Wood P, Stanworth S, Burton J Recognition, clinical diagnosis and management of patients with primary antibody deficiencies: a systematic review. Clin Exp Immunol. 2007; 149:410-423
Batista EL, Novaes AB, Calvano LM, do Prado EA, Goudouris ES, Batista FC Necrotizing ulcerative periodontitis associated with severe congenital immunodeficiency in a prepubescent subject: clinical findings and response to intravenous immunoglobulin treatment. J Clin Periodontol. 1999; 26:499-504
Kishimoto H, Urade M, Noguchi K, Sakurai K Common variable immunodeficiency with unusual vegetative lesions of the tongue and labial mucosa – a case report. Oral Surg Oral Med Oral Path. 2001; 91:85-88
Gemmell E, Yamazaki K, Seymour GJ Destructive periodontitis lesions are determined by the nature of the lymphocytic response. Crit Rev Oral Biol Med. 2002; 13:17-34
Kinane DF, Takahashi K, Mooney J Crevicular fluid and serum IgG subclasses and corresponding mRNA expressing plasma cells in periodontitis lesions. J Perio Res. 1997; 32:176-178
Bimstein E, Matsson L Growth and development considerations in the diagnosis of gingivitis and periodontitis in children. Pediatr Dent. 1999; 21:186-191
Guidelines for periodontal screening and management of children and adolescents under 18 years of age. 2012. (Accessed January 4, 2013)
Gingival inflammation and aggressive periodontitis in a child with a specific antibody deficiency Singithi Liyange David Edgar Michael D Shields Gerard J Linden Dental Update 2024 43:2, 707-709.
Authors
SingithiLiyange
BDS
Senior House Officer, Periodontal Department, School of Dentistry, Belfast Health Social Care Trust
Professor of Periodontology, Periodontal Department, School of Dentistry, Belfast Health Social Care Trust and Centre for Public Health, Queen's University Belfast, Northern Ireland, UK
Exuberant gingival inflammation accompanied by periodontitis is a rare finding in a very young child and may indicate a defect in the host response. Affected children should be referred to appropriate specialists to establish a definitive diagnosis. A 5-year-old girl presented with persistent gingival inflammation and periodontal destruction. Immunological investigations identified specific polysaccharide antibody deficiency which, when treated, resulted in a significant improvement in the gingival condition. This case illustrates the need for integrated management by a wide range of dental and medical specialists. Antibody deficiency is rare but, if not identified and treated effectively, can be associated with chronic ill health and decreased life expectancy.
CPD/Clinical Relevance: This article describes a rare case of gingival inflammation accompanied by periodontitis in a very young child secondary to an underlying host antibody deficiency and details the investigation, management and clinical outcomes.
Article
Gingival inflammation can occur in very young children prior to the eruption of the permanent teeth, however, for the same exposure to plaque, gingivitis is not as intense as that found in older children and adolescents.1 Periodontitis is extremely rare in childhood and the term prepubertal periodontitis was introduced by Page et al2 to describe localized or generalized periodontal destruction in children. In a more recent classification, this condition has been renamed aggressive periodontitis.3 Functional defects in inflammatory or immune responses are often associated with periodontal problems, such as aggressive periodontitis in childhood.4 Since possible defects in the host response often underpin such conditions, it is important to refer affected children to appropriate specialists for investigations to establish a diagnosis. This case describes the occurrence of persistent gingival inflammation with evidence of periodontal destruction in a 5-year-old girl. Further investigations identified an underlying defect in the immune system which had significant implications for the general health of the affected girl. The case highlights the need for the integrated care of such cases to ensure that they receive appropriate and timely treatment to maintain good general health.
Clinical presentation
A 5-year-old Caucasian girl was referred to the Periodontal Department at the School of Dentistry, Belfast with a history of persistent gingival inflammation. The patient's mother reported that her daughter's gingivae were swollen, tended to bleed in response to toothbrushing, and that the condition had deteriorated in the previous year. She felt that this was linked to her daughter being ‘generally unwell’ throughout her childhood. The mother was also concerned that her daughter, who was 19 kg, was not gaining weight, which she attributed to her unwillingness to eat due to her painful gingivae. Her medical history included pneumonia in the previous winter and recurrent chest and urinary tract infections since she was an infant, with prescriptions of systemic antibiotics on almost a monthly basis in the previous year. There was no family history of either periodontitis or any genetic susceptibility to recurrent infections.
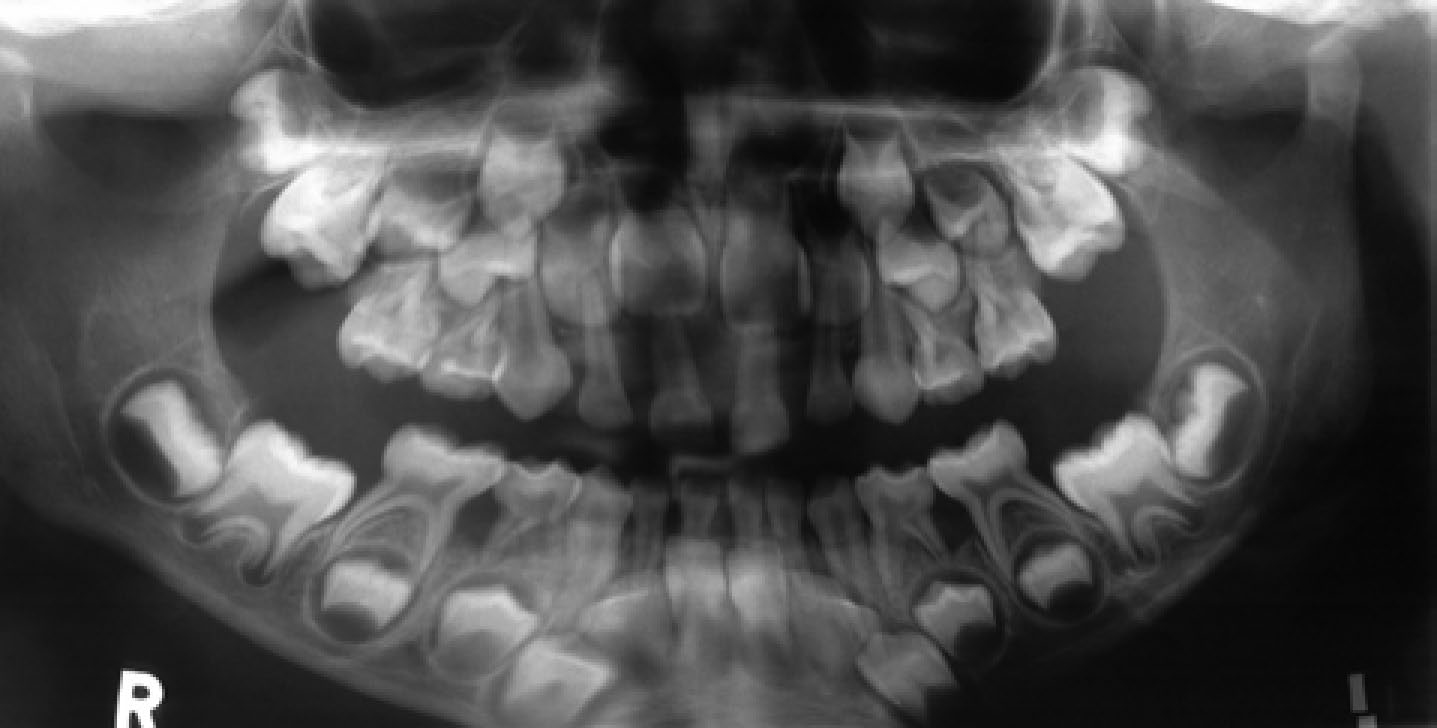
Clinical examination revealed a complete primary dentition with gross swelling of the labial gingivae associated with the upper and lower anterior teeth (Figure 1). Gingival sulcus depths of 5 mm were recorded, although probing was limited due to tenderness of the tissues. Radiographic examination indicated reduced interdental bone levels associated with the incisors and primary molars (Figure 2).
Figure 1. Gingival condition at initial presentation.Figure 2. Bone loss on distal aspects of lower first primary molars.
Case management
The differential diagnosis included gingival enlargement due to oedematous gingivitis, with localized aggressive periodontitis secondary to a granulomatous condition such as orofacial granulomatosis (OFG) or a primary immune deficiency (PID). A biopsy of the lower labial gingivae showed a moderate chronic inflammatory cell infiltrate but no evidence of granulomatous inflammation and was consistent with non-specific chronic inflammatory changes. The pathology report ruled out OFG and plasma cell gingivitis. Patch testing was negative and excluded an allergic basis. The results of the blood investigations were generally within normal limits except for a mild lymphopenia. The total lymphocyte count was 1.62 x 109/L which was below the lower limit of normal (2.9 x 109/L). The patient was referred for immunological assessment.
