Nelson SJ, Ash MMSt Louis: Saunders Elsevier; 2003
Pantvisai P, Messer HH Cuspal deflection in molars in relation to endodontic and restorative procedures. J Endodont. 1995; 21:(2)57-61
Khalaf ME, Alomari QD, Omar R Factors relating to usage patterns of amalgam and resin composite for posterior restorations - a prospective analysis. J Dent. 2014; 42:(7)785-792
Reeh ES, Messer HH, Douglas WH Reduction in tooth stiffness as a result of endodontic and restorative procedures. J Endod. 1989; 15:(11)512-516
Kidd EA, Smith BGN, Pickard HM Making clinical decisions, 7th edn. Oxford: Oxford University Press; 1996
Mondelli J, Steagall L, Ishikiriama A, de Lima Navarro MF, Soares FB Fracture strength of human teeth with cavity preparations. J Prosthet Dent. 1980; 43:419-422
Hansen EK, Asmussen E, Christiansen NC In vivo fractures of endodontically treated posterior teeth restored with amalgam. Endodont Dent Traumatol. 1990; 6:49-55
Aquilino SA, Caplan DJ Relationship between crown placement and the survival of endodontically treated teeth. J Prosthet Dent. 2002; 87:(3)256-263
Fennis WMM, Kuijs RH, Kreulen CM, Roeters FJM, Creuger NHJ, Burgersdijk RCW A survey of cusp fractures in a population of general dental practices. Int J Prosthodont. 2002; 15:(6)559-563
Nagasiri R, Chitmongkolsuk S Long-term survival of endodontically treated molars without crown coverage: a retrospective cohort study. J Prosthet Dent. 2005; 93:(2)164-170
Sorensen JA, Martinoff JT Intracoronal reinforcement and coronal coverage: a study of endodontically treated teeth. J Prosthet Dent. 1984; 51:(6)780-784
Fedorowicz Z, Carter B, De Souza RF, Chaves CA, Nasser M, Sequeira-Byron P Single crowns versus conventional fillings for the restoration of root filled teeth. Cochrane Database Syst Rev. 2012; 5
Craig RG Experimental stress analysis of dental restorations: Part I. Two-dimensional photoelastic stress analysis of inlays. J Prosthet Dent. 1967; 17:(3)277-291
Craig RG, El-Ebrashi MK, Peyton FA Experimental stress analysis of dental restorations: Part II. Two-dimensional photoelastic stress analysis of crowns. J Prosthet Dent. 1967; 17:(3)292-302
Farah JW, Dennison JB, Powers JM Effects of design on stress distribution of intracoronal gold restorations. J Am Dent Assoc. 1977; 94:1151-1154
Faigenblum M Tooth surface loss: removeable prostheses. Br Dent J. 1999; 186:273-276
Murphy F, McDonald A, Petrie A, Palmer G, Setchell D Coronal tooth structure in root-treated teeth prepared for complete and partial coverage restorations. J Oral Rehab. 2006; 36:451-461
Bandlish RB, McDonald AV, Setchell DJ Assessment of the amount of remaining coronal dentine in root-treated teeth. J Dent. 2006; 34:(9)699-708
Fleiss JL, 2nd edn. New York: John Wiley; 1981
Landis JR, Koch GG The measurement of observer agreement for categorical data. Biometrics. 1997; 33:(1)159-174
Brunton PA Fracture resistance of teeth restored with onlays of three contemporary tooth-colored resin-bonded restorative materials. J Prosthet Dent. 1999; 82:(2)167-171
Setcos JC, Babaei-Mahani A, Di Silvio L, Mjör IA, Wilson NHF The safety of nickel containing dental alloys. Dent Mater. 2006; 22:(12)1163-1168
Massa F, Dias C, Blos CE Resistance to fracture of mandibular premolars restored using post-and-core systems. Quintessence Int. 2010; 41:49-57
Burke FJT, Wilson NH, Watts DC The effect of cuspal coverage on the fracture resistance of teeth restored with indirect composite resin restorations. Quintessence Int. 1993; 24:875-880
Basir MM, Ghomsheh ET, Azari A, Hosseini ZM, Far MV Effect of amalgam cuspal coverage on the fracture resistance of endodontically treated teeth. J Dent Med. 2013; 26:(2)91-98
Krämer N, Frankenberger R, Pelka M, Petschelt A IPS Empress inlays and onlays after four years – a clinical study. J Dent. 1999; 27:(5)325-331
Krämer N, Frankenberger R Clinical performance of bonded leucite-reinforced glass ceramic inlays and onlays after eight years. Dent Mat. 2005; 21:(3)262-271
Ozyoney G, Yanıkoglu F, Tagtekin D, Hayran O The efficacy of glass-ceramic onlays in the restoration of morphologically compromised and endodontically treated molars. Int J Prosthodont. 2013; 26:(3)230-234
Stappert CFJ†, Guess PC, Chitmongkolsuk S, Gerds T, Strub JR Partial coverage restoration systems on molars – comparison of failure load after exposure to a mastication simulator. J Oral Rehab. 2006; 33:698-705
Hmaidouch R, Weigl P Tooth wear against ceramic crowns in posterior region: a systematic literature review. Int J Oral Sci. 2013; 5:(4)183-190
Cuspal-coverage restorations are important to preserve the integrity of a weakened tooth against the forces of occlusion. This article discusses the clinical indications for both direct and indirect cuspal-coverage restorations and the evidence supporting their use. Factors that modify a tooth's ability to dissipate normal occlusal forces and the effect cuspal-coverage restorations have on force distribution are examined. Clinical criteria, choice of restorative material and methods for tooth preparation are also discussed.
CPD/Clinical Relevance: Re-enforcement of weakened teeth with cuspal-coverage restorations provides a minimally invasive alternative to conventional crowns.
Article
A cuspal-coverage restoration may be defined as one where the restorative material covers all, or part of, one or more cusps of a molar, premolar or canine tooth. In this regard, conventional crowns may be classed as cuspal-coverage restorations. Cuspal-coverage restorations may be either direct or indirect restorations.
For the purposes of this article, the term ‘cuspal coverage’ will refer to a technique used for either direct or indirect restorations that covers only part of one or more cusps of a molar or premolar tooth. These restorations may also be called direct or indirect onlays.
The main role of a cuspal-coverage restoration is to reinforce a weakened cusp, thus reducing the chance for fracture and overall failure of the tooth. Other roles include:
Augmentation of cusp shape to facilitate modifications to an existing occlusal scheme;
A means of securing additional resistance form or bonding area for indirect or direct restorations.
To understand the indications for cuspal coverage it is necessary to discuss the forces on teeth and factors that modify the ability of the tooth to resist such forces.
Force distribution on teeth
In normal function, teeth have the greatest forces applied to them as a result of mastication of food. For individual teeth, the ideal occlusal contact distributes the force down the long axis of the tooth and occurs at the same time as all the other teeth in the arch.1 Molar and premolar teeth are most often involved in crushing and grinding of food to aid swallowing and subsequent digestion. Normally, occlusal loading on such teeth is between 350–700N and for an average cumulative total of 17.5 minutes per day.2 There are a number of factors that can affect the ability of the tooth to withstand these parameters including:
The prevalence of dental caries and restorative interventions;
Previous endodontic treatment;
Previous tooth loss; and
Parafunction.
Dental caries and restorative interventions
Dental caries and subsequent restorative interventions result in substantial loss of tooth structure, weakening the tooth and increasing the likelihood of fracture of remaining tooth tissue. The three-dimensional extent of dental caries in a tooth can affect the residual tooth strength. For example, caries may undermine cusps of teeth, resulting in a predisposition to undergo excessive flexure with an increased likelihood of subsequent cuspal fracture.3 Such undermining of cusps may also be a feature of conventional amalgam cavity preparation for the purposes of retention of the restoration. However, advances in the use of adhesive technology and a shift towards minimally invasive dentistry have encouraged an increase in the clinical use of composite as a posterior restorative material and a reduction in cavity size due to the obsolescence of retention and resistance form.4
Reeh et al demonstrated the effect that restorative and endodontic procedures have on the stiffness, and therefore fracture resistance, of remaining tooth tissue.5 Their results indicated that occlusal and mesio-occlusal-distal (MOD) cavity preparations reduced tooth stiffness by 20% and 63%, respectively. The additional reduction in tooth stiffness as a result of a subsequent endodontic preparation was approximately five percent. There is some limited in vitro evidence that premolar teeth after endodontic treatment and restoration are particularly prone to cuspal fractures without a cuspal-coverage restoration, possibly due to their overall shape.6
Mondelli et al prepared Class I and Class II cavities in freshly extracted premolar teeth. They demonstrated, in vitro, the protective effect of preserving the marginal ridges and recommended that Class II cavities, where the occlusal isthmus was half the intercuspal width, or more, should receive indirect restorations with cuspal coverage.7
The mechanism of failure results from the application of a ‘wedging’ force on the tooth, exerting buccal and lingually directed lateral forces on the remaining tooth walls.8 Fisher et al demonstrated areas of high stress concentration in conventional inlay restorations that increased the likelihood of fracture of remaining tooth walls when compared to the ‘protective’ force distribution exhibited with onlay restorations.9
Traditionally, photoelastic stress analysis has been used to analyse the distribution of forces through restorations and teeth.10 This involves the analysis of colourful chromatic fringes, seen on cross-sectional slices of teeth when viewed in polarized light, and how these fringes change when stresses are applied to teeth.11 Although this has been a valuable method of stress analysis, in the current literature, finite element analysis is more commonly used due to its accuracy, ease and adaptability in stress analysis. This involves the analysis of complex structures using a computer-based mathematical model. Structures are broken down into simple blocks and equations of how these behave individually are generated and combined to assess the overall response of a structure to stress. Finite element analysis demonstrates greater sensitivity in the analysis of structural response to stress, although this is dependant on the accurate description of several parameters, such as the structure of the outer surface of the tooth.10
Care must be taken with the final restoration contour. Simultaneous occlusal contact with axial loading may not occur if the occlusal surface is restored incorrectly. A poorly contoured occlusal surface of an intracoronal restoration may result in a premature contact which, if on the incline of a cusp, will result in lateral forces to that cusp with the possibility of subsequent fracture.1
Previous endodontic treatment
Lack of pulp tissue in an endodontically treated tooth will reduce the opportunity for preventive biofeedback under occlusal loading and could partly explain the increased fracture rate in posterior root-filled teeth when restored with an intra-coronal restoration.12 A retrospective cohort study, involving 220 endodontically treated teeth over an 11-year period, concluded that composite restorations offered a degree of improved fracture resistance, whereas amalgam restorations provided little or no resistance to cuspal movement. However, when compared, conventional direct restorations have been shown to be less successful with regard to overall tooth survival than restorations with cuspal coverage.13
A further factor that must be considered with regard to endodontic treatment is the fracture pattern and subsequent tooth restorability. Fennis et al demonstrated that endodontically treated teeth are more often associated with a subgingival fracture location, potentially impacting on the subsequent restorability of the tooth.14
Reports of improved survival rates of endodontically treated teeth restored with a crown are widely cited in the dental literature.13,15,16 Although it must be noted that a Cochrane systematic review in 2012, appraising ‘the success rate of single crowns versus conventional fillings for the restoration of endodontically treated teeth', concluded that there is insufficient high quality evidence to endorse the clinical effectiveness of crown placement for the long-term survival of endodontically treated teeth.17
Cuspal-coverage restorations facilitate the distribution of masticatory forces down the long axis of the tooth, providing an element of support for residual cusps.18 This finding was corroborated by Craig et al, who demonstrated the protective dissipation of forces evident when the restoration overlays the cusps of a tooth. The authors analysed the stress distribution, using photoelastic two-dimensional stress analysis, when teeth restored with MOD inlays and crown preparations were loaded. They concluded that cuspal-coverage restorations reduce the compressive stresses elicited by MOD restorations and redistributed them towards more protected areas of remaining tooth tissue.19,20 It was also noted that a rounded cuspal reduction prevents high compressive stresses being focused on the fitting surface of the restoration, possibly leading to restoration failure.20 Farah et al demonstrated substantially lower compressive stresses were present when cusps were overlaid with gold restorations. Furthermore, the authors evidenced, through an in vitro study, that when a cusp was completely protected by a restoration, the average compressive stress exerted on residual tooth structure was significantly lower and more uniformly distributed than with restorations that did not overlay the residual cusps of a tooth.21
Tooth loss
Tooth loss may result in tilting, rotating or drifting of teeth and a subsequent change in the occlusal forces applied to them. In many cases, the change in position of teeth may result in the application of non-axial forces during function.22 The application of this force may result in excessive flexure and fracture of cusps previously weakened by caries or restorative intervention. Indeed, there may be forward movement of the mandible to achieve best occlusal contact in cases where tipping or tilting has resulted in an abnormal occlusal scheme, further influencing the application of non-axial forces to teeth.23 Craig et al also demonstrated that stress concentration was greater in tilted teeth than their non-tilted counterparts and this may increase the likelihood of fracture.19
Parafunctional activity
Increased occlusal loading on all teeth may occur due to various types of normal activity, for example, clenching the teeth together when lifting heavy loads, or due to abnormal activity such as clenching or grinding habits, otherwise known as parafunction or bruxism. Such forces on a tooth that has already been compromised by caries or extensive or poorly contoured restorations may result in crack formation or fracture. Additionally, bruxism may result in the application of non-axial forces to teeth and further increase the likelihood of tooth fracture due to suboptimal distribution of occlusal forces.22
Clinical factors for cuspal coverage
Through the use of cuspal-coverage restorations, practitioners have the opportunity to develop a greater degree of control over the direction of occlusal loading on a tooth. Therefore, care can be taken to ensure an optimal occlusal scheme aiming for direct loading down the long axis of the tooth and preventing potentially pathological interferences in excursion.
It can be seen that a variety of factors can modify the intensity and direction of forces upon teeth, as well as the ability of the tooth to resist such forces. With this information, clinicians have developed a number of indications for cuspal coverage.
When cuspal coverage is indicated for a tooth, a practitioner has several restorative options for replacement of lost tooth tissue. In the authors' experience, general dental practitioners more commonly opt to restore teeth with full cuspal-coverage restorations (crowns) as opposed to partial cusp coverage restorations (onlays). There is a lack of evidence available to support this. However, much of the endodontic literature discusses tooth survival of endodontically treated teeth restored with crowns, rather than onlay restorations, and so practitioners may automatically make this choice. There may be a variety of possible reasons for this choice including; practitioner experience, ease of preparation, laboratory costs and remuneration fees.
Clearly, there is less tooth destruction with partial coverage preparations compared with full coverage tooth preparations. Murphy et al demonstrated that, when practitioners were given the opportunity to assess the degree of tooth tissue loss following preparation for a full coverage restoration, they tended to revise their choice of preparation to a less destructive cuspal-coverage preparation, such as an onlay.24
Essentially, the decision to provide a cuspal-coverage restoration comes down to:
The amount and distribution of remaining coronal tooth tissue;
The type of restorative material to be used;
The load to be applied to a tooth during daily function; and, possibly,
The knowledge and experience of the practitioner.
The first two of these factors will now be discussed.
The amount and distribution of remaining coronal tooth tissue (tooth restorability)
Any restorative procedure requires an initial diagnosis to facilitate the planning of treatment. A key stage in this is the assessment of the restorability of compromised teeth and planning for appropriate reconstruction. In order to plan the placement of restorations appropriately, practitioners must be able to appraise the value of remaining tooth tissue prior to definitive restoration. Ideally, this should be done before undertaking any endodontic treatment for a tooth. However, this is not always possible.
The evidence base for appraising tooth restorability is not extensive. A common method of assessing tooth restorability involves the visualization of the remaining tooth tissue following preparation for a cast restoration.13,16
In an attempt to increase objectivity, Bandlish et al formulated the Tooth Restorability Index (TRI), an assessment methodology to determine the strategic value of remaining tooth tissue.25 This technique divided the remaining tooth structure into sextants and assigned a score to each sextant based on the thickness, height and distribution of coronal dentine present. The scores allocated to each sextant ranged from 0 to 3. Individual sextant scores are added together to give a score from 0 to 18, indicating the restorability of the tooth. Lower scores represent a more guarded prognosis for restoration. This study also highlights the utility of assessing teeth in this way, as there was fair-to-good or substantial agreement between assessors (Kappa = 0.63).26,27 Although this assessment criterion is a useful objective tool in the appraisal of tooth restorability, it is necessary to consider that advances in adhesive dentistry have also facilitated the restoration of many teeth which may have low TRI scores.28
The type of restorative material to be used
Cuspal-coverage restorations can be created using a variety of dental materials. Most commonly, gold, composite, amalgam, porcelain or porcelain-fused-to-metal restorations are utilized. Other cast restorations, including nickel chromium, may also be considered but have fallen out of favour with practitioners, possibly due to concerns regarding possible allergic reactions.29
Gold
Gold onlay restorations are commonly utilized as a suitable alternative to full or partial coverage crowns when maintaining residual tooth tissue is a priority. These restorations have the advantage that they are usually less destructive to tooth tissue, as less preparation is required, although a significant laboratory cost may be incurred to the practitioner. Nagasiri and Chitmongkolsuk demonstrated that the strength of teeth restored with gold onlay restorations was significantly higher than teeth restored with amalgam or composite restorations15 (Figure 1).
Figure 1.
(a, b) Cuspal coverage with gold for DO onlay retainer for tooth LR5 as part of an all gold conventional bridge.
Composite
Brunton et al carried out an in vivo randomized controlled trial assessing the fracture resistance of several tooth-coloured onlay materials. They concluded that indirect composite restorations provided a greater degree of protection to the residual tooth compared to ceramic or fibre-reinforced composite restorations of a similar design.28,30 Additional work by Burke et al also concluded, through in vitro testing of composite inlay and onlay restorations, that a significant increase is seen in fracture resistance of teeth restored with composite onlay restorations when compared to composite inlay restorations.31
Amalgam
Although amalgam is often advocated in expert opinion articles as an alternative material for cuspal-coverage restorations, current literature is bereft of high quality studies assessing the long-term survival of complex amalgam restorations overlaying the cusps of teeth.32 An in vitro study by Basir et al compared the fracture resistance of cuspal-coverage amalgam MOD restorations with that of conventional amalgam MOD restoration, concluding that cuspal overlay techniques were more effective in the prevention of tooth fracture.33 Additionally, amalgam restorations may offer an economic advantage to other materials owing to its relatively low cost.
Ceramic
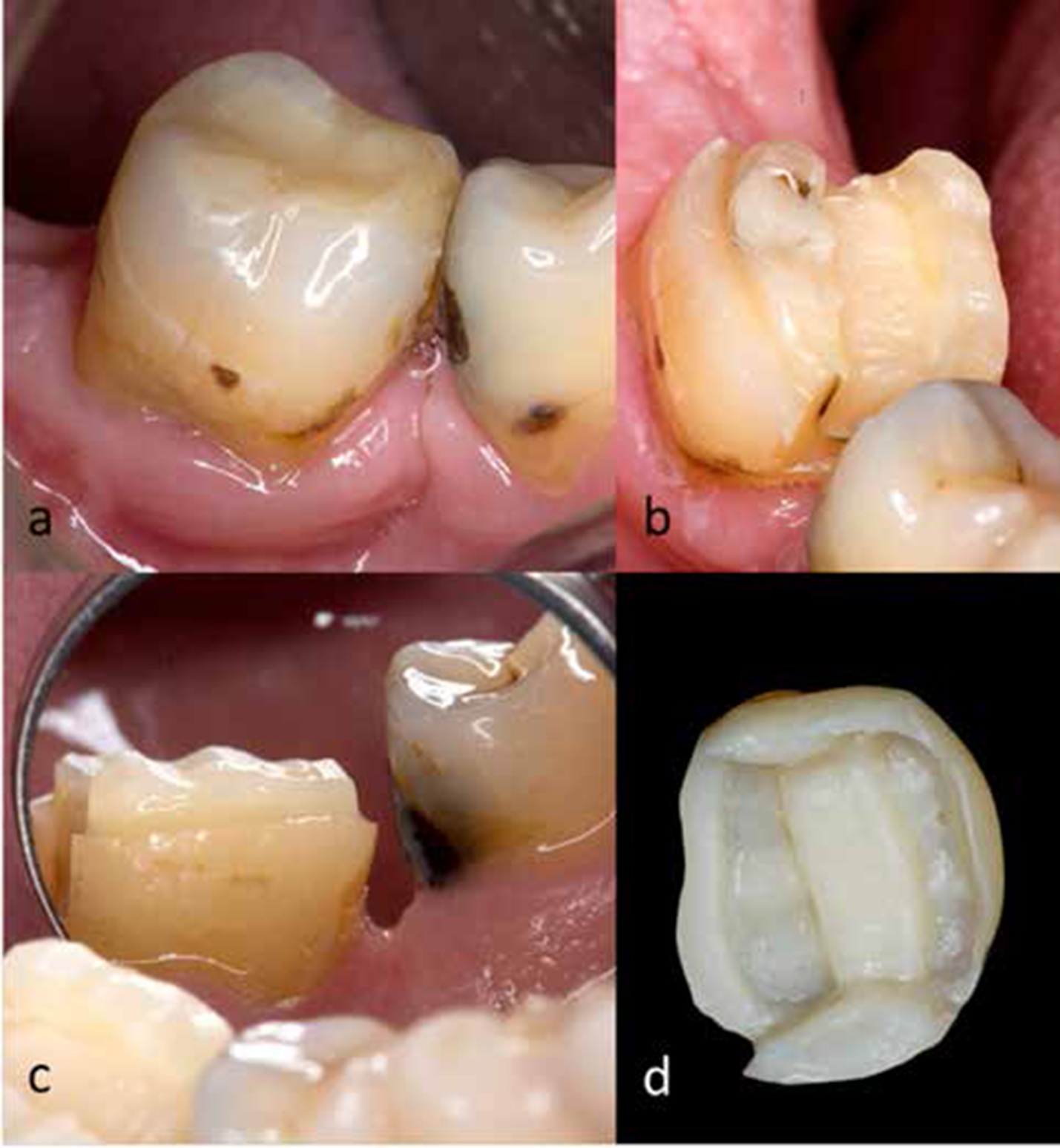
Advances in milled and pressable ceramics have encouraged an increase in their use, although there is currently insufficient evidence as to their long-term success rates.34 Krämer et al demonstrated a 7% and 8% failure rate of ceramic inlays and onlays after four and eight years, respectively.35,36 Additionally, Ozyoney et al demonstrated a 92.5% success over a four-year period with glass ceramic onlays restoring endodontically treated teeth, although it is evident that current literature lacks high quality long-term studies.37 The increasing use of CAD/CAM technology within modern dentistry is encouraging a growing number of practitioners to use ceramic restorations. Although the evidence base for their use is limited and lacking long-term follow-up, ceramic onlay materials have been shown to achieve restoration strengths suitable for use in cuspal overlay restorations38 (Figure 2).
Figure 2. All-ceramic onlay preparation for tooth LR6, previously restored with narrow but deep amalgam that developed a mesial-distal fracture initially resolved with root canal therapy and a bonded intra-coronal composite restoration. (a) Pre-operative, (b) shoulder preparation at supporting cusp with 1.5 mm inter-occlusal clearance, (c) deep chamfer preparation on lingual aspect and (d) fitting surface morphology of provisional restoration.
One concern regarding the use of all-ceramic restorations is the potential for abrasion of opposing tooth substance. Although commonly referenced, a systematic review carried out by Hmaidouch and Weigl demonstrated that there is currently insufficient evidence to conclude that all-ceramic restorations are associated with increased toothwear. This study concluded that some ceramic restorations are as wear friendly as metal ceramic restorations, although all-ceramic restorations may have an abrasive nature due to suboptimal surface treatment, such as failure to polish adequately or re-glaze following occlusal adjustment.39
Methods of tooth preparation
When preparing a tooth for a cuspal-coverage restoration it is important to consider the requirements for the successful use of the restorative material chosen. Preparation of the residual tooth/ core must facilitate an adequate thickness of restorative material to prevent perforation of the restoration or fracture of inadequately supported sections of the restoration.22
A common clinical practice is to ensure that there is adequate reduction of supporting cusps. This is also known as a functional cusp bevel. Supporting cusps are defined as those cusps or incisal edges of teeth that contact in and support maximum intercuspation. These are usually buccal cusps of the mandibular posterior teeth, the maxillary palatal cusps, and the incisal edges of the mandibular anterior teeth.40 Generally, increased occlusal forces are applied to supporting cusps. For gold restorations a minimum of 1.5 mm thickness is commonly required over a supporting cusp, whereas metal-ceramic and all-ceramic restorations require 1.5 mm and 1.5 mm to 2 mm occlusal reduction, respectively.41
There is a degree of uncertainty in the literature as to the absolute indications for a shoulder, chamfer or deep chamfer margin preparation for a cuspal overlay restoration. In the authors' opinion, the most commonly utilized margin preparations include: a chamfer preparation for a gold restoration; a deep chamfer preparation for all-ceramic preparations and a shoulder preparation for metal ceramic restorations. There is also some evidence from standard texts to suggest that a shoulder preparation should be utilized when a restoration is required to overlay a supporting cusp, regardless of the material chosen, as this promotes a bulk of onlay material to protect the supporting cusp.18
Conclusions and recommendations
Based on the previous information, the following recommendations for cuspal-coverage/onlay restorations could be applied to molar and premolar teeth.
Restoration of teeth
Conventional cavity preparation, where the marginal ridge is lost and where the isthmus is more than half the occlusal width, would benefit from cuspal protection by either bonding the restoration within the cavity or cuspal coverage.7
Endodontically treated molars and premolars where cavity preparation has resulted in the loss of one or more marginal ridges would probably benefit from a final restoration with cuspal protection.6,7
Cuspal coverage may be used to increase the resistance form of an indirect restoration thus reducing the stress on any cementation agent.
Materials
Gold is still a popular choice of material for cuspal coverage when aesthetics are not a priority. It requires minimal tooth preparation and has a long track record of success.15,18
Indirect composite restorations may be used with some success.30,31
Ceramic is a popular choice for cuspal-coverage onlays, but there are no long-term data available for their survival or the effect of the newer ceramic restorations on the opposing tooth structure.39
With the increasing popularity of tooth-coloured restorative materials and the skill required for placement, amalgam is less favoured than gold or restorative materials with better aesthetic properties.
Method of preparation
If cuspal coverage is to be undertaken this should ideally be thicker over the supporting cusps.18
Between 1 and 2 mm of occlusal tooth reduction is required to overlay a cusp. This will be greater on the supporting cusp compared with the non-supporting cusp.18
The type of margin preparation is generally not relevant, although shoulder margins result in increased strength of restorative material and might be considered over a supporting cusp.18
The current literature lacks clarity on:
The specific criteria important when deciding to undertake cuspal coverage for vital teeth;
The choice of restorative material used for cuspal coverage; and
The method of tooth reduction when a decision has been made to provide cuspal coverage.