
Dry mouth
Memory impairment
Dry eyes
Confusion
Constipation
Disorientation
Reduced peristalsis
Agitation
Blurred vision
Hallucinations
Acute angle closure glaucoma
Delirium
Urinary retention
Falls
Tachycardia
Dizziness
Increased body temperature
Case study part 2
The drug history was confirmed with the general medical practitioner as: aspirin, amitriptyline and oxybutynin. The patient had also been sourcing over-the-counter ranitidine (Zantac, GlaxoSmithKline) from his local pharmacy for heart burn.
How can I identify antimuscarinic drugs and their likely impact?
In addition to the antimuscarinic medications listed in Table 1, there are many drugs with well recognized antimuscarinic effects, including: tricyclic antidepressants (eg amitriptyline), antipsychotics (eg chlorpromazine), antihistamines (eg chlorpheniramine [Piriton, GSK Consumer Healthcare]) and antiemetics (eg prochlorperazine [Stemetil, Sanofi-Aventis; Buccastem, Alliance]). There are also many drugs that are not classically considered to be antimuscarinics, but that have been shown to have antimuscarinic effects (eg ranitidine [Zantac, GlaxoSmithKline]).
Antimuscarinic scoring systems have been developed to aid in the identification of antimuscarinic drugs, and to assist in quantifying the likely antimuscarinic effect. A simple and well-validated tool in older people is the Anticholinergic Risk Scale (ARS) (Table 3). The ARS was designed to estimate the extent to which an older patient may be at risk of antimuscarinic adverse effects.9 Each medication listed on the ARS has a score depending on its antimuscarinic activity of either: 1 (moderate), 2 (strong) or 3 (very strong). The ARS for a patient is the sum of the scores of all medication taken by that patient. Unlisted medications score zero. An ARS of 3 gives a 70% chance of two or more adverse antimuscarinic effects being reported. It is important to check all medications, including over-the-counter medications and inhaled medications. Inhaled tiotropium and ipratropium, used in the treatment of lung disease, have been shown to have systemic antimuscarinic adverse effects10 and, in recent studies, have been assigned an ARS score of 2 for tiotropium and 3 for ipratropium,11 and have therefore been added to Table 3.9
The patient's ARS was calculated to be: oxybutynin (3) + amitriptyline (3) + ranitidine (1) = 7. As an ARS of 3 gives a 70% chance of ≥2 adverse antimuscarinic effects, a strategy to reduce this score should help in alleviating his oral symptoms.
Conclusions and recommendations
Identification of antimuscarinic drugs in the causality of dry mouth can be assisted through the use of scoring systems, such as the ARS. In a patient presenting with dry mouth, the authors recommend:
A detailed medication history, including over-the-counter and inhaled preparations;
Checking medication on a validated scale, eg Anticholinergic Risk Scale;
An enquiry regarding other antimuscarinic adverse effects, eg constipation, dry eyes, confusion;
Communication with the general medical practitioner to enquire whether a medication review could reduce the ARS score.
These steps can prompt medication review with positive health implications. Reduction of antimuscarinic medication may be a modifiable risk factor to reduce morbidity and cognitive impairment, with consequent improvements in quality of life.
Case study part 4
The general medical practitioner was contacted and a medication review requested in view of antimuscarinic use and adverse effects, particularly with regards to the patient's dry mouth. Oxybutynin was discontinued, and nonpharmacological measures were employed for the management of an overactive bladder. The patient's amitriptyline dose was gradually reduced and then stopped. Consequently, dry mouth, constipation and confusion all resolved and the patient reported feeling much better. His mouth felt more comfortable and his full upper denture felt more retentive (Figure 4). His presenting complaint had been resolved, together with an overall improvement in quality of life.
Figure 4. Successful wearing of dentures following resolution of oral symptoms.
Summary for general dental practitioners
Be aware of an increasingly older patient group who live with long-term medical conditions and take multiple medications;
In a patient presenting with dry mouth, take a detailed medication history, including over-the-counter and inhaled preparations, to check for use of antimuscarinic medications. Further help can be gained from antimuscarinic scoring systems (Table 3), or through liaison with the general medical practitioner or Pharmacist;
Following recognition of a drug-related oral problem, advise the patient to attend the general medical practitioner for a medication review. It is useful to provide a brief written summary of your assessment, and your concerns regarding potential culprit antimuscarinic medication;
Reduction of antimuscarinic medication, through medication review, can improve dry mouth, as well as physical and cognitive health and quality of life;
A medication review is defined by the National Prescribing Centre as a ‘structured, critical examination of a patient’s medicines with the objective of reaching an agreement with the patient about treatment, optimizing the impact of medicines, minimizing the number of medication-related problems, and reducing waste.'