The patient was seen at the Immunology Clinic, Royal Belfast Hospital for Sick Children, for assessment of immune function. Results of initial investigations confirmed normal levels of total immunoglobulins and IgG subclasses (Table 1). The classical complement pathway function was 615 KU/L, which was within normal limits (250–700 KU/L). There was an absolute lymphopenia but no absolute deficiency of major T, B or NK cell subsets (Table 2). Neutrophil expression of adhesion molecules (CD11a, b, c and CD15) was normal, as was neutrophil respiratory oxidative burst activity. Lymphocyte proliferative responses (to PHA, PMA and anti-CD3) were normal.
Test
Result (g/L)
Normal Range (g/L)
IgG
7.32
4.9–16.1
IgA
0.55
0.4–2.0
IgM
1.02
0.5–2.0
IgG1
5.14
3.6–7.3
IgG2
2.41
1.4–4.5
IgG3
1.16
0.3–1.1
IgG4
0.32
<1.0
Test
Absolute Count (x 109/L)
Normal Range (x 109/L)
Total lymphocyte count
1.62
2.9–5.1
CD3
1.14
1.8–3.0
CD4
0.47
1.0–1.8
CD8
0.52
0.8–1.5
CD19
0.29
0.7–1.3
CD16/56
0.17
0.2–0.6
Test immunizations with tetanus toxoid and Pneumovax II (Sanofi Pasteur MSD) vaccines were performed to check whether the immune response was functioning properly, as indicated by changes in the production of antibodies to the test toxins. The initial response to tetanus vaccination was good but there was little or no response to vaccination with pneumococcal antigens, as measured both by whole response ELISA and pneumococcal serotype specific analysis (PSSA) (Table 3). In PSSA analysis post immunization, no serotypes exceeded the WHO reference level (0.35 mg/mg/L). These results were consistent with a specific defect in antibody production, however, given the patient's age, were not considered to provide definitive proof of requirement for immunoglobulin replacement therapy (IRT), although a trial of IRT was offered at that stage. The girl had intermittent chest, urinary and herpetic eye infections over the following 2 years and had persistent gingival swelling throughout (Figure 3). During that period a number of her primary incisors were replaced by their permanent successors. Examination of the exfoliated teeth showed calculus present on the root surface (Figure 4), which confirmed that there had been loss of periodontal attachment and supported the clinical and radiographic diagnosis of periodontitis.
Antibody
Pre-immunization
Post-immunization
Tetanus toxoid IgG (mg/L)
1.5
86.1
Tetanus toxoid IgG1 (mg/L)
0.5
45.3
Pneumococcal IgG (mg/L)
7.0
11.3
Pneumococcal IgG2 (mg/L)
5.1
5.6
Pneumococcal serotype (mg/L)
1
<0.10
<0.10
4
<0.01
<0.01
5
0.09
<0.02
6B
<0.06
<0.06
7B
0.45
<0.08
9V
0.12
<0.02
14
<0.45
<0.45
18C
<0.06
<0.06
19F
4.60
0.28
23F
<0.03
<0.03
Figure 3. Gingival condition 2 years later during eruption of the lower permanent incisors. Note swelling of the upper palatal gingival tissue.Figure 4. Exfoliated upper primary central incisor showing calculus deposit on root surface below the enamel cement junction.
Further immunological investigations in 2005 confirmed a deficient antibody response to pneumococcal antigens, with failure to mount a satisfactory response to any of the 10 serotypes tested. The girl was 23 kg, which equated to the 9th centile for weight, which meant that, for every 100 children of her age, only 9 would be expected to be of lower weight. A diagnosis of significant antibody deficiency with normal levels of immunoglobulin was confirmed and commencement of intravenous immunoglobulin was recommended, however, this was again declined by the patient's parents. The following year a local oral surgeon excised the swollen gingival tissue related to the lower anterior teeth. This resulted in an initial improvement in appearance, but was followed by regrowth of the gingival tissue. At review in the Periodontal Department 3 months after the surgical treatment, the swelling had re-established (Figure 5).
Figure 5. Gingival condition at mixed dentition stage.
Over the next 3 years the girl attended the Periodontal Department, her local dentist and dental hygienist for regular supportive periodontal treatment on a 2-monthly basis. The gingival condition showed no improvement over this period. In February 2009, the girl was admitted to her local hospital with cavitating pneumonia affecting the left lung. At this stage the immunologist emphasized the absolute indication for immunoglobulin treatment to prevent further life-threatening infections. The risks and benefits of the proposed treatment were discussed with the parents of the affected girl. A course of immunoglobulin replacement was started in September 2009. The regimen was infusion of human immunoglobulin G (Kiovig, Baxter UK), 15 mg every 3 weeks.
Clinical outcomes
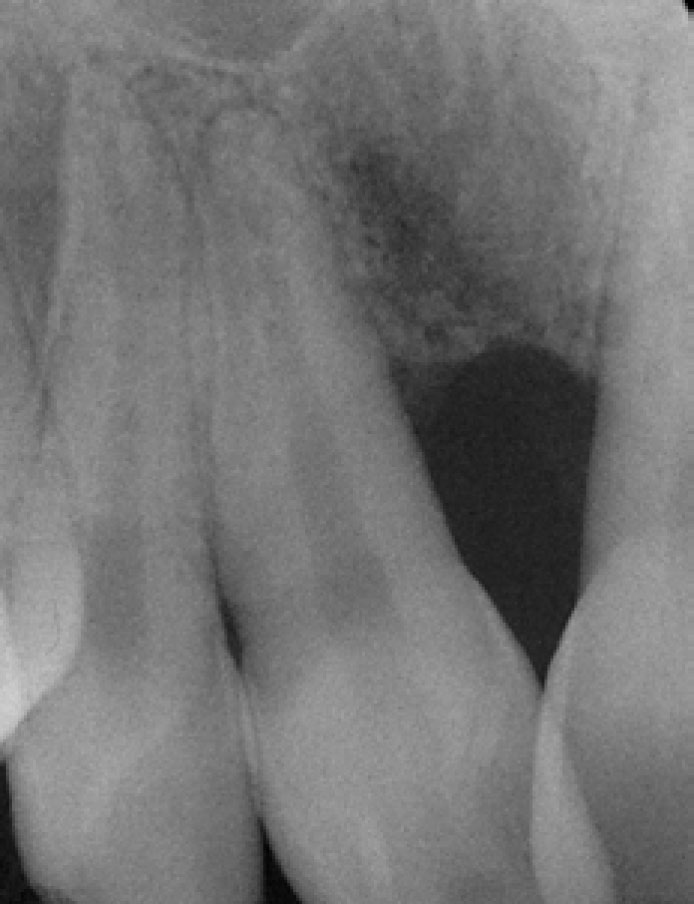
In the 6 months following the start of immunoglobulin replacement therapy the girl gained 6 kg in weight and reported no acute chest infections over the winter months. There was a significant change in her gingival condition in this period (Figure 6) with resolution of the gingival swelling. In the following year to April 2011, the girl contracted swine flu, which resulted in secondary bacterial infection requiring antibiotics, but otherwise remained well. At that time there was localized loss of attachment and bone loss related to the upper central incisor teeth (Figure 7) and this was managed with non-surgical periodontal treatment.
Figure 6. Resolution of gingival condition in March 2010 following immunoglobulin replacement. Localized recession has exposed the full clinical crown of the labially placed lower left central incisor.Figure 7. Radiographic appearance of permanent upper central incisors in 2011 showing reduced bone levels consistent with localized aggressive periodontitis.
The patient was recently reviewed in January 2016 and is now in tertiary education. She remains under the care of the Immunology Department and receives regular immunoglobulin therapy. She reported a few intercurrent chest infections in the past, but none has been severe or required hospitalization. At the review, there was evidence of reduced bone levels, largely limited to the upper incisor teeth, but this was stable and maintained by her primary care hygienist. She was referred to the Orthodontic Department to address the anterior segment crowding and has completed this course of treatment. The patient remains under annual review at the Periodontal Department in the Belfast School of Dentistry.
Discussion
This case describes a young girl who presented with persistent gingivitis and localized aggressive periodontitis. Immunological investigations identified an antibody deficiency, which resulted in increased susceptibility to bacterial infection, in particular recurrent respiratory infections. She responded to immunoglobulin replacement therapy, which led to not only a reduction in the occurrence of respiratory and other infections, but also to a significant improvement in her gingival condition. It could be argued that this was in fact a case of periodontitis as a manifestation of systemic disease, as defined in the generally accepted classification of periodontal diseases.3 The term aggressive periodontitis was used for simplicity, as this described the changes in the periodontal tissues of this young girl, but it is accepted that the changes were the result of defective immune function.
Primary antibody deficiencies are rare and, in many cases, have a genetic basis.5 The identification of the subtype of such a deficiency is often challenging. In the case reported, there was a specific polysaccharide antibody deficiency (SPAD), a condition characterized by an inability to produce functional antibodies to polysaccharide antigens. SPAD can be difficult to identify as the overall level of total immunoglobulins can be normal, as in this case. Low levels of IgA may be present, as was the case with this patient, however, it is defective specific IgG humoral responses which seem to be most important in relation to the expression of symptoms.5 Patients have increased susceptibility to infections, particularly respiratory infections, leading to bronchitis or pneumonia, but are also at increased risk of other bacterial or viral infections. Secondary lung disorders, such as bronchiectasis, constitute the commonest cause of chronic ill health or death.6 There may be non-specific features, such as failure to thrive, and the patient reported was below the 10th centile of weight throughout. There was a reduced response to Pneumovax II vaccination at initial presentation, however, because of difficulty in defining specific antibody deficiency in very young children. The poor response was not taken as definitive evidence of antibody deficiency. It was not until further investigation, which showed virtually no response to vaccination a few years later, that an unequivocal diagnosis of SPAD was made. Initially, the parents declined replacement immunoglobulin treatment as they were concerned about the possible side-effects for their child. Despite symptomatic treatment with antibiotics, there may be irreversible structural tissue damage as a result of repeated local infections. Indeed, it was only when the patient suffered a serious cavitating lung infection, resulting in hospital admission, that they consented to treatment with replacement immunoglobulin.
Treatment involves the replacement of IgG with polyclonal human normal immunoglobulin. There are potential risks of adverse infusion-related reactions, of viral transmission and a theoretical risk of vCJD.6 Management is aimed at preventing complications associated with infections or retarding their progression, optimizing quality of life and life expectancy and, in children, ensuring optimal growth and development.5 Affected individuals require regular specialist monitoring of their clinical status and risk assessment of ongoing therapy, particularly when this is based on immunoglobulin replacement.
Over 5 years elapsed between the initial presentation and the start of immunoglobulin therapy. Over this period the gingival condition remained largely unchanged. Gingival tissue was surgically removed on two occasions but the tissues rapidly returned to the pre-surgical state. The gingival condition rapidly resolved after the institution of immunoglobulin treatment, suggesting that the gingival changes resulted from the antibody deficiency. The clinical picture of the gingival tissues was similar to that described by Batista et al,7 who reported periodontitis in an 8-year-old Caucasian boy with common variable immunodeficiency (CVID), which also responded favourably to the institution of immunoglobulin replacement therapy. One further report of oral changes associated with CVID described exophytic lesions of the tongue and lower labial mucosa, but no gingival involvement, in a 28-year-old male with recurrent pulmonary infections. The lesions rapidly reduced on treatment with intravenous immunoglobulin.8
There was evidence of localized aggressive periodontitis affecting both the deciduous and permanent dentition. Immunoglobulin-producing plasma cells have been demonstrated in the gingival tissues of patients with periodontal disease and there is evidence of antibody response in an antigen-specific manner which is protective and facilitates bacterial clearance and arrests disease progression.9 Patients with higher levels of inflammation have lower IgG levels and failure in local antibody production may contribute to the change from gingivitis to periodontitis.10 It seems likely, therefore, that the lack of antibody response was a factor in upsetting the host response to bacterial species present in dental plaque, resulting in the development of aggressive periodontitis. It is hoped that immunoglobulin replacement combined with periodontal treatment and maintenance will stabilize the periodontal condition in this case.
Conclusion
The observable signs of gingival inflammation in the very young child are modest.11 Guidelines for the assessment of the periodontal condition in children and adolescents, based on the use of the Basic Periodontal Examination, have been produced by the British Societies for Periodontology and Paediatric Dentistry12 and these provide a rational basis for the management of gingival conditions in the young. However, failure to respond to appropriate treatment should raise concerns that there may be an underlying problem. Persistent and obvious gingival inflammation in young children should raise suspicion of PID. The case reported illustrates the need for closely integrated management, with input from a wide range of clinicians, including general dental and medical practitioners and specialists in periodontology, clinical immunology, pathology and respiratory medicine. Antibody deficiency is rare but, if not identified and treated effectively, can be associated with repeated infections, resulting in chronic ill health, diminished quality of life and decreased life expectancy